



Volume 9, Issue 2 (2021)
Health Educ Health Promot 2021, 9(2): 135-140 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mashhadi S, Hosseinkhani S, Heidari M, Norouzadeh R. Impact of Family Support Program on Depression of Family Caregiver of Hospitalized Patients in Cardiac Intensive Care Unit. Health Educ Health Promot 2021; 9 (2) :135-140
URL: http://hehp.modares.ac.ir/article-5-47804-en.html
URL: http://hehp.modares.ac.ir/article-5-47804-en.html
1- Department of Nursing, Faculty of Nursing and Midwifery, Shahed University, Tehran, Iran
2- Department of Nursing, Faculty of Nursing and Midwifery, Shahed University, Tehran, Iran ,hosseinkhani@shahed.ac.ir
2- Department of Nursing, Faculty of Nursing and Midwifery, Shahed University, Tehran, Iran ,
Full-Text [PDF 409 kb]
(1664 Downloads)
| Abstract (HTML) (1446 Views)
Full-Text: (324 Views)
Introduction
Cardiovascular disease is one of the most common diseases leading to hospitalization and is the cause of 30% of deaths [1]. The hospitalization of these patients in the intensive care unit always puts much tension on the family [2]. In such situations, the family plays an important role in maintaining the patient's health and well-being [3]. Paying attention to the family is an important issue as the family is often responsible for supporting the patient [4]. Studies show that the families of ICU patients always suffer from psychological problems such as anxiety, depression, post-traumatic stress disorder (PTSD), or post-intensive care syndrome (PICS), which significantly affect the quality of life of the family socially and emotionally [5]. For example, Kourti et al. found that more than 60% of the families of patients admitted to the intensive care unit show symptoms of anxiety and depression [6]. According to Pochard et al.'s studies, over 75% of the family members of the patients hospitalized in the intensive care unit suffer symptoms of anxiety and severe depression [7]. Depression is a sickening sad feeling that includes low mood, indifference, and dissatisfaction with the surroundings [8]. One of the psychological symptoms of these families is depression. Depression as a variety of symptoms includes low mood, indifference, and dissatisfaction with the environment. Depression has been shown to affect family caregivers whose patients are admitted to the ICU due to open-heart surgery, impairing the ability to understand information correctly and making it difficult for them to make decisions about the patient [9]. Regarding the symptoms of depression in the relatives of patients admitted to the intensive care unit, Bolosi et al. suggest that during the first week of hospitalization in the ICU, depressive symptoms in patients' relatives gradually increase [10]. Therefore, in such a situation of emotional turmoil in the family, nurses must prioritize addressing the psychological needs of the family [11].
Considering the families' psychological needs admitted to the cardiac intensive care unit, Dalirirad et al. point out that families show emotional reactions to the stress of cardiac surgery. For this reason, families need long-term help and support [12]. Nurses have an important role in identifying and meeting the needs of the patient's family. These needs are information, trust, continuity, support, and convenience [5]. Also, Maxwell et al. categorized the needs of family members of critically ill patients' assurance, proximity, information, comfort, and support [13]. One of the effective ways to support the families of patients admitted to the intensive care unit is information support. Information support is structured interventions emphasizing family needs to enhance family knowledge about patient conditions using problem-solving and communication skills [14]. Informational support can be provided in the form of counseling, face-to-face individual or group training, and the distribution of booklets or educational pamphlets in oral or written form. One of the tasks of nurses to support distressed families is to provide timely and carefully planned information about the patient's condition [15]. Also, Farzadmehr et al. considered nursing counseling with family and other supportive measures as a good solution to increase satisfaction and reduce the stress on the family of cardiac surgery patients admitted to the intensive care unit [16]. Studies on the methods of informing the families of critically ill patients indicate the challenge of nurses to address the needs of stressed family members. Failure to provide information support to the family leads to the family's further helplessness and psychological vulnerability; families who are in a state of ambiguity about the patient's outcome and their role during the patient's stay in the ICU. Ölçüm et al., the families of heart surgery patients in the ICU, determine the information needs of the patient's spouses were higher than other family members, and depression rate was higher than other non-consanguineous relatives [17].
In explaining the family experiences of heart surgery patients on information and support when serious complications occur after cardiac surgery, how the family informed determined as a basis for fruitful conversations between family and the healthcare professionals [18]. Evidence suggests that giving information to the families of patients admitted to the cardiac intensive care unit is particularly crucial to prevent or reduce family psychological stress caused by the patient's hospitalization. Because depression, as a serious emotional disorder, can overshadow the performance of family caregivers during the patient's stay in the hospital and even in the rehabilitation phase after discharge, nurses need to support the family information needs with appropriate strategy adequately. In this regard, the authors decided to investigate the impact of family support programs on depression in the family caregiver of patients admitted to the cardiac intensive care unit.
Materials and Methods
This quasi-experimental study was conducted in the cardiac intensive care unit of Sevom Shaban hospital in Damavand, Tehran, in 2019. Participants included families of patients with a history of the first admission to the cardiac intensive care unit (CICU) were recruited using the simple random sampling method. The required number of samples was calculated based on a study conducted by Zakeri Moghadam et al. [19]. The sample size was calculated based on the formula for comparing means (a=5%), 80 % power (b=20%). Considering 10% of attrition in samples, a total of 60 families (30 cases for each group) were selected. Inclusion criteria include no history of previous hospitalization of the patient in the cardiac intensive care unit and family without psychiatric problems or taking over-the-counter sedatives. The family caregivers that were members of the health care providers were excluded.
The demographic data sheet and the anxiety and depression questionnaire (HADS) were completed twice by the family. The Anxiety and Depression Questionnaire includes seven items (items 1, 4, 5, 8, 9, 12, 13) for anxiety symptoms and seven items (items 2, 3, 6, 7, 10, 11, and 14) for depressive symptoms. The anxiety and depression questionnaire (HADS) is scored based on a four-point Likert scale from zero to 3. Accordingly, the maximum score of family depression and anxiety is 42. The cut-off point of the questionnaire is 11, the higher values of which are clinically significant for anxiety or depression. The reliability and validity of Anxiety and Depression Hospital Scales (HADS) were confirmed by Kaviani et al. [20]. The reliability coefficient for the depression subscale is reported to be 0.7. The time required to complete the questionnaires was 10 minutes approximately.
The researchers had received permission from the ethics committee of Shahed University. Then, coordination was made with the director and matron of the Sevom Shaban hospital, Damavand, Tehran province. Families were informed verbally of the aim of the study, voluntary participation, anonymity, confidentiality of information, and the right to withdraw from the research at the time of the request. The educational brochure was provided to the control group when the support program was performed on the intervention group, and the families of the intervention group were provided with face-to-face question and answer training, and at the end of the intervention, they were given an educational booklet. A preliminary review was used to create educational content using checklists and open-ended questions. Most family caregivers were not aware of the nature of heart disease, prognosis, and length of hospital stay, medications, home care, and how to act during a heart attack; therefore, the content of the educational booklet was prepared based on the needs of the family review the literature. Content validity was confirmed by four nursing faculty members. The educational content included the reason for hospitalization, explanation of the disease, treatment process, familiarity with the environment, consultation program with a specialist, medication, physical needs, nutrition, activity, crisis adaptation methods, management of anxiety and depression. The duration of the intervention was a maximum of one hour in one session. After the education, a question and answer session was conducted, and an educational booklet was given to the family to ensure that they learned the material. The questionnaire was completed in the first 24 hours and on the third day of hospitalization.
In variables with normal distribution, an independent sample t-test was used to compare the mean of quantitative variables at any time between the control and intervention groups. Paired t-test was used to compare the mean of these variables within the groups before and after the intervention. Also in quantitative variables without normal distribution, Mann-Whitney and Wilcoxon tests were used by SPSS 18 software. The significance level in this study was set at p<0.05.
Findings
In this study, the mean±SD age of family caregivers in the control and intervention group was 41.10±12.34 and 39.83±10.20 years, respectively. Before the intervention, both groups were homogeneous in terms of other demographic variables (p>0.05; Table 1).
Before the intervention, the depression score in the families of patients admitted to the cardiac intensive care unit was not normally distributed (p<0.05), and both groups were homogeneous in terms of depression and did not differ significantly before the intervention (p=0.37; Table 2). Depression score after the intervention was significantly different, indicating the effect of support program intervention (p=0.02; Table 2).
Table 1) Comparison of the frequency (the numbers in parentheses are percent) of the demographic variables related to the family members of the patients between two groups

Table 2) Result of depression score before and after the intervention in the families of patients admitted to the cardiac intensive care unit (n=30 in each group)
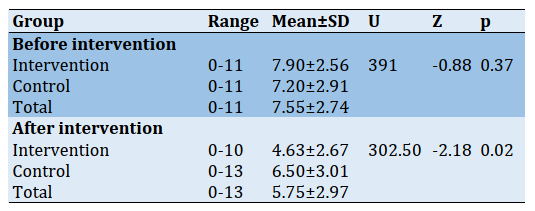
In the intervention group, Wilcoxon signed-rank test showed a downtrend in depression from the intermediate dysfunction to the normal level (p=0.001). In the control group, the rate of depression reached an intermediate level but was not statistically significant (p=0.08). After the information support intervention, the two groups of the family had a significant difference in the depression. The effect size was moderate (Cohens'd=0.59). According to the Wilcoxon signed-rank test, the depression level in the intervention group was significantly reduced. In order to prevent type 1 error and to determine the effect of the intervention, the test of generalized estimation equations was used at zero time, and it was found that the information support has a significant effect on reducing depression in patients' families admitted to the cardiac intensive care unit (p=0.001).
Discussion
This study investigates the effect of informational support on depression in the families of patients admitted to the cardiac intensive care unit. According to the findings, information support reduces the depression of families during the patient's hospitalization in the intensive care unit. In the intervention group, the level of depression decreased and reached an intermediate level of normal. The results showed a statistically significant difference in the families in the intervention group in terms of depression on the first day of hospitalization and the third day of hospitalization. However, the decreasing trend of depression to normal is not noticeable in the control group. This finding highlights the effective role of information support intervention in reducing depression in the families of patients admitted to the cardiac intensive care unit. Consistent with this finding, Navidian et al., in a study on family members of hospitalized patients at the ICU in the trauma center, suggest that after the educational-supportive intervention, the mean change score of depression of family was significantly higher than the control group [21]. As studies emphasize, the patient and family are under severe stress from critical conditions, and the patient's life is threatened. In this situation, providing specialized stress-relieving care is an important requirement for this group of clients [5]. One of the most important issues for intensive care nurses is considering the family's prominent role as a caregiver for the patient admitted to the intensive care unit. Given the need for family involvement in decision-making for the hospitalized patient, educational and informational support can be helpful. Informational support for patients' families will help them better adapt while facing a stressful situation and hospitalization crisis. Informational support of families increases the level of awareness, reduces the stress and depression of families. One of our study's desirable characteristics is the preparation of an information support program based on initial needs of the patient's family admitted to the cardiac intensive care unit (i.e., nature of heart disease, prognosis, and length of hospital stay, medications, and home care). In this regard, Chien et al. examine the effect of a needs-based education programmed within the first three days of patients' hospitalization on the families of newly admitted critically ill patients and confirm the effectiveness of a needs-based educational intervention to satisfy immediate psychosocial needs [22].
Regarding the effect of information support programs on family depression, there are similar studies. For example, in the study of Zakeri Moghadam et al., a Supportive nursing Program including informational and emotional support reduced the level of depression of family members at the end of coronary bypass surgery [19]. Although the present study's focus is on the variable of depression, as other studies show, the information support program can reduce other psychological aspects of the patient's family admitted to the ICU. Studies such as Jabbarpour et al. suggest that face-to-face informational programs can reduce the anxiety of family members of patients with traumatic brain injury [15]. In this study, two methods of face-to-face question education an educational booklet show a significant effect on the depression of the families. Azouley et al. showed that in addition to standard information, providing an ICU family information leaflet including general information on the ICU and hospital, the name of the ICU physician, a diagram of the ICU room, and the devices and common terminology used in ICUs can improve the families' comprehension of the provided information [23]. The present study shows the effect of information support program intervention on the day of admission up to 72 hours after hospitalization. The results show a significant reduction in family depression over time. As mentioned in the findings section, this decrease is higher in the intervention group. In line with this study, Shoushi et al. investigate the impact of family support programs on depression, anxiety, stress, and satisfaction in the open-heart surgery patients' family members at different time intervals. The finding shows the family in both groups had lower depression at 24h before and 14 days after the patient's discharge. Similar to our study, this study reveals that the family in the intervention group shows a greater decrease than the control group in terms of the mean score of depression [24].
One of the limitations of this study is that the effect of the intervention on depression in the families of patients admitted to the cardiac intensive care unit has been investigated only in the only medical center, which limits the generalizability of the results. The second limitation is the difference in the demographic characteristics of the families, which can affect their responses to the questionnaire. Finally, the duration of the study is limited to the first three days of the patient's hospitalization. Increasing the duration of family presence due to the longer hospital stay can affect the rate and fluctuations of family depression. It is necessary to pay attention to this issue in future studies. The present study could help the family during hospitalization and before discharge, followed by a sense of satisfaction and comfort and consequently less depression in the family of heart patients. In the family-centered care approaches, nurses can plan information support as a suitable psychological modality for the family and implement it coherently in intensive care units.
Conclusion
Informational support by providing comprehensive educational content orally and face to face along with question-answer sessions for patients' caregivers increases the family awareness of the conditions and decreases the depression among families during the stay of patients in the cardiac intensive care unit.
Acknowledgments: we need to thank all the professors of the Faculty of Nursing of Shahed University and the esteemed staff of the heart ward of the hospital cardiac care units in Sevome Shaban Damavand and the esteemed families who have accompanied us in the implementation of this study.
Ethical Permissions: The code of ethics IR.SHAHED.REC.1398.047.
Conflicts of Interests: The present study is taken from the master's thesis of nursing in the Faculty of nursing and midwifery of shahed University entitled "The effect of information support on anxiety and depression of caregivers of the family of hospitalized patients in cardiac care unit" and the authors declare that there is no conflict of interest.
Authors' Contribution: Mashhadi S.S. (First author), Methodologist/Original researcher/Statistical analyst/
Discussion author (30%); Hosseinkhani S.N. (Second author), Introduction author/Original researcher/
Discussion author (30%); Heidari M. (Third author), Methodologist/ Original researcher/Discussion author (20%); Norouzadeh R (Fourth author), Introduction author/Discussion author (20%).
Funding/Sources: The authors received no financial support for the research, authorship, and/or publication of this article.
Cardiovascular disease is one of the most common diseases leading to hospitalization and is the cause of 30% of deaths [1]. The hospitalization of these patients in the intensive care unit always puts much tension on the family [2]. In such situations, the family plays an important role in maintaining the patient's health and well-being [3]. Paying attention to the family is an important issue as the family is often responsible for supporting the patient [4]. Studies show that the families of ICU patients always suffer from psychological problems such as anxiety, depression, post-traumatic stress disorder (PTSD), or post-intensive care syndrome (PICS), which significantly affect the quality of life of the family socially and emotionally [5]. For example, Kourti et al. found that more than 60% of the families of patients admitted to the intensive care unit show symptoms of anxiety and depression [6]. According to Pochard et al.'s studies, over 75% of the family members of the patients hospitalized in the intensive care unit suffer symptoms of anxiety and severe depression [7]. Depression is a sickening sad feeling that includes low mood, indifference, and dissatisfaction with the surroundings [8]. One of the psychological symptoms of these families is depression. Depression as a variety of symptoms includes low mood, indifference, and dissatisfaction with the environment. Depression has been shown to affect family caregivers whose patients are admitted to the ICU due to open-heart surgery, impairing the ability to understand information correctly and making it difficult for them to make decisions about the patient [9]. Regarding the symptoms of depression in the relatives of patients admitted to the intensive care unit, Bolosi et al. suggest that during the first week of hospitalization in the ICU, depressive symptoms in patients' relatives gradually increase [10]. Therefore, in such a situation of emotional turmoil in the family, nurses must prioritize addressing the psychological needs of the family [11].
Considering the families' psychological needs admitted to the cardiac intensive care unit, Dalirirad et al. point out that families show emotional reactions to the stress of cardiac surgery. For this reason, families need long-term help and support [12]. Nurses have an important role in identifying and meeting the needs of the patient's family. These needs are information, trust, continuity, support, and convenience [5]. Also, Maxwell et al. categorized the needs of family members of critically ill patients' assurance, proximity, information, comfort, and support [13]. One of the effective ways to support the families of patients admitted to the intensive care unit is information support. Information support is structured interventions emphasizing family needs to enhance family knowledge about patient conditions using problem-solving and communication skills [14]. Informational support can be provided in the form of counseling, face-to-face individual or group training, and the distribution of booklets or educational pamphlets in oral or written form. One of the tasks of nurses to support distressed families is to provide timely and carefully planned information about the patient's condition [15]. Also, Farzadmehr et al. considered nursing counseling with family and other supportive measures as a good solution to increase satisfaction and reduce the stress on the family of cardiac surgery patients admitted to the intensive care unit [16]. Studies on the methods of informing the families of critically ill patients indicate the challenge of nurses to address the needs of stressed family members. Failure to provide information support to the family leads to the family's further helplessness and psychological vulnerability; families who are in a state of ambiguity about the patient's outcome and their role during the patient's stay in the ICU. Ölçüm et al., the families of heart surgery patients in the ICU, determine the information needs of the patient's spouses were higher than other family members, and depression rate was higher than other non-consanguineous relatives [17].
In explaining the family experiences of heart surgery patients on information and support when serious complications occur after cardiac surgery, how the family informed determined as a basis for fruitful conversations between family and the healthcare professionals [18]. Evidence suggests that giving information to the families of patients admitted to the cardiac intensive care unit is particularly crucial to prevent or reduce family psychological stress caused by the patient's hospitalization. Because depression, as a serious emotional disorder, can overshadow the performance of family caregivers during the patient's stay in the hospital and even in the rehabilitation phase after discharge, nurses need to support the family information needs with appropriate strategy adequately. In this regard, the authors decided to investigate the impact of family support programs on depression in the family caregiver of patients admitted to the cardiac intensive care unit.
Materials and Methods
This quasi-experimental study was conducted in the cardiac intensive care unit of Sevom Shaban hospital in Damavand, Tehran, in 2019. Participants included families of patients with a history of the first admission to the cardiac intensive care unit (CICU) were recruited using the simple random sampling method. The required number of samples was calculated based on a study conducted by Zakeri Moghadam et al. [19]. The sample size was calculated based on the formula for comparing means (a=5%), 80 % power (b=20%). Considering 10% of attrition in samples, a total of 60 families (30 cases for each group) were selected. Inclusion criteria include no history of previous hospitalization of the patient in the cardiac intensive care unit and family without psychiatric problems or taking over-the-counter sedatives. The family caregivers that were members of the health care providers were excluded.
The demographic data sheet and the anxiety and depression questionnaire (HADS) were completed twice by the family. The Anxiety and Depression Questionnaire includes seven items (items 1, 4, 5, 8, 9, 12, 13) for anxiety symptoms and seven items (items 2, 3, 6, 7, 10, 11, and 14) for depressive symptoms. The anxiety and depression questionnaire (HADS) is scored based on a four-point Likert scale from zero to 3. Accordingly, the maximum score of family depression and anxiety is 42. The cut-off point of the questionnaire is 11, the higher values of which are clinically significant for anxiety or depression. The reliability and validity of Anxiety and Depression Hospital Scales (HADS) were confirmed by Kaviani et al. [20]. The reliability coefficient for the depression subscale is reported to be 0.7. The time required to complete the questionnaires was 10 minutes approximately.
The researchers had received permission from the ethics committee of Shahed University. Then, coordination was made with the director and matron of the Sevom Shaban hospital, Damavand, Tehran province. Families were informed verbally of the aim of the study, voluntary participation, anonymity, confidentiality of information, and the right to withdraw from the research at the time of the request. The educational brochure was provided to the control group when the support program was performed on the intervention group, and the families of the intervention group were provided with face-to-face question and answer training, and at the end of the intervention, they were given an educational booklet. A preliminary review was used to create educational content using checklists and open-ended questions. Most family caregivers were not aware of the nature of heart disease, prognosis, and length of hospital stay, medications, home care, and how to act during a heart attack; therefore, the content of the educational booklet was prepared based on the needs of the family review the literature. Content validity was confirmed by four nursing faculty members. The educational content included the reason for hospitalization, explanation of the disease, treatment process, familiarity with the environment, consultation program with a specialist, medication, physical needs, nutrition, activity, crisis adaptation methods, management of anxiety and depression. The duration of the intervention was a maximum of one hour in one session. After the education, a question and answer session was conducted, and an educational booklet was given to the family to ensure that they learned the material. The questionnaire was completed in the first 24 hours and on the third day of hospitalization.
In variables with normal distribution, an independent sample t-test was used to compare the mean of quantitative variables at any time between the control and intervention groups. Paired t-test was used to compare the mean of these variables within the groups before and after the intervention. Also in quantitative variables without normal distribution, Mann-Whitney and Wilcoxon tests were used by SPSS 18 software. The significance level in this study was set at p<0.05.
Findings
In this study, the mean±SD age of family caregivers in the control and intervention group was 41.10±12.34 and 39.83±10.20 years, respectively. Before the intervention, both groups were homogeneous in terms of other demographic variables (p>0.05; Table 1).
Before the intervention, the depression score in the families of patients admitted to the cardiac intensive care unit was not normally distributed (p<0.05), and both groups were homogeneous in terms of depression and did not differ significantly before the intervention (p=0.37; Table 2). Depression score after the intervention was significantly different, indicating the effect of support program intervention (p=0.02; Table 2).
Table 1) Comparison of the frequency (the numbers in parentheses are percent) of the demographic variables related to the family members of the patients between two groups
Table 2) Result of depression score before and after the intervention in the families of patients admitted to the cardiac intensive care unit (n=30 in each group)
In the intervention group, Wilcoxon signed-rank test showed a downtrend in depression from the intermediate dysfunction to the normal level (p=0.001). In the control group, the rate of depression reached an intermediate level but was not statistically significant (p=0.08). After the information support intervention, the two groups of the family had a significant difference in the depression. The effect size was moderate (Cohens'd=0.59). According to the Wilcoxon signed-rank test, the depression level in the intervention group was significantly reduced. In order to prevent type 1 error and to determine the effect of the intervention, the test of generalized estimation equations was used at zero time, and it was found that the information support has a significant effect on reducing depression in patients' families admitted to the cardiac intensive care unit (p=0.001).
Discussion
This study investigates the effect of informational support on depression in the families of patients admitted to the cardiac intensive care unit. According to the findings, information support reduces the depression of families during the patient's hospitalization in the intensive care unit. In the intervention group, the level of depression decreased and reached an intermediate level of normal. The results showed a statistically significant difference in the families in the intervention group in terms of depression on the first day of hospitalization and the third day of hospitalization. However, the decreasing trend of depression to normal is not noticeable in the control group. This finding highlights the effective role of information support intervention in reducing depression in the families of patients admitted to the cardiac intensive care unit. Consistent with this finding, Navidian et al., in a study on family members of hospitalized patients at the ICU in the trauma center, suggest that after the educational-supportive intervention, the mean change score of depression of family was significantly higher than the control group [21]. As studies emphasize, the patient and family are under severe stress from critical conditions, and the patient's life is threatened. In this situation, providing specialized stress-relieving care is an important requirement for this group of clients [5]. One of the most important issues for intensive care nurses is considering the family's prominent role as a caregiver for the patient admitted to the intensive care unit. Given the need for family involvement in decision-making for the hospitalized patient, educational and informational support can be helpful. Informational support for patients' families will help them better adapt while facing a stressful situation and hospitalization crisis. Informational support of families increases the level of awareness, reduces the stress and depression of families. One of our study's desirable characteristics is the preparation of an information support program based on initial needs of the patient's family admitted to the cardiac intensive care unit (i.e., nature of heart disease, prognosis, and length of hospital stay, medications, and home care). In this regard, Chien et al. examine the effect of a needs-based education programmed within the first three days of patients' hospitalization on the families of newly admitted critically ill patients and confirm the effectiveness of a needs-based educational intervention to satisfy immediate psychosocial needs [22].
Regarding the effect of information support programs on family depression, there are similar studies. For example, in the study of Zakeri Moghadam et al., a Supportive nursing Program including informational and emotional support reduced the level of depression of family members at the end of coronary bypass surgery [19]. Although the present study's focus is on the variable of depression, as other studies show, the information support program can reduce other psychological aspects of the patient's family admitted to the ICU. Studies such as Jabbarpour et al. suggest that face-to-face informational programs can reduce the anxiety of family members of patients with traumatic brain injury [15]. In this study, two methods of face-to-face question education an educational booklet show a significant effect on the depression of the families. Azouley et al. showed that in addition to standard information, providing an ICU family information leaflet including general information on the ICU and hospital, the name of the ICU physician, a diagram of the ICU room, and the devices and common terminology used in ICUs can improve the families' comprehension of the provided information [23]. The present study shows the effect of information support program intervention on the day of admission up to 72 hours after hospitalization. The results show a significant reduction in family depression over time. As mentioned in the findings section, this decrease is higher in the intervention group. In line with this study, Shoushi et al. investigate the impact of family support programs on depression, anxiety, stress, and satisfaction in the open-heart surgery patients' family members at different time intervals. The finding shows the family in both groups had lower depression at 24h before and 14 days after the patient's discharge. Similar to our study, this study reveals that the family in the intervention group shows a greater decrease than the control group in terms of the mean score of depression [24].
One of the limitations of this study is that the effect of the intervention on depression in the families of patients admitted to the cardiac intensive care unit has been investigated only in the only medical center, which limits the generalizability of the results. The second limitation is the difference in the demographic characteristics of the families, which can affect their responses to the questionnaire. Finally, the duration of the study is limited to the first three days of the patient's hospitalization. Increasing the duration of family presence due to the longer hospital stay can affect the rate and fluctuations of family depression. It is necessary to pay attention to this issue in future studies. The present study could help the family during hospitalization and before discharge, followed by a sense of satisfaction and comfort and consequently less depression in the family of heart patients. In the family-centered care approaches, nurses can plan information support as a suitable psychological modality for the family and implement it coherently in intensive care units.
Conclusion
Informational support by providing comprehensive educational content orally and face to face along with question-answer sessions for patients' caregivers increases the family awareness of the conditions and decreases the depression among families during the stay of patients in the cardiac intensive care unit.
Acknowledgments: we need to thank all the professors of the Faculty of Nursing of Shahed University and the esteemed staff of the heart ward of the hospital cardiac care units in Sevome Shaban Damavand and the esteemed families who have accompanied us in the implementation of this study.
Ethical Permissions: The code of ethics IR.SHAHED.REC.1398.047.
Conflicts of Interests: The present study is taken from the master's thesis of nursing in the Faculty of nursing and midwifery of shahed University entitled "The effect of information support on anxiety and depression of caregivers of the family of hospitalized patients in cardiac care unit" and the authors declare that there is no conflict of interest.
Authors' Contribution: Mashhadi S.S. (First author), Methodologist/Original researcher/Statistical analyst/
Discussion author (30%); Hosseinkhani S.N. (Second author), Introduction author/Original researcher/
Discussion author (30%); Heidari M. (Third author), Methodologist/ Original researcher/Discussion author (20%); Norouzadeh R (Fourth author), Introduction author/Discussion author (20%).
Funding/Sources: The authors received no financial support for the research, authorship, and/or publication of this article.
Article Type: Original Research |
Subject:
Health Promotion Approaches
Received: 2020/11/20 | Accepted: 2021/03/6 | Published: 2021/06/20
Received: 2020/11/20 | Accepted: 2021/03/6 | Published: 2021/06/20
References
1. Rabie Siahkali S, Pourmemari MH, Khaleghdoost Mohamadi T, Eskandari F, Avazeh A. Study on effective factors on patients' family members anxiety in intensive care units. J Adv Med Biomed Res. 2010;18(70):91-101. [Persian] [Link]
2. Sarhadi M, Navidian A, Fasihi Harandi T, Keykhaei A. Assessment of psychological-social needs, family, special in patient unit ICU and CCU. Iran J Crit Care Nurs. 2013;6(4):259-68. [Persian] [Link]
3. Rabie Siahkali S, Avazeh A, Eskandari F, Khaleghdoost Mohammadi T, Mazzloom S, Paryad E, et al. A survey on psychological and environmental factors on family anxiety of the hospitalized patient in intensive care units. Iran J Crit Care Nurs. 2011;3(4):171-6. [Persian] [Link]
4. Shafipour V, Moosazadeh M, Jannati Y, Shoushi F. The effect of education on the anxiety of a family with a patient in critical care unit: A systematic review and meta-analysis. Electron Physician. 2017;9(3):3918-24. [Link] [DOI:10.19082/3918] [PMID] [PMCID]
5. Beesley SJ, Hopkins RO, Holt-Lunstad J, Wilson EL, Butler J, Kuttler KG, et al. Acute physiologic stress and subsequent anxiety among family members of ICU patients. Crit Care Med. 2018;46(2):229-35. [Link] [DOI:10.1097/CCM.0000000000002835] [PMID] [PMCID]
6. Kourti M, Christofilou E, Kallergis G. Anxiety and depression symptoms in family members of ICU patients. Av Enferm. 2015;33(1):47-54. [Link] [DOI:10.15446/av.enferm.v33n1.48670]
7. Pochard F, Darmon M, Fassier T, Bollaert PE, Cheval C, Coloigner M, et al. Symptoms of anxiety and depression in family members of intensive care unit patients before discharge or death: A prospective multicenter study. J Crit Care. 2005;20(1):90-6. [Link] [DOI:10.1016/j.jcrc.2004.11.004] [PMID]
8. Sadock BJ, Sadock VA. Kaplan and Sadock's synopsis of psychiatry: Behavioral sciences/clinical psychiatry. Alphen Aan Den Rijn: Wolters Kluwer; 2015. [Link]
9. Shoushi F, Jannati Y, Mousavinasab NA, Shafipour V. The impact of family centered care on depression, anxiety and stress of family caregivers of patients undergoing open heart surgery. Iran J Rehabilit Res. 2017;3(2):53-60. [Persian] [Link]
10. Bolosi M, Peritogiannis V, Tzimas P, Margaritis A, Milios K, Rizos DV. Depressive and anxiety symptoms in relatives of intensive care unit patients and the perceived need for support. J Neurosci Rural Pract. 2018;9(4):522-8. [Link] [DOI:10.4103/jnrp.jnrp_112_18] [PMID] [PMCID]
11. Safari M, Sedighi L, Fallahi Nia G, Rahimi Bashar F, Soltanian AR, Nikoo Seresht M. The effectiveness of behavioral pain scale (BPS) in the assessment of pain in patients with low level of consciousness. Anesthesiol Pain. 2012;3(1):22-8. [Persian] [Link]
12. Dalirirad H, Ghrzeljeh T, Seyedfatemi N. The effect of education support on anxiety in family caregivers of patient undergoing coronary artery bypass graft surgery. Nurs Midwifery J. 2019;16(10):738-48. [Persian] [Link]
13. Maxwell KE, Stuenkel D, Saylor C. Needs of family members of critically ill patients: A comparison of nurse and family perceptions. Heart Lung. 2007;36(5):367-76. [Link] [DOI:10.1016/j.hrtlng.2007.02.005] [PMID]
14. Hudson P, Payne S. Family caregivers and palliative care: Current status and agenda for the future. J Palliat Med. 2011;14(7):864-9. [Link] [DOI:10.1089/jpm.2010.0413] [PMID]
15. Jabbarpour M, Abdoli F, Kazemi M. The effect of providing information about the patient's condition on the anxiety level of the family members of hospitalized patients with traumatic brain injury. HAYAT. 2018;24(2):127-39. [Persian] [Link]
16. Farzadmehr M, Fallahi Khoshknab M, Hosseini MA, Khankeh HR. The effect of nursing consultation on anxiety and satisfaction of patient's families at the cardiac surgical intensive care unit. Iran J Psychiatr Nurs. 2016;4(2):57-64. [Persian] [Link] [DOI:10.21859/ijpn-04027]
17. Olcum HI, Ozsen K, Diken AI, Yazla E, Karadere E. Association between anxiety and depression and needs of patient families in cardiovascular surgery intensive care unit. Turk J Med Surg Intensive Care Med. 2018;9(3):63-7. [Link] [DOI:10.5152/dcbybd.2018.1906]
18. Ivarsson B, Larsson S, Luhrs C, Sjoberg T. Serious complications in connection with cardiac surgery-next of kin's views on information and support. Intensive Crit Care Nurs. 2011;27(6):331-7. [Link] [DOI:10.1016/j.iccn.2011.10.002] [PMID]
19. Zakerimoghadm M, Ghiasvandian S, Salahshoor P, Kazemnezhad A. The effect of supportive nursing program on depression, anxiety and stress of family members of patients during coronary artery bypass graft (CABG) surgery. Iran J Cardiovasc Nurs. 2014;3(1):50-8. [Persian] [Link]
20. Kaviani H, Seyfourian H, Sharifi V, Ebrahimkhani N. Reliability and validity of anxiety and depression hospital scales (HADS): Iranian patients with anxiety and depression disorders. Tehran Univ Med J. 2009;67(5):379-85. [Persian] [Link]
21. Navidian A, Rezaei J, Payan H. Efficacy of supportive-educational intervention on psychological reactions of family members of intensive care unit patients. J Nurs Educ. 2016;5(4):51-8. [Persian] [Link] [DOI:10.21859/jne-05047]
22. Chien WT, Chiu YL, Lam LW, Ip WY. Effects of a needs-based education programme for family carers with a relative in an intensive care unit: A quasi-experimental study. Int J Nurs Stud. 2006;43(1):39-50. [Link] [DOI:10.1016/j.ijnurstu.2005.01.006] [PMID] [PMCID]
23. Azouley E, Pochard F, Chevret S, Jourdain M, Bornstain C, Wernet A, et al. impact of a family information leaflet on effectiveness of information provided to family members of intensive care unit patients: A multicenter, prospective, randomized, controlled trial. Am J Respir Crit Care Med. 2005;165(4):438-42. [Link] [DOI:10.1164/ajrccm.165.4.200108-006oc] [PMID]
24. Shoushi F, Janati Y, Mousavinasab N, Kamali M, Shafipour V. The impact of family support program on depression, anxiety, stress, and satisfaction in the family members of open-heart surgery patients. J Nurs Midwifery Sci. 2020;7(2):69-77. [Persian] [Link] [DOI:10.4103/JNMS.JNMS_21_19]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |