



Volume 12, Issue 3 (2024)
Health Educ Health Promot 2024, 12(3): 399-405 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Negara C, Sukartini T, Dewi Y, Nursalam N, Yunara Y. Effect of Animaker and Augmented Reality on knowledge, Attitude, and Behavior toward Non-Ulcer Foot Care in Patients with Type 2 Diabetes. Health Educ Health Promot 2024; 12 (3) :399-405
URL: http://hehp.modares.ac.ir/article-5-76255-en.html
URL: http://hehp.modares.ac.ir/article-5-76255-en.html
1- Department of Medical Surgical Nursing, Faculty of Nursing, Airlangga University, Surabaya, Indonesia
2- Department of Community, Family, Gerontological Nursing, Faculty of Medicine and Health Science, Lambung Mangkurat University, Banjarmasin, Indonesia
2- Department of Community, Family, Gerontological Nursing, Faculty of Medicine and Health Science, Lambung Mangkurat University, Banjarmasin, Indonesia
Full-Text [PDF 624 kb]
(2280 Downloads)
| Abstract (HTML) (1193 Views)
Findings
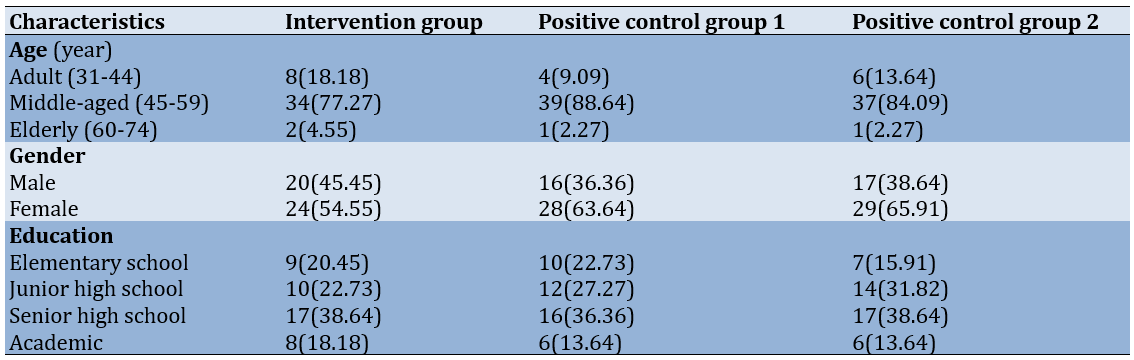
The three age groups were homogenous as the majority of respondents were middle-aged (45-59 years old), predominantly female, and had a senior high school education (Table 1).
Table 1. Frequency of participants’ demographic characteristics (n=132)
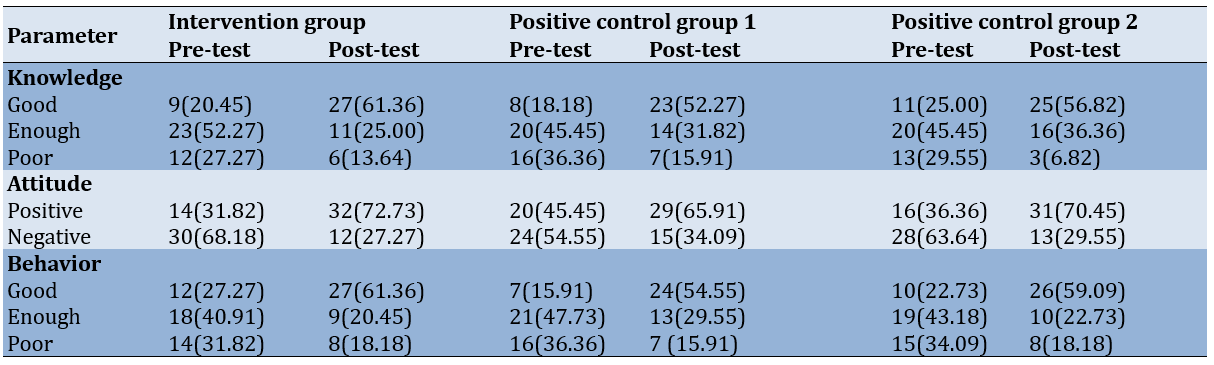
The post-test knowledge scores increased in the intervention group (from 20.45% to 61.36%), positive control group 1 (from 18.18% to 52.27%), and positive control group 2 (from 25% to 56.82%). Meanwhile, the post-test attitude scores increased significantly in the intervention group (from 31.82% to 72.73%), positive control group 1 (from 45.45% to 65.91%), and positive control group 2 (from 36.36% to 70.45%). Also, the post-test behavior scores were assessed as good in all three groups and increased in the intervention group (from 27.27% to 61.36%), positive control group 1 (from 15.91% to 54.55%), and positive control group 2 (from 22.73% to 59.09%; Table 2).
Table 2. Frequency of the knowledge, attitude, and behavior pre- and post-test scores
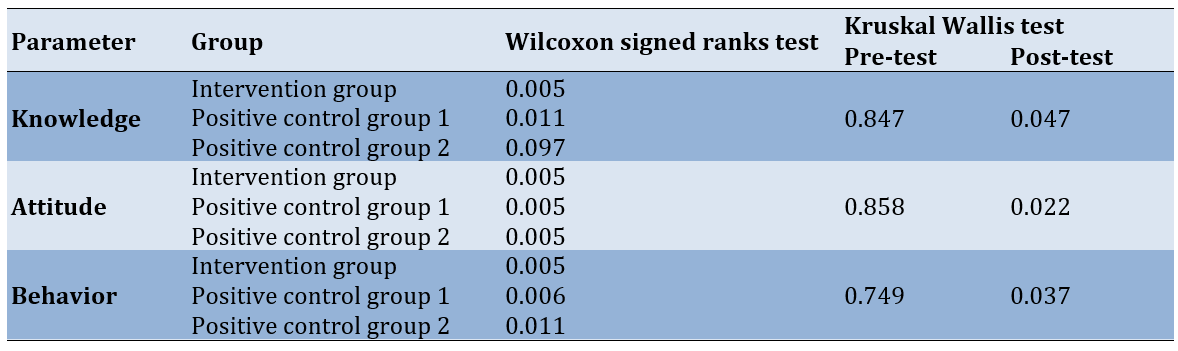
According to the Wilcoxon signed-rank test, foot care education using the combined media of AR+Animaker (p=0.005) and AR (p=0.011) had an impact on patients’ knowledge of non-ulcer foot care in individuals with T2DM; however, no discernible impact of Animaker media education was observed (p=0.097). In addition, the Kruskal-Wallis test showed a significant difference in knowledge among the three groups after receiving non-ulcer foot care education through the AR+Animaker, AR, and Animaker in T2DM sufferers (p=0.047).
On the other hand, the Wilcoxon signed-rank test revealed that the attitudes of type 2 diabetic patients toward non-ulcer foot care were influenced by the foot care education provided through the combined media of AR+Animaker, AR, and Animaker (p=0.005). Also, according to the Kruskal-Wallis test, there was a significant difference in attitudes among the three groups after receiving non-ulcer foot care education through the AR+Animaker, AR, and Animaker (p=0.022)
According to the Wilcoxon signed-rank test, foot care education significantly affected behavior in all groups. Also, according to the Kruskal-Wallis test, a significant difference was found in behavior among the three groups following non-ulcer foot care education through the AR+Animaker, AR, and Animaker (p=0.037; Table 3).
Table 3. Bivariate test of measurement pre- and post-test
Discussion
This research aimed to discover how augmented reality media and Animaker affect non-ulcer foot care behavior among people with type 2 diabetes, specifically regarding foot care education. The results indicated that the level of knowledge about non-ulcer foot care in the positive control group 2 at the beginning of the measurement was predominantly in the poor category; however, after receiving education through Animaker media, most participants moved to the good category. The results of the Wilcoxon signed-rank test showed no significant difference between knowledge levels before and after education through Animaker media. In positive control group 1, the level of knowledge about non-ulcer foot care before receiving education through AR media was primarily in the poor category; after the education, most participants were in the good category. Similarly, the level of knowledge about non-ulcer foot care in the treatment group before receiving education through AR+Animaker media was mostly in the poor category, whereas after the education, almost all participants were in the good category. The results of the Wilcoxon test for knowledge in the positive control group 1 and the treatment group showed that there was a significant difference between knowledge before and after the intervention. Prior to receiving education through AR+Animaker media, the majority of the treatment group’s knowledge regarding non-ulcer foot care fell into the poor category; however, following education through AR+Animaker media, nearly all of them moved into the good category. The knowledge obtained from the Wilcoxon test in both the treatment group and the positive control group 1 demonstrated a significant difference between their pre- and post-intervention knowledge.
When used in conjunction with audio-visual materials, Animaker media can raise the knowledge scores of individuals with T2DM regarding non-ulcer foot care [17]. The application of AR improved patient satisfaction and knowledge retention. Additionally, video media enhances the understanding of women of childbearing age about early cervical cancer detection in various circumstances [18]. One of the key factors in determining how someone acts is their knowledge. Knowledge is gained after an individual perceives a specific object. The goal of the learning process is to equip patients with knowledge so that cognitive control (which is ultimately responsible for the brain’s learning and adaptation mechanisms) can be altered in relation to information processing, decision-making, and emotions [19]. Various factors, including media, education, social culture and economics, environment, experience, age, and others, all impact an individual’s level of knowledge. Fifty percent of what we learn will stick in our memory if we hear and see it, compared to only 10% if we read it. The utilization of multiple health education media types can enhance the quality of learning outcomes [20].
When individuals receive education through media or other tools, they become aware of stimuli, which piques their curiosity to observe and learn from the material in the educational media [21]. Animaker, a type of educational media, is limited to text and only stimulates one sense (the sense of sight), whereas video and AR media can simultaneously stimulate two senses (the senses of hearing and sight), making it easier to retain information—about half of what is learned [22]. Due to the respondents’ interest in and awareness of non-ulcer foot care as a means of preventing diabetic ulcers, there was a change in knowledge across all three groups. It is easier for respondents to understand the information provided, and their interest and awareness increase when education is delivered through video/AR media [23], which contains moving images illustrating foot care steps, compared to Animaker, which consists of written content about foot care steps and is presented to respondents three times directly. Respondents were also provided with video/AR on CDs, which had a significant impact and allowed for independent study in addition to face-to-face instruction.
As a result of respondents’ distaste for the Animaker media, which featured articles detailing steps for taking care of their feet along with multiple images, the change in their knowledge of non-ulcer foot care was less pronounced in the positive control group 2. This may be due to the aging demographic of the respondents, which makes it challenging for them to comprehend information presented solely through visual stimulation (a few pictures and some writing) [24]. All other factors were equal, most only completed high school. The knowledge shift among the respondents was greater when compared with the benefits of foot care education provided by the AR+Animaker combination media.
Prior to receiving education through Animaker media, the non-ulcer foot care attitude of positive control group 2 was primarily in the negative attitude category. However, following education through Animaker media, the non-ulcer foot care attitude shifted to half being in the positive attitude category. Before receiving education through AR media, half of the positive control group 1’s attitude toward caring for non-ulcer feet fell into the negative attitude category. However, following education through AR media, the majority of the group’s attitude toward caring for non-ulcer feet shifted to the positive attitude category. The intervention group’s non-ulcer foot care attitude was primarily in the positive attitude category prior to receiving education through AR+Animaker media. However, following education through AR+Animaker media, the non-ulcer foot care attitude nearly completely transitioned to the positive attitude category. After receiving the educational intervention on foot care, the attitudes of the three groups differed significantly, as indicated by the results of the Wilcoxon test.
Animaker media is effective in improving attitudes toward self-medication in accordance with the rules, while research by Animaker media researchers is effective in enhancing attitudes regarding non-ulcer foot care in people with T2DM. A person’s attitude is constructed from three basic components: cognitive, affective, and conative [25]. The cognitive component represents trust and confidence in a particular object. The affective component reflects feelings and subjective emotional conditions toward certain objects. This emotional response can lead a person to maintain their attitude, even if that attitude is not necessarily positive. Meanwhile, the conative component refers more to the tendency of a person’s actions and behaviors toward an object [25]. This framework provides an overview and reasons why some respondents have negative attitudes while others have positive attitudes [26]. Family support or the influence of other individuals who are considered important also strengthens changes in the sufferer’s attitude [27].
An attitude is a conditioned response to a stimulus that considers relevant attention, feelings, opinions, and emotions [28]. Therefore, attitude can be defined as an extension of previously acquired knowledge, which itself originates from stimuli in the form of previously provided information [26]. Respondents had the opportunity to receive and comment on the foot care education they received through three rounds of AR and Animaker media. Because there is a window of time, during which they can decide which attitude is best for their health, individuals are more likely to accept the various inputs they receive. The respondents’ desire to improve their health status and their education through the use of Animaker media, which provided explanations and illustrated how to care for one’s feet through pictures, contributed to the change in attitude that occurred in all three groups. Education through the use of AR and video content that explains concepts and demonstrates how to care for one’s feet can have a direct impact on respondents’ actions [29]. Adding explanations and visuals to the Animaker combination can enhance learning through video and AR.
A change in attitude occurred in all three groups, partly due to the respondents’ desire to use Animaker media to improve their education and health status. Animaker media provided explanations and images of how to take care of one’s feet. The actions of respondents may be directly influenced by the education provided through AR and video content that clarifies concepts and demonstrates how viewers should care for their feet [28]. AR and video learning can be enhanced by incorporating explanations and images into the Animaker combination.
Before receiving education via AR media, Animaker, and a combination of the two, the three groups’ levels of non-ulcer foot care behaviors were primarily in the poor category; however, after the intervention, the levels of non-ulcer foot care behaviors were primarily in the good category. The Wilcoxon test results for the three groups indicated notable variations between the behaviors observed prior to and following the intervention. Audiovisual media are useful tools when it comes to helping people with T2DM achieve ulcer-free feet [30]. After receiving education, a person’s knowledge and attitudes can also change, and this process of changing behaviors follows; however, one can act or behave differently without first understanding the significance of the stimuli to which they are exposed [31]. Predisposing factors, such as views, values, and motivations to act, supporting factors, such as the availability of health facilities, and driving factors, such as the attitudes and behaviors of health professionals, families, or other officials who serve as role models for community behavior, as well as the health information they receive—including the media they consume—all influence an individual’s behavior [32].
The information media used, namely Animaker, influenced changes in action, as it contains explanations and pictures of how to carry out non-ulcer foot care, which can serve as examples for respondents. Video and AR are more memorable because respondents not only see but also hear the information conveyed, and include moving images that are easier for respondents to understand and imitate [33]. Education provided through video/AR media, which features moving images about foot care steps and is complemented by sound, can stimulate the senses of sight and hearing, leading to better retention of information by respondents, specifically 50% [34]. The combination of Animaker media can positively influence changes in actions, serving as a complement for respondents who may be reluctant to turn on the video player. In this way, respondents will better understand and be more diligent in carrying out foot care actions because they have clear examples of the actions to be taken.
One of the limitations of the study was the possibility that differences in cultural beliefs or demographic characteristics (such as age, education level, and socioeconomic status) may impact how participants perceive and engage with the interventions, thereby affecting the study’s overall findings. It is necessary to conduct similar research using more precise measurements, such as direct observation of non-ulcer foot care behavior in an effort to prevent diabetic ulcers in patients with T2DM. Additionally, it is important to examine factors that influence knowledge, such as sociocultural, economic, and experiential factors, factors that influence attitudes, such as social interactions and personal experiences, and factors that influence behaviors, such as family support and health facilities.
Conclusion
The use of AR media, Animaker, or a combination of both increases knowledge, attitudes, and behavior in education about treating diabetic foot ulcers for prevention.
Acknowledgments: Gratitude is extended to Universitas Airlangga in Surabaya and Universitas Lambung Mangkurat in Banjarmasin, as well as the Directorate of Technology Research of the Republic of Indonesia (DRTPM), for their unwavering support throughout this study.
Ethical Permissions: The procedure was reviewed and granted ethical clearance (Number: 0819-KEPK) by the Health Research Ethics Commission of the Regional Representative Council of the Indonesian National Nurses Association (INNA), Banjarbaru, Indonesia.
Conflicts of Interests: The authors reported no conflicts of interests.
Authors' Contribution: Negara CK (First Author), Introduction Writer/Discussion Writer/Main Researcher (20%); Sukartini T (Second Author), Assistant Researcher/Statistical Analyst (20%); Dewi YS (Third Author), Assistant Researcher/Results Writer (20%); Nursalam N (Fourth Author), Assistant Researcher/Methodologist (20%); Yunara Y (Fifth Author), Assistant Researcher/Discussion Writer (20%)
Funding/Support: This research was funded by the Directorate General of Higher Education, Ministry of Education and Culture of the Republic of Indonesia (DRTPM) in 2024, under the doctoral dissertation research scheme.
Full-Text: (176 Views)
Introduction
Diabetic ulcers are chronic, open wounds that penetrate through the skin’s outer layer into the deeper dermal tissue, predominantly affecting individuals with diabetes mellitus (DM). These ulcers represent a significant health concern due to their complexity and the extensive resources required for treatment [1]. Managing diabetic ulcers involves considerable financial and time investments, and these complications are among the most feared by patients with DM because of their potential to lead to severe outcomes such as amputation [2, 3]. Amputation not only exacerbates physical disabilities but also profoundly impacts a patient’s quality of life, leading to increased psychological distress and reduced functional independence [3].
Globally, diabetes is a burgeoning epidemic, with the International Diabetes Federation (IDF) estimating that over 371 million individuals will be affected by diabetes by 2023 [4]. In Indonesia, the prevalence of DM has risen from 1.1% in 2021 to 2.1% in 2022, underscoring a growing public health challenge [5]. This increase in prevalence highlights the importance of addressing risk factors associated with diabetic ulcers, such as vascular disease, neuropathy, and other diabetes-related complications.
Several factors contribute to the development of diabetic ulcers. Risk factors include the presence of foot deformities, calluses, visual impairments, age-related changes, and poor glycemic control. Additionally, individuals with a history of foot wounds or decreased sensation in the feet are particularly vulnerable [6]. Hyperglycemia, a hallmark of diabetes, leads to neuropathy and diminished sensation, which impairs the ability to detect injuries and results in altered pressure distribution on the feet, facilitating ulcer formation [7, 8]. The compromised immune response associated with hyperglycemia also increases susceptibility to infections, potentially leading to severe complications, such as gangrene if not managed appropriately [9, 10].
Preventing and managing diabetic ulcers requires a multifaceted approach, including regular assessment of vascular and circulatory health, stringent glucose control, and patient education on foot care [11]. Effective foot care aims to minimize the risk of complications and potential amputations by encouraging proactive management and regular monitoring of foot health [12]. Educational interventions play a crucial role in empowering patients to take charge of their foot health, thereby reducing the incidence of foot complications and improving overall outcomes [13].
Recent advances in technology offer innovative solutions for enhancing patient education. Augmented reality (AR) has emerged as a promising tool in this domain, demonstrating increased patient satisfaction and knowledge retention compared to traditional methods [14-16]. For instance, AR applications, like Animaker use interactive graphics and sound to convey essential foot care information, providing a more engaging and effective learning experience than conventional text-based materials. By integrating AR technology into educational programs, we can potentially improve patient outcomes by fostering a better understanding and adherence to foot care practices.
This study aimed to explore the impact of AR media, specifically an Animaker video, on non-ulcer foot care behaviors among individuals with type 2 diabetes mellitus (T2DM). By comparing AR-based educational interventions with traditional methods, we aimed to determine the effectiveness of AR in enhancing foot care practices and reducing the risk of diabetic ulcers.
Diabetic ulcers are chronic, open wounds that penetrate through the skin’s outer layer into the deeper dermal tissue, predominantly affecting individuals with diabetes mellitus (DM). These ulcers represent a significant health concern due to their complexity and the extensive resources required for treatment [1]. Managing diabetic ulcers involves considerable financial and time investments, and these complications are among the most feared by patients with DM because of their potential to lead to severe outcomes such as amputation [2, 3]. Amputation not only exacerbates physical disabilities but also profoundly impacts a patient’s quality of life, leading to increased psychological distress and reduced functional independence [3].
Globally, diabetes is a burgeoning epidemic, with the International Diabetes Federation (IDF) estimating that over 371 million individuals will be affected by diabetes by 2023 [4]. In Indonesia, the prevalence of DM has risen from 1.1% in 2021 to 2.1% in 2022, underscoring a growing public health challenge [5]. This increase in prevalence highlights the importance of addressing risk factors associated with diabetic ulcers, such as vascular disease, neuropathy, and other diabetes-related complications.
Several factors contribute to the development of diabetic ulcers. Risk factors include the presence of foot deformities, calluses, visual impairments, age-related changes, and poor glycemic control. Additionally, individuals with a history of foot wounds or decreased sensation in the feet are particularly vulnerable [6]. Hyperglycemia, a hallmark of diabetes, leads to neuropathy and diminished sensation, which impairs the ability to detect injuries and results in altered pressure distribution on the feet, facilitating ulcer formation [7, 8]. The compromised immune response associated with hyperglycemia also increases susceptibility to infections, potentially leading to severe complications, such as gangrene if not managed appropriately [9, 10].
Preventing and managing diabetic ulcers requires a multifaceted approach, including regular assessment of vascular and circulatory health, stringent glucose control, and patient education on foot care [11]. Effective foot care aims to minimize the risk of complications and potential amputations by encouraging proactive management and regular monitoring of foot health [12]. Educational interventions play a crucial role in empowering patients to take charge of their foot health, thereby reducing the incidence of foot complications and improving overall outcomes [13].
Recent advances in technology offer innovative solutions for enhancing patient education. Augmented reality (AR) has emerged as a promising tool in this domain, demonstrating increased patient satisfaction and knowledge retention compared to traditional methods [14-16]. For instance, AR applications, like Animaker use interactive graphics and sound to convey essential foot care information, providing a more engaging and effective learning experience than conventional text-based materials. By integrating AR technology into educational programs, we can potentially improve patient outcomes by fostering a better understanding and adherence to foot care practices.
This study aimed to explore the impact of AR media, specifically an Animaker video, on non-ulcer foot care behaviors among individuals with type 2 diabetes mellitus (T2DM). By comparing AR-based educational interventions with traditional methods, we aimed to determine the effectiveness of AR in enhancing foot care practices and reducing the risk of diabetic ulcers.
Materials and Methods
Design
This quasi-experimental study employed a pre-test-post-test design with a control group and was conducted in Banjarmasin City from January through June 2023.
Inclusion and exclusion criteria
Inclusion criteria were patients aged 18 and older with a confirmed diagnosis of T2DM, willingness to provide informed consent to participate in the study, ability to understand and engage with educational materials, access to smartphones, tablets, or computers to engage with Animaker and AR interventions, and no previous formal education on non-ulcer foot care within the past year. Exclusion criteria included patients with acute diabetic complications (e.g., diabetic ketoacidosis and severe infections) that may interfere with participation, patients with cognitive impairments or conditions affecting their ability to engage with educational content, individuals with serious comorbidities, patients who have participated in similar educational programs within the last year, and patients who do not speak the language of the educational materials and cannot communicate effectively with researchers.
Sample size and groups
To account for potential dropouts, the sample size was increased by 10% for each group based on the Lameshow formula, resulting in a total sample size of 44 respondents for each group, including the intervention group (AR+Animaker), positive control group 1 (AR), and positive control group 2 (Animaker). Purposive sampling was used to select the respondents for each group. No respondents withdrew from the study.
Intervention
The intervention involved providing animation-based videos and patterned images that support AR; the AR images were displayed using an Android camera, which then made the AR images appear to move and come to life. The intervention was carried out for 7-10 minutes a day, three times a week for three months.
Data collection
The tools used included an action observation sheet adapted from the Patient Interpretation of Neuropathy (PIN) Questionnaire, and a questionnaire on demographic information, knowledge, and attitudes regarding neuropathy.
Data analysis
The collected data were analyzed by SPSS 29 using the Wilcoxon signed-rank and Kruskal-Wallis tests at a significance level of p≤0.05.
Findings
The three age groups were homogenous as the majority of respondents were middle-aged (45-59 years old), predominantly female, and had a senior high school education (Table 1).
Table 1. Frequency of participants’ demographic characteristics (n=132)
The post-test knowledge scores increased in the intervention group (from 20.45% to 61.36%), positive control group 1 (from 18.18% to 52.27%), and positive control group 2 (from 25% to 56.82%). Meanwhile, the post-test attitude scores increased significantly in the intervention group (from 31.82% to 72.73%), positive control group 1 (from 45.45% to 65.91%), and positive control group 2 (from 36.36% to 70.45%). Also, the post-test behavior scores were assessed as good in all three groups and increased in the intervention group (from 27.27% to 61.36%), positive control group 1 (from 15.91% to 54.55%), and positive control group 2 (from 22.73% to 59.09%; Table 2).
Table 2. Frequency of the knowledge, attitude, and behavior pre- and post-test scores
According to the Wilcoxon signed-rank test, foot care education using the combined media of AR+Animaker (p=0.005) and AR (p=0.011) had an impact on patients’ knowledge of non-ulcer foot care in individuals with T2DM; however, no discernible impact of Animaker media education was observed (p=0.097). In addition, the Kruskal-Wallis test showed a significant difference in knowledge among the three groups after receiving non-ulcer foot care education through the AR+Animaker, AR, and Animaker in T2DM sufferers (p=0.047).
On the other hand, the Wilcoxon signed-rank test revealed that the attitudes of type 2 diabetic patients toward non-ulcer foot care were influenced by the foot care education provided through the combined media of AR+Animaker, AR, and Animaker (p=0.005). Also, according to the Kruskal-Wallis test, there was a significant difference in attitudes among the three groups after receiving non-ulcer foot care education through the AR+Animaker, AR, and Animaker (p=0.022)
According to the Wilcoxon signed-rank test, foot care education significantly affected behavior in all groups. Also, according to the Kruskal-Wallis test, a significant difference was found in behavior among the three groups following non-ulcer foot care education through the AR+Animaker, AR, and Animaker (p=0.037; Table 3).
Table 3. Bivariate test of measurement pre- and post-test
Discussion
This research aimed to discover how augmented reality media and Animaker affect non-ulcer foot care behavior among people with type 2 diabetes, specifically regarding foot care education. The results indicated that the level of knowledge about non-ulcer foot care in the positive control group 2 at the beginning of the measurement was predominantly in the poor category; however, after receiving education through Animaker media, most participants moved to the good category. The results of the Wilcoxon signed-rank test showed no significant difference between knowledge levels before and after education through Animaker media. In positive control group 1, the level of knowledge about non-ulcer foot care before receiving education through AR media was primarily in the poor category; after the education, most participants were in the good category. Similarly, the level of knowledge about non-ulcer foot care in the treatment group before receiving education through AR+Animaker media was mostly in the poor category, whereas after the education, almost all participants were in the good category. The results of the Wilcoxon test for knowledge in the positive control group 1 and the treatment group showed that there was a significant difference between knowledge before and after the intervention. Prior to receiving education through AR+Animaker media, the majority of the treatment group’s knowledge regarding non-ulcer foot care fell into the poor category; however, following education through AR+Animaker media, nearly all of them moved into the good category. The knowledge obtained from the Wilcoxon test in both the treatment group and the positive control group 1 demonstrated a significant difference between their pre- and post-intervention knowledge.
When used in conjunction with audio-visual materials, Animaker media can raise the knowledge scores of individuals with T2DM regarding non-ulcer foot care [17]. The application of AR improved patient satisfaction and knowledge retention. Additionally, video media enhances the understanding of women of childbearing age about early cervical cancer detection in various circumstances [18]. One of the key factors in determining how someone acts is their knowledge. Knowledge is gained after an individual perceives a specific object. The goal of the learning process is to equip patients with knowledge so that cognitive control (which is ultimately responsible for the brain’s learning and adaptation mechanisms) can be altered in relation to information processing, decision-making, and emotions [19]. Various factors, including media, education, social culture and economics, environment, experience, age, and others, all impact an individual’s level of knowledge. Fifty percent of what we learn will stick in our memory if we hear and see it, compared to only 10% if we read it. The utilization of multiple health education media types can enhance the quality of learning outcomes [20].
When individuals receive education through media or other tools, they become aware of stimuli, which piques their curiosity to observe and learn from the material in the educational media [21]. Animaker, a type of educational media, is limited to text and only stimulates one sense (the sense of sight), whereas video and AR media can simultaneously stimulate two senses (the senses of hearing and sight), making it easier to retain information—about half of what is learned [22]. Due to the respondents’ interest in and awareness of non-ulcer foot care as a means of preventing diabetic ulcers, there was a change in knowledge across all three groups. It is easier for respondents to understand the information provided, and their interest and awareness increase when education is delivered through video/AR media [23], which contains moving images illustrating foot care steps, compared to Animaker, which consists of written content about foot care steps and is presented to respondents three times directly. Respondents were also provided with video/AR on CDs, which had a significant impact and allowed for independent study in addition to face-to-face instruction.
As a result of respondents’ distaste for the Animaker media, which featured articles detailing steps for taking care of their feet along with multiple images, the change in their knowledge of non-ulcer foot care was less pronounced in the positive control group 2. This may be due to the aging demographic of the respondents, which makes it challenging for them to comprehend information presented solely through visual stimulation (a few pictures and some writing) [24]. All other factors were equal, most only completed high school. The knowledge shift among the respondents was greater when compared with the benefits of foot care education provided by the AR+Animaker combination media.
Prior to receiving education through Animaker media, the non-ulcer foot care attitude of positive control group 2 was primarily in the negative attitude category. However, following education through Animaker media, the non-ulcer foot care attitude shifted to half being in the positive attitude category. Before receiving education through AR media, half of the positive control group 1’s attitude toward caring for non-ulcer feet fell into the negative attitude category. However, following education through AR media, the majority of the group’s attitude toward caring for non-ulcer feet shifted to the positive attitude category. The intervention group’s non-ulcer foot care attitude was primarily in the positive attitude category prior to receiving education through AR+Animaker media. However, following education through AR+Animaker media, the non-ulcer foot care attitude nearly completely transitioned to the positive attitude category. After receiving the educational intervention on foot care, the attitudes of the three groups differed significantly, as indicated by the results of the Wilcoxon test.
Animaker media is effective in improving attitudes toward self-medication in accordance with the rules, while research by Animaker media researchers is effective in enhancing attitudes regarding non-ulcer foot care in people with T2DM. A person’s attitude is constructed from three basic components: cognitive, affective, and conative [25]. The cognitive component represents trust and confidence in a particular object. The affective component reflects feelings and subjective emotional conditions toward certain objects. This emotional response can lead a person to maintain their attitude, even if that attitude is not necessarily positive. Meanwhile, the conative component refers more to the tendency of a person’s actions and behaviors toward an object [25]. This framework provides an overview and reasons why some respondents have negative attitudes while others have positive attitudes [26]. Family support or the influence of other individuals who are considered important also strengthens changes in the sufferer’s attitude [27].
An attitude is a conditioned response to a stimulus that considers relevant attention, feelings, opinions, and emotions [28]. Therefore, attitude can be defined as an extension of previously acquired knowledge, which itself originates from stimuli in the form of previously provided information [26]. Respondents had the opportunity to receive and comment on the foot care education they received through three rounds of AR and Animaker media. Because there is a window of time, during which they can decide which attitude is best for their health, individuals are more likely to accept the various inputs they receive. The respondents’ desire to improve their health status and their education through the use of Animaker media, which provided explanations and illustrated how to care for one’s feet through pictures, contributed to the change in attitude that occurred in all three groups. Education through the use of AR and video content that explains concepts and demonstrates how to care for one’s feet can have a direct impact on respondents’ actions [29]. Adding explanations and visuals to the Animaker combination can enhance learning through video and AR.
A change in attitude occurred in all three groups, partly due to the respondents’ desire to use Animaker media to improve their education and health status. Animaker media provided explanations and images of how to take care of one’s feet. The actions of respondents may be directly influenced by the education provided through AR and video content that clarifies concepts and demonstrates how viewers should care for their feet [28]. AR and video learning can be enhanced by incorporating explanations and images into the Animaker combination.
Before receiving education via AR media, Animaker, and a combination of the two, the three groups’ levels of non-ulcer foot care behaviors were primarily in the poor category; however, after the intervention, the levels of non-ulcer foot care behaviors were primarily in the good category. The Wilcoxon test results for the three groups indicated notable variations between the behaviors observed prior to and following the intervention. Audiovisual media are useful tools when it comes to helping people with T2DM achieve ulcer-free feet [30]. After receiving education, a person’s knowledge and attitudes can also change, and this process of changing behaviors follows; however, one can act or behave differently without first understanding the significance of the stimuli to which they are exposed [31]. Predisposing factors, such as views, values, and motivations to act, supporting factors, such as the availability of health facilities, and driving factors, such as the attitudes and behaviors of health professionals, families, or other officials who serve as role models for community behavior, as well as the health information they receive—including the media they consume—all influence an individual’s behavior [32].
The information media used, namely Animaker, influenced changes in action, as it contains explanations and pictures of how to carry out non-ulcer foot care, which can serve as examples for respondents. Video and AR are more memorable because respondents not only see but also hear the information conveyed, and include moving images that are easier for respondents to understand and imitate [33]. Education provided through video/AR media, which features moving images about foot care steps and is complemented by sound, can stimulate the senses of sight and hearing, leading to better retention of information by respondents, specifically 50% [34]. The combination of Animaker media can positively influence changes in actions, serving as a complement for respondents who may be reluctant to turn on the video player. In this way, respondents will better understand and be more diligent in carrying out foot care actions because they have clear examples of the actions to be taken.
One of the limitations of the study was the possibility that differences in cultural beliefs or demographic characteristics (such as age, education level, and socioeconomic status) may impact how participants perceive and engage with the interventions, thereby affecting the study’s overall findings. It is necessary to conduct similar research using more precise measurements, such as direct observation of non-ulcer foot care behavior in an effort to prevent diabetic ulcers in patients with T2DM. Additionally, it is important to examine factors that influence knowledge, such as sociocultural, economic, and experiential factors, factors that influence attitudes, such as social interactions and personal experiences, and factors that influence behaviors, such as family support and health facilities.
Conclusion
The use of AR media, Animaker, or a combination of both increases knowledge, attitudes, and behavior in education about treating diabetic foot ulcers for prevention.
Acknowledgments: Gratitude is extended to Universitas Airlangga in Surabaya and Universitas Lambung Mangkurat in Banjarmasin, as well as the Directorate of Technology Research of the Republic of Indonesia (DRTPM), for their unwavering support throughout this study.
Ethical Permissions: The procedure was reviewed and granted ethical clearance (Number: 0819-KEPK) by the Health Research Ethics Commission of the Regional Representative Council of the Indonesian National Nurses Association (INNA), Banjarbaru, Indonesia.
Conflicts of Interests: The authors reported no conflicts of interests.
Authors' Contribution: Negara CK (First Author), Introduction Writer/Discussion Writer/Main Researcher (20%); Sukartini T (Second Author), Assistant Researcher/Statistical Analyst (20%); Dewi YS (Third Author), Assistant Researcher/Results Writer (20%); Nursalam N (Fourth Author), Assistant Researcher/Methodologist (20%); Yunara Y (Fifth Author), Assistant Researcher/Discussion Writer (20%)
Funding/Support: This research was funded by the Directorate General of Higher Education, Ministry of Education and Culture of the Republic of Indonesia (DRTPM) in 2024, under the doctoral dissertation research scheme.
Article Type: Original Research |
Subject:
Health Education and Health Behavior
Received: 2024/07/7 | Accepted: 2024/08/18 | Published: 2024/09/11
Received: 2024/07/7 | Accepted: 2024/08/18 | Published: 2024/09/11
References
1. Harreiter J, Roden M. Diabetes mellitus: Definition, classification, diagnosis, screening and prevention (update 2023). Wiener Klinische Wochenschrift. 2023;135(Suppl 1):7-17. [German] [Link] [DOI:10.1007/s00508-022-02122-y]
2. Fan W, Pang H, Xie Z, Huang G, Zhou Z. Circular RNAs in diabetes mellitus and its complications. Front Endocrinol. 2022;13:885650. [Link] [DOI:10.3389/fendo.2022.885650]
3. Chowdhury TA. Post-transplant diabetes mellitus. Clin Med. 2019;19(5):392-5. [Link] [DOI:10.7861/clinmed.2019-0195]
4. Webber S. International diabetes federation. Diabetes Res Clin Pract. 2013;102:147-8. [Link] [DOI:10.1016/j.diabres.2013.10.013]
5. Ministry of Health Indonesia. Prevalence, impact, and hypertension & diabetes prevention in Indonesia. Jakarta: Indonesia Health Survey; 2023. [Indonesian] [Link]
6. Popoviciu MS, Paduraru L, Nutas RM, Ujoc AM, Yahya G, Metwally K, et al. Diabetes mellitus secondary to endocrine diseases: An update of diagnostic and treatment particularities. Int J Mol Sci. 2023;24(16):12676. [Link] [DOI:10.3390/ijms241612676]
7. Monteiro-Soares M, Boyko EJ, Jeffcoate W, Mills JL, Russell D, Morbach S, et al. Diabetic foot ulcer classifications: A critical review. Diabetes Metab Res Rev. 2020;36(Suppl 1):e3272. [Link] [DOI:10.1002/dmrr.3272]
8. Rai V, Moellmer R, Agrawal DK. Clinically relevant experimental rodent models of diabetic foot ulcer. Mol Cell Biochem. 2022;477(4):1239-47. [Link] [DOI:10.1007/s11010-022-04372-w]
9. McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2023;46(1):209-21. [Link] [DOI:10.2337/dci22-0043]
10. Alsabek MB, Abdul Aziz AR. Diabetic foot ulcer, the effect of resource-poor environments on healing time and direct cost: A cohort study during Syrian crisis. Int Wound J. 2022;19(3):531-7. [Link] [DOI:10.1111/iwj.13651]
11. Jiang P, Li Q, Luo Y, Luo F, Che Q, Lu Z, et al. Current status and progress in research on dressing management for diabetic foot ulcer. Front Endocrinol. 2023;14:1221705. [Link] [DOI:10.3389/fendo.2023.1221705]
12. Huang H, Xin R, Li X, Zhang X, Chen Z, Zhu Q, et al. Physical therapy in diabetic foot ulcer: Research progress and clinical application. Int Wound J. 2023;20(8):3417-34. [Link] [DOI:10.1111/iwj.14196]
13. Ramachandran V, Mohanasundaram T, Karunakaran D, Gunasekaran M, Tiwari R. Physiological and pathophysiological aspects of diabetic foot ulcer and its treatment strategies. Curr Diabetes Rev. 2023;19(8):e031122210617. [Link] [DOI:10.2174/1573399819666221103141715]
14. Urlings J, Sezer S, Ter Laan M, Bartels R, Maal T, Boogaarts J, et al. The role and effectiveness of augmented reality in patient education: A systematic review of the literature. Patient Educ Couns. 2022;105(7):1917-27. [Link] [DOI:10.1016/j.pec.2022.03.005]
15. Vaughan N. Virtual reality meets diabetes. J Diabetes Sci Technol. 2024;19322968231222022. [Link] [DOI:10.1177/19322968231222022]
16. Yeung AWK, Tosevska A, Klager E, Eibensteiner F, Laxar D, Stoyanov J, et al. Virtual and augmented reality applications in medicine: Analysis of the scientific literature. J Med Internet Res. 2021;23(2):e25499. [Link] [DOI:10.2196/25499]
17. Christova M, Strohmaier R, Fuchs-Neuhold B, Guggenberger B, Loder-Fink B, Draxler T, et al. Mixed reality prototype of multimodal screening for early detection of cognitive impairments in older adults: Protocol development and usability study. JMIR Res Protoc. 2022;11(10):e39513. [Link] [DOI:10.2196/39513]
18. Taha BA, Addie AJ, Kadhim AC, Azzahran AS, Haider AJ, Chaudhary V, et al. Photonics-powered augmented reality skin electronics for proactive healthcare: Multifaceted opportunities. Mikrochim Acta. 2024;191(5):250. [Link] [DOI:10.1007/s00604-024-06314-3]
19. Menon JC, John D, Sreedevi A, Janakiram C, Akshaya R, Sumithra S, et al. Improving medication adherence among persons with cardiovascular disease through m-health and community health worker-led interventions in Kerala; Protocol for a type II effectiveness-implementation research-(SHRADDHA-ENDIRA). Trials. 2024;25(1):437. [Link] [DOI:10.1186/s13063-024-08244-0]
20. Negara C, Sukartini T, Setiya D, Nursalam N. Effectiveness of diabetes self-management education on non-ulcer diabetic foot incidents. Health Educ Health Promot. 2024;12(1):53-8. [Link]
21. Field HT, Woodier N, Clayton J, Plichta P, Teo KS. Use of an educational, audiovisual podcast to maximise safety with variable rate intravenous insulin infusions. BMJ Open Qual. 2018;7(2):e000111. [Link] [DOI:10.1136/bmjoq-2017-000111]
22. Iskander M, Ogunsola T, Ramachandran R, McGowan R, Al-Aswad LA. Virtual reality and augmented reality in ophthalmology: A contemporary prospective. Asia Pac J Ophthalmol. 2021;10(3):244-52. [Link] [DOI:10.1097/APO.0000000000000409]
23. Tourkmani AM, Alharbi TJ, Bin Rsheed AM, Alotaibi AF, Aleissa MS, Alotaibi S, et al. A hybrid model of in-person and telemedicine diabetes education and care for management of patients with uncontrolled type 2 diabetes mellitus: Findings and implications from a multicenter prospective study. Telemed Rep. 2024;5(1):46-57. [Link] [DOI:10.1089/tmr.2024.0003]
24. Krenn C, Semlitsch T, Zipp C, Lengauer S, Shao L, Schreck T, et al. Customization options in consumer health information materials on type-2 diabetes mellitus-an analysis of modifiable features in different types of media. Front Public Health. 2024;12:1252244. [Link] [DOI:10.3389/fpubh.2024.1252244]
25. Li X, Shi Y, Wei D, Gong Y, Yan X, Cai S. Knowledge, attitude, and practice toward weight management among diabetic patients in Qidong City, Jiangsu Province. BMC Public Health. 2024;24(1):922. [Link] [DOI:10.1186/s12889-024-18392-2]
26. Bekele NT, Habtewold EM, Deybasso HA, Mekuria Negussie Y. Poor self-care practices and contributing factors among adults with type 2 diabetes in Adama, Ethiopia. Sci Rep. 2024;14(1):13660. [Link] [DOI:10.1038/s41598-024-63524-8]
27. Zhang ZC, Du QH, Jia HH, Li YM, Liu YQ, Li SB. A qualitative study on inner experience of self-management behavior among elderly patients with type 2 diabetes in rural areas. BMC Public Health. 2024;24(1):1456. [Link] [DOI:10.1186/s12889-024-18994-w]
28. Rahbar S, Zarifsanaiey N, Mehrabi M. The effectiveness of social media-based microlearning in improving knowledge, self-efficacy, and self-care behaviors among adult patients with type 2 diabetes: An educational intervention. BMC Endocr Disord. 2024;24(1):99. [Link] [DOI:10.1186/s12902-024-01626-0]
29. Zhu D, Zhu B, Zhao J, Zhang C, He J, Song D, et al. Investigation on the effectiveness of augmented reality memory training game for Chinese older adults: A randomized controlled trial. Games Health J. 2024;13(1):5-12. [Link] [DOI:10.1089/g4h.2022.0183]
30. Saeed R, Ahmed F, Danish SH, Talha M, Usmani M, Durrani N, et al. Video based educational intervention in waiting area to improve awareness about health screening among patients visiting family medicine clinics. BMC Health Serv Res. 2024;24(1):818. [Link] [DOI:10.1186/s12913-024-11143-4]
31. Motamed-Jahromi M, Kaveh MH, Vitale E. Mindfulness and self-regulation intervention for improved self-neglect and self-regulation in diabetic older adults. Sci Rep. 2024;14(1):13857. [Link] [DOI:10.1038/s41598-024-64314-y]
32. Jafari A, Naddafi F, Gholian‑Aval M, Tehrani H. Relationship between diabetes health literacy, distress, burnout, social support, complications, self-care behaviors, and quality of life among patients with type 2 diabetes: A path analysis study. Diabetol Metab Syndr. 2024;16(1):150. [Link] [DOI:10.1186/s13098-024-01391-z]
33. Mamone V, Fonzo MD, Esposito N, Ferrari M, Ferrari V. Monitoring wound healing with contactless measurements and augmented reality. IEEE J Transl Eng Health Med. 2020;8:2700412. [Link] [DOI:10.1109/JTEHM.2020.2983156]
34. Benčurik V, Skrovina M, Martínek L, Bartoš J, Macháčková M, Dosoudil M, et al. Fluorescent angiography in colorectal surgery, the influence of augmented reality in the operating room on the anastomotic leakage after low rectal resection. Rozhl Chir. 2021;100(11):543-51. [Link] [DOI:10.33699/PIS.2021.100.11.543-551]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |