



Volume 9, Issue 2 (2021)
Health Educ Health Promot 2021, 9(2): 153-164 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Molaeinezhad M, Scheidt C, Afshar H, Jahanfar S, Sohran F, Salehi M et al . Bodily Map of Emotions in Iranian People. Health Educ Health Promot 2021; 9 (2) :153-164
URL: http://hehp.modares.ac.ir/article-5-47532-en.html
URL: http://hehp.modares.ac.ir/article-5-47532-en.html
1- Behavioral Sciences Research Center, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran
2- Department of Psychosomatic, Albert-Ludwigs-Universitat Freiburg, Freiburg, Germany
3- “Psychosomatic Research Center” and “Departments of Psychiatry, School of Medicine”, Isfahan University of Medical Sciences, Isfahan, Iran
4- School of Public health, College of Health Professionals, Central University of Michigan, Mount Pleasant, Michigan, United States of America
5- Department of Midwifery, Nursing and Midwifery School, Khorasgan Branch, Islamic Azad University, Khorasgan, Iran
6- Danesh-e Tandorosti Institute, Isfahan, Iran ,drfgoli@gmail.com
2- Department of Psychosomatic, Albert-Ludwigs-Universitat Freiburg, Freiburg, Germany
3- “Psychosomatic Research Center” and “Departments of Psychiatry, School of Medicine”, Isfahan University of Medical Sciences, Isfahan, Iran
4- School of Public health, College of Health Professionals, Central University of Michigan, Mount Pleasant, Michigan, United States of America
5- Department of Midwifery, Nursing and Midwifery School, Khorasgan Branch, Islamic Azad University, Khorasgan, Iran
6- Danesh-e Tandorosti Institute, Isfahan, Iran ,
Keywords: Emotion [MeSH], Cross-Cultural Comparison [MeSH], Culture [MeSH], Sensation [MeSH], Gender Difference [MeSH]
Full-Text [PDF 1055 kb]
(1727 Downloads)
| Abstract (HTML) (1963 Views)
Table 1) Frequency of demographic Characteristics of participants (N=220)
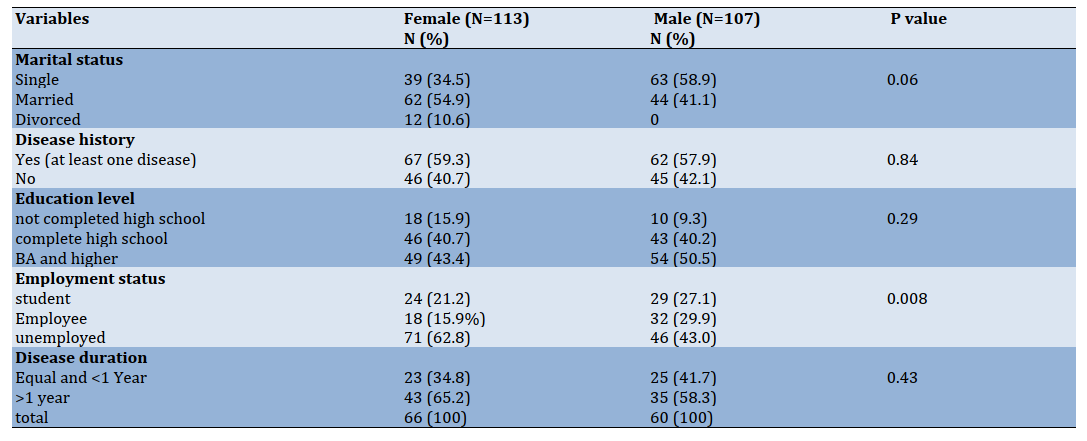
Table 2) Cumulative frequency of Bodily sensation hits with six basic emotions plus anxiety and the rank order of body sites (top 50% reported sites) by gender and overall
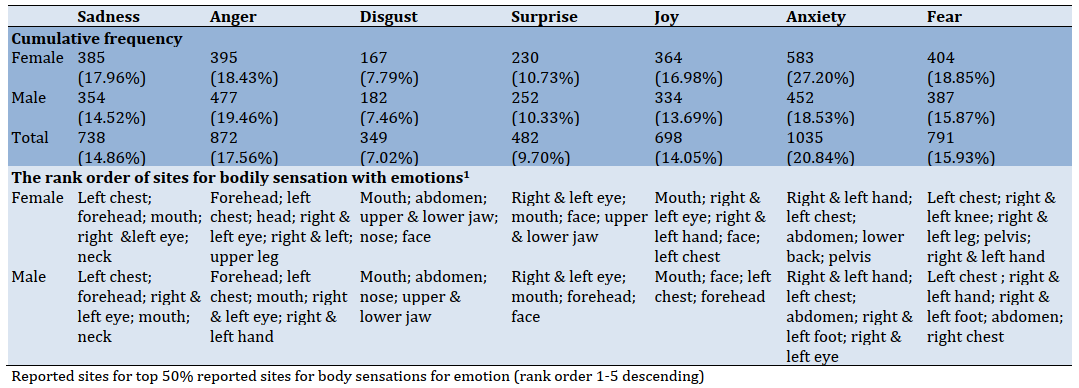
Table 6) General Linear Models predicting emotion-related body changes (EBCRs) and Emotion* Gender Interaction on Facial sensation parts
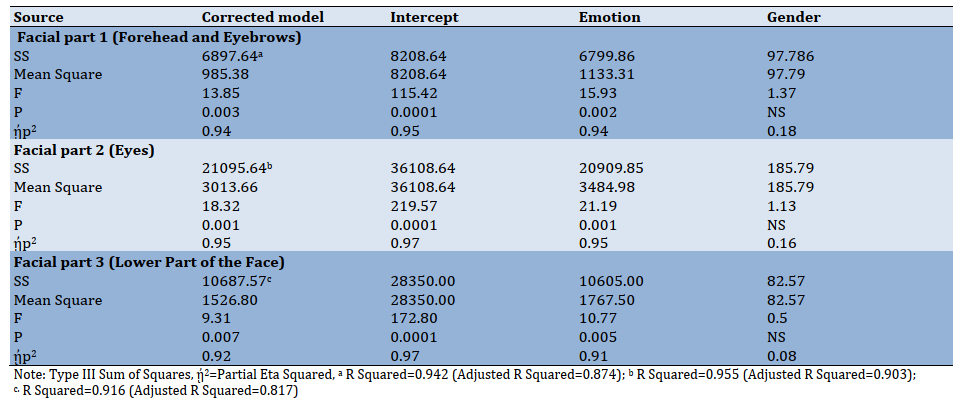
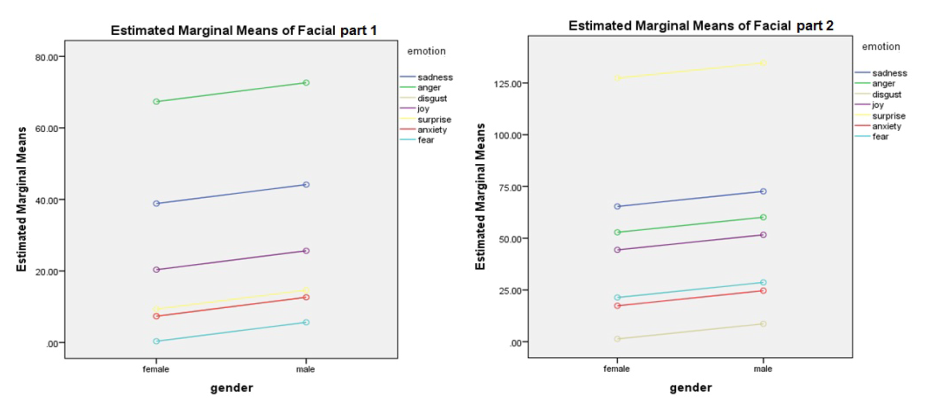
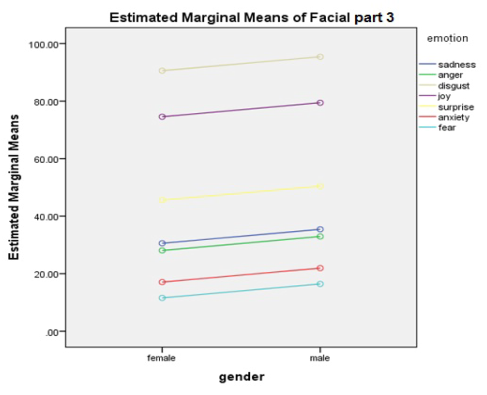
Figure 3) Gender*Emotion interaction on facial parts 1-3; Gender for the Horizontal Axis and emotion for Separate Lines and plot gender*Emotion
Discussion
Topographic evaluation of emotionally intensified physical changes can provide a unique tool for emotion studies as well as biomarkers for the detection of emotional disorders [3]. Our participants have reported emotional differentiation of body sensations for all six basic emotions and anxiety, and their reported patterns of BSM were consistent with universal patterns [10]. This finding agrees with [3] findings that showed that different emotions are associated with topographically distinct and culturally universal bodily sensations.
Contrary to expectations, our data suggest that total EBRCs for all different emotions do not differ between sexes. Graphs in the upper trunk were almost the same, and emotion perception in the back body, although showed greater mean scores for female participants, model failed to reach significance for both sexes. Similarly, men reported mean scores in head & neck and upper limbs, which failed to show a significant difference across genders.
Consistent with Nummenmaa et al.’s finding, our results reveal a gender-free similarity with universal patterns of BSM. Though in small sample sizes, some of the differences might not be detected because of lower statistical power. Therefore we suggest that issues related to interception such as emotional awareness- recognition of the connection between body sensations and emotional states and body listening - the tendency to actively listen to the body for insight, which is assumed to be different in both sexes, should be further investigated in future studies [30, 35].
Nonetheless, we found differences in the lower limb when comparing males and females in ERBCs, especially for fear, anxiety, and anger. Bear in mind, the generalizability of “weakening in the knees” as one of the most common bodily sensations with fear, anger [10] and anxiety, across studies and cross-cultural samples, is not surprising that these emotions were reported as the most perceived emotions in the lower limb. Nevertheless, interpretation for gender differences is more difficult. These differences can be explained in part by sex differences in noticing and emotional awareness [30, 35] with considering other potential sources of differences such as; the cultural meaning of the body sensation [10], gender stereotypes, and social desirability of this emotional sensation pattern [36]. Therefore, these factors could be suggested for further investigation in future studies.
Anxiety and anger were the most reported emotions associated with enhanced sensations all over the body with no significant emotion* gender interaction. The most striking result to emerge from the data is that, unlike our expectations and many researchers’ idea about the pervasive presence of sorrow in Persian culture [23], sadness was not the most prominent emotion through user-generated bodily sensation maps. The prior studies were mostly linguistic, have attempted to trace the manifestation of sadness in different areas of Iranian daily life using semantic methods and emotional terminology [18, 22, 23, 27]. Based on our knowledge, this study was the first research conducted to clarify the reported emotion-related BSM (for implicit detection of emotions) independence of emotion-related words in Iran. So, one can assume that those high-frequency sadness reports have emerged from stereotypical usage of non -exact terms connected with sadness for diverse subtle emotional states by Iranians, with more extended usage in the past [24].
Another explanation is assuming a transition from sadness to anxiety and anger that may have occurred in recent years in the Iranian population. Considering the interrelations between context, emotions, and individual and societal actions in conflict situations [37] and turning now to the historical evidence of socio-political changes in Iran, much of the anger and anxiety may stem from the catastrophic effects of economic instability during recent years due to prolong sanctions, the unpredictability of future and challenges of adaptation to all these events. It may contribute to learned helplessness and non-verbal and somatic modes of emotional expression [15, 38]. Our data must be interpreted with caution, though, because the design of the study and our questionnaires did not allow us to test whether this association is a culture-specific change or no.
Contrary to our expectation,” left chest “was not the first rank order of body sensation across emotions. There are many words for heart-focused emotions in Persian literature that do not essentially mean more emotional change on the left side of the chest [14]. In other words, what is called as heart “equal to Del in Farsi” in Persian metaphorical expressions of emotions equals a large part of the front upper trunk as well as mind and may not necessarily mean the heart [25]. Given that in many cultures, there are many words for the expression of the emotional state. Many of these terms are just metaphors and stereotypical bodily responses associated with emotions [3] and may not necessarily reflect physiological changes associated with different emotions (e.g., the word butterfly in the
stomach [3, 39].
However, a careful comparison cannot be made until a detailed study clarifies what specific bodily sensations are related to the expression of emotions through experiments using emotion induction techniques [3].
Moreover, the participants' reports of the most emotional perception in the mouth area may reflect the people's verbal culture at this point in the world. Probably reflecting the pattern of emotion suppression in Iranian culture in the presence of unwritten rules of politeness which sometimes prohibited Iranians from the verbal expressing of unpleasant feelings, they report an increased amount of feeling and increased pressure in their mouth area (i.e., Feeling pressure in teethes and teeth grinding during anger- which is not specified in this article). In recent decades, few Iranian researchers have attempted to explore possible causes of an intensified range of state-trait anger expression and aggression in the Iranian community [40-45]. However, with a small sample size and in the absence of any well-designed epidemiological study about the prevalence of anger in Iranians, caution must be applied.
Considering several devastating social and political events (i.e., Iraq-Iran war, natural disasters, and prolong economic and political sanctions against Iran) and in the context of vulnerability of Iranians for the somatization of anger and anxiety [15, 38], their patterns of anger management and emotion regulation have to be more studied in multidisciplinary researches.
As we know, negative emotions such as anger and fear are integral parts of the generation and experience of conflicts [37, 46]. Therefore, although it may be assumed as a very preliminary conclusion based on our findings, we just here want to imply the conceptual premise for” the long-term role of negative emotions in shaping conflictual interaction and conflict transformation” [37]. We hope that our findings serve as a base for future studies by social psychologists and practitioners in the field to understand more clearly Iranian individuals’ emotions and their collective behaviors and to facilitate conflict resolution approaches [37, 47-49] intent to re-establishing social cooperation and conducive to build the culture of peace in our population [37]. However, further studies on this topic need to be undertaken before associating negative emotions, and Iranians’ conflictual collective behaviors are more clearly understood.
Sensations of anger in the upper limb as an approach-oriented emotion align with a universal pattern [3, 10]. Anxiety, followed by fear and anger, is the most perceived emotion in this area, showing similarity to universal patterns [10].
Concerning Facial patterns, our results were in contrast to the upper face facial expression pattern in Western studies [49], reported as six “discrete" emotions, resembling the East Asian emotional expression pattern and showing an overlap for fear, surprise, anger, and sadness. However, in our study, anger and sadness were more distinct than other emotions. Although the studies mentioned were related to emotional expression and not to perceptions of emotions, our findings are not exactly comparable to the corresponding studies. Nevertheless, it can be cited as a basis for further studies on comparing emotion expression maps in the Iranian population.
Disgust and happiness were the most common emotions in the lower part of the face (mouth, cheeks, and chin) that resemble universal patterns in this respect. Surprisingly, sadness, anger, anxiety, and fear form a cluster that seems to resemble East Asian emotional expression patterns [49]. However, the compatibility of these patterns with patterns of emotional expression in the three facial areas should be explored in future studies.
Sensations in the digestive system and mouth region were mainly found in disgust, consistent with universal sensation patterns [3]. This result is also in line with finding a study by Breugelmans et al., which showed that “disgust is one of the basic emotions which appears to be better differentiated by body sensations across cultures” [10]. As the graph shows, our participants reported disgust as the least frequent emotion perceived in total bodily sensation map. Considering very little studies conducted about disgust emotion among Iranian individuals, questions raised about “the construct of emotion disgust” among Iranian people [50] and the association between disgust sensitivity and disorders such as obsessive compulsive disorder [50] and vaginismus [51]. Hence, further experimental investigations are needed.
Although it is a very preliminary study in the field of emotion study, these findings have important implications for developing the bodily map of the emotions and emotion sensation profile of Iranian people. Overall, the results of this study revealed similarity of Iranians’ EBRCs for six basic emotions and anxiety with universal patterns but considering few differences regarding facial patterns of emotion sensation and mouth as a top rank point of emotion sensation in our results, further investigation for comprehensive comparing Iranians’ emotional sensation patterns with common universal standards are suggested [3, 10].
Breugelmans et al. agree that “a combination of culture-specific and cross cultural approach” [10] should be applied for exact assessment of association between perceived emotions, embodied feelings, and unexplained somatic symptoms.
Finally, some important limitations need to be considered. First, the study sample size was small and was not included different subcultures of Iranian individuals. Second, we could not use the application mode of EmBODY questionnaire; hence our results could not exactly compare with EmBODY response profiles. Therefore, for future studies, we should consider a comparable android or IOS Farsi version of this application permitting from EmBODY manufacturers [3]. Third, in the absence of a constructivist view [6] and the characteristics of the Questionnaire we used, we did not consider socially constructed components of emotions that people use to express their body sensation [10, 52], such as metaphorical and linguistic components of emotions. So, the results of our study may not explicitly reflect the Iranian cultural specific variations in body sensation with emotions, which is a subject of further study.
Conclusion
The results suggested a gender-free consistency of distinct emotion-triggered bodily sensation maps of Iranians with universal patterns. The total EBRCs for all different emotions do not differ between sexes, but regarding 5-main body areas, a significant gender difference was observed in lower limbs.
Acknowledgments: We gratefully acknowledge the staff of the psychosomatic center and our participants.
Ethical Permissions: The research was approved by Isfahan University of Medical Sciences, Ethical Committee (IR.MUI.REC.1395.2.256).
Conflicts of Interests: This article is a part of a research project approved by Psychosomatic Research Center, Faculty of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran (Code: 295256). No potential conflict of interest was reported by the authors.
Authors’ Contribution: Molaeinezhad M (First Author), Introduction Writer/Main Researcher/Statistical Analyst/Discussion Writer (40%); Scheidt C.E. (Second Author), Methodologist/Discussion Writer (10%); Afshar H. (Third Author), Introduction Writer/Discussion Writer (10%); Jahanfar Sh. (Forth Author), Statistical Analyst/Discussion Writer (15%); Sohran F. (Fifth Author), Assistant Researcher (5%); Salehi M. (Sixth Author), Assistant Researcher (5%); Goli F. (Seventh Author), Introduction Writer/Discussion Writer (15%)
Funding/Support: The grant supported by Isfahan University of Medical Sciences, Psychosomatic Research Center is acknowledged.
Full-Text: (814 Views)
Introduction
There is an accepted notion that the six basic emotions (sadness, anger, surprise, disgust, happiness, and fear) have a specific neural basis and are associated with specific body changes in adults [1, 2]. The association between physical changes and various emotions is also reflected in our daily activities; feeling weakness on the knees during fear, or reddening the face with anger, tachycardia with arousal, and muscle contraction during anxiety are examples of personal perception of emotions, which are mostly recognized as universal experiences. Both the classic and modern models of emotional processing believe that subjective experiences of emotions are characterized by emotion-related bodily states that reflect changes in musculoskeletal systems, neuro-endocrine, and autonomous nervous systems [3].
The major theories of emotion suggest that a person's subjective feelings of emotion originate from bodily changes perceived by individuals [4, 5], and the physical perception of emotions has a distinct and well-known pattern discussed in various studies [4, 6].
While Ekman et al. believe in the universality of the six main emotions [1], few studies pointed to the role of culture in emotional sensation and expression [7-9]. Based on this parallel view, emotion is a construct that is psychologically and biologically determined and influenced by the environment, so cross-cultural differences are expected [6, 10]. Cultural differences may affect some aspects, including incidence, facial expression, recognition, the nature of experienced emotion [7, 11, 12], and affect valuation [13].
Iran is a country made up of heterogeneous populations and different subcultures with common historical and linguistic roots and similarities through Old Persian culture. The Iranian nation has some particularities in impressing their experiences as a nation, which distinguished them from the cultures of East Asia and the Arab and Islamic countries of the region [14, 15]. In general, Iranians are considered socially and interpersonally as sensitive individuals [14, 15].
The partial limits of Iranian culture to frankness and openness in expressing expectations, wishes, wills, desires, and dissatisfaction as an unwritten rule of respect and politeness [16, 17] make individuals try concealing their emotions in some ways or put a partial limit in display rules of emotions in specific situations [15, 18, 19]. The inability of those people to express verbally unpleasant feelings that are not accepted by the community, such as anger and annoyance, [15, 17, 19] also can contribute to the somatization of emotions in Iranian culture [15, 19]. Somatization of anxiety and anger symptoms such as musculoskeletal pain, heart disease, and digestive problems are frequently found among Iranians [14, 15, 19]. There is also an excessive emphasis on grief and sadness in Persian culture and language, which is a topic that some linguistic studies have been addressing [18]. Few researchers believe that the Iranian population is more inclined to cry, tears, and expressing sadness than other people in the world. They assumed sadness and grief as the most commonly perceived emotion in the Iranians [18, 20, 21].
One of the problems in recognizing and communicating about emotions in Persian discourse is the use of vague terms related to Persian metaphorical expressions of emotions [19, 22] and the richness of terminology related to emotions in the Persian Language, which is impossible to find an equivalent and exact term for those countless expressions [22, 23].
In a constructivist view, the body-part terms used in the Persian language are also very ambiguous [24]. For example, in Persian, the word "Del" is conceptualized as being either an internal organ and anatomical points of the "heart," -the motor of the body- [14] and the stomach, and on the other hand, means a container in which emotions, desires, patience, motivation, affection, thoughts and the person's memories [14, 22, 25, 26].
To date, limited linguistic studies have been conducted using questionnaires and discourse analysis on linguistic concepts and metaphors related to the basic emotions in Iran [18, 22, 27], Which tell us about the inter-language and cross-cultural similarities of emotion conceptualization for Iranians with different cultures.
However, no study has been conducted yet, on Iranians’ perception of emotion-related bodily changes (ERBCs) or bodily sensation map of emotions (BSMs) using topographic maps and non-verbal questionnaires. The study by Nummenmaa et al. using the embody app is one of the limited studies which eradicates language and semantic barriers in expressing emotions through user-generated bodily sensation maps (BSMs) [3] and helps individuals create a BSM of how they feel. Hence, makes it easier for researchers to detect and classify users' emotions based on body maps [28].
Moreover, sex differences in the perception and expression of emotions are also controversial [24, 29]. Theoretically, there are differences between men and women in bodily sensation and understanding relations between bodily sensations and emotional states [30]. The Iranian community places more restrictions on the female body to express emotions [16, 17]. Considering the low threshold of tolerance of Iranian culture for expressing emotions, especially positive emotions such as happiness, and more acceptances for expressing feelings such as sadness by women in Iranian culture, differences in physical feelings between sexes can be observed [16, 17, 24]. Nevertheless, the question that Iranian women and men are different in the perception and bodily sensation of emotions remains unresolved.
Considering the lack of appropriate information about the emotions perceived by the Iranian people and the location of experienced bodily changes associated with basic emotions, further investigations are needed. This study was part of a mixed exploratory study with two consecutive qualitative and quantitative phases. The first phase of the study was conducted in a method of discourse and thematic analysis through semi-structured interviews, and the second phase was a quantitative cross-sectional study designed to assess ERBCs and BSMs in a sample of Iranian people.
In summary, this study has conducted in order: 1- to assess whether Iranian samples can differentiate bodily sensation associated with six basic emotions (sadness, anger, disgust, surprise, happiness, and fear) plus anxiety, 2- to clarify the rank order of basic emotion which are most likely to be perceived with bodily changes among Iranians, 3- to identify the body regions in Iranian sample which reflects the greatest frequency of ERBC. 4-To compare the emotion-related bodily changes in the whole body and 5part -BSMs by sex. One of our hypotheses is that the ERBCs are sensitive to sex.
Materials and Methods
This cross-sectional study was conducted on an Iranian seemingly healthy population from May to August 2019 in Iran. The study sample (N=240) consisted of volunteers selected among a web-based advertisement and the visitors to public libraries and parks, students, and referrals to health centers (two in Isfahan and one in Tehran) that were referred to periodic examinations and vaccinations for their children, originally from various parts of Iran such Isfahan, Tehran, Ahvaz, Shiraz, Yasuj, Shahrekord, Zahedan. The number of samples was considered to be at least five cases for each body map point (41 points) according to the rule of thumb [31], and the consecutive sampling was stopped after collecting the minimum number of participants. Consecutive participants were selected if the age was more than 15 years and they were never diagnosed with thought disorders. A lack of psychotropic substances, drugs, and alcohol and the ability to express thoughts and feelings were the other inclusion criteria. The exclusion criterion was The participant’s decision to stop the completion of the questionnaires for any reason and at any stage. The demographic characteristics of the participants were recorded, such as age, marital and employment status, education level, history of the disease, and duration of diseases. The Farsi emBODY Questionnaire was including two 10cm front and back images of the body. Using colored pencils with distinct colors, the participants evaluated the intensity of bodily sensation of emotions based on a 5-point Likert scale (i.e., 1=Very mild to 5=very severe). The body maps did not reflect any internal organs or forms representing gender to avoid participants' misperception and consistency between the two genders. Not using the emBODY application was the lack of public access to IOS phones in Iran, besides translating the exact words used for emotions in the app to the Persian language. The face and content validity of the Persian version was assessed by presenting the preliminary body map questionnaire to ten experts in psychology, psychiatry, and linguistic to assure the correct and valid translation of Persian equivalents were used for each of the emotions. Since concordant BSMs result in the adult population for both techniques shown in previous studies [3, 5], a memory-based report was used instead of participants’ inducing emotions. To simplify the interpretation of the data, we employed a 41 point version of the Michigan Body Map (35 points from the Michigan Pain Map and six additional points including the mouth, right and left eyes, forehead, nose and ears, and the left and right jaws replaced with upper and lower Jaw). [32]. Then a transparent page was prepared and digitized based on these sections of a standard body template, and response sheets were screened and compared manually to determine the colored points in each Questionnaire. Responses outside the body area were not accounted for. The parts of the BSMs colored by the participants were calculated as the point of perceived emotion (1=yes) and the blank, uncolored points and less than a quarter of the point area accounted as (No=0). Then the intensity assigned to the perceived emotion at the relevant point in BSMs was manually entered into separate tables related to each emotion. Participants could specify more than one point for each emotion. They could also determine more than one emotion for a specific body point; hence BSMs were screened separately for each emotion. For a better interpretation of the results, the body maps results were divided into five general sections, i.e., the head and neck, upper trunk, back, upper and lower limbs. Furthermore, Using the FAST system (Facial Affect Scoring technique by Ekman group) [33], reported emotion-related facial changes results were divided into three sections (i.e., Facial part 1=head and forehead, Facial part 2=eyes, and Facial part 3=lower part of the face). The performance of the Farsi version of emBODY in detecting actual emotions was measured with accuracy and calculating Cohen’s kappa coefficient (k= (P0-Pe)/ (1-Pe), while P0 considered as the observed rate of agreement and Pe as the theoretical probability of agreement by chance, calculated based on the formula given the number of possible classes (here is the number of considered emotions) [27]. The smartphone version of emBODY by Nummenmaa et al. [3] and the Farsi version were presented to 15 participants, and they told to paint the sensation they felt at the moment and the body parts they felt changes with each emotion (BSMs), then two versions of user-painted body region were compared. The average similarity and standard deviation for six discrete basic emotions plus the anxiety of the BSMs were calculated. The Farsi version of Embody showed a high rate of accuracy (ranged from 83-91%) and Cohen’s kappa coefficient (0.812) [3]. The test-retest correlates also indicated an appropriate level of stability for the Farsi version of the embodying tool for 15 participants in two experiments (ranged from 0.73 to 0.83).
The research was approved by Isfahan University of Medical Sciences, and all of the participants gave their informed consent before completing of body map questionnaire. All subjects were volunteers agreeing to fill in a Farsi paper-and-pencil version of the emBODY tool designed by Nummenmaa et al. [3]. During completion of questionnaires, participants were asked to identify and color the bodily regions whose activity they felt to be changed during (Sadness, anger, disgust, happiness, surprise, and fear) plus anxiety.
The data were analyzed by descriptive statistical and inferential methods such as chi-square, t-test, ANCOVA, and GLM using SPSS 22. The significant level for statistical tests considered p<0.05.
Findings
Response sheets of 220 participants were analyzed (113 women and 107 men). The age range was from 16 to 55, and the mean±SD age of women and men was 34.09±10.87 and 28.21±8.88, respectively (p=0.04). There was a significant difference regarding employment status and age between men and women, which indicated that the majority of the female participants were unemployed and older (p<0.05; Table 1).
The frequency of reported point by point ERBCs associated with each emotion showed in Table 2. The first five frequent points where activation was felt for each emotion were listed in the below rows of the table.
Considering the rank order of body sensations for each emotion, all emotions were associated with changes mostly in the mouth, left chest, forehead, eyes, and hands, respectively (Tables 2 and 3).
In the 5-part BSM, head and neck, upper trunk, upper and lower limbs, and back were reported as the most common places of emotional perception (Tables 3 and 4).
There is an accepted notion that the six basic emotions (sadness, anger, surprise, disgust, happiness, and fear) have a specific neural basis and are associated with specific body changes in adults [1, 2]. The association between physical changes and various emotions is also reflected in our daily activities; feeling weakness on the knees during fear, or reddening the face with anger, tachycardia with arousal, and muscle contraction during anxiety are examples of personal perception of emotions, which are mostly recognized as universal experiences. Both the classic and modern models of emotional processing believe that subjective experiences of emotions are characterized by emotion-related bodily states that reflect changes in musculoskeletal systems, neuro-endocrine, and autonomous nervous systems [3].
The major theories of emotion suggest that a person's subjective feelings of emotion originate from bodily changes perceived by individuals [4, 5], and the physical perception of emotions has a distinct and well-known pattern discussed in various studies [4, 6].
While Ekman et al. believe in the universality of the six main emotions [1], few studies pointed to the role of culture in emotional sensation and expression [7-9]. Based on this parallel view, emotion is a construct that is psychologically and biologically determined and influenced by the environment, so cross-cultural differences are expected [6, 10]. Cultural differences may affect some aspects, including incidence, facial expression, recognition, the nature of experienced emotion [7, 11, 12], and affect valuation [13].
Iran is a country made up of heterogeneous populations and different subcultures with common historical and linguistic roots and similarities through Old Persian culture. The Iranian nation has some particularities in impressing their experiences as a nation, which distinguished them from the cultures of East Asia and the Arab and Islamic countries of the region [14, 15]. In general, Iranians are considered socially and interpersonally as sensitive individuals [14, 15].
The partial limits of Iranian culture to frankness and openness in expressing expectations, wishes, wills, desires, and dissatisfaction as an unwritten rule of respect and politeness [16, 17] make individuals try concealing their emotions in some ways or put a partial limit in display rules of emotions in specific situations [15, 18, 19]. The inability of those people to express verbally unpleasant feelings that are not accepted by the community, such as anger and annoyance, [15, 17, 19] also can contribute to the somatization of emotions in Iranian culture [15, 19]. Somatization of anxiety and anger symptoms such as musculoskeletal pain, heart disease, and digestive problems are frequently found among Iranians [14, 15, 19]. There is also an excessive emphasis on grief and sadness in Persian culture and language, which is a topic that some linguistic studies have been addressing [18]. Few researchers believe that the Iranian population is more inclined to cry, tears, and expressing sadness than other people in the world. They assumed sadness and grief as the most commonly perceived emotion in the Iranians [18, 20, 21].
One of the problems in recognizing and communicating about emotions in Persian discourse is the use of vague terms related to Persian metaphorical expressions of emotions [19, 22] and the richness of terminology related to emotions in the Persian Language, which is impossible to find an equivalent and exact term for those countless expressions [22, 23].
In a constructivist view, the body-part terms used in the Persian language are also very ambiguous [24]. For example, in Persian, the word "Del" is conceptualized as being either an internal organ and anatomical points of the "heart," -the motor of the body- [14] and the stomach, and on the other hand, means a container in which emotions, desires, patience, motivation, affection, thoughts and the person's memories [14, 22, 25, 26].
To date, limited linguistic studies have been conducted using questionnaires and discourse analysis on linguistic concepts and metaphors related to the basic emotions in Iran [18, 22, 27], Which tell us about the inter-language and cross-cultural similarities of emotion conceptualization for Iranians with different cultures.
However, no study has been conducted yet, on Iranians’ perception of emotion-related bodily changes (ERBCs) or bodily sensation map of emotions (BSMs) using topographic maps and non-verbal questionnaires. The study by Nummenmaa et al. using the embody app is one of the limited studies which eradicates language and semantic barriers in expressing emotions through user-generated bodily sensation maps (BSMs) [3] and helps individuals create a BSM of how they feel. Hence, makes it easier for researchers to detect and classify users' emotions based on body maps [28].
Moreover, sex differences in the perception and expression of emotions are also controversial [24, 29]. Theoretically, there are differences between men and women in bodily sensation and understanding relations between bodily sensations and emotional states [30]. The Iranian community places more restrictions on the female body to express emotions [16, 17]. Considering the low threshold of tolerance of Iranian culture for expressing emotions, especially positive emotions such as happiness, and more acceptances for expressing feelings such as sadness by women in Iranian culture, differences in physical feelings between sexes can be observed [16, 17, 24]. Nevertheless, the question that Iranian women and men are different in the perception and bodily sensation of emotions remains unresolved.
Considering the lack of appropriate information about the emotions perceived by the Iranian people and the location of experienced bodily changes associated with basic emotions, further investigations are needed. This study was part of a mixed exploratory study with two consecutive qualitative and quantitative phases. The first phase of the study was conducted in a method of discourse and thematic analysis through semi-structured interviews, and the second phase was a quantitative cross-sectional study designed to assess ERBCs and BSMs in a sample of Iranian people.
In summary, this study has conducted in order: 1- to assess whether Iranian samples can differentiate bodily sensation associated with six basic emotions (sadness, anger, disgust, surprise, happiness, and fear) plus anxiety, 2- to clarify the rank order of basic emotion which are most likely to be perceived with bodily changes among Iranians, 3- to identify the body regions in Iranian sample which reflects the greatest frequency of ERBC. 4-To compare the emotion-related bodily changes in the whole body and 5part -BSMs by sex. One of our hypotheses is that the ERBCs are sensitive to sex.
Materials and Methods
This cross-sectional study was conducted on an Iranian seemingly healthy population from May to August 2019 in Iran. The study sample (N=240) consisted of volunteers selected among a web-based advertisement and the visitors to public libraries and parks, students, and referrals to health centers (two in Isfahan and one in Tehran) that were referred to periodic examinations and vaccinations for their children, originally from various parts of Iran such Isfahan, Tehran, Ahvaz, Shiraz, Yasuj, Shahrekord, Zahedan. The number of samples was considered to be at least five cases for each body map point (41 points) according to the rule of thumb [31], and the consecutive sampling was stopped after collecting the minimum number of participants. Consecutive participants were selected if the age was more than 15 years and they were never diagnosed with thought disorders. A lack of psychotropic substances, drugs, and alcohol and the ability to express thoughts and feelings were the other inclusion criteria. The exclusion criterion was The participant’s decision to stop the completion of the questionnaires for any reason and at any stage. The demographic characteristics of the participants were recorded, such as age, marital and employment status, education level, history of the disease, and duration of diseases. The Farsi emBODY Questionnaire was including two 10cm front and back images of the body. Using colored pencils with distinct colors, the participants evaluated the intensity of bodily sensation of emotions based on a 5-point Likert scale (i.e., 1=Very mild to 5=very severe). The body maps did not reflect any internal organs or forms representing gender to avoid participants' misperception and consistency between the two genders. Not using the emBODY application was the lack of public access to IOS phones in Iran, besides translating the exact words used for emotions in the app to the Persian language. The face and content validity of the Persian version was assessed by presenting the preliminary body map questionnaire to ten experts in psychology, psychiatry, and linguistic to assure the correct and valid translation of Persian equivalents were used for each of the emotions. Since concordant BSMs result in the adult population for both techniques shown in previous studies [3, 5], a memory-based report was used instead of participants’ inducing emotions. To simplify the interpretation of the data, we employed a 41 point version of the Michigan Body Map (35 points from the Michigan Pain Map and six additional points including the mouth, right and left eyes, forehead, nose and ears, and the left and right jaws replaced with upper and lower Jaw). [32]. Then a transparent page was prepared and digitized based on these sections of a standard body template, and response sheets were screened and compared manually to determine the colored points in each Questionnaire. Responses outside the body area were not accounted for. The parts of the BSMs colored by the participants were calculated as the point of perceived emotion (1=yes) and the blank, uncolored points and less than a quarter of the point area accounted as (No=0). Then the intensity assigned to the perceived emotion at the relevant point in BSMs was manually entered into separate tables related to each emotion. Participants could specify more than one point for each emotion. They could also determine more than one emotion for a specific body point; hence BSMs were screened separately for each emotion. For a better interpretation of the results, the body maps results were divided into five general sections, i.e., the head and neck, upper trunk, back, upper and lower limbs. Furthermore, Using the FAST system (Facial Affect Scoring technique by Ekman group) [33], reported emotion-related facial changes results were divided into three sections (i.e., Facial part 1=head and forehead, Facial part 2=eyes, and Facial part 3=lower part of the face). The performance of the Farsi version of emBODY in detecting actual emotions was measured with accuracy and calculating Cohen’s kappa coefficient (k= (P0-Pe)/ (1-Pe), while P0 considered as the observed rate of agreement and Pe as the theoretical probability of agreement by chance, calculated based on the formula given the number of possible classes (here is the number of considered emotions) [27]. The smartphone version of emBODY by Nummenmaa et al. [3] and the Farsi version were presented to 15 participants, and they told to paint the sensation they felt at the moment and the body parts they felt changes with each emotion (BSMs), then two versions of user-painted body region were compared. The average similarity and standard deviation for six discrete basic emotions plus the anxiety of the BSMs were calculated. The Farsi version of Embody showed a high rate of accuracy (ranged from 83-91%) and Cohen’s kappa coefficient (0.812) [3]. The test-retest correlates also indicated an appropriate level of stability for the Farsi version of the embodying tool for 15 participants in two experiments (ranged from 0.73 to 0.83).
The research was approved by Isfahan University of Medical Sciences, and all of the participants gave their informed consent before completing of body map questionnaire. All subjects were volunteers agreeing to fill in a Farsi paper-and-pencil version of the emBODY tool designed by Nummenmaa et al. [3]. During completion of questionnaires, participants were asked to identify and color the bodily regions whose activity they felt to be changed during (Sadness, anger, disgust, happiness, surprise, and fear) plus anxiety.
The data were analyzed by descriptive statistical and inferential methods such as chi-square, t-test, ANCOVA, and GLM using SPSS 22. The significant level for statistical tests considered p<0.05.
Findings
Response sheets of 220 participants were analyzed (113 women and 107 men). The age range was from 16 to 55, and the mean±SD age of women and men was 34.09±10.87 and 28.21±8.88, respectively (p=0.04). There was a significant difference regarding employment status and age between men and women, which indicated that the majority of the female participants were unemployed and older (p<0.05; Table 1).
The frequency of reported point by point ERBCs associated with each emotion showed in Table 2. The first five frequent points where activation was felt for each emotion were listed in the below rows of the table.
Considering the rank order of body sensations for each emotion, all emotions were associated with changes mostly in the mouth, left chest, forehead, eyes, and hands, respectively (Tables 2 and 3).
In the 5-part BSM, head and neck, upper trunk, upper and lower limbs, and back were reported as the most common places of emotional perception (Tables 3 and 4).
Table 1) Frequency of demographic Characteristics of participants (N=220)
Table 2) Cumulative frequency of Bodily sensation hits with six basic emotions plus anxiety and the rank order of body sites (top 50% reported sites) by gender and overall
Table 3) Rank order of body sites (top 50% reported sites and 5-major body parts) for bodily sensation for all emotions by gender and overall
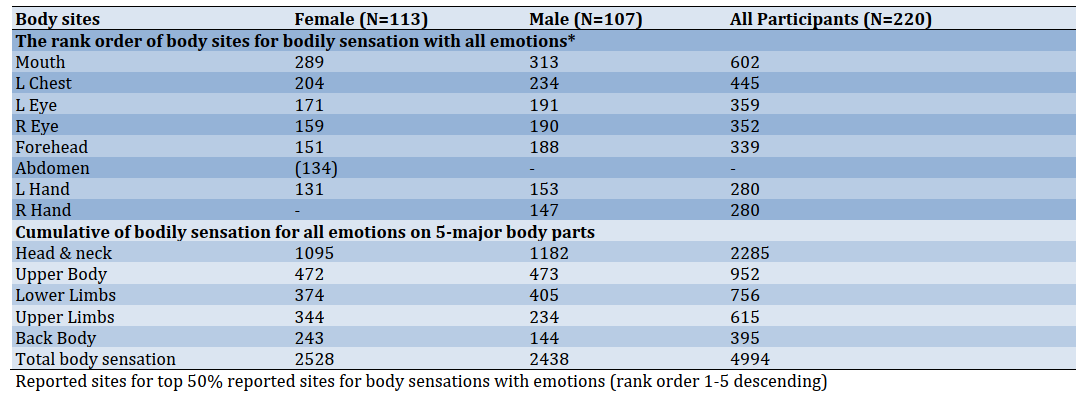
Table 4) Cumulative number of hits across six basic emotions plus anxiety by gender on 5-major body parts (N=220)
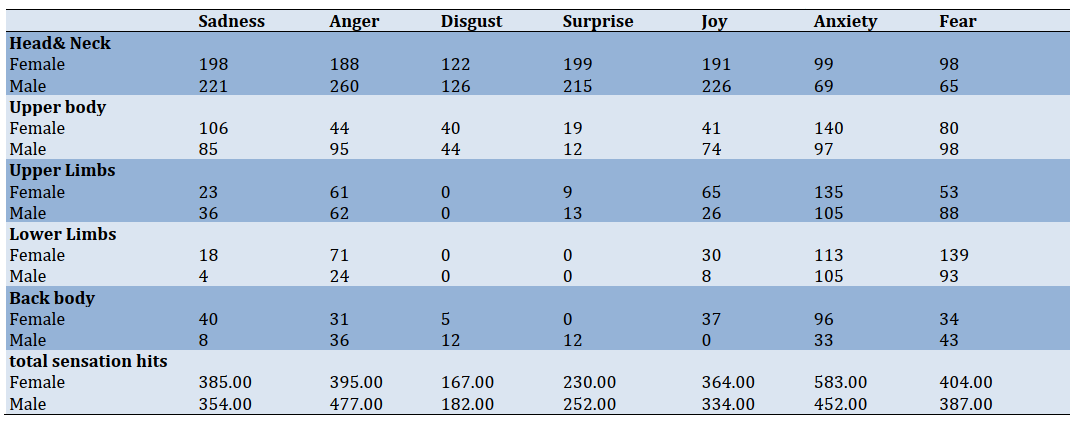
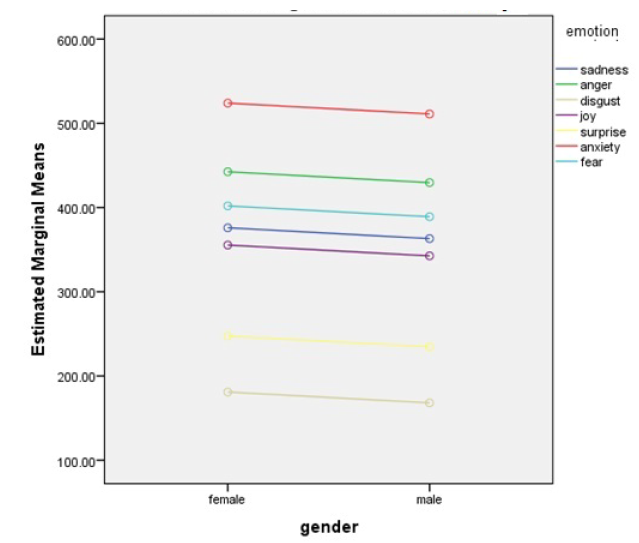
Figure 1) Gender*Emotion interaction on total body sensation; Gender for the Horizontal Axis and emotion for Separate Lines and plot gender*Emotion
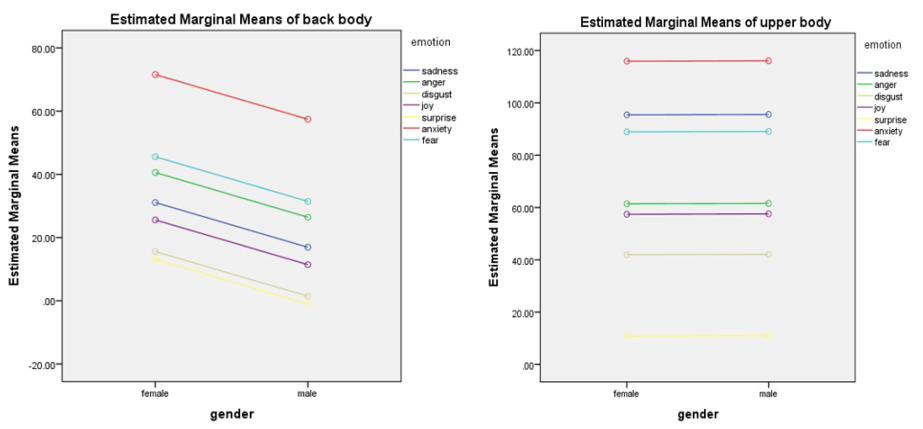
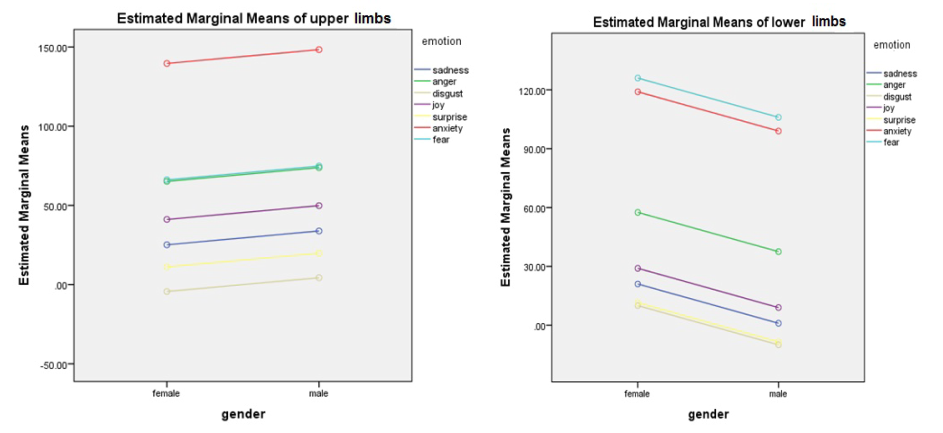
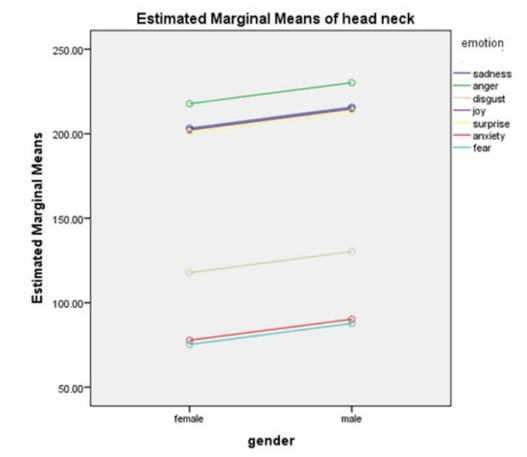
Figure 2) Gender*Emotion interaction on the upper body, back, upper & lower limbs, head, and neck; Gender for the Horizontal Axis and emotion for Separate Lines and plot gender*Emotion
The studied population reported the bodily sensation changes associated with all of the six basic emotions plus anxiety. Figures 1 and 2 represent the estimated marginal means of ERBCs (total bodily sensation and 5part - BSMs) across emotions by sex. Anxiety was the most reported and among the main six emotions, anger, fear, sadness, happiness, surprise, and disgust, respectively were associated with increased activity all over the body.
A general linear model (GLM) was conducted to investigate the interaction between perceived emotion and gender. Six basic discrete emotion and anxiety significantly predicted mean ratings for total EBRCs among Iranians (R2=0.93, p=0.004), and variance of the total body sensation was predicted with 92% accuracy by the emotion perceived (Table 4). The model for total body sensation also showed the absence of a significant interaction between gender and perceived emotions (p>0.05) in total ERBCs. When gender was adjusted for emotion perceived, it accounts for only 4.3% of the total variance of total bodily perceived emotion, so the assumption that regression slopes are similar for both sexes is justified. We accept the results of the original ANCOVA analysis (Table 5).
Table 5) General Linear Models predicting emotion-related body changes (EBCRs) and Emotion* Gender Interaction on five major body parts
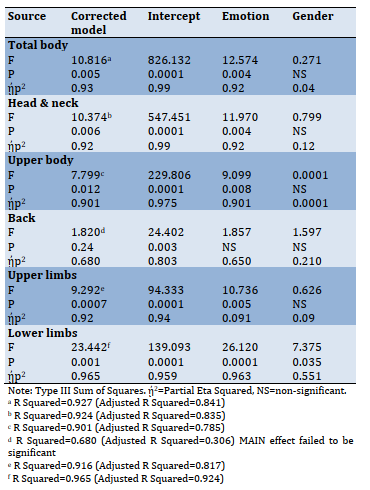
Similarly, the emotion perceived*gender interaction suggested no significant differences between genders in the head & neck, upper body, upper limbs, and facial parts across emotions. Tables 4 displays GLMs and the estimated effect sizes (partial ᾐp2) of the main effects and interactions for perceived emotions which were significant for ERBCs in head and neck, upper trunk, upper and lower limbs, and all three major facial parts with a cross-gender similarity (p<0.05).
Among participants, reported the subjective sensation of emotions, anxiety was the most prominent in the upper body, and sensations were shared across all emotions in this part. Figure 2 shows that BSMs are almost identical for both sexes across different emotions in the upper trunk (chest and stomach areas). Disgust has been reported in the corresponding parts of the digestive system and mouth.
Anxiety, fear, and anger in the back region are the most perceived emotions reported more by female participants, but the GLM for the interaction between gender and perceived emotions was not significant (Table 5). Table 5 shows the GLM for the interaction between perceived emotion and gender failed to significantly explain the variance between bodily sensation in the back body part. This finding is difficult to interpret because, as graph four indicated, female participants reported more marginal means in the back area than male participants. It may indicate a small sample size and reflect differences in the detection of emotion that has to be accounted for in this interpretation. However, we did not enter the analysis because of the limitation of our questionnaires and study design.
Anxiety separated early; fear and anger topographies were the most perceived emotions in the upper limb (Figure 2). In the lower limbs, women perceived anxiety, fear, anger, and happiness significantly more than men (p<0.05), while surprise, disgust, and sadness were the least perceived emotion in the lower limbs. The gender differences in differentiation of body sensations across emotions were found in lower limbs were significant (p<0.05), and gender accounts for about half of the total variance of bodily sensations in lower limbs (0.551*100=5.51%).
Participants reported anxiety and all six basic emotions in the head and neck area, whereas anger (i.e.an, approach-oriented emotion) was the most felt-changed emotion in the head and neck reflecting in facial areas (Table 6). The graph in Figure 3 indicates that while men reported relatively more estimated marginal means of ERBCs than women with no significant difference (p>0.05), anger separated early; happiness, surprise, and sad, clustered together followed by disgust separated and anxiety and fear in their cluster in head and neck for both genders. In the upper part of the face (head, forehead, and eyebrows), anger and sadness initially showed the most estimated means, following by happiness, surprise, anxiety, fear. The surprise was separated earlier in facial part 2 from other emotions, and sadness, anger, and happiness clustered (Figure 3). In facial part 3, participants reported disgust and happiness as the most reported emotions were associated with increased activity, followed by surprise and sadness and anger, clustered together, followed by anxiety and fear. There was no significant difference between the two sexes (p>0.05; Figure 3).
Table 4) Cumulative number of hits across six basic emotions plus anxiety by gender on 5-major body parts (N=220)
Figure 1) Gender*Emotion interaction on total body sensation; Gender for the Horizontal Axis and emotion for Separate Lines and plot gender*Emotion
Figure 2) Gender*Emotion interaction on the upper body, back, upper & lower limbs, head, and neck; Gender for the Horizontal Axis and emotion for Separate Lines and plot gender*Emotion
The studied population reported the bodily sensation changes associated with all of the six basic emotions plus anxiety. Figures 1 and 2 represent the estimated marginal means of ERBCs (total bodily sensation and 5part - BSMs) across emotions by sex. Anxiety was the most reported and among the main six emotions, anger, fear, sadness, happiness, surprise, and disgust, respectively were associated with increased activity all over the body.
A general linear model (GLM) was conducted to investigate the interaction between perceived emotion and gender. Six basic discrete emotion and anxiety significantly predicted mean ratings for total EBRCs among Iranians (R2=0.93, p=0.004), and variance of the total body sensation was predicted with 92% accuracy by the emotion perceived (Table 4). The model for total body sensation also showed the absence of a significant interaction between gender and perceived emotions (p>0.05) in total ERBCs. When gender was adjusted for emotion perceived, it accounts for only 4.3% of the total variance of total bodily perceived emotion, so the assumption that regression slopes are similar for both sexes is justified. We accept the results of the original ANCOVA analysis (Table 5).
Table 5) General Linear Models predicting emotion-related body changes (EBCRs) and Emotion* Gender Interaction on five major body parts
Similarly, the emotion perceived*gender interaction suggested no significant differences between genders in the head & neck, upper body, upper limbs, and facial parts across emotions. Tables 4 displays GLMs and the estimated effect sizes (partial ᾐp2) of the main effects and interactions for perceived emotions which were significant for ERBCs in head and neck, upper trunk, upper and lower limbs, and all three major facial parts with a cross-gender similarity (p<0.05).
Among participants, reported the subjective sensation of emotions, anxiety was the most prominent in the upper body, and sensations were shared across all emotions in this part. Figure 2 shows that BSMs are almost identical for both sexes across different emotions in the upper trunk (chest and stomach areas). Disgust has been reported in the corresponding parts of the digestive system and mouth.
Anxiety, fear, and anger in the back region are the most perceived emotions reported more by female participants, but the GLM for the interaction between gender and perceived emotions was not significant (Table 5). Table 5 shows the GLM for the interaction between perceived emotion and gender failed to significantly explain the variance between bodily sensation in the back body part. This finding is difficult to interpret because, as graph four indicated, female participants reported more marginal means in the back area than male participants. It may indicate a small sample size and reflect differences in the detection of emotion that has to be accounted for in this interpretation. However, we did not enter the analysis because of the limitation of our questionnaires and study design.
Anxiety separated early; fear and anger topographies were the most perceived emotions in the upper limb (Figure 2). In the lower limbs, women perceived anxiety, fear, anger, and happiness significantly more than men (p<0.05), while surprise, disgust, and sadness were the least perceived emotion in the lower limbs. The gender differences in differentiation of body sensations across emotions were found in lower limbs were significant (p<0.05), and gender accounts for about half of the total variance of bodily sensations in lower limbs (0.551*100=5.51%).
Participants reported anxiety and all six basic emotions in the head and neck area, whereas anger (i.e.an, approach-oriented emotion) was the most felt-changed emotion in the head and neck reflecting in facial areas (Table 6). The graph in Figure 3 indicates that while men reported relatively more estimated marginal means of ERBCs than women with no significant difference (p>0.05), anger separated early; happiness, surprise, and sad, clustered together followed by disgust separated and anxiety and fear in their cluster in head and neck for both genders. In the upper part of the face (head, forehead, and eyebrows), anger and sadness initially showed the most estimated means, following by happiness, surprise, anxiety, fear. The surprise was separated earlier in facial part 2 from other emotions, and sadness, anger, and happiness clustered (Figure 3). In facial part 3, participants reported disgust and happiness as the most reported emotions were associated with increased activity, followed by surprise and sadness and anger, clustered together, followed by anxiety and fear. There was no significant difference between the two sexes (p>0.05; Figure 3).
Table 6) General Linear Models predicting emotion-related body changes (EBCRs) and Emotion* Gender Interaction on Facial sensation parts
Figure 3) Gender*Emotion interaction on facial parts 1-3; Gender for the Horizontal Axis and emotion for Separate Lines and plot gender*Emotion
Discussion
Topographic evaluation of emotionally intensified physical changes can provide a unique tool for emotion studies as well as biomarkers for the detection of emotional disorders [3]. Our participants have reported emotional differentiation of body sensations for all six basic emotions and anxiety, and their reported patterns of BSM were consistent with universal patterns [10]. This finding agrees with [3] findings that showed that different emotions are associated with topographically distinct and culturally universal bodily sensations.
Contrary to expectations, our data suggest that total EBRCs for all different emotions do not differ between sexes. Graphs in the upper trunk were almost the same, and emotion perception in the back body, although showed greater mean scores for female participants, model failed to reach significance for both sexes. Similarly, men reported mean scores in head & neck and upper limbs, which failed to show a significant difference across genders.
Consistent with Nummenmaa et al.’s finding, our results reveal a gender-free similarity with universal patterns of BSM. Though in small sample sizes, some of the differences might not be detected because of lower statistical power. Therefore we suggest that issues related to interception such as emotional awareness- recognition of the connection between body sensations and emotional states and body listening - the tendency to actively listen to the body for insight, which is assumed to be different in both sexes, should be further investigated in future studies [30, 35].
Nonetheless, we found differences in the lower limb when comparing males and females in ERBCs, especially for fear, anxiety, and anger. Bear in mind, the generalizability of “weakening in the knees” as one of the most common bodily sensations with fear, anger [10] and anxiety, across studies and cross-cultural samples, is not surprising that these emotions were reported as the most perceived emotions in the lower limb. Nevertheless, interpretation for gender differences is more difficult. These differences can be explained in part by sex differences in noticing and emotional awareness [30, 35] with considering other potential sources of differences such as; the cultural meaning of the body sensation [10], gender stereotypes, and social desirability of this emotional sensation pattern [36]. Therefore, these factors could be suggested for further investigation in future studies.
Anxiety and anger were the most reported emotions associated with enhanced sensations all over the body with no significant emotion* gender interaction. The most striking result to emerge from the data is that, unlike our expectations and many researchers’ idea about the pervasive presence of sorrow in Persian culture [23], sadness was not the most prominent emotion through user-generated bodily sensation maps. The prior studies were mostly linguistic, have attempted to trace the manifestation of sadness in different areas of Iranian daily life using semantic methods and emotional terminology [18, 22, 23, 27]. Based on our knowledge, this study was the first research conducted to clarify the reported emotion-related BSM (for implicit detection of emotions) independence of emotion-related words in Iran. So, one can assume that those high-frequency sadness reports have emerged from stereotypical usage of non -exact terms connected with sadness for diverse subtle emotional states by Iranians, with more extended usage in the past [24].
Another explanation is assuming a transition from sadness to anxiety and anger that may have occurred in recent years in the Iranian population. Considering the interrelations between context, emotions, and individual and societal actions in conflict situations [37] and turning now to the historical evidence of socio-political changes in Iran, much of the anger and anxiety may stem from the catastrophic effects of economic instability during recent years due to prolong sanctions, the unpredictability of future and challenges of adaptation to all these events. It may contribute to learned helplessness and non-verbal and somatic modes of emotional expression [15, 38]. Our data must be interpreted with caution, though, because the design of the study and our questionnaires did not allow us to test whether this association is a culture-specific change or no.
Contrary to our expectation,” left chest “was not the first rank order of body sensation across emotions. There are many words for heart-focused emotions in Persian literature that do not essentially mean more emotional change on the left side of the chest [14]. In other words, what is called as heart “equal to Del in Farsi” in Persian metaphorical expressions of emotions equals a large part of the front upper trunk as well as mind and may not necessarily mean the heart [25]. Given that in many cultures, there are many words for the expression of the emotional state. Many of these terms are just metaphors and stereotypical bodily responses associated with emotions [3] and may not necessarily reflect physiological changes associated with different emotions (e.g., the word butterfly in the
stomach [3, 39].
However, a careful comparison cannot be made until a detailed study clarifies what specific bodily sensations are related to the expression of emotions through experiments using emotion induction techniques [3].
Moreover, the participants' reports of the most emotional perception in the mouth area may reflect the people's verbal culture at this point in the world. Probably reflecting the pattern of emotion suppression in Iranian culture in the presence of unwritten rules of politeness which sometimes prohibited Iranians from the verbal expressing of unpleasant feelings, they report an increased amount of feeling and increased pressure in their mouth area (i.e., Feeling pressure in teethes and teeth grinding during anger- which is not specified in this article). In recent decades, few Iranian researchers have attempted to explore possible causes of an intensified range of state-trait anger expression and aggression in the Iranian community [40-45]. However, with a small sample size and in the absence of any well-designed epidemiological study about the prevalence of anger in Iranians, caution must be applied.
Considering several devastating social and political events (i.e., Iraq-Iran war, natural disasters, and prolong economic and political sanctions against Iran) and in the context of vulnerability of Iranians for the somatization of anger and anxiety [15, 38], their patterns of anger management and emotion regulation have to be more studied in multidisciplinary researches.
As we know, negative emotions such as anger and fear are integral parts of the generation and experience of conflicts [37, 46]. Therefore, although it may be assumed as a very preliminary conclusion based on our findings, we just here want to imply the conceptual premise for” the long-term role of negative emotions in shaping conflictual interaction and conflict transformation” [37]. We hope that our findings serve as a base for future studies by social psychologists and practitioners in the field to understand more clearly Iranian individuals’ emotions and their collective behaviors and to facilitate conflict resolution approaches [37, 47-49] intent to re-establishing social cooperation and conducive to build the culture of peace in our population [37]. However, further studies on this topic need to be undertaken before associating negative emotions, and Iranians’ conflictual collective behaviors are more clearly understood.
Sensations of anger in the upper limb as an approach-oriented emotion align with a universal pattern [3, 10]. Anxiety, followed by fear and anger, is the most perceived emotion in this area, showing similarity to universal patterns [10].
Concerning Facial patterns, our results were in contrast to the upper face facial expression pattern in Western studies [49], reported as six “discrete" emotions, resembling the East Asian emotional expression pattern and showing an overlap for fear, surprise, anger, and sadness. However, in our study, anger and sadness were more distinct than other emotions. Although the studies mentioned were related to emotional expression and not to perceptions of emotions, our findings are not exactly comparable to the corresponding studies. Nevertheless, it can be cited as a basis for further studies on comparing emotion expression maps in the Iranian population.
Disgust and happiness were the most common emotions in the lower part of the face (mouth, cheeks, and chin) that resemble universal patterns in this respect. Surprisingly, sadness, anger, anxiety, and fear form a cluster that seems to resemble East Asian emotional expression patterns [49]. However, the compatibility of these patterns with patterns of emotional expression in the three facial areas should be explored in future studies.
Sensations in the digestive system and mouth region were mainly found in disgust, consistent with universal sensation patterns [3]. This result is also in line with finding a study by Breugelmans et al., which showed that “disgust is one of the basic emotions which appears to be better differentiated by body sensations across cultures” [10]. As the graph shows, our participants reported disgust as the least frequent emotion perceived in total bodily sensation map. Considering very little studies conducted about disgust emotion among Iranian individuals, questions raised about “the construct of emotion disgust” among Iranian people [50] and the association between disgust sensitivity and disorders such as obsessive compulsive disorder [50] and vaginismus [51]. Hence, further experimental investigations are needed.
Although it is a very preliminary study in the field of emotion study, these findings have important implications for developing the bodily map of the emotions and emotion sensation profile of Iranian people. Overall, the results of this study revealed similarity of Iranians’ EBRCs for six basic emotions and anxiety with universal patterns but considering few differences regarding facial patterns of emotion sensation and mouth as a top rank point of emotion sensation in our results, further investigation for comprehensive comparing Iranians’ emotional sensation patterns with common universal standards are suggested [3, 10].
Breugelmans et al. agree that “a combination of culture-specific and cross cultural approach” [10] should be applied for exact assessment of association between perceived emotions, embodied feelings, and unexplained somatic symptoms.
Finally, some important limitations need to be considered. First, the study sample size was small and was not included different subcultures of Iranian individuals. Second, we could not use the application mode of EmBODY questionnaire; hence our results could not exactly compare with EmBODY response profiles. Therefore, for future studies, we should consider a comparable android or IOS Farsi version of this application permitting from EmBODY manufacturers [3]. Third, in the absence of a constructivist view [6] and the characteristics of the Questionnaire we used, we did not consider socially constructed components of emotions that people use to express their body sensation [10, 52], such as metaphorical and linguistic components of emotions. So, the results of our study may not explicitly reflect the Iranian cultural specific variations in body sensation with emotions, which is a subject of further study.
Conclusion
The results suggested a gender-free consistency of distinct emotion-triggered bodily sensation maps of Iranians with universal patterns. The total EBRCs for all different emotions do not differ between sexes, but regarding 5-main body areas, a significant gender difference was observed in lower limbs.
Acknowledgments: We gratefully acknowledge the staff of the psychosomatic center and our participants.
Ethical Permissions: The research was approved by Isfahan University of Medical Sciences, Ethical Committee (IR.MUI.REC.1395.2.256).
Conflicts of Interests: This article is a part of a research project approved by Psychosomatic Research Center, Faculty of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran (Code: 295256). No potential conflict of interest was reported by the authors.
Authors’ Contribution: Molaeinezhad M (First Author), Introduction Writer/Main Researcher/Statistical Analyst/Discussion Writer (40%); Scheidt C.E. (Second Author), Methodologist/Discussion Writer (10%); Afshar H. (Third Author), Introduction Writer/Discussion Writer (10%); Jahanfar Sh. (Forth Author), Statistical Analyst/Discussion Writer (15%); Sohran F. (Fifth Author), Assistant Researcher (5%); Salehi M. (Sixth Author), Assistant Researcher (5%); Goli F. (Seventh Author), Introduction Writer/Discussion Writer (15%)
Funding/Support: The grant supported by Isfahan University of Medical Sciences, Psychosomatic Research Center is acknowledged.
Article Type: Original Research |
Subject:
Social Health
Received: 2020/11/11 | Accepted: 2021/02/26 | Published: 2021/07/11
Received: 2020/11/11 | Accepted: 2021/02/26 | Published: 2021/07/11
References
1. Ekman P. An argument for basic emotions. Cogn Emot. 1992;6(3-4):169-200. [Link] [DOI:10.1080/02699939208411068]
2. Kassam KS, Markey AR, Cherkassky VL, Loewenstein G, Just MA. Identifying emotions on the basis of neural activation. PLoS One. 2013;8(6):66032. [Link] [DOI:10.1371/journal.pone.0066032] [PMID] [PMCID]
3. Nummenmaa L, Glerean E, Hari R, Hietanen JK. Bodily maps of emotions. Proc Natl Acad Sci. 2014;111(2):646-51. [Link] [DOI:10.1073/pnas.1321664111] [PMID] [PMCID]
4. Damasio A, Carvalho GB. The nature of feelings: Evolutionary and neurobiological origins. Nat Rev Neurosci. 2013;14(2):143-52. [Link] [DOI:10.1038/nrn3403] [PMID]
5. Hietanen JK, Glerean E, Hari R, Nummenmaa L. Bodily maps of emotions across child development. Dev Sci. 2016;19(6):1111-8. doi:10.1111/desc.12389 [Link] [DOI:10.1111/desc.12389] [PMID]
6. Philippot P, Rime B. The perception of bodily sensations during emotion: A cross-cultural perspective. Pol Psychol Bull. 1997;28(2):175-88. [Link]
7. Matsumoto D, Kudoh T, Scherer K, Wallbott H. Antecedents of and reactions to emotions in the United States and Japan. J Cross Cult Psychol. 1988;19(3):267-86. [Link] [DOI:10.1177/0022022188193001]
8. Matsumoto D, Ekman P. American-Japanese cultural differences in intensity ratings of facial expressions of emotion. Motiv Emot. 1989;13(2):143-57. [Link] [DOI:10.1007/BF00992959]
9. Dzokoto V. Different ways of feeling: Emotion and somatic awareness in Ghanaians and Euro-Americans. J Soc Evolut Cult Psychol. 2010;4(2):68-78. [Link] [DOI:10.1037/h0099299]
10. Breugelmans SM, Ambadar Z, Vaca JB, Poortinga YH, Setiadi B, Widiyanto P, et al. Body sensations associated with emotions in Raramuri Indians, rural Javanese, and three student samples. Emotion. 2005;5(2):166-74. [Link] [DOI:10.1037/1528-3542.5.2.166] [PMID]
11. Kitayama S, Markus HR. The pursuit of happiness and the realization of sympathy: Cultural patterns of self, social relations, and well-being. In: Diener E, Suh EM. Culture and subjective well-being. Cambridge: The MIT Press; 2000. [Link]
12. Kitayama S, Markus HR, Kurokawa M. Culture, emotion, and well-being: Good feelings in Japan and the United States. Cogn Emot. 2000;14(1):93-124. [Link] [DOI:10.1080/026999300379003]
13. Tsai JL, Knutson B, Rung HH. Cultural variation in affect valuation. J Pers Soc Psychol. 2006;90(2):288-307. [Link] [DOI:10.1037/0022-3514.90.2.288] [PMID]
14. Good BJ. The heart of what's the matter: The semantics of illness in Iran. Cult Med Psychiatry. 1977;1(1):25-58. [Link] [DOI:10.1007/BF00114809] [PMID]
15. Malekian A, Ahamadzadeh G, Afshar H. Cultural issues in anxiety disorders: Some particularities of the Iranian culture. Eur Psychiatry. 2013;28(1):1. [Link] [DOI:10.1016/S0924-9338(13)75943-1]
16. Novin S, Banerjee R, Dadkhah A, Rieffe C. Self-reported use of emotional display rules in the Netherlands and Iran: Evidence for sociocultural influence. Soc Dev. 2009;18(2):397-411. [Link] [DOI:10.1111/j.1467-9507.2008.00485.x]
17. Dadkhah A, Shirinbayan P. Emotion regulation characteristics development in Iranian primary school pupils. Iran Rehabil J. 2014;12(4):17-21. [Persian] [Link]
18. Beeman WO. Emotion and sincerity in Persian discourse: Accomplishing the representation of inner states. Int J Soc Lang. 2001;148:31-57. [Link] [DOI:10.1515/ijsl.2001.013]
19. Pliskin KL. Dysphoria and somatization in Iranian culture. West J Med. 1992;157(3):295-300 [Link]
20. Surdykowska S. Martyrdom and ecstasy: Emotion training in Iranian culture. Newcastle upon Tyne: Cambridge Scholars Publishing; 2012. [Link]
21. Surdykowska S. The idea of sadness: The richness of Persian experiences and expressions. Rocz Orient. 2014;2:68-80. [Link]
22. Pirzad Mashak S, Pazhakh A, Hayati A. A comparative study on basic emotion conceptual metaphors in English and Persian literary texts. Int Educ Stud. 2012;5(1):200-7. [Link] [DOI:10.5539/ies.v5n1p200]
23. Shahshahani S. Body as a means of non-verbal communication in Iran. Int J Mod Anthropol. 2008;1:65-81. [Link]
24. Sharifian F, Culture, body and language: Conceptualizations of internal body organs across cultures and languages. Berlin: Mouton de Gruyter; 2008. [Link] [DOI:10.1515/9783110199109]
25. Imani A, Rafie A, Amoozadeh M. A socio-constructal analysis of "Del" (heart) in Persian language in Linguistic literature. Ling Res J. 2014;9(2):33-42. [Persian] [Link]
26. Riegel M, Moslehi A, Michalowski JM, Zurawski L, Horvat M, Wypych M, et al. Nencki affective picture system: Cross-cultural study in Europe and Iran. Front Psychol. 2017;8:274. [Link] [DOI:10.3389/fpsyg.2017.00274] [PMID] [PMCID]
27. Garcia-Magarino I, Chittaro L, Plaza I. Bodily sensation maps: Exploring a new direction for detecting emotions from user self-reported data. Int J Hum Comput Stud. 2018;113:32-47. [Link] [DOI:10.1016/j.ijhcs.2018.01.010]
28. Pennebaker JW, Roberts TA. Toward a his and hers theory of emotion: Gender differences in visceral perception. J Soc Clin Psychol. 1992;11(3):199-212. [Link] [DOI:10.1521/jscp.1992.11.3.199]
29. Grabauskaite A, Baranauskas M, Griskova-Bulanova I. Interoception and gender: What aspects should we pay attention to. Conscious Cogn. 2017;48:129-37. [Link] [DOI:10.1016/j.concog.2016.11.002] [PMID]
30. Tabachnik BG, Fidell LS. Using multivariate statistics. Boston: Allyn and Bacon; 2001. [Link]
31. Brummett CM, Bakshi RR, Goesling J, Leung D, Moser SE, Zollars JW, et al. Preliminary validation of the Michigan body map. Pain. 2016;157(6):1205-12. [Link] [DOI:10.1097/j.pain.0000000000000506] [PMID] [PMCID]
32. Ekman P, Friesen WV, Tomkins SS. Facial affect scoring technique: A first validity study. Semiotica. 1971;3(1):1. [Link] [DOI:10.1515/semi.1971.3.1.37]
33. Taylor A. Using the GLM procedure in SPSS. Sydney: Macquarie University; 2011. [Link]
34. Mehling WE, Acree M, Stewart A, Silas J, Jones A. The multidimensional assessment of interoceptive awareness, version 2 (MAIA-2). PLoS One. 2018;13(12):0208034. [Link] [DOI:10.1371/journal.pone.0208034] [PMID] [PMCID]
35. Zargar F, Asgharnejad Farid AA, Atef-Vahid MK, Afshar H, Maroofi M, Omranifard V. Effect of acceptance-based behavior therapy on severity of symptoms, worry and quality of life in women with generalized anxiety disorder. Iran J Psychiatry Behav Sci. 2012;6(2):23-32. [Link]
36. Skladankowa M. Iran-paradygmaty wyobrazni (II). Acta Asiat Varsoviensia. 1993;7:38-9. [Link]
37. Bramsen I, Poder P. Emotional dynamics in conflict and conflict transformation. Berlin: Berghof Foundation; 2018. [Link]
38. Hosseini SH, Mokhberi V, Ali Mohammadpour R, Mehrabianfard M, Bali Lashak N. Anger expression and suppression among patients with essential hypertension. Int J Psychiatry Clin Pract. 2011;15(3):214-8. [Link] [DOI:10.3109/13651501.2011.572168] [PMID]
39. Harre R. The social construction of emotions. Oxford: Blackwell; 1989. [Link]
40. Baghaei Lake M, Khalatbari J. Effectiveness of anger management program training on control and self-regulation of anger and impulsivity of mothers of male students of primary schools of Rasht. J Holist Nurs Midwifery. 2010;20(63):1-9. [Persian] [Link]
41. Shokouhi Yekta M, Zamani N, Parand A, Akbari Zardkhaneh S. The effectiveness of anger management training on parents' anger expression and control. Dev Psychol. 2011;7(26):137-46. [Persian] [Link]
42. Khodayari Fard M, Lavasani MG, Akbari Zardkhane Liaghat S. Standardization of Spielberger's State-trait anger expression inventory II for Iranian students. Arch Rehabil. 2010;11(1):47-56. [Persian] [Link]
43. Asghari Moghadam MA, Hakimi Rad E, Rezazadeh T. Preliminary validation of the revised version of the anger expression trait questionnaire in the student population. Daneshvar Behav. 2008;15(28):21-34. [Persian] [Link]
44. Moheba N, Ram U. Cross-cultural study of stress and anger. Proced Soc Behav Sci. 2010;5:1765-9. [Link] [DOI:10.1016/j.sbspro.2010.07.361]
45. Shahsavarani AM, Noohi S. Explaining the bases and fundamentals of anger: A literature review. Int J Med Rev. 2014;1(4):143-9. [Link]
46. Crawford NC. The passion of world politics: Propositions on emotion and emotional relationships. Int Secur. 2000;24(4):116-56. [Link] [DOI:10.1162/016228800560327]
47. Brewer JD. Peace processes: A sociological approach. Hoboken: Wiley; 2010. [Link]
48. Brudholm T. Resentment's virtue: Jean Amery and the refusal to forgive. Philadelphia: Temple University Press; 2009. [Link]
49. Chakravarti S. Sing the rage: Listening to anger after mass violence. Chicago: The University of Chicago Press; 2014. [Link] [DOI:10.7208/chicago/9780226120041.001.0001]
50. Jack RE, Garrod OGB, Yu H, Caldara R, Schyns PG. Facial expressions of emotion are not culturally universal. Proc Natl Acad Sci USA. 2012;109(19):7241-4. [Link] [DOI:10.1073/pnas.1200155109] [PMID] [PMCID]
51. Shams G, Janani L, Milosevic I, Foroughi E. Disgust emotion and obsessive-compulsive symptoms in an Iranian clinical sample. Psychology. 2015;6(13):1721-31. [Link] [DOI:10.4236/psych.2015.613168]
52. Overton PG, Powell PA, Simpson J. The revolting self: Perspectives on the psychological and clinical implications of self-directed disgust. Abingdon: Routledge; 2015. [Link]
53. Ots T. The angry liver, the anxious heart, and the melancholy spleen: The phenomenology of perceptions in Chinese culture. Cult Med Psychiatry. 1990;14(1):21-58. [Link] [DOI:10.1007/BF00046703] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |