



Volume 9, Issue 3 (2021)
Health Educ Health Promot 2021, 9(3): 303-308 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohammad P, Amine S, Sabir D, Saeed F, Hama Amin D. Psychological Impact of COVID-19 on Healthcare Workers in the Kurdistan Region, Iraq. Health Educ Health Promot 2021; 9 (3) :303-308
URL: http://hehp.modares.ac.ir/article-5-51616-en.html
URL: http://hehp.modares.ac.ir/article-5-51616-en.html
1- Charmo Center for Research, Training and Consultancy, Charmo University, Chamchamal, Iraq , parzheen.mohammad@charmouniversity.org
2- Department of Medical Laboratory Science, Charmo University, Chamchamal, Iraq
3- Sulaimani Teaching Hospital, Sulaimani, Iraq
4- Life Mental Health Center, Anwar Sheikha Medical City, Sulaimani, Iraq
2- Department of Medical Laboratory Science, Charmo University, Chamchamal, Iraq
3- Sulaimani Teaching Hospital, Sulaimani, Iraq
4- Life Mental Health Center, Anwar Sheikha Medical City, Sulaimani, Iraq
Keywords: COVID-19 [MeSH], Healthcare Workers [MeSH], PTSD [MeSH], Anxiety [MeSH], Depression [MeSH]
Full-Text [PDF 440 kb]
(3474 Downloads)
| Abstract (HTML) (2899 Views)
Full-Text: (1025 Views)
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the etiological agent of the coronavirus disease of 2019 (COVID-19), which first was identified in late December 2019 in the city of Wuhan in China [1]. According to World Health Organization (WHO) data, on 2020, on July 18, 86,100 confirmed cases of covid-19 and 3,500 deaths in Iraq [2]. In the Kurdistan Region of Iraq (KRI) alone, 10,595 were infected, and 402 lost their lives, according to data that was released by the Kurdistan Regional Government (KRG) on 2020, March 30 [3]. To address this critical situation, the government declared February 26 to March 10, 2020, a public holiday for all public and private schools and kindergartens. Moreover, public and private universities were closed from February 29 to March 10 and will remain closed during the spring break (10–23 March) before reopening on March 24, if the situation improves. The KRG also decided to halt all religious ceremonies, rituals, and activities-including Friday sermons-in in mosques, churches, and temples throughout the KRI until further notice. Although the lockdown duration was extended later, the healthcare workers remained at work to tackle the situation.
Healthcare workers in hospitals equipped and specialized for COVID-19; because of the direct and indirect contact with the COVID-19 patients and being vulnerable to the infection [4], they are at risk for developing mental health problems [1]. Evidence from previous studies on SARS showed that healthcare workers concern about infecting others (especially family members) than being infected themselves [4]. They also had suffered from an acute stress disorder, felt stigmatized and rejected in their neighborhood because of their hospital work, and reported reluctance to work or had considered resignation [5]. Tremendous psychological distress, particularly among healthcare workers, and increasing feelings of isolation were reported [6]. More recently, a study in Singapore examined the psychological impact of the COVID-19 outbreak on healthcare workers. Four hundred seventy healthcare workers from two major tertiary institutions participated in this study. The results showed that 30% of the healthcare workers screened positive for depression, anxiety, and stress.
Furthermore, 7.7% of the participants had clinical features of Post-Traumatic Stress Disorder (PTSD) [7]. Studies on the psychological impact of COVID-19 in China found that frontline healthcare workers, who are working with COVID-19 patients, reported stress, depression, and anxiety [1, 8, 9], as well as insomnia symptoms [1]. They have also been found to become emotionally affected and traumatized [9]. These findings from China are despite the availability of local and national mental health institutions that provide psychological support services, deployed to a large degree amid the COVID-19 outbreak. On February 2, 2020, the State Council of China announced that they were launching nationwide psychological support hotlines to assist people during the Coronavirus outbreak [10].
In the KRI, there is a lack of such actions both in normal times and during a crisis such as the COVID-19 pandemic. Psychological support services, counseling, or other professional interventions are scarce, disregarded, and not easily accessed by laypeople and healthcare workers. Additionally, the psychological impact of the COVID-19 outbreak remains largely unexplored in the region. Based on our knowledge, the current study is one of the firsts to address the psychological wellbeing of healthcare workers exposed to COVID-19 in the KRI. The current study aimed to assess the psychological impact of COVID-19 healthcare workers involved in providing medical care to the patients by identifying the levels of PTSD, anxiety, and depression. Moreover, this study aimed to assess the level of PTSD, depression, and anxiety based on gender, family status, occupation, city, and line of work.
Instrument and Methods
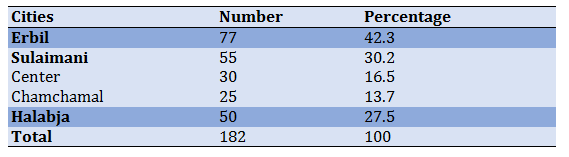
This descriptive study was conducted through the in-person distribution of the survey, and the data was collected from April 10, 2020, to May 20, 2020. To compare the interregional differences of mental health outcomes among healthcare workers in KRI, samples were classified by their geographic location (Erbil, Sulaimani, Chamchamal, and Halabja). Since the city of Sulaimani was the first place to be severely affected, more hospitals in this province were sampled. Hospitals equipped and specialized for COVID-19 were eligible to participate in this survey. Convenience Sampling was used in this study based on the accessibility of the sample by the authors. Healthcare workers in selected COVID-19 hospitals in three provinces; Erbil, Sulaimani; (Center, Chamchamal), and Halabja, and part of healthcare workers in those hospitals were asked to participate in this study on a convenience sampling method. Since Erbil is the largest city in Iraq's Kurdistan region, more Erbil participants were included. A total of 182 of 237 invited healthcare workers completed the survey in the four
different locations, with a participation rate of 76.8% (Table 1).
Table 1) sample size across settings
Three questionnaires were used as follow:
PTSD Checklist for DSM-5 (PCL-5): Since one of the aims of this study was to assess PTSD symptoms, the Kurdish version of PCL-5, which had been translated and adapted by a group of researchers from Bielefeld University, Germany, and Koya University, was used to assess PTSD symptoms among health care workers [11]. The PCL-5 contains twenty items rated on a five-point Likert-type scale, with options ranging from "Not at all" (0) to "Extremely" (4), and scores ranging between 0 and 80. A cut-off point of 23 would be accounted as PTSD in the Kurdish version of the PCL-5. The scale's internal consistency was reported to be high, with an alpha score of 0.89 in a study on Syrian refugees [12]. In the current study, the internal consistency of the PCL-5 was also high (alpha=0.94).
Hopkins Symptom Checklist (HSCL-25) [13]: The Kurdish version of the 25 item Hopkins symptom checklist HSCL-25, which has been translated and adapted by Heartland Alliance, was used to assess the levels of depression and anxiety. HSCL-25 is a four Likert-type scale, with options ranging from "Not at all" (1) to "Extremely" (4). The HSCL-25 contains two sections, the first section includes ten items of anxiety symptoms, and the second section includes 15 items of depression symptoms. Further, individuals with an average score greater than 1.75 in anxiety and depression are considered symptomatic. On this scale, 1.75 is considered a scientifically valid cut-off point. The depression subscale of the HSCL-25, with an alpha score of 0.86, was high internal consistency [12]. Similarly, in the present study, the depression sub-scale of the HSCL-25 showed high internal consistency (Alpha=0.85). The anxiety sub-scale had an alpha score of 0.88, indicating a high level of internal consistency.
Sociodemographic Information: Sociodemographic data were collected from the participants, including sex (male, female, or not specified), age (18-25, 26-30, 31-40, or >40 years), marital status (single, married, and divorced), occupation (physician, nurse, and lab technician), residence (inside provinces: Sulaimani and/or Erbil, outside provinces: Chamchamal and/or Halabja), place of work (inside provinces: Sulaimani and/or Erbil, outside provinces: Chamchamal and/or Halabja), technical title, working with COVID-19 patients (frontline; directly exposed and engaged in providing care to the patients, second-line; no exposure or engagement with patients yet working inside the hospitals of COVID-19). Moreover, participants were asked an additional question about whether they had experienced any traumatic events, for example, being frightened of getting the virus, witnessing a patient suffering, or any other severe humanitarian event. This was to find the differences in the PTSD, anxiety, and depression symptoms between those who respond "yes" to the trauma question and those who respond "no".
This study followed the ethical principles of the authors' institution's reporting guidelines. Approval from the research ethics committee of the Charmo University was received before the initiation of this study. Informed consent was given by all participants before their enrolment. Participants were allowed to terminate the survey at any time they desired. The survey was anonymous, and confidentiality of information was assured.
Data analysis was performed using SPSS 20.0. The original data were counted as a sum "total score" for PTSD and mean score for anxiety and depression to determine each level for symptoms of PTSD, anxiety, depression, and presented as numbers and percentages. An exploratory data analysis was carried out to determine the distribution of the scores. The scores of PTSD were not normally distributed based on the results of the Shapiro-Wilk test (p≤0.01) and Kolmogorov-Smirnov test (p≤0.05), as well as the visual inspection of Q-Q plots and histograms. Therefore, the nonparametric Mann-Whitney U test and Kruskal-Wallis test were applied to compare the severity of each disorder between two or more groups, respectively.
Findings
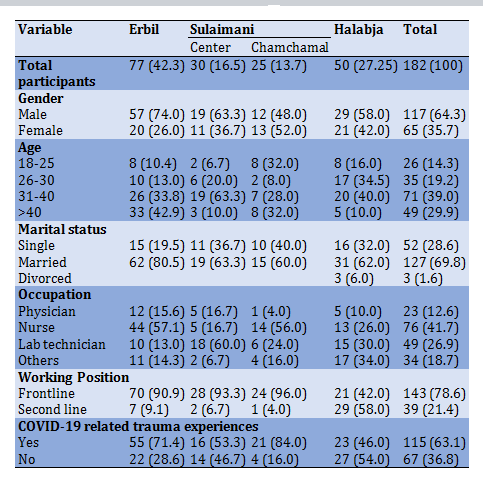
All 182 healthcare workers participated. Most of the participants were male, aged 31 to 40 years, married, nurse, working in Erbil, and frontline workers. Of all participants, 115 (63.2%) people reported having had a traumatic experience during their work with COVID-19 patients (Table 2).
Table 2) Results of frequency of demographic characteristics (the numbers in parentheses are in percentage)
Based on results, 53.3% of healthcare workers screened positive for PTSD, 29.1% screened positive for anxiety, and 39.0% screened positive for depression (Table 3).
There was no statistically significant difference in the symptoms of PTSD, anxiety, and depression based on gender, according to the Mann-Whitney U test (Table 4), and based on family status according to the Kruskal-Wallis test results (Table 5).
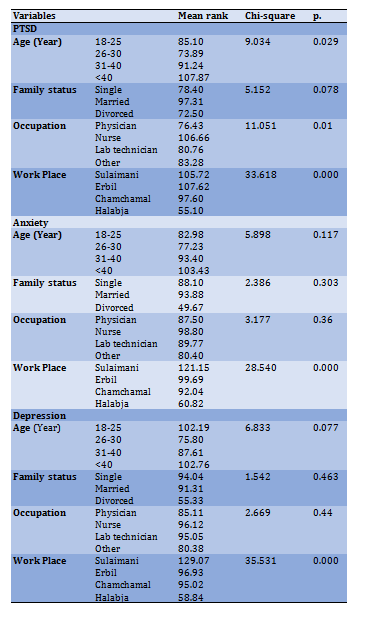
However, Kruskal-Wallis test results revealed statistically significant differences in age cohort, occupation, and workplace (p<0.05). Mann-Whitney U test results showed statistically significant differences according to work position and those who experienced traumatic events and those who did not (p<0.05). Healthcare workers who were aged >40 scored higher on PCL-5 for PTSD, and responders who were aged 26-30 years seemed least affected than other age groups p<0.02, but there were no significant differences on anxiety and depression scales (p>0.05). Similarly, Nurses reported the highest scores on the PTSD scale, and physicians reported the lowest at a significant difference level p<0.01 but no significant difference on other scales (p>0.05).
Table 3) Prevalence of PTSD, depression, and anxiety and mean HSC-25 and PCL-5 Scores in Health Care workers (N=182)
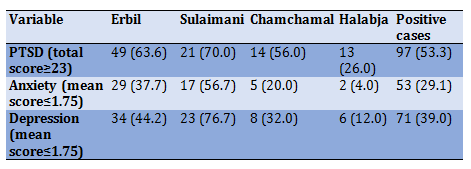
Table 4) Results of Mann-Whitney U test for comparing mean rank scores of PTSD, depression, and anxiety measurements according to gender, working position, and COVID-19 related trauma experience
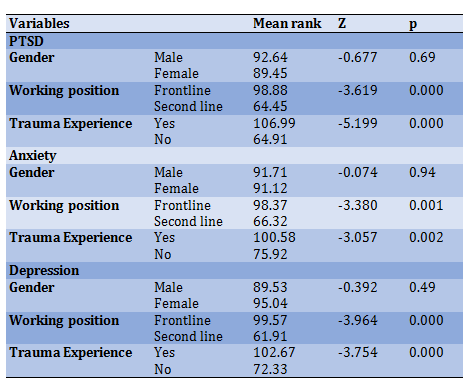
Healthcare workers in Sulaimani reported higher scores on the three scales than those in other cities, and health care workers in Halabja were the least affected. Similar to findings, frontline healthcare workers had higher scores in all three scales than second-line healthcare workers. Further, health care workers who reported having experienced a
traumatic event during their work with COVID-19 patients reported higher scores on all three scales (Table 4).
Table 5) The scores of PTSD, depression, and anxiety measurements according to age, family status, occupation, and workplace according to Kruskal-Wallis test
Discussion
This study examined the psychological impact of the COVID-19 outbreak on 182 health care workers in Iraqi Kurdistan. It was found out that nearly 53.3% of the participants screened positive for PTSD, 29.1% for anxiety, and 39.0% for depression. These results are novel since, to our knowledge, to our knowledge, this is the first study to find the psychological impact of the pandemic on health care workers in Iraqi Kurdistan. Our findings align with previous findings of a study conducted during the pandemic in China, where 53.8% reported their psychological impact of the outbreak as moderate or severe [14]. However, the result showed surprisingly higher prevalence than some of those conducted among the health care workers in Wuhan in China, in which the prevalence rates were reported to be 29.8%, 13.5%, and 24.1% for stress depression, and anxiety symptoms, respectively [8].
Moreover, the current study showed higher prevalence rates of mental health problems than those conducted on COVID-19 and SARS in Singapore [7, 15] and even higher than those conducted on SARS in China [16, 17]. Previous studies performed after the SARS pandemic and recently on COVID-19 found contradictory results concerning the presence of posttraumatic symptoms among health care workers. They potentially attributed the high prevalence of these symptoms to the lack of preparedness to face the emergency [7, 18-20]. Our findings complement previous findings, and it could be attributed to a low psychological preparedness and infection control regulation measures since this region have not experienced a highly contagious viral virus before (e.g., SARS experience) or because of the low availability of medical supplies.
In addition, we compared the prevalence of PTSD, anxiety, and depression among male and female health workers. We have found that there are no differences in the prevalence of psychological problems between males and females. However, Contrary to the findings of our study, previous studies done in China and Saudi Arabia have found that females were more affected and had higher scores across all depression, anxiety, and stress scales [1, 14, 21, 22]. Nurses, Participants aged <40 years old, those in Sulaimani, and health care workers who reported a traumatic event during their work with COVID-19 patients scored higher on all the measures. These findings align with a large cross-sectional study on 1257 health care workers in Wuhan [1], which reported the same findings. Our findings indicate concerns about the mental health of healthcare workers in Kurdistan; the psychological impacts of which might persist over a long time [16, 23, 24]. Thus, immediate response and psychosocial support, such as online intervention, are needed.
In this study, we also found out that healthcare workers who were <40 years old scored much higher than younger workers. This is perhaps because COVID-19 was repeatedly reported to have higher morbidity and mortality rates among older adults [25, 26]. Contrary to our findings, a recently published study in Iran showed that anxiety is significantly higher in the 21–40 age group [27].
In addition, the healthcare workers in the city of Sulaimani appeared to be more affected than the healthcare workers in the other places that were eligible to participate in this study. This could be because the first positive case of COVID-19 in the KRI was in Sulaimani [26], which could lead to higher levels of stress among healthcare workers. Our study also revealed higher levels of stress, depression, and anxiety in frontline healthcare workers who work directly with COVID-19. This could also be due to their close contact with patients, which increases the risk of getting infected and experiencing traumatic events.
This indicates the need for governments to adopt new strategies to improve mental health services for the community and respond to individuals' needs by emphasizing quality service delivery and evidence-based therapy to reduce the impact of COVID-19 on high-risk populations. Especially those who are first-line workers in emergencies and establishing immediate prevention programs that could be done through adopting a mental health first aid program in a timely and cost-effective manner.
In Kurdistan, few hotlines have been set up during COVID-19 to respond to mental health needs. The hotline is intended to offer psychological and counseling services to people who face psychological problems during COVID-19. Such hotlines are developed by a small number of non-governmental organizations who are working in mental health. However, the effectiveness of such services is questionable for and to date, it has not been studied. The reasons could be that; first, the focus of the ministry of health is mainly concentrated on reducing the physical and not the psychological consequences of the disease; secondly, there is a lack of psychosocial professionals who have already been trained for emergencies. Furthermore, there is no lack of media campaigns that are focused on boosting public awareness and emphasizing the importance of psychosocial interventions to prevent and reduce the psychological impact of COVID-19, targeting neither the general population nor the first-line responders who are at high risk for developing mental health problems.
The limitation of this study is the difference in the sample size across the four places. However, working on mean scores address this issue. In addition, we thought this is reasonable to include more participants in Erbil since Erbil is the capital and it is much larger than the other places. In addition to that, we included Sulaimani province, a center and an outside city. Then we believed that there might be differences between the center and a suburb city. Therefore, they remained separate in the study. We were also unable to access a larger group of health care workers due to the lockdown and banned movement between places.
Conclusion
The current study shows a high prevalence of PTSD, anxiety, and depression among healthcare responders to the COVID-19 pandemic in the KRI. The findings of this study highlight the need for immediate adaptive psychological interventions targeting healthcare workers aged above 40, nurses, and frontline workers to address the psychological impact of the COVID-19 outbreak.
Acknowledgments: We thank Wchan Foundation, Sleman Xoshnaw, Nasih Abdulraheem Rasheed, Hawkar Abubakir, and Mohammed Wali for their contribution to our study
Ethical Permissions: The code is: 1427.
Conflicts of Interests: The authors declare that they have no conflict of interest.
Authors’ Contribution: Mohammad P.J. (First Author), Introduction Writer/Methodologist/Main Researcher/
Statistical Analyst/Discussion Writer (20%); Amine S.M. (Second Author), Assistant Researcher (20%); Sabir D.K. (Third Author), Assistant Researcher (20%); Saeed F.J. (Forth Author), Assistant Researcher (20%); Hama Amin D.S. (Fifth Author), Methodologist/Assistant Researcher/
Statistical Analyst (20%).
Funding/Support: -
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the etiological agent of the coronavirus disease of 2019 (COVID-19), which first was identified in late December 2019 in the city of Wuhan in China [1]. According to World Health Organization (WHO) data, on 2020, on July 18, 86,100 confirmed cases of covid-19 and 3,500 deaths in Iraq [2]. In the Kurdistan Region of Iraq (KRI) alone, 10,595 were infected, and 402 lost their lives, according to data that was released by the Kurdistan Regional Government (KRG) on 2020, March 30 [3]. To address this critical situation, the government declared February 26 to March 10, 2020, a public holiday for all public and private schools and kindergartens. Moreover, public and private universities were closed from February 29 to March 10 and will remain closed during the spring break (10–23 March) before reopening on March 24, if the situation improves. The KRG also decided to halt all religious ceremonies, rituals, and activities-including Friday sermons-in in mosques, churches, and temples throughout the KRI until further notice. Although the lockdown duration was extended later, the healthcare workers remained at work to tackle the situation.
Healthcare workers in hospitals equipped and specialized for COVID-19; because of the direct and indirect contact with the COVID-19 patients and being vulnerable to the infection [4], they are at risk for developing mental health problems [1]. Evidence from previous studies on SARS showed that healthcare workers concern about infecting others (especially family members) than being infected themselves [4]. They also had suffered from an acute stress disorder, felt stigmatized and rejected in their neighborhood because of their hospital work, and reported reluctance to work or had considered resignation [5]. Tremendous psychological distress, particularly among healthcare workers, and increasing feelings of isolation were reported [6]. More recently, a study in Singapore examined the psychological impact of the COVID-19 outbreak on healthcare workers. Four hundred seventy healthcare workers from two major tertiary institutions participated in this study. The results showed that 30% of the healthcare workers screened positive for depression, anxiety, and stress.
Furthermore, 7.7% of the participants had clinical features of Post-Traumatic Stress Disorder (PTSD) [7]. Studies on the psychological impact of COVID-19 in China found that frontline healthcare workers, who are working with COVID-19 patients, reported stress, depression, and anxiety [1, 8, 9], as well as insomnia symptoms [1]. They have also been found to become emotionally affected and traumatized [9]. These findings from China are despite the availability of local and national mental health institutions that provide psychological support services, deployed to a large degree amid the COVID-19 outbreak. On February 2, 2020, the State Council of China announced that they were launching nationwide psychological support hotlines to assist people during the Coronavirus outbreak [10].
In the KRI, there is a lack of such actions both in normal times and during a crisis such as the COVID-19 pandemic. Psychological support services, counseling, or other professional interventions are scarce, disregarded, and not easily accessed by laypeople and healthcare workers. Additionally, the psychological impact of the COVID-19 outbreak remains largely unexplored in the region. Based on our knowledge, the current study is one of the firsts to address the psychological wellbeing of healthcare workers exposed to COVID-19 in the KRI. The current study aimed to assess the psychological impact of COVID-19 healthcare workers involved in providing medical care to the patients by identifying the levels of PTSD, anxiety, and depression. Moreover, this study aimed to assess the level of PTSD, depression, and anxiety based on gender, family status, occupation, city, and line of work.
Instrument and Methods
This descriptive study was conducted through the in-person distribution of the survey, and the data was collected from April 10, 2020, to May 20, 2020. To compare the interregional differences of mental health outcomes among healthcare workers in KRI, samples were classified by their geographic location (Erbil, Sulaimani, Chamchamal, and Halabja). Since the city of Sulaimani was the first place to be severely affected, more hospitals in this province were sampled. Hospitals equipped and specialized for COVID-19 were eligible to participate in this survey. Convenience Sampling was used in this study based on the accessibility of the sample by the authors. Healthcare workers in selected COVID-19 hospitals in three provinces; Erbil, Sulaimani; (Center, Chamchamal), and Halabja, and part of healthcare workers in those hospitals were asked to participate in this study on a convenience sampling method. Since Erbil is the largest city in Iraq's Kurdistan region, more Erbil participants were included. A total of 182 of 237 invited healthcare workers completed the survey in the four
different locations, with a participation rate of 76.8% (Table 1).
Table 1) sample size across settings
Three questionnaires were used as follow:
PTSD Checklist for DSM-5 (PCL-5): Since one of the aims of this study was to assess PTSD symptoms, the Kurdish version of PCL-5, which had been translated and adapted by a group of researchers from Bielefeld University, Germany, and Koya University, was used to assess PTSD symptoms among health care workers [11]. The PCL-5 contains twenty items rated on a five-point Likert-type scale, with options ranging from "Not at all" (0) to "Extremely" (4), and scores ranging between 0 and 80. A cut-off point of 23 would be accounted as PTSD in the Kurdish version of the PCL-5. The scale's internal consistency was reported to be high, with an alpha score of 0.89 in a study on Syrian refugees [12]. In the current study, the internal consistency of the PCL-5 was also high (alpha=0.94).
Hopkins Symptom Checklist (HSCL-25) [13]: The Kurdish version of the 25 item Hopkins symptom checklist HSCL-25, which has been translated and adapted by Heartland Alliance, was used to assess the levels of depression and anxiety. HSCL-25 is a four Likert-type scale, with options ranging from "Not at all" (1) to "Extremely" (4). The HSCL-25 contains two sections, the first section includes ten items of anxiety symptoms, and the second section includes 15 items of depression symptoms. Further, individuals with an average score greater than 1.75 in anxiety and depression are considered symptomatic. On this scale, 1.75 is considered a scientifically valid cut-off point. The depression subscale of the HSCL-25, with an alpha score of 0.86, was high internal consistency [12]. Similarly, in the present study, the depression sub-scale of the HSCL-25 showed high internal consistency (Alpha=0.85). The anxiety sub-scale had an alpha score of 0.88, indicating a high level of internal consistency.
Sociodemographic Information: Sociodemographic data were collected from the participants, including sex (male, female, or not specified), age (18-25, 26-30, 31-40, or >40 years), marital status (single, married, and divorced), occupation (physician, nurse, and lab technician), residence (inside provinces: Sulaimani and/or Erbil, outside provinces: Chamchamal and/or Halabja), place of work (inside provinces: Sulaimani and/or Erbil, outside provinces: Chamchamal and/or Halabja), technical title, working with COVID-19 patients (frontline; directly exposed and engaged in providing care to the patients, second-line; no exposure or engagement with patients yet working inside the hospitals of COVID-19). Moreover, participants were asked an additional question about whether they had experienced any traumatic events, for example, being frightened of getting the virus, witnessing a patient suffering, or any other severe humanitarian event. This was to find the differences in the PTSD, anxiety, and depression symptoms between those who respond "yes" to the trauma question and those who respond "no".
This study followed the ethical principles of the authors' institution's reporting guidelines. Approval from the research ethics committee of the Charmo University was received before the initiation of this study. Informed consent was given by all participants before their enrolment. Participants were allowed to terminate the survey at any time they desired. The survey was anonymous, and confidentiality of information was assured.
Data analysis was performed using SPSS 20.0. The original data were counted as a sum "total score" for PTSD and mean score for anxiety and depression to determine each level for symptoms of PTSD, anxiety, depression, and presented as numbers and percentages. An exploratory data analysis was carried out to determine the distribution of the scores. The scores of PTSD were not normally distributed based on the results of the Shapiro-Wilk test (p≤0.01) and Kolmogorov-Smirnov test (p≤0.05), as well as the visual inspection of Q-Q plots and histograms. Therefore, the nonparametric Mann-Whitney U test and Kruskal-Wallis test were applied to compare the severity of each disorder between two or more groups, respectively.
Findings
All 182 healthcare workers participated. Most of the participants were male, aged 31 to 40 years, married, nurse, working in Erbil, and frontline workers. Of all participants, 115 (63.2%) people reported having had a traumatic experience during their work with COVID-19 patients (Table 2).
Table 2) Results of frequency of demographic characteristics (the numbers in parentheses are in percentage)
Based on results, 53.3% of healthcare workers screened positive for PTSD, 29.1% screened positive for anxiety, and 39.0% screened positive for depression (Table 3).
There was no statistically significant difference in the symptoms of PTSD, anxiety, and depression based on gender, according to the Mann-Whitney U test (Table 4), and based on family status according to the Kruskal-Wallis test results (Table 5).
However, Kruskal-Wallis test results revealed statistically significant differences in age cohort, occupation, and workplace (p<0.05). Mann-Whitney U test results showed statistically significant differences according to work position and those who experienced traumatic events and those who did not (p<0.05). Healthcare workers who were aged >40 scored higher on PCL-5 for PTSD, and responders who were aged 26-30 years seemed least affected than other age groups p<0.02, but there were no significant differences on anxiety and depression scales (p>0.05). Similarly, Nurses reported the highest scores on the PTSD scale, and physicians reported the lowest at a significant difference level p<0.01 but no significant difference on other scales (p>0.05).
Table 3) Prevalence of PTSD, depression, and anxiety and mean HSC-25 and PCL-5 Scores in Health Care workers (N=182)
Table 4) Results of Mann-Whitney U test for comparing mean rank scores of PTSD, depression, and anxiety measurements according to gender, working position, and COVID-19 related trauma experience
Healthcare workers in Sulaimani reported higher scores on the three scales than those in other cities, and health care workers in Halabja were the least affected. Similar to findings, frontline healthcare workers had higher scores in all three scales than second-line healthcare workers. Further, health care workers who reported having experienced a
traumatic event during their work with COVID-19 patients reported higher scores on all three scales (Table 4).
Table 5) The scores of PTSD, depression, and anxiety measurements according to age, family status, occupation, and workplace according to Kruskal-Wallis test
Discussion
This study examined the psychological impact of the COVID-19 outbreak on 182 health care workers in Iraqi Kurdistan. It was found out that nearly 53.3% of the participants screened positive for PTSD, 29.1% for anxiety, and 39.0% for depression. These results are novel since, to our knowledge, to our knowledge, this is the first study to find the psychological impact of the pandemic on health care workers in Iraqi Kurdistan. Our findings align with previous findings of a study conducted during the pandemic in China, where 53.8% reported their psychological impact of the outbreak as moderate or severe [14]. However, the result showed surprisingly higher prevalence than some of those conducted among the health care workers in Wuhan in China, in which the prevalence rates were reported to be 29.8%, 13.5%, and 24.1% for stress depression, and anxiety symptoms, respectively [8].
Moreover, the current study showed higher prevalence rates of mental health problems than those conducted on COVID-19 and SARS in Singapore [7, 15] and even higher than those conducted on SARS in China [16, 17]. Previous studies performed after the SARS pandemic and recently on COVID-19 found contradictory results concerning the presence of posttraumatic symptoms among health care workers. They potentially attributed the high prevalence of these symptoms to the lack of preparedness to face the emergency [7, 18-20]. Our findings complement previous findings, and it could be attributed to a low psychological preparedness and infection control regulation measures since this region have not experienced a highly contagious viral virus before (e.g., SARS experience) or because of the low availability of medical supplies.
In addition, we compared the prevalence of PTSD, anxiety, and depression among male and female health workers. We have found that there are no differences in the prevalence of psychological problems between males and females. However, Contrary to the findings of our study, previous studies done in China and Saudi Arabia have found that females were more affected and had higher scores across all depression, anxiety, and stress scales [1, 14, 21, 22]. Nurses, Participants aged <40 years old, those in Sulaimani, and health care workers who reported a traumatic event during their work with COVID-19 patients scored higher on all the measures. These findings align with a large cross-sectional study on 1257 health care workers in Wuhan [1], which reported the same findings. Our findings indicate concerns about the mental health of healthcare workers in Kurdistan; the psychological impacts of which might persist over a long time [16, 23, 24]. Thus, immediate response and psychosocial support, such as online intervention, are needed.
In this study, we also found out that healthcare workers who were <40 years old scored much higher than younger workers. This is perhaps because COVID-19 was repeatedly reported to have higher morbidity and mortality rates among older adults [25, 26]. Contrary to our findings, a recently published study in Iran showed that anxiety is significantly higher in the 21–40 age group [27].
In addition, the healthcare workers in the city of Sulaimani appeared to be more affected than the healthcare workers in the other places that were eligible to participate in this study. This could be because the first positive case of COVID-19 in the KRI was in Sulaimani [26], which could lead to higher levels of stress among healthcare workers. Our study also revealed higher levels of stress, depression, and anxiety in frontline healthcare workers who work directly with COVID-19. This could also be due to their close contact with patients, which increases the risk of getting infected and experiencing traumatic events.
This indicates the need for governments to adopt new strategies to improve mental health services for the community and respond to individuals' needs by emphasizing quality service delivery and evidence-based therapy to reduce the impact of COVID-19 on high-risk populations. Especially those who are first-line workers in emergencies and establishing immediate prevention programs that could be done through adopting a mental health first aid program in a timely and cost-effective manner.
In Kurdistan, few hotlines have been set up during COVID-19 to respond to mental health needs. The hotline is intended to offer psychological and counseling services to people who face psychological problems during COVID-19. Such hotlines are developed by a small number of non-governmental organizations who are working in mental health. However, the effectiveness of such services is questionable for and to date, it has not been studied. The reasons could be that; first, the focus of the ministry of health is mainly concentrated on reducing the physical and not the psychological consequences of the disease; secondly, there is a lack of psychosocial professionals who have already been trained for emergencies. Furthermore, there is no lack of media campaigns that are focused on boosting public awareness and emphasizing the importance of psychosocial interventions to prevent and reduce the psychological impact of COVID-19, targeting neither the general population nor the first-line responders who are at high risk for developing mental health problems.
The limitation of this study is the difference in the sample size across the four places. However, working on mean scores address this issue. In addition, we thought this is reasonable to include more participants in Erbil since Erbil is the capital and it is much larger than the other places. In addition to that, we included Sulaimani province, a center and an outside city. Then we believed that there might be differences between the center and a suburb city. Therefore, they remained separate in the study. We were also unable to access a larger group of health care workers due to the lockdown and banned movement between places.
Conclusion
The current study shows a high prevalence of PTSD, anxiety, and depression among healthcare responders to the COVID-19 pandemic in the KRI. The findings of this study highlight the need for immediate adaptive psychological interventions targeting healthcare workers aged above 40, nurses, and frontline workers to address the psychological impact of the COVID-19 outbreak.
Acknowledgments: We thank Wchan Foundation, Sleman Xoshnaw, Nasih Abdulraheem Rasheed, Hawkar Abubakir, and Mohammed Wali for their contribution to our study
Ethical Permissions: The code is: 1427.
Conflicts of Interests: The authors declare that they have no conflict of interest.
Authors’ Contribution: Mohammad P.J. (First Author), Introduction Writer/Methodologist/Main Researcher/
Statistical Analyst/Discussion Writer (20%); Amine S.M. (Second Author), Assistant Researcher (20%); Sabir D.K. (Third Author), Assistant Researcher (20%); Saeed F.J. (Forth Author), Assistant Researcher (20%); Hama Amin D.S. (Fifth Author), Methodologist/Assistant Researcher/
Statistical Analyst (20%).
Funding/Support: -
Article Type: Descriptive & Survey |
Subject:
Health Education and Health Behavior
Received: 2021/04/24 | Accepted: 2021/08/2 | Published: 2021/11/6
Received: 2021/04/24 | Accepted: 2021/08/2 | Published: 2021/11/6
References
1. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. 2020;3(3):203976. [Link] [DOI:10.1001/jamanetworkopen.2020.3976] [PMID] [PMCID]
2. World health organization. Coronavirus explorer the data [Internet]. Geneva: World Health Organization; 2021 [cited 2021 June 25]. Available from: https://covid19.who.int/explorer/. [Link]
3. Kurdistan regional government. Latest information about COVID-19 [Internet]. Erbil: Kurdistan Regional Government; 2021 [cited 2021 June 25]. Available from: https://gov.krd/coronavirus-en/situation-update/. [Link]
4. Ho SMY, Kwong-Lo RSY, Mak CWY, Wong JS. Fear of severe acute respiratory syndrome (SARS) among health care workers. J Consult Clin Psychol. 2005;73(2):344-9. [Link] [DOI:10.1037/0022-006X.73.2.344] [PMID]
5. Bai Y, Lin CC, Lin CY, Chen JY, Chue CM, Chou P. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr Serv. 2004;55(9):1055-7. [Link] [DOI:10.1176/appi.ps.55.9.1055] [PMID]
6. Maunder R, Hunter J, Vincent L, Bennett J, Peladeau N, Leszcz M, et al. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ. 2003;168(10):1245-51. [Link]
7. Tan BYQ, Chew NWS, Lee GKH, Jing M, Goh Y, Yeo LL, et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann Intern Med. 2020;173(4):317-20. [Link] [DOI:10.7326/M20-1083] [PMID] [PMCID]
8. Zhu Z, Xu S, Wang H, Liu Z, Wu J, Li G et al. COVID-19 in Wuhan: Sociodemographic characteristics and hospital support measures associated with the immediate psychological impact on healthcare workers. Lancet. 2020;24:100443. [Link] [DOI:10.1016/j.eclinm.2020.100443] [PMID] [PMCID]
9. Ho CS, Chee CY, Ho R.C. Mental health strategies to combat the psychological impact of coronavirus disease 2019 (COVID-19) beyond paranoia and panic. Ann Acad Med Singap. 2020;49(3):155-60. [Link] [DOI:10.47102/annals-acadmedsg.202043]
10. The State Council issued a notice on the joint prevention and control mechanism for the pneumonia epidemic caused by the new coronavirus infection: Establishing a psychological assistance hotline in response to the epidemic [Internet]. Beijing: Gov.cn; 2021 [cited 2021 June 26]. Available from: http://www.gov.cn/xinwen/2020-02/02/content_5473937.htm. [Link]
11. Ibrahim H, Ertl V, Catani C, Ismail A, Neuner F. The validity of posttraumatic stress disorder checklist for DSM-5 (PCL-5) as screening instrument with Kurdish and Arab displaced populations living in the Kurdistan region of Iraq. BMC Psychiatry. 2018;18(1):259. [Link] [DOI:10.1186/s12888-018-1839-z] [PMID] [PMCID]
12. Mahmood HN, Ibrahim H, Goessmann K, Ismail AA, Neuner F. Post-traumatic stress disorder and depression among Syrian refugees residing in the Kurdistan region of Iraq. Confl Health. 2019;13:51. [Link] [DOI:10.1186/s13031-019-0238-5] [PMID] [PMCID]
13. Hesbacher P, Rickels K, Morris R, Newman H, Rosenfeld H. Psychiatric illness in family practice. J Clin Psychiatry. 1980;41:6-10. [Link]
14. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. [Link] [DOI:10.3390/ijerph17051729] [PMID] [PMCID]
15. Sin S, Thompson DR. Psychological impact of the SARS outbreak on a Singaporean rehabilitation department. Int J Ther Rehabil. 2004;11(9):417-24. [Link] [DOI:10.12968/ijtr.2004.11.9.19589]
16. Wu P, Fang Y, Guan Z, Fan B, Kong J, Yao Z, et al. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Can J Psychiatry. 2009;54(5):302-11. [Link] [DOI:10.1177/070674370905400504] [PMID] [PMCID]
17. Maunder R. The experience of the 2003 SARS outbreak as a traumatic stress among frontline healthcare workers in Toronto: Lessons learned. Philos Trans R Soc Lond B Biol Sci. 2004;359(1447):1117-25. [Link] [DOI:10.1098/rstb.2004.1483] [PMID] [PMCID]
18. Chan AOM, Huak CY. Psychological impact of the 2003 severe acute respiratory syndrome outbreak on health care workers in a medium size regional general hospital in Singapore. Occup Med. 2004;54(3):190-6. [Link] [DOI:10.1093/occmed/kqh027] [PMID] [PMCID]
19. Lee AM, Wong JG, McAlonan GM, Cheung V, Cheung C, Sham PC, et al. stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiatry. 2007;52(4):233-40. [Link] [DOI:10.1177/070674370705200405] [PMID]
20. Giusti EM, Pedroli E, D'Aniello GE, Badiale CS, Pietrabissa G, Manna C, et al. The psychological impact of the COVID-19 outbreak on health professionals: A cross-sectional study. Front Psychol. 2020;11:1684. [Link] [DOI:10.3389/fpsyg.2020.01684] [PMID] [PMCID]
21. Liu N, Zhang F, Wei C, Jia Y, Shang Z, Sun L, et al. prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020;287:112921. [Link] [DOI:10.1016/j.psychres.2020.112921] [PMID] [PMCID]
22. Alkhamees AA, Alrashed SA, Alzunaydi AA, Almohimeed AS, Aljohani MS. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr Psychiatry. 2020;102:152192. [Link] [DOI:10.1016/j.comppsych.2020.152192] [PMID] [PMCID]
23. North CS, Pfefferbaum B, Tivis L, Aya K, Reddy C, Spitznagel EL. The course of posttraumatic stress disorder in a follow-up study of survivors of the Oklahoma city bombing. Ann Clin Psychiatry. 2004;16(4):209-15. [Link] [DOI:10.1080/10401230490522034] [PMID]
24. Sim K, Chua HC. The psychological impact of SARS: A matter of heart and mind. CMAJ. 2004;170(5):811-2. [Link] [DOI:10.1503/cmaj.1032003] [PMID] [PMCID]
25. Sidiq KR, Sabir DK, Ali SM, Kodzius R. Does early childhood vaccination protect against COVID-19. Front Mol Biosci. 2020;7:120. [Link] [DOI:10.3389/fmolb.2020.00120] [PMID] [PMCID]
26. Sabir DK, Sidiq KR, Abdullah HM, Ali SM, Khwarahm NR. Factors contributing to the containment of the COVID-19 in Kurdistan region of Iraq. Adv Emerg Med. 2020;4(2):47. [Link]
27. Moghanibashi-Mansourieh A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J Psychiatry. 2020;51:102076. [Link] [DOI:10.1016/j.ajp.2020.102076] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |