



Volume 11, Issue 5 (2023)
Health Educ Health Promot 2023, 11(5): 723-731 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Omid M, Aminshokravi F, Zarei F. Impact of a Blended Educational Intervention on COVID-19 Preventive Behavior in Teachers. Health Educ Health Promot 2023; 11 (5) :723-731
URL: http://hehp.modares.ac.ir/article-5-73501-en.html
URL: http://hehp.modares.ac.ir/article-5-73501-en.html
1- Department of Health Education & Health Promotion, Faculty of Medical Sciences, Tarbiat Modares University (TMU), Tehran, Iran
Keywords: Educational Intervention [MeSH], COVID-19 [MeSH], Health Belief Model [MeSH], Risk Reduction Behavior [MeSH]
Full-Text [PDF 692 kb]
(2994 Downloads)
| Abstract (HTML) (678 Views)
Full-Text: (134 Views)
Introduction
Since its emergence in December 2019, Coronavirus disease (COVID-19) has spread globally and become a global concern. COVID-19, which is spread by droplets and direct contact from human to human and is known to cause emergent respiratory infections and ranges from colds to acute severe respiratory syndrome, has imposed a global burden on health and the economy that has never been seen before. It has resulted in more than 1.4 million deaths in 220 countries or territories as of November 29, 2020 [1]. While it appears that the whole world is looking forward to the arrival of safe behavior, the adherence to COVID-19 prevention by the general public remains uncertain [2].
In the Eastern Mediterranean region, Iran has the highest incidence and mortality of COVID-19 [3-5]. On February 19, 2020, the first case of death from COVID-19 was reported in Iran, and the infection spread rapidly [6, 7]. As of January 26, 2020, 1,183,182 definite cases and 54,308 deaths due to COVID-19 have been reported in Iran [8]. The main ways of transmitting coronavirus are by inhaling the infected person’s respiratory droplets and being in close contact with the infected person or their secretions [9]. Even though several types of vaccines protect against COVID-19, the best way to avoid infection is to avoid exposure to this virus [10, 11]. Implementation of the community-based knowledge recommended by the World Health Organization (WHO) for prevention is crucial [12]. COVID-19 preventive behaviors include using a face mask, washing hands frequently with soap and water, covering the mouth and nose with a handkerchief when coughing and sneezing, avoiding touching eyes, mouth, and nose with a sitting hand, avoiding close contact with infected people, and maintaining social distance [11].
Undoubtedly, the COVID-19 epidemic has affected everyone, including teachers, and caused many challenges [13, 14]. In a study in the United States, teachers rated the negative impact of COVID-19 on themselves as moderate [15]. It is important to protect older teachers with an underlying illness because they are a high-risk group for COVID-19 [13, 15]. Teachers should be trained on how to deal with COVID-19 and properly implement health guidelines for the high incidence and mortality of COVID-19 in Iran and the lack of specific treatment. Primary prevention increases knowledge based on scientific evidence creates the proper attitude, and creates COVID-19 preventive behaviors among people, especially teachers. Therefore, considering teachers’ health because of their relationship with many students and having an effective role in them and their parents’ mindsets seems essential; The meaning of the phrase "prevention is better than cure" sheds light on the path.
The Health Belief Model (HBM) is a psychosocial model for behavioral change. It is more often used to describe the relationship between health beliefs and health behaviors. HBM assumes that individuals’ participation in prevention, early detection, and treatment measures for a specific health problem is depended on their perception that they are at risk of this condition, even if they do not exhibit symptoms (perceived susceptibility). They recognize that COVID-19 is a significant health problem with serious consequences (perceived severity); They believe in the benefits of suggested preventive measures (perceived benefits) and recognize that the benefits outweigh the common barriers associated with these measures (perceived barriers). Furthermore, they believe they have the motivation and ability to engage in a healthy lifestyle [16].
According to the above, teachers’ health beliefs, behaviors, and knowledge about preventive behaviors are important. Changing the health beliefs regarding the infectious disease epidemic may deeply root the importance of self-efficacy in healthy behavior regarding COVID-19. The educational intervention content leveled them up with the latest updates about COVID-19's way of transmission, signs and symptoms, and preventive behaviors.
Therefore, promoting preventive behavior-related COVID-19 with an appropriate educational method is important. Individual enabling factors such as level of literacy, socio-economic status, age, etc. as well as access-limiting situations such as the COVID-19 pandemic and lockdowns affect educational method selection. Furthermore, choosing the proper training method in line with using a fit change behavior conceptual framework is as important too. The present study was one of the first studies that approached behavior change in the early waves of the COVID-19 pandemic in Iran. Understanding the cognitive factors affecting corona-preventing behaviors in the early waves due to the high perceived fear and sensitivity in people required the design of a curriculum based on the theory and framework of behavior change. On the other hand, in terms of facilitating educational programs by providing training both in online and offline ways blended learning was designed. The current study aimed to investigate the effect of an educational intervention based on the HBM about COVID-19 on teachers' knowledge, health beliefs, and behaviors.
Materials and Methods
Study design
This randomized controlled trial was conducted on elementary school teachers of Karaj City, Iran, in 2021. Comprehensive sampling was followed to include all below 60 female teachers who were residents of Karaj, Alborz Province, Iran (140 teachers). The cluster sampling method was used for sampling. First, two districts were randomly selected from the four districts affiliated with the Karaj Education Organization (districts 3 and 4). Then, one of these two areas was assigned to the intervention group (district 3) and the other to the control group (area 4) by lottery method. Then, from each of these two districts, 12 primary schools were randomly selected by an externally trained researcher (Figure 1). Teachers from selected schools were invited to participate in this study, taking into account the inclusion and exclusion criteria, set by the teachers of these schools during a telephone or in-person call after a brief description of the subject of the study and its objectives. Written and online consent was obtained from them.
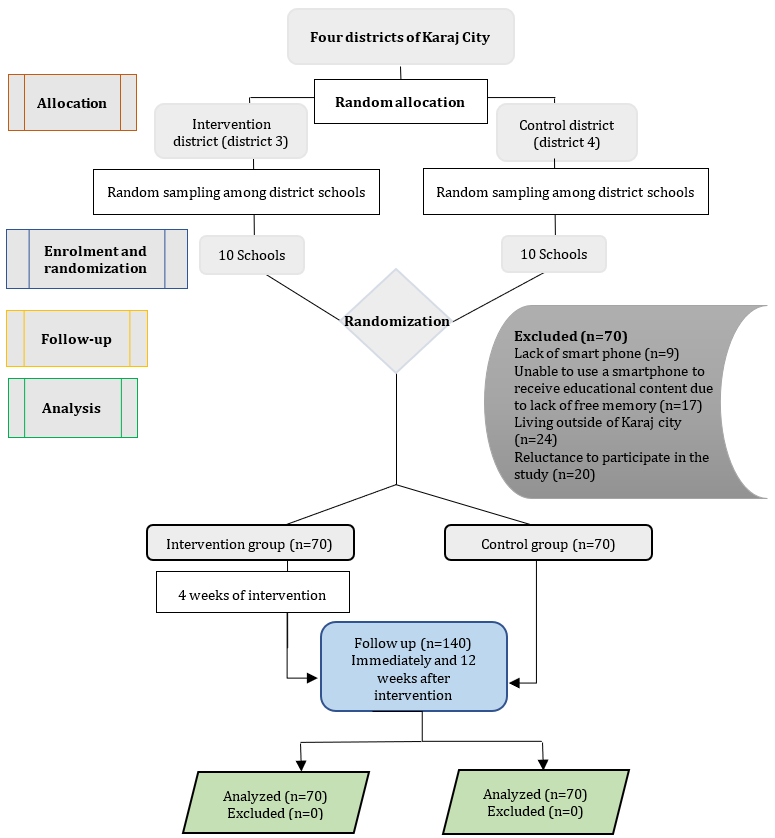
Figure 1. Consort diagram
Data collection tools
Data were collected using a validated questionnaire [17]. It has two sections: Part I: Socio-demographic data, designed to collect data such as age, educational level, residence, work experience, and history of COVID-19. Part II: Assessment of teacher’s knowledge regarding COVID-19: Researchers developed it after reviewing current literature. It included the COVID-19 definition, signs and symptoms, mode of transmission, and World Health Organization recommendations. Part III: Health belief model scale; To assess teacher’s beliefs regarding COVID-19. Researchers developed it after reviewing current literature to examine perceived susceptibility (8 items), perceived severity (5 items), perceived benefits (5 items), perceived barriers (6 items), cues to action (4 items) and self-efficacy (11 items). In each item, the teachers have to choose one of five alternatives: Strongly agree=5, agree=4, indifference=3, don't agree=2, and strongly don't agree=1. Part IV: Assessment of teachers’ behavior regarding COVID-19: Teachers’ likelihood to engage in healthy behaviors regarding COVID-19. In this item, the teachers have to choose one of five alternatives: Always=5, often=4, sometimes=3, rarely=2, and never=1. The researchers developed the instrument, and then it was tested for face, content, and construct validity by 15 experts in health education, health care providers, and nursing fields. Instrument reliability was conducted using Cronbach's Alpha coefficient test (r=0.78) and Intra-Class Correlation (ICC=0.75). A pilot study was carried out on 20% of the participants. The pilot study's goal is to determine the instruments' clarity and validity. Based on the findings of the pilot study, no instrument modifications were made.
Procedure
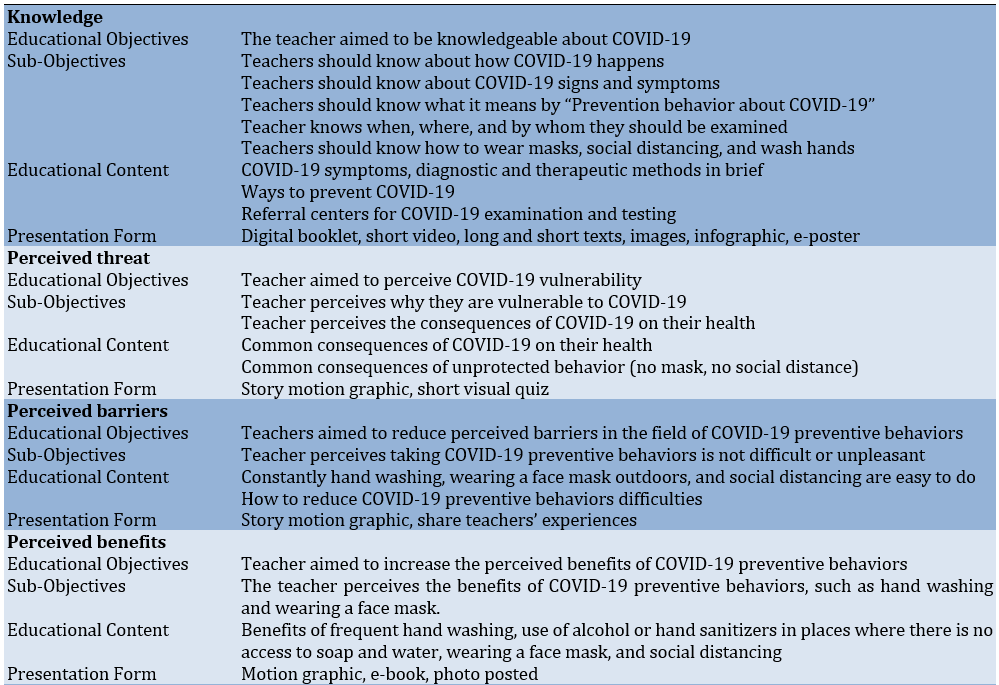
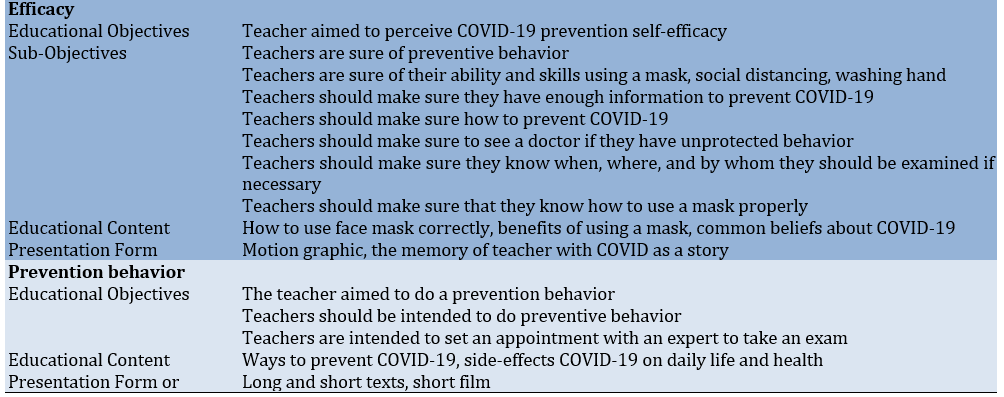
The content of the BEHTA intervention was not individually tailored to each participant, as all participants were homogenous in terms of socio-cultural status. Therefore, the educational contents generally included: 1) Basic health information about the coronaviruses and global timeline of COVID-19, including statistical facts such as COVID-19 prevalence and mortality, when the COVID-19 test will be performed; 2) Introducing the correct ways of implementing COVID-19 preventive behaviors such as wearing a face mask, frequent hand washing, and maintaining social distance; 3) Information about accessibility and availability of local healthcare centers regarding COVID-19 testing and care; 4) Information on how to prevent coronavirus spreading by disinfecting surfaces; 5) Stories, myths, misunderstandings, pseudo-knowledge that describe teachers' overcoming socio-cultural barriers to preventive behaviors regarding COVID-19; 6) When a person should be visited by a doctor; 7) The benefits of obeying preventive behaviors correctly (Table 1).
Table 1. Educational content for BEHTA
The educational intervention was designed and conducted based on the HBM through four sequential phases:
Assessment phase: Assessment of teachers' knowledge, health beliefs and behavior regarding COVID-19 through using the developed tools as an online pretest. The results of the pre-test were analyzed to reveal teachers' training needs for COVID-19.
Planning phase: According to the results of the needs assessment and in light of the relevant literature, the investigators designed an educational intervention in the form of a blended educational program, and then it was independently evaluated by external peer reviewers. The educational intervention emphasized the areas of teacher’s knowledge and health beliefs about COVID-19.
Educational phase: Because of closures in Iranian schools at the time of the COVID-19 pandemic, all the educational intervention was conducted via three online platforms. Our intervention is named BEHTA, abbreviated for Behavior Education Health Teachers Awareness. Actually, the BEHTA intervention was designed as a blended education. In other words, BEHTA’s educational content was delivered through a specifically designed website available at www.behta-tmu.ir, holding virtual and group discussion classes via an online platform called Big Blue Bottom (BBB) supported by Tarbiat Modares University, and using a popular social network messenger (such as WhatsApp) for multimedia messages. Teachers in the intervention group were provided with educational content by accessing the BEHTA website (Behta-tmu.ir) with a password. To increase their knowledge regarding COVID-19, they were allowed to receive all the contents of the website just for two weeks. After this period, access was denied and they had to take part in an online class to share their experiences, beliefs, and attitudes regarding COVID-19 in a group discussion. Accordingly, each Wednesday at 10:00 a.m., four 45-minute online class discussions were moderated by two mentors identified as a healthcare provider and a nurse affiliated with health centers in Tehran. Participants also agreed to receive multimedia messages each day for four weeks at 8:00 a.m. They also, received a reminder notification for the online class participation through their social media (such as WhatsApp) one hour before the class would begin. To enhance participants’ adherence to the BEHTA intervention program, we bought internet service for their smartphones. The subjects were committed to refusing to check educational content and messages about the COVID-19 pandemic received by other platforms during the performance of the study.
Evaluation phase: A follow-up test was conducted immediately and 12 weeks after the one-month intervention using the same pre-test tools for intervention groups. It was an online questionnaire, and the results were collected using the self-report method.
In this study, the control group did not receive intervention. The subjects of the control group participated in the pre and post-test with basic and ordinary information, achievable through mass media such as television, newspapers, and social networks. Therefore, an online post-test was provided to the control group immediately after completing the questionnaire and 12 weeks later, using the same questionnaire in the pre-test stage. Due to the usefulness of the planned education, the interventions were provided to the control group, after evaluation of the findings.
Data analysis
After data collection was completed, it was entered into SPSS 16 software to perform the required analysis. Descriptive statistics such as frequency, percentage, and mean±SD were used to describe the data. Differences between the intervention and control groups were tested using Chi-square, Fisher exact, and independent t-test.
Findings
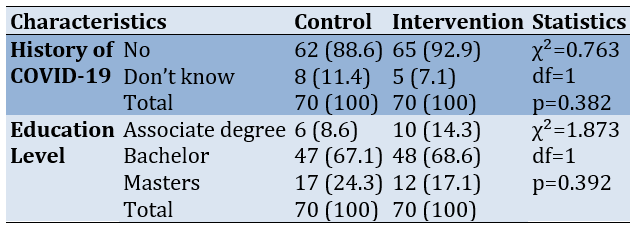
There was no significant difference (t=0.306; df=138; p=0.76) between the mean age of the intervention (44.74±8.50) and the control (44.33±7.48) groups. Also, there was no significant difference (t=1.949; df=138; p=0.053) between the mean job experience of the intervention (20.99±8.56) and the control (17.96±9.78) groups. There were no statistically significant differences between intervention and control groups concerning their demographic characteristic (Table 2).
Table 2. Comparing the sociodemographic characteristics frequency (the numbers in parentheses are percentages) between the intervention (n=70) and control (n=70) groups
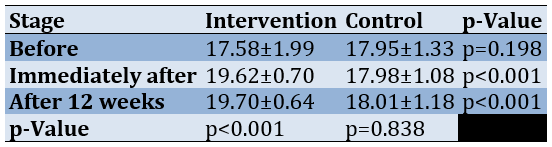
There were no statistically significant differences between the intervention and control groups in all areas of knowledge assessed before the intervention. On the contrary, immediately and 12 weeks after the intervention, significant differences were observed between the intervention and control groups in knowledge (Table 3).
Table 3. Comparing the knowledge score regarding COVID-19 mean between the intervention (n=70) and control (n=70) groups before, immediately and 12 weeks after the intervention
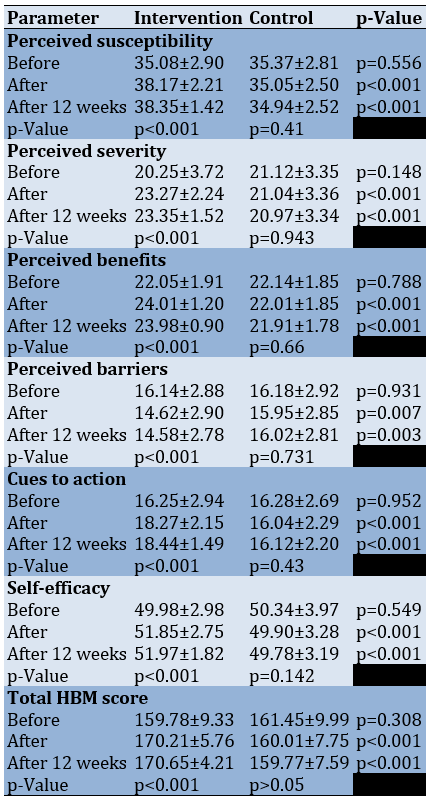
Before the intervention, there were no statistically significant differences between the intervention and control group concerning perceived susceptibility, perceived severity, perceived barriers, perceived benefits, cues to action, self-efficacy, and total health beliefs (p<0.05). Immediately and 12 weeks after the intervention, there were statistically significant differences between intervention and control groups in all elements of the health belief model and the total health beliefs score (p<0.05; Table 4).
Table 4. Comparing the Health Belief Model (HBM) constructs scores mean between the intervention (n=70) and control (n=70) groups before, immediately and 12 weeks after the intervention
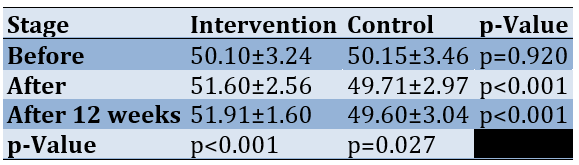
Before the intervention, there were no statistically significant differences between the intervention and control group concerning practice (p<0.05). Immediately and 12 weeks after the intervention, there was a statistically significant difference in practice scores between the intervention and control groups (p<0.05; Table 5).
Table 5. Comparing the practice scores mean between the intervention (n=70) and control (n=70) groups before, immediately and 12 weeks after the intervention
Discussion
The current study was conducted to assess the effect of an educational intervention based on HBM about COVID-19 on teachers’ preventive behavior. Indeed, this study was conducted at a time of the COVID-19 pandemic outbreaks, caused to online education.
The results of the pre-test showed no significant difference in the mean scores of HBM constructs, including perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy between the control and test groups. Indeed, at the pre-test stage, the mean scores were observed in the same range. However, a significant difference was observed between the mean scores of the two groups after providing the interventions to the test group and then comparing the means with the control group, using the post-test. Due to the commitment of the subjects to refuse to receive educational content from other platforms during this study, the difference shows the effectiveness of providing planned education to the test group.
Also, during an interview with the test group subjects, they considered the positive effect of promoting COVID-19 prevention behaviors due to their participation in the online training sessions rather than receiving education messages. They stated that holding online classes has given them the commitment to follow the training.
We investigated the preventive behavior among the teachers, who can have an important role in developing and promoting preventive behaviors among learners. There were several studies with different objectives, such as assessing the public’s perceptions and practices toward COVID-19 by HBM [18], investigating the public’s adherence to COVID-19 preventive practices by HBM [19-22], investigating the factors related to preventive health behaviors during the COVID-19 pandemic by HBM [23, 24], or evaluating the psychological impact of COVID-19 by HBM [25]. So, most of the studies in this area have been performed on students or the public, whereas the sample of our study was the teachers who can promote preventative behaviors among learners.
Based on our results, a statistically significant difference was observed between the two groups in terms of the mean scores of constructs of HBM, including perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy immediately and 12 weeks after the intervention. This statistical difference was also observed in the mean knowledge and practice scores of the two groups 12 weeks later.
There were no studies found online that applied HBM educational intervention for COVID-19 among teachers. Because it is a newly emerging virus, it is the first study that assessed the effectiveness of educational programs on teachers' attitudes regarding HBM constructs. Therefore, we must discuss and compare our findings with other relevant studies regarding general attitude changes about COVID-19.
Significant differences were observed between the pre-intervention score and those immediately and 12 weeks after the intervention group intervention. The results of the present study are in line with Elgzar et al. [19] on Saudi nursing students, Amaliyah [18] on Indonesian individuals, and Ayed et al. [22], on high school students that education is significantly effective in increasing their level of knowledge about COVID-19. On the other hand, in a study to enhance children's handwashing and understanding of microbes. She compared the effects of two types of educational interventions on knowledge and practice. In the first part, a multi-component educational intervention was performed on the experimental group, and their mean knowledge score was significantly improved. However, in the second part, vocal training was performed for the intervention group in which the mean score of knowledge did not increase significantly. The reason for this discrepancy may be due to the educational method; The teaching was done only by playing a poem about hand washing, but in our study, the content was taught during several sessions, and the two-way communication, question and answer sessions, and a website for continuous access to educational content was available.
Significant differences were observed between the pre-intervention score of HBM constructs and those immediately, and 12 weeks after the intervention in the intervention group, which is in line with the results of Elgzar et al. [19], and Nasirzadeh & Aligol [20] that predicted a significant correlation between adopting preventive behaviors for COVID-19 with knowledge, attitude, and HBM constructs, Elasrag et al. [21] on nurses’ attitudes about preventive behaviors from COVID-19, Amaliyah [18] on people's attitudes about COVID-19 preventive behaviors by giving door-to-door health information, and Ayed et al. [22] that use various educational materials, e.g., photos, videos, PowerPoint and booklets to teach students about COVID-19. We haven’t found any study showing that education was ineffective in increasing attitudes associated with COVID-19.
Attitude had the highest correlation coefficient with the adoption of preventive behaviors and was the strongest predictor of preventive behaviors. In different studies, researchers have emphasized the effect and importance of attitude on adopting preventive behaviors [23, 24].
Significant differences were observed between the pre-intervention score of practice and those immediately, and 12 weeks after the intervention in the intervention group which is in line with at least five other studies; Abbas et al. [25] that showed web-based educational intervention as an effective tool for training and promoting preventive behaviors from COVID-19, Tidwell et al. [26] that showed the positive effect of educational intervention through mass media on promoting health habits, Elasrag et al. [21] that showed the positive effect of educational intervention on improving nurses’ performance, Fung et al. [27] that showed the effectiveness of the telephone-based educational intervention on preventing COVID-19 in Hong Kong, Said [28] that showed the educational intervention has a significant effect on the performance of nurses in prevention of COVID-19. In contrast, Mistree et al. [29] compared 10-minute and 22-minute video training interventions on prevention behaviors of COVID-19 and showed that both interventions led to an increase in knowledge, but the first intervention could not significantly change attitudes and behaviors. The reason for this can be the short time of the intervention (3 days) and the inadequacy and lack of variety of educational content. Behavioral change is a complicated process that is likely to occur in different phases through increasing knowledge, making and improving beliefs, perceptions, and attitudes, and providing behavioral facilitators [30, 31].
Although our findings support the effectiveness of the educational intervention, this study had some limitations such as the ineffective collaboration of participants to complete the online questionnaire resulted in time lasting. Moreover, structural and personal barriers to receiving virtual education were the other points that overshadowed our educational program. The data and information were reported by the self-report method. Collecting information through a self-report has limitations. Because people are often biased when they report on their own experiences. Despite the limitations, this study had some strengths too. Promoting preventive behavior-related COVID-19 with an appropriate educational method is important. Individual enabling factors such as level of literacy, socio-economic status, age, etc. as well as access-limiting situations such as the COVID-19 pandemic and lockdown affect educational method selection. Furthermore, choosing the proper training method in line with using a fit change behavior conceptual framework is as important too. The present study was one of the first studies that approached behavior change in the early waves of the COVID-19 pandemic in Iran. Understanding the cognitive factors affecting corona-preventing behaviors in the early waves due to the high perceived fear and sensitivity in people required the design of a curriculum based on the theory and framework of behavior change. On the other hand, in terms of facilitating educational programs by providing training both online and offline, ways Blended learning was designed. This study needs to be replicated in different settings and a larger population to be able to generalize the results.
Conclusion
By increasing the level of knowledge, perceived sensitivity, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy regarding COVID-19, preventive behaviors improve in teachers. Perceived severity is one of the most important predictors of behavior. The 4-week continuous training by various training methods, has a last-long effect on teachers’ behavior. The use of blended educational intervention proved to be an effective flexible educational technique. Given these findings, the healthcare system may wish to consider the BEHTA in concealing education programs for all populations to improve people’s COVID-19 preventive behavior.
Acknowledgments: We would like to extend our sincere gratitude to all the teachers involved in this study. Furthermore, we appreciate the research deputy support at the Faculty of Medical Sciences, Tarbiat Modares University.
Ethical Permissions: The Medical Faculty of Tarbiat Modares University supported this work in 2020 (under the clinical trial registration code IRCT20210416050988N1 and ethics code IR.MODARES.REC.1399.182).
Conflicts of Interests: Nothing declared by the authors.
Authors’ Contribution: Omid M (First Author), Introduction Writer/Main Researcher (50%); Aminshokravi F (Second Author), Methodologist (20%); Zarei F (Third Author), Methodologist/Discussion Writer/Statistical Analyst (30%)
Funding/Support: No funding was received for this study.
Since its emergence in December 2019, Coronavirus disease (COVID-19) has spread globally and become a global concern. COVID-19, which is spread by droplets and direct contact from human to human and is known to cause emergent respiratory infections and ranges from colds to acute severe respiratory syndrome, has imposed a global burden on health and the economy that has never been seen before. It has resulted in more than 1.4 million deaths in 220 countries or territories as of November 29, 2020 [1]. While it appears that the whole world is looking forward to the arrival of safe behavior, the adherence to COVID-19 prevention by the general public remains uncertain [2].
In the Eastern Mediterranean region, Iran has the highest incidence and mortality of COVID-19 [3-5]. On February 19, 2020, the first case of death from COVID-19 was reported in Iran, and the infection spread rapidly [6, 7]. As of January 26, 2020, 1,183,182 definite cases and 54,308 deaths due to COVID-19 have been reported in Iran [8]. The main ways of transmitting coronavirus are by inhaling the infected person’s respiratory droplets and being in close contact with the infected person or their secretions [9]. Even though several types of vaccines protect against COVID-19, the best way to avoid infection is to avoid exposure to this virus [10, 11]. Implementation of the community-based knowledge recommended by the World Health Organization (WHO) for prevention is crucial [12]. COVID-19 preventive behaviors include using a face mask, washing hands frequently with soap and water, covering the mouth and nose with a handkerchief when coughing and sneezing, avoiding touching eyes, mouth, and nose with a sitting hand, avoiding close contact with infected people, and maintaining social distance [11].
Undoubtedly, the COVID-19 epidemic has affected everyone, including teachers, and caused many challenges [13, 14]. In a study in the United States, teachers rated the negative impact of COVID-19 on themselves as moderate [15]. It is important to protect older teachers with an underlying illness because they are a high-risk group for COVID-19 [13, 15]. Teachers should be trained on how to deal with COVID-19 and properly implement health guidelines for the high incidence and mortality of COVID-19 in Iran and the lack of specific treatment. Primary prevention increases knowledge based on scientific evidence creates the proper attitude, and creates COVID-19 preventive behaviors among people, especially teachers. Therefore, considering teachers’ health because of their relationship with many students and having an effective role in them and their parents’ mindsets seems essential; The meaning of the phrase "prevention is better than cure" sheds light on the path.
The Health Belief Model (HBM) is a psychosocial model for behavioral change. It is more often used to describe the relationship between health beliefs and health behaviors. HBM assumes that individuals’ participation in prevention, early detection, and treatment measures for a specific health problem is depended on their perception that they are at risk of this condition, even if they do not exhibit symptoms (perceived susceptibility). They recognize that COVID-19 is a significant health problem with serious consequences (perceived severity); They believe in the benefits of suggested preventive measures (perceived benefits) and recognize that the benefits outweigh the common barriers associated with these measures (perceived barriers). Furthermore, they believe they have the motivation and ability to engage in a healthy lifestyle [16].
According to the above, teachers’ health beliefs, behaviors, and knowledge about preventive behaviors are important. Changing the health beliefs regarding the infectious disease epidemic may deeply root the importance of self-efficacy in healthy behavior regarding COVID-19. The educational intervention content leveled them up with the latest updates about COVID-19's way of transmission, signs and symptoms, and preventive behaviors.
Therefore, promoting preventive behavior-related COVID-19 with an appropriate educational method is important. Individual enabling factors such as level of literacy, socio-economic status, age, etc. as well as access-limiting situations such as the COVID-19 pandemic and lockdowns affect educational method selection. Furthermore, choosing the proper training method in line with using a fit change behavior conceptual framework is as important too. The present study was one of the first studies that approached behavior change in the early waves of the COVID-19 pandemic in Iran. Understanding the cognitive factors affecting corona-preventing behaviors in the early waves due to the high perceived fear and sensitivity in people required the design of a curriculum based on the theory and framework of behavior change. On the other hand, in terms of facilitating educational programs by providing training both in online and offline ways blended learning was designed. The current study aimed to investigate the effect of an educational intervention based on the HBM about COVID-19 on teachers' knowledge, health beliefs, and behaviors.
Materials and Methods
Study design
This randomized controlled trial was conducted on elementary school teachers of Karaj City, Iran, in 2021. Comprehensive sampling was followed to include all below 60 female teachers who were residents of Karaj, Alborz Province, Iran (140 teachers). The cluster sampling method was used for sampling. First, two districts were randomly selected from the four districts affiliated with the Karaj Education Organization (districts 3 and 4). Then, one of these two areas was assigned to the intervention group (district 3) and the other to the control group (area 4) by lottery method. Then, from each of these two districts, 12 primary schools were randomly selected by an externally trained researcher (Figure 1). Teachers from selected schools were invited to participate in this study, taking into account the inclusion and exclusion criteria, set by the teachers of these schools during a telephone or in-person call after a brief description of the subject of the study and its objectives. Written and online consent was obtained from them.
Figure 1. Consort diagram
Data collection tools
Data were collected using a validated questionnaire [17]. It has two sections: Part I: Socio-demographic data, designed to collect data such as age, educational level, residence, work experience, and history of COVID-19. Part II: Assessment of teacher’s knowledge regarding COVID-19: Researchers developed it after reviewing current literature. It included the COVID-19 definition, signs and symptoms, mode of transmission, and World Health Organization recommendations. Part III: Health belief model scale; To assess teacher’s beliefs regarding COVID-19. Researchers developed it after reviewing current literature to examine perceived susceptibility (8 items), perceived severity (5 items), perceived benefits (5 items), perceived barriers (6 items), cues to action (4 items) and self-efficacy (11 items). In each item, the teachers have to choose one of five alternatives: Strongly agree=5, agree=4, indifference=3, don't agree=2, and strongly don't agree=1. Part IV: Assessment of teachers’ behavior regarding COVID-19: Teachers’ likelihood to engage in healthy behaviors regarding COVID-19. In this item, the teachers have to choose one of five alternatives: Always=5, often=4, sometimes=3, rarely=2, and never=1. The researchers developed the instrument, and then it was tested for face, content, and construct validity by 15 experts in health education, health care providers, and nursing fields. Instrument reliability was conducted using Cronbach's Alpha coefficient test (r=0.78) and Intra-Class Correlation (ICC=0.75). A pilot study was carried out on 20% of the participants. The pilot study's goal is to determine the instruments' clarity and validity. Based on the findings of the pilot study, no instrument modifications were made.
Procedure
The content of the BEHTA intervention was not individually tailored to each participant, as all participants were homogenous in terms of socio-cultural status. Therefore, the educational contents generally included: 1) Basic health information about the coronaviruses and global timeline of COVID-19, including statistical facts such as COVID-19 prevalence and mortality, when the COVID-19 test will be performed; 2) Introducing the correct ways of implementing COVID-19 preventive behaviors such as wearing a face mask, frequent hand washing, and maintaining social distance; 3) Information about accessibility and availability of local healthcare centers regarding COVID-19 testing and care; 4) Information on how to prevent coronavirus spreading by disinfecting surfaces; 5) Stories, myths, misunderstandings, pseudo-knowledge that describe teachers' overcoming socio-cultural barriers to preventive behaviors regarding COVID-19; 6) When a person should be visited by a doctor; 7) The benefits of obeying preventive behaviors correctly (Table 1).
Table 1. Educational content for BEHTA
The educational intervention was designed and conducted based on the HBM through four sequential phases:
Assessment phase: Assessment of teachers' knowledge, health beliefs and behavior regarding COVID-19 through using the developed tools as an online pretest. The results of the pre-test were analyzed to reveal teachers' training needs for COVID-19.
Planning phase: According to the results of the needs assessment and in light of the relevant literature, the investigators designed an educational intervention in the form of a blended educational program, and then it was independently evaluated by external peer reviewers. The educational intervention emphasized the areas of teacher’s knowledge and health beliefs about COVID-19.
Educational phase: Because of closures in Iranian schools at the time of the COVID-19 pandemic, all the educational intervention was conducted via three online platforms. Our intervention is named BEHTA, abbreviated for Behavior Education Health Teachers Awareness. Actually, the BEHTA intervention was designed as a blended education. In other words, BEHTA’s educational content was delivered through a specifically designed website available at www.behta-tmu.ir, holding virtual and group discussion classes via an online platform called Big Blue Bottom (BBB) supported by Tarbiat Modares University, and using a popular social network messenger (such as WhatsApp) for multimedia messages. Teachers in the intervention group were provided with educational content by accessing the BEHTA website (Behta-tmu.ir) with a password. To increase their knowledge regarding COVID-19, they were allowed to receive all the contents of the website just for two weeks. After this period, access was denied and they had to take part in an online class to share their experiences, beliefs, and attitudes regarding COVID-19 in a group discussion. Accordingly, each Wednesday at 10:00 a.m., four 45-minute online class discussions were moderated by two mentors identified as a healthcare provider and a nurse affiliated with health centers in Tehran. Participants also agreed to receive multimedia messages each day for four weeks at 8:00 a.m. They also, received a reminder notification for the online class participation through their social media (such as WhatsApp) one hour before the class would begin. To enhance participants’ adherence to the BEHTA intervention program, we bought internet service for their smartphones. The subjects were committed to refusing to check educational content and messages about the COVID-19 pandemic received by other platforms during the performance of the study.
Evaluation phase: A follow-up test was conducted immediately and 12 weeks after the one-month intervention using the same pre-test tools for intervention groups. It was an online questionnaire, and the results were collected using the self-report method.
In this study, the control group did not receive intervention. The subjects of the control group participated in the pre and post-test with basic and ordinary information, achievable through mass media such as television, newspapers, and social networks. Therefore, an online post-test was provided to the control group immediately after completing the questionnaire and 12 weeks later, using the same questionnaire in the pre-test stage. Due to the usefulness of the planned education, the interventions were provided to the control group, after evaluation of the findings.
Data analysis
After data collection was completed, it was entered into SPSS 16 software to perform the required analysis. Descriptive statistics such as frequency, percentage, and mean±SD were used to describe the data. Differences between the intervention and control groups were tested using Chi-square, Fisher exact, and independent t-test.
Findings
There was no significant difference (t=0.306; df=138; p=0.76) between the mean age of the intervention (44.74±8.50) and the control (44.33±7.48) groups. Also, there was no significant difference (t=1.949; df=138; p=0.053) between the mean job experience of the intervention (20.99±8.56) and the control (17.96±9.78) groups. There were no statistically significant differences between intervention and control groups concerning their demographic characteristic (Table 2).
Table 2. Comparing the sociodemographic characteristics frequency (the numbers in parentheses are percentages) between the intervention (n=70) and control (n=70) groups
There were no statistically significant differences between the intervention and control groups in all areas of knowledge assessed before the intervention. On the contrary, immediately and 12 weeks after the intervention, significant differences were observed between the intervention and control groups in knowledge (Table 3).
Table 3. Comparing the knowledge score regarding COVID-19 mean between the intervention (n=70) and control (n=70) groups before, immediately and 12 weeks after the intervention
Before the intervention, there were no statistically significant differences between the intervention and control group concerning perceived susceptibility, perceived severity, perceived barriers, perceived benefits, cues to action, self-efficacy, and total health beliefs (p<0.05). Immediately and 12 weeks after the intervention, there were statistically significant differences between intervention and control groups in all elements of the health belief model and the total health beliefs score (p<0.05; Table 4).
Table 4. Comparing the Health Belief Model (HBM) constructs scores mean between the intervention (n=70) and control (n=70) groups before, immediately and 12 weeks after the intervention
Before the intervention, there were no statistically significant differences between the intervention and control group concerning practice (p<0.05). Immediately and 12 weeks after the intervention, there was a statistically significant difference in practice scores between the intervention and control groups (p<0.05; Table 5).
Table 5. Comparing the practice scores mean between the intervention (n=70) and control (n=70) groups before, immediately and 12 weeks after the intervention
Discussion
The current study was conducted to assess the effect of an educational intervention based on HBM about COVID-19 on teachers’ preventive behavior. Indeed, this study was conducted at a time of the COVID-19 pandemic outbreaks, caused to online education.
The results of the pre-test showed no significant difference in the mean scores of HBM constructs, including perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy between the control and test groups. Indeed, at the pre-test stage, the mean scores were observed in the same range. However, a significant difference was observed between the mean scores of the two groups after providing the interventions to the test group and then comparing the means with the control group, using the post-test. Due to the commitment of the subjects to refuse to receive educational content from other platforms during this study, the difference shows the effectiveness of providing planned education to the test group.
Also, during an interview with the test group subjects, they considered the positive effect of promoting COVID-19 prevention behaviors due to their participation in the online training sessions rather than receiving education messages. They stated that holding online classes has given them the commitment to follow the training.
We investigated the preventive behavior among the teachers, who can have an important role in developing and promoting preventive behaviors among learners. There were several studies with different objectives, such as assessing the public’s perceptions and practices toward COVID-19 by HBM [18], investigating the public’s adherence to COVID-19 preventive practices by HBM [19-22], investigating the factors related to preventive health behaviors during the COVID-19 pandemic by HBM [23, 24], or evaluating the psychological impact of COVID-19 by HBM [25]. So, most of the studies in this area have been performed on students or the public, whereas the sample of our study was the teachers who can promote preventative behaviors among learners.
Based on our results, a statistically significant difference was observed between the two groups in terms of the mean scores of constructs of HBM, including perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy immediately and 12 weeks after the intervention. This statistical difference was also observed in the mean knowledge and practice scores of the two groups 12 weeks later.
There were no studies found online that applied HBM educational intervention for COVID-19 among teachers. Because it is a newly emerging virus, it is the first study that assessed the effectiveness of educational programs on teachers' attitudes regarding HBM constructs. Therefore, we must discuss and compare our findings with other relevant studies regarding general attitude changes about COVID-19.
Significant differences were observed between the pre-intervention score and those immediately and 12 weeks after the intervention group intervention. The results of the present study are in line with Elgzar et al. [19] on Saudi nursing students, Amaliyah [18] on Indonesian individuals, and Ayed et al. [22], on high school students that education is significantly effective in increasing their level of knowledge about COVID-19. On the other hand, in a study to enhance children's handwashing and understanding of microbes. She compared the effects of two types of educational interventions on knowledge and practice. In the first part, a multi-component educational intervention was performed on the experimental group, and their mean knowledge score was significantly improved. However, in the second part, vocal training was performed for the intervention group in which the mean score of knowledge did not increase significantly. The reason for this discrepancy may be due to the educational method; The teaching was done only by playing a poem about hand washing, but in our study, the content was taught during several sessions, and the two-way communication, question and answer sessions, and a website for continuous access to educational content was available.
Significant differences were observed between the pre-intervention score of HBM constructs and those immediately, and 12 weeks after the intervention in the intervention group, which is in line with the results of Elgzar et al. [19], and Nasirzadeh & Aligol [20] that predicted a significant correlation between adopting preventive behaviors for COVID-19 with knowledge, attitude, and HBM constructs, Elasrag et al. [21] on nurses’ attitudes about preventive behaviors from COVID-19, Amaliyah [18] on people's attitudes about COVID-19 preventive behaviors by giving door-to-door health information, and Ayed et al. [22] that use various educational materials, e.g., photos, videos, PowerPoint and booklets to teach students about COVID-19. We haven’t found any study showing that education was ineffective in increasing attitudes associated with COVID-19.
Attitude had the highest correlation coefficient with the adoption of preventive behaviors and was the strongest predictor of preventive behaviors. In different studies, researchers have emphasized the effect and importance of attitude on adopting preventive behaviors [23, 24].
Significant differences were observed between the pre-intervention score of practice and those immediately, and 12 weeks after the intervention in the intervention group which is in line with at least five other studies; Abbas et al. [25] that showed web-based educational intervention as an effective tool for training and promoting preventive behaviors from COVID-19, Tidwell et al. [26] that showed the positive effect of educational intervention through mass media on promoting health habits, Elasrag et al. [21] that showed the positive effect of educational intervention on improving nurses’ performance, Fung et al. [27] that showed the effectiveness of the telephone-based educational intervention on preventing COVID-19 in Hong Kong, Said [28] that showed the educational intervention has a significant effect on the performance of nurses in prevention of COVID-19. In contrast, Mistree et al. [29] compared 10-minute and 22-minute video training interventions on prevention behaviors of COVID-19 and showed that both interventions led to an increase in knowledge, but the first intervention could not significantly change attitudes and behaviors. The reason for this can be the short time of the intervention (3 days) and the inadequacy and lack of variety of educational content. Behavioral change is a complicated process that is likely to occur in different phases through increasing knowledge, making and improving beliefs, perceptions, and attitudes, and providing behavioral facilitators [30, 31].
Although our findings support the effectiveness of the educational intervention, this study had some limitations such as the ineffective collaboration of participants to complete the online questionnaire resulted in time lasting. Moreover, structural and personal barriers to receiving virtual education were the other points that overshadowed our educational program. The data and information were reported by the self-report method. Collecting information through a self-report has limitations. Because people are often biased when they report on their own experiences. Despite the limitations, this study had some strengths too. Promoting preventive behavior-related COVID-19 with an appropriate educational method is important. Individual enabling factors such as level of literacy, socio-economic status, age, etc. as well as access-limiting situations such as the COVID-19 pandemic and lockdown affect educational method selection. Furthermore, choosing the proper training method in line with using a fit change behavior conceptual framework is as important too. The present study was one of the first studies that approached behavior change in the early waves of the COVID-19 pandemic in Iran. Understanding the cognitive factors affecting corona-preventing behaviors in the early waves due to the high perceived fear and sensitivity in people required the design of a curriculum based on the theory and framework of behavior change. On the other hand, in terms of facilitating educational programs by providing training both online and offline, ways Blended learning was designed. This study needs to be replicated in different settings and a larger population to be able to generalize the results.
Conclusion
By increasing the level of knowledge, perceived sensitivity, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy regarding COVID-19, preventive behaviors improve in teachers. Perceived severity is one of the most important predictors of behavior. The 4-week continuous training by various training methods, has a last-long effect on teachers’ behavior. The use of blended educational intervention proved to be an effective flexible educational technique. Given these findings, the healthcare system may wish to consider the BEHTA in concealing education programs for all populations to improve people’s COVID-19 preventive behavior.
Acknowledgments: We would like to extend our sincere gratitude to all the teachers involved in this study. Furthermore, we appreciate the research deputy support at the Faculty of Medical Sciences, Tarbiat Modares University.
Ethical Permissions: The Medical Faculty of Tarbiat Modares University supported this work in 2020 (under the clinical trial registration code IRCT20210416050988N1 and ethics code IR.MODARES.REC.1399.182).
Conflicts of Interests: Nothing declared by the authors.
Authors’ Contribution: Omid M (First Author), Introduction Writer/Main Researcher (50%); Aminshokravi F (Second Author), Methodologist (20%); Zarei F (Third Author), Methodologist/Discussion Writer/Statistical Analyst (30%)
Funding/Support: No funding was received for this study.
Article Type: Original Research |
Subject:
Technology of Health Education
Received: 2024/01/19 | Accepted: 2024/04/4 | Published: 2025/05/15
Received: 2024/01/19 | Accepted: 2024/04/4 | Published: 2025/05/15
References
1. Jebril N. World Health Organization declared a pandemic public health menace: A systematic review of the coronavirus disease 2019 "COVID-19". Int J Psychosoc Rehabil. 2020;24(9):2784-95. [Link] [DOI:10.2139/ssrn.3566298]
2. Eikenberry SE, Mancuso M, Iboi E, Phan T, Eikenberry K, Kuang Y, et al. To mask or not to mask: Modeling the potential for face mask use by the general public to curtail the COVID-19 pandemic. Infect Dis Model. 2020;5:293-308. [Link] [DOI:10.1016/j.idm.2020.04.001]
3. Worldometer. COVID-19 coronavirus pandemic [Internet]. United States: Worldometer; 2020 [cited 2020 Dec 25]. Available from: https://www.worldometers.info/coronavirus/. [Link]
4. Salameh P. COVID-19 in the Eastern Mediterranean Region: Testing frequency, cumulative cases and mortality analysis. East Mediterr Health J. 2020;26(9):1005-10. [Link] [DOI:10.26719/emhj.20.110]
5. Dil S, Dil N, Maken ZH. COVID-19 trends and forecast in the Eastern Mediterranean Region with a particular focus on Pakistan. Cureus. 2020;12(6):e8582. [Link] [DOI:10.7759/cureus.8582]
6. Takian A, Raoofi A, Kazempour-Ardebili S. COVID-19 battle during the toughest sanctions against Iran. Lancet. 2020;395(10229):1035-36. [Link] [DOI:10.1016/S0140-6736(20)30668-1]
7. Maghsudlu M, Eshghi P, Amini Kafi-Abad S, Sedaghat A, Ranjbaran H, Mohammadi S, et al. Blood supply sufficiency and safety management in Iran during the COVID‐19 outbreak. Vox Sang. 2021;116(2):175-80. [Link] [DOI:10.1111/vox.13012]
8. World Health Organization. WHO COVID-19 dashboard [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Dec 25]. Available from: https://covid19.who.int/. [Link]
9. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506. [Link] [DOI:10.1016/S0140-6736(20)30183-5]
10. Cirrincione L, Plescia F, Ledda C, Rapisarda V, Martorana D, Moldovan RE, et al. COVID-19 pandemic: Prevention and protection measures to be adopted at the workplace. Sustainability. 2020;12(9):3603. [Link] [DOI:10.3390/su12093603]
11. Min C, Shen F, Yu W, Chu Y. The relationship between government trust and preventive behaviors during the COVID-19 pandemic in China: Exploring the roles of knowledge and negative emotion. Prev Med. 2020;141:106288. [Link] [DOI:10.1016/j.ypmed.2020.106288]
12. Weston D, Ip A, Amlôt R. Examining the application of behaviour change theories in the context of infectious disease outbreaks and emergency response: A review of reviews. BMC Public Health. 2020;20(1):1483. [Link] [DOI:10.1186/s12889-020-09519-2]
13. Reimers FM, Schleicher A. Schooling disrupted, schooling rethought: How the COVID-19 pandemic is changing education. Berlin: OECD; 2020. p. 12. [Link]
14. Lemon N. Impact of COVID-19 on grade school teachers [Preprint]. 2020 [cited 2024, 28 June]. Available from: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3639315. [Link] [DOI:10.2139/ssrn.3639315]
15. University of Maryland. New study! The impact of COVID-19 on teachers. College Park: University of Maryland; 2020 [cited 2020 Nov 16]. Available from: https://education.umd.edu/research-college/impact-covid-19-teachers. [Link]
16. Safaari M, Shojaeizadeh D, Heidarnia A, Pakpoor Haji Agha A, Ghafranipoor F. Theories, models and methods of health education and health promotion. Tehran: Asar-E Sobhan Publishing; 2014. [Persian] [Link]
17. Omid M, Aminshokravi F, Zarei F. Design and psychometrics of a questionnaire on COVID-19 preventive behaviors evaluation based on health behavior model. Health Educ Health Promot. 2022;10(2):315-21. [Link]
18. Amaliyah E, Aminah. A pilot study of seven-day education program "door-to-door" to improve knowledge, attitude, and practices towards 2019-nCoV during stay at home in Indonesia. KnE Life Sci. 2021;6(1):124-31. [Link] [DOI:10.18502/kls.v6i1.8597]
19. Elgzar WT, Al-Qahtani AM, Elfeki NK, Ibrahim HA. COVID-19 outbreak: Effect of an educational intervention based on health belief model on nursing students' awareness and health beliefs at Najran University, Kingdom of Saudi Arabia. Afr J Reprod Health. 2020;24(s1):78-86. [Link]
20. Nasirzadeh M, Aligol M. Assessment of knowledge, attitude, and factors associated with the preventive behaviors of Covid-19 in Qom, Iran, in 2020. Qom Univ Med Sci J. 2020;14(7):50-7. [Persian] [Link] [DOI:10.29252/qums.14.7.50]
21. Elasrag GAEA, Elsabagh NE, Abdelmonem AF, Ahmed AA. Impact of educational intervention on nurses' knowledge, practice and attitude related prevention measures of COVID 19. Indian J Forensic Med Toxicol. 2021;15(3):2939-48. [Link] [DOI:10.37506/ijfmt.v15i3.15751]
22. Ayed MMA, Mohamed AAE, Mahmoud TM, AbdElaziz SM. Impact of educational intervention on secondary school students' knowledge, practices and attitudes regarding to COVID-19. 2021;12(2):58-74. [Link] [DOI:10.21608/ejhc.2021.145405]
23. Zeng Y, Yuan Z, Yin J, Han Y, Chu CI, Fang Y. Factors affecting parental intention to vaccinate kindergarten children against influenza: A cross-sectional survey in China. Vaccine. 2019;37(11):1449-56. [Link] [DOI:10.1016/j.vaccine.2019.01.071]
24. Goss MD, Temte JL, Barlow S, Temte E, Bell C, Birstler J, et al. An assessment of parental knowledge, attitudes, and beliefs regarding influenza vaccination. Vaccine. 2020;38(6):1565-71. [Link] [DOI:10.1016/j.vaccine.2019.11.040]
25. Abbas K, Nawaz SMA, Amin N, Soomro FM, Abid K, Ahmed M, et al. A web-based health education module and its impact on the preventive practices of health-care workers during the COVID-19 pandemic. Health Educ Res. 2020;35(5):353-61. [Link] [DOI:10.1093/her/cyaa034]
26. Tidwell JB, Gopalakrishnan A, Lovelady S, Sheth E, Unni A, Wright R, et al. Effect of two complementary mass-scale media interventions on handwashing with soap among mothers. J Health Commun. 2019;24(2):203-15. [Link] [DOI:10.1080/10810730.2019.1593554]
27. Fung MY, Lee YH, Lee YTA, Wong ML, Li JTS, Lee V. PIH22 efficacy of telephone-based educational intervention on knowledge transfer of COVID-19 related health topics to elderly citizens in Hong Kong: A pilot study. Value Health. 2021;24:S103. [Link] [DOI:10.1016/j.jval.2021.04.540]
28. Said AR. Knowledge and practices of nurses regarding Corona Virus (COVID-19): An educational intervention. Medico Leg Update. 2021;21(2):36-47. [Link] [DOI:10.37506/mlu.v21i2.2642]
29. Mistree D, Loyalka P, Fairlie R, Bhuradia A, Angrish M, Lin J, et al. Instructional interventions for improving COVID-19 knowledge, attitudes, behaviors: Evidence from a large-scale RCT in India. Soc Sci Med. 2021;276:113846. [Link] [DOI:10.1016/j.socscimed.2021.113846]
30. Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education: Theory, research, and practice. 4th ed. Hoboken: Jossey-Bass; 2008. [Link]
31. Michie S, Van Stralen MM, West R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. [Link] [DOI:10.1186/1748-5908-6-42]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |