



Volume 9, Issue 2 (2021)
Health Educ Health Promot 2021, 9(2): 111-117 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bagheri M, Niknami S, Rahmati Najarkolaei F. Effect of Communication Skills Training of the Elderly and their Caregivers’ on Elderly Lifestyle. Health Educ Health Promot 2021; 9 (2) :111-117
URL: http://hehp.modares.ac.ir/article-5-46670-en.html
URL: http://hehp.modares.ac.ir/article-5-46670-en.html
1- Department of Health Education & Health Promotion, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
2- Department of Health Education & Health Promotion, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran ,Niknamis@modares.ac.ir
3- Health Research Center, Lifestyle Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran
2- Department of Health Education & Health Promotion, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran ,
3- Health Research Center, Lifestyle Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran
Full-Text [PDF 443 kb]
(3468 Downloads)
| Abstract (HTML) (1904 Views)
Full-Text: (1026 Views)
Introduction
In the second half of the twentieth century, increasing life expectancy was the positive result of social, economic, and health system development worldwide, with the natural consequence of an aging population [1]. Therefore, paying attention to the problems and the needs of the elderly is a social necessity, so that, with a healthy life and special care, this period becomes desired and healthy for the elderly [2]. Considering the important role of health-promoting behaviors in health and life expectancy, it can be concluded that adopting a healthy lifestyle in the elderly is very important [3]. According to Walker's definition, a health-promoting lifestyle is a multidimensional model of perceptions and actions that starts with self-motivation and helps one maintain and enhance one's health and make it closer to real-life [4]. Having an unhealthy lifestyle is a major cause of early deaths and non-preventive complications and diseases among the elderly. Promoting personal health behaviors is the most important and effective factor in enhancing life expectancy and maintaining and promoting health in the elderly [5].
The majority of older individuals have one or two chronic diseases, leading to premature aging and changes in their communication patterns [6]. Thus, this group of individuals may need to communicate with others to meet their daily needs and to benefit from health care, home care, hospitalization, and in some cases, nursing homes [7]. The results of a study showed that about one-quarter of 70-year-olds for managing their daily lives, and the other half of them, because of their old age for daily activities, rely on help and communication with others [8]. The Human is a social being, and communicating with others in its life is considered normal; understanding the importance of communicating with others and eliminating communication disabilities can be important for a healthy lifestyle. Therefore, social and interpersonal relationships are one of the dimensions of a healthy lifestyle [9].
To address the communication disabilities of the elderly, the focus of the interventions should be on both participants because communication involves the exchange between two individuals with a set of communication skills, and the most important thing is understanding each other's point of view, the stronger the understanding, the more effective the communication will be [10]. The deficiency of Communication skills with increasing age causes family problems, stress, stress physical illnesses [11], Social isolation, loneliness, and social vulnerability [12]. By learning these skills, individuals can use different communication approaches to respond to a wide range of needs in different situations [13]. Communication skills can be learned and practiced, and a set of learned communication skills become integrated skilled communication and used purposefully in social, clinical, and health care communications [14]. It should be noted that similar studies, including studies by Visser et al. and [15] Palmer et al. [16], showed that desired communication skills enable the elderly to share more accurate messages through effective communication, let them enjoy their old age by managing their conflicts with others. It seems that individuals with disabilities in the communication process appear to face many challenges in areas such as maintaining social roles, jobs, identity, and access to needed services such as health care [17].
Although research in this field is still limited, preliminary evidence suggests that many of the problems associated with aging are rooted in the lack of communication skills [18]. Because of the complex and chronic nature of many communication disabilities experienced in old age, interventional measures should include strategies to minimize communication disabilities. These strategies may be helpful with the participation of the elderly and the second person who plays an important role in the decision-making and activities of the elderly.
Regarding the importance of caregiver-centered communication skills training for the care of the elderly, which is one of the health system's challenges, the study aimed to determine the effect of interpersonal communication skills training of the elderly and caregivers on the lifestyle of the elderly.
Materials and Methods
This quasi-experimental study was conducted on 140 elderly and their caregiver in Khorzugh, Isfahan province, in 2018. A stratified random sampling method was used. Among the city's four districts, two districts with similar cultural, social, and economic levels were selected. Of two districts, using the random method, one district was selected as an experiments group and another district as the control group. Participants were selected by random sampling method from these groups. The sample size was determined based on the results of the conducted studies with a 95% confidence level, 80% statistical error, and 10% drop [19], which reached 70 subjects in the experimental and control groups. The inclusion criteria for the elderly included age 60 years and over, lack of cognitive and mental disorders that impede learning and transferring the content, a score less than 135 obtained from the Health-Promoting Lifestyle Questionnaire, and a score less than 103 obtained the Interpersonal Communication Skills Questionnaire. The inclusion criteria for the caregivers of the elderly were caring for the elderly at home, lack of cognitive and mental disorders that impede learning and transferring content, and obtaining a score less than 103 on the Communication Skills Questionnaire. Participants who withdrawal from cooperation, unwilling to attend training sessions, and the incomplete questionnaires were excluded from the study.
The study tool consisted of a 3-part questionnaire. The first part included information on age, gender, marital status, education level, occupation for all participants, and type of diseases, number of children, and living conditions for the elderly only. The second part included a standardized interpersonal communication skills test. This questionnaire has 34 five-choice questions (never, rarely, sometimes, most often and always) to measure five skills of listening, ability to receive and send messages, vision to the communication process, excitement control, and communication with certainty in adults [20]. The reliability and validity of this questionnaire were confirmed by Hosseinchari & Fedakar [20], and Cronbach's alpha for this test has been reported 0.69. The stability of measurements, validity, and reliability of this questionnaire has also been reported as high and acceptable [20]. Because four levels of weak, average, good, excellent, were considered, the division was done as follows: scores 33-67 show weak communication skill; 68-102: moderate communication skill; 103-137: good communication skill; and 138-171: excellent. The third part included the Health-Promoting Lifestyle Questionnaire with 52 questions to measure spiritual growth behaviors, responsibility for health, interpersonal relation, stress management, physical activity, and nutrition, as modified by Walker et al. [21]. Also, Walker et al. [21] and Mohammadi Zeidi et al. [22] reported the reliability of this questionnaire as 0.94 and 0.82, respectively. Because three levels of weak, average, good were considered, the division was done as follows: scores 51-103 show weak communication skill; 104-156: moderate communication skill; and 157-209: good communication skill.
The study process started after receiving the code of medical ethics IR: TMU.REC.1396.662 and official introduction letter of Tarbiat Modares University research deputy. The questionnaires were filled out by the participants' self-report; though, due to the illiteracy of most of the participants, the researcher's cooperation was also used. After reviewing the pre-test results, educational priorities were identified based on the needs of the audience and the purpose of the study. Finally, the educational content was developed and implemented in the experimental group by reviewing relevant texts, including reference books, theses, published papers, experts' and research teams' opinions. A total of 180min of interpersonal communication skills training for the caregivers and the elderly experimental group were conducted separately during four weeks. According to the conditions of the elderly and at the request of the participants, training sessions were held in the house of one of them. But no training was provided for the control group. The caregiver and the elderly experimental group received information with identical explanations in two separate sessions to increase awareness. To develop communication skills and transform the content of theory into practical skills, eliminate wrong inferences, and answering the questions, the method of presentation, group discussion, and consultation for the experimental group were used. The outline of the first and second training sessions included familiarizing the elderly and caregivers with how to conduct research, the concept of communication, the importance and purpose of communication skills, communication obstacles, different communication personalities and styles, and effective tips on facilitating communication. The outline of the third and fourth training sessions included acquaintance of the elderly and caregivers with verbal and nonverbal communication skills, interpersonal communication skills, interpersonal communication obstacles, opposition, and non-opposition management and interpersonal communication skills, key points of how to communicate with the elderly (caregivers) effectively, the ability to manage the pressures of care and prevent the effect on interpersonal relations (caregivers) and key points on how to communicate effectively with caregivers to express their needs and problems (the elderly) held in a lecture with a presentation for the elderly and their caregivers separately. These sessions also included topics such as starting a hello greeting, making eye contact, speaking at a modest pace, simplifying and using common words, prioritizing what to discuss and emphasizing key points, repeating key points, the elderly and caregivers' participation, encourage them to ask questions. Also, during training, participants improved communication so that participants better accept recommendations and training and understand the content presented. The experimental group was also asked not to share the educational content with others until the end of the study. 2 months after the training, the questionnaires were completed again by both the experimental and control groups.
Scores of each questionnaire were recorded using SPSS 25 software. The descriptive statistics, mean±SD were used to describe the state of the subjects, and for data analysis, at a significance level 0.05, Mann-Whitney, Kolmogorov–Smirnov, Wilcoxon, and Spearman tests were used. The normal distribution of data was controlled by the Kolmogorov-Smirnov test. The Mann-Whitney test was applied to compare demographic data of the intervention and control groups before the intervention. Wilcoxon test was used to compare the pre-test and post-test scores. Spearman test was used to show the correlation between elderly and caregivers’ communication skills variables with elderly lifestyle variables.
Findings
The mean age of the caregivers of the elderly in the experimental and control groups were 55.01±6.38 and 54.44±6.22 years, respectively. Moreover, the mean age of the elderly in the experimental and control groups were 66.39±6.16 and 66.47±6.41 years (Table 1). No statistically significant difference was found between the experimental and control groups of the elderly and caregivers in terms of demographic variables for performing the intervention (p>0.05).
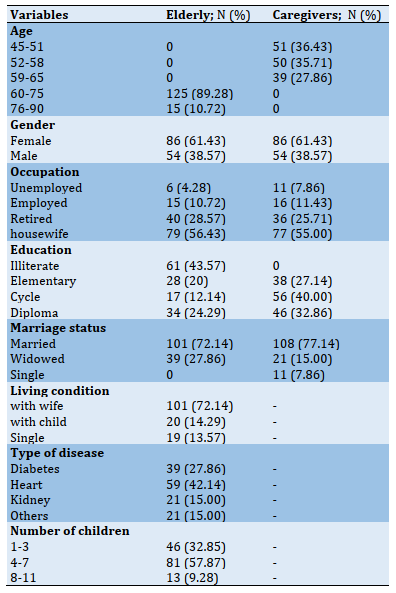
Table 1) Frequency distribution of individual variables in the elderly and their caregiver
The study results showed that communication skills training significantly increased the experimental group of caregivers and the elderly (Tables 2 and 3).
The mean±SD score of communication skills and lifestyle for the elderly were 90.56±4.00 and 107.34±9.14, respectively (Tables 3 and 4). The total score of lifestyle in both experimental and control groups of the elderly (Table 4) and the total score of communication skills in both experimental and control groups of the elderly (Table 3) and their caregivers (Table 2) were at the same level before the intervention. They were not significantly different (p>0.05), but two months after the training intervention, this difference was significant (p<0.001).
No significant difference was observed in the mean score of the spiritual dimension between the experimental and control groups before and after two months of the intervention (p>0.05). According to the obtained results, implementation of educational intervention did not affect the spiritual dimension of the elderly (p>0.05); but it was effective on other dimensions of their healthy lifestyle (p<0.001; Table 4).
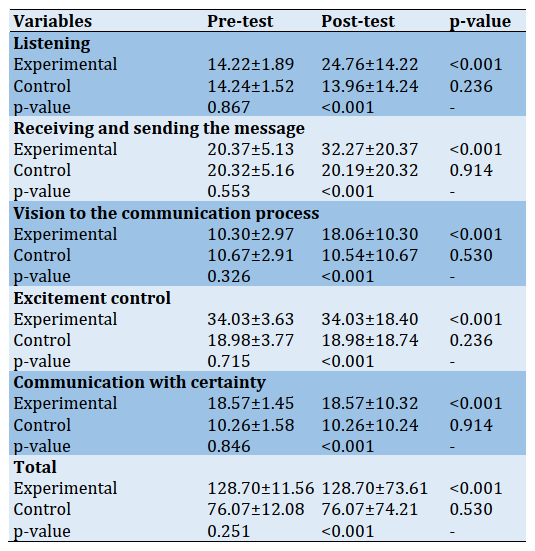
Table 2) Comparison of the mean±SD score of the total communication skills and its dimensions between the experimental and control groups of the caregivers before and after two months of the educational intervention
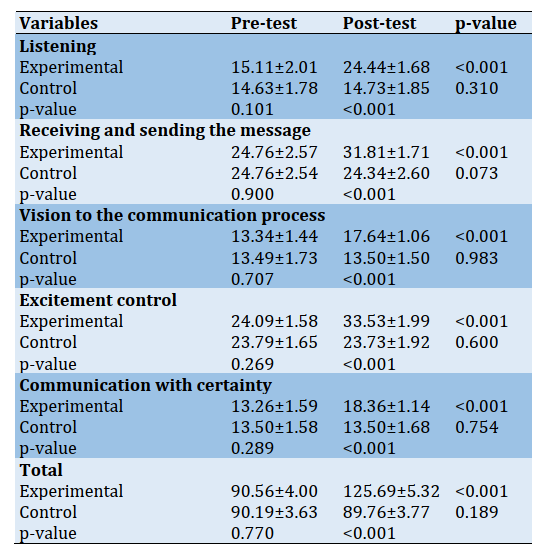
Table 3) Comparison of the mean±SD score of the total communication skills and its dimensions between the experimental and control groups of the elderly before and after two months of the educational intervention
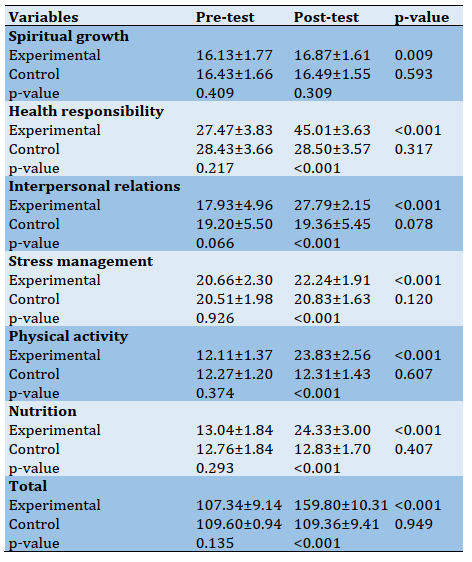
Table 4) Comparison of the mean±SD lifestyle score and its different dimensions between the experimental and control elderly groups before and after two months of the educational intervention
Discussion
The present study results showed that the mean lifestyle score of the elderly according to the Walker questionnaire before the intervention was at the mean level, which is consistent with the results of other studies [23, 24]. While in the other studies, the mean lifestyle score was at a desirable status [25, 26]. It can be predicted that the geographic location and ethnic, economic, cultural, and social differences can affect their lifestyle. Also, in the present study, the mean score of communication skills of the elderly according to the Queendam questionnaire before the intervention was at the moderate level like Siamian's study [27]. In some studies, the mean score of communication skills was weak [28, 29]. While in a study by Mojadam et al., the level of communication skills of the elderly was well reported [30]. It seems that these differences are due to the method of completing the questionnaire, questionnaire type, age of the studied population, cultural and social differences, and other demographic characteristics of the research community.
This study tries to investigate the effect of the caregiver and elderly communication skills training on the lifestyle of the elderly. Diagnosis of communication skills in the elderly is necessary because communication skills are very important in interpersonal relationships. Furthermore, the elderly's communication functions change in normal aging at different rates, and it is important to notify
the elderly's family about these changes. Accordingly, the main issues here concern communication difficulties in elderly relations and their determinants [14]. According to the results, communication skills training significantly increased the communication skills of the experimental group of caregivers and the elderly. The results of the present study are consistent with the results of the study done by Sprangers et al. [31], Heidari et al. [32], and Basiri et al. [33] but inconsistent with the results of the study done by Rask et al. [34] The cause of the existing difference can be attributed to the type of skills training and follow-up after the intervention. Therefore, communication skills training is a tool for helping the elderly and their caregivers to communicate effectively so that by changing inappropriate behaviors, they can prevent destructive interactions and help the elderly participate in social activities and avoid loneliness [35].
The effect of the training intervention on the total score of lifestyle and its dimensions in the elderly experimental group is another result of this intervention consistent with other studies [15, 24, 36]. Therefore, the elderly should be provided with the necessary knowledge to engage in healthy behaviors through basic training to enjoy a longer life without disabilities.
According to the obtained results, no significant difference was observed in the mean score of the spiritual dimension between the experimental and control groups before and after two months of the intervention. Implementation of educational intervention did not affect the spiritual dimension of the elderly, but it was effective on other dimensions of their healthy lifestyle. This could mean this educational intervention alone could not positively affect all dimensions of the lifestyle of the elderly.
The present study results are consistent with the results of the study done by Movahedi et al. [37] but inconsistent with the results of the study done by Sobhani et al. [38].
It seems that the spiritual health of the elderly depends on various factors such as religion [39], demographic, family factors, levels of worry about death, coping with problems, personal life events, having physical and mental health, levels of social activity, and purposefulness in life [40]. Regarding the difference in the level of spirituality of individuals in different settings, it is suggested that future interventions for the development of care and education programs should consider the above to improve the spiritual health of the elderly. The limitations of the present study include the low literacy of most participants and the time required to complete the two questionnaires, which resulted in wasting time so the sampling process lasted more until the sample size was sufficient enough to be able to perform the first stage of the study.
Conclusion
Communication skills training for caregivers and the elderly positively correlates with the level of the lifestyle of the elderly. This training improves the level of lifestyle and its dimensions (except spiritual growth) in the elderly group and the level of total communication skills and its dimensions in the caregiver and the elderly. Observing a healthy lifestyle, receiving health promotion training, and improving social relationships have a significant effect on improving health and increasing life expectancy in the elderly, and failure to observe the lifestyle indicators can aggravate the aging process.
Acknowledgments: The authors express their gratitude to the research deputy of Tarbiat Modares University, and they would like to express their gratitude and appreciation to elderlies and their caregivers because of their sincere cooperation.
Ethical Permissions: This article is part of the MSc thesis on health education and health promotion with the number 2017.662 in Tarbiat Modares University's ethics committee: TR.TMU.REC.2017.662.
Conflicts of Interests: The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Authors’ Contribution: Marjan Bagheri (First author), Introduction author/Methodologist/Original researcher/Statistical analyst/Discussion author (40%); Shamsaddin Niknami (Second author), Methodologist/Assistant/Discussion author (30%); Fatemeh Rahmati Najarkolaei (Third author), Methodologist/Assistant/Discussion author (30%).
Funding/Support: This article is part of MSc thesis on health education and health promotion with the number 2017.662 in Tarbiat Modarres University's ethics committee.
In the second half of the twentieth century, increasing life expectancy was the positive result of social, economic, and health system development worldwide, with the natural consequence of an aging population [1]. Therefore, paying attention to the problems and the needs of the elderly is a social necessity, so that, with a healthy life and special care, this period becomes desired and healthy for the elderly [2]. Considering the important role of health-promoting behaviors in health and life expectancy, it can be concluded that adopting a healthy lifestyle in the elderly is very important [3]. According to Walker's definition, a health-promoting lifestyle is a multidimensional model of perceptions and actions that starts with self-motivation and helps one maintain and enhance one's health and make it closer to real-life [4]. Having an unhealthy lifestyle is a major cause of early deaths and non-preventive complications and diseases among the elderly. Promoting personal health behaviors is the most important and effective factor in enhancing life expectancy and maintaining and promoting health in the elderly [5].
The majority of older individuals have one or two chronic diseases, leading to premature aging and changes in their communication patterns [6]. Thus, this group of individuals may need to communicate with others to meet their daily needs and to benefit from health care, home care, hospitalization, and in some cases, nursing homes [7]. The results of a study showed that about one-quarter of 70-year-olds for managing their daily lives, and the other half of them, because of their old age for daily activities, rely on help and communication with others [8]. The Human is a social being, and communicating with others in its life is considered normal; understanding the importance of communicating with others and eliminating communication disabilities can be important for a healthy lifestyle. Therefore, social and interpersonal relationships are one of the dimensions of a healthy lifestyle [9].
To address the communication disabilities of the elderly, the focus of the interventions should be on both participants because communication involves the exchange between two individuals with a set of communication skills, and the most important thing is understanding each other's point of view, the stronger the understanding, the more effective the communication will be [10]. The deficiency of Communication skills with increasing age causes family problems, stress, stress physical illnesses [11], Social isolation, loneliness, and social vulnerability [12]. By learning these skills, individuals can use different communication approaches to respond to a wide range of needs in different situations [13]. Communication skills can be learned and practiced, and a set of learned communication skills become integrated skilled communication and used purposefully in social, clinical, and health care communications [14]. It should be noted that similar studies, including studies by Visser et al. and [15] Palmer et al. [16], showed that desired communication skills enable the elderly to share more accurate messages through effective communication, let them enjoy their old age by managing their conflicts with others. It seems that individuals with disabilities in the communication process appear to face many challenges in areas such as maintaining social roles, jobs, identity, and access to needed services such as health care [17].
Although research in this field is still limited, preliminary evidence suggests that many of the problems associated with aging are rooted in the lack of communication skills [18]. Because of the complex and chronic nature of many communication disabilities experienced in old age, interventional measures should include strategies to minimize communication disabilities. These strategies may be helpful with the participation of the elderly and the second person who plays an important role in the decision-making and activities of the elderly.
Regarding the importance of caregiver-centered communication skills training for the care of the elderly, which is one of the health system's challenges, the study aimed to determine the effect of interpersonal communication skills training of the elderly and caregivers on the lifestyle of the elderly.
Materials and Methods
This quasi-experimental study was conducted on 140 elderly and their caregiver in Khorzugh, Isfahan province, in 2018. A stratified random sampling method was used. Among the city's four districts, two districts with similar cultural, social, and economic levels were selected. Of two districts, using the random method, one district was selected as an experiments group and another district as the control group. Participants were selected by random sampling method from these groups. The sample size was determined based on the results of the conducted studies with a 95% confidence level, 80% statistical error, and 10% drop [19], which reached 70 subjects in the experimental and control groups. The inclusion criteria for the elderly included age 60 years and over, lack of cognitive and mental disorders that impede learning and transferring the content, a score less than 135 obtained from the Health-Promoting Lifestyle Questionnaire, and a score less than 103 obtained the Interpersonal Communication Skills Questionnaire. The inclusion criteria for the caregivers of the elderly were caring for the elderly at home, lack of cognitive and mental disorders that impede learning and transferring content, and obtaining a score less than 103 on the Communication Skills Questionnaire. Participants who withdrawal from cooperation, unwilling to attend training sessions, and the incomplete questionnaires were excluded from the study.
The study tool consisted of a 3-part questionnaire. The first part included information on age, gender, marital status, education level, occupation for all participants, and type of diseases, number of children, and living conditions for the elderly only. The second part included a standardized interpersonal communication skills test. This questionnaire has 34 five-choice questions (never, rarely, sometimes, most often and always) to measure five skills of listening, ability to receive and send messages, vision to the communication process, excitement control, and communication with certainty in adults [20]. The reliability and validity of this questionnaire were confirmed by Hosseinchari & Fedakar [20], and Cronbach's alpha for this test has been reported 0.69. The stability of measurements, validity, and reliability of this questionnaire has also been reported as high and acceptable [20]. Because four levels of weak, average, good, excellent, were considered, the division was done as follows: scores 33-67 show weak communication skill; 68-102: moderate communication skill; 103-137: good communication skill; and 138-171: excellent. The third part included the Health-Promoting Lifestyle Questionnaire with 52 questions to measure spiritual growth behaviors, responsibility for health, interpersonal relation, stress management, physical activity, and nutrition, as modified by Walker et al. [21]. Also, Walker et al. [21] and Mohammadi Zeidi et al. [22] reported the reliability of this questionnaire as 0.94 and 0.82, respectively. Because three levels of weak, average, good were considered, the division was done as follows: scores 51-103 show weak communication skill; 104-156: moderate communication skill; and 157-209: good communication skill.
The study process started after receiving the code of medical ethics IR: TMU.REC.1396.662 and official introduction letter of Tarbiat Modares University research deputy. The questionnaires were filled out by the participants' self-report; though, due to the illiteracy of most of the participants, the researcher's cooperation was also used. After reviewing the pre-test results, educational priorities were identified based on the needs of the audience and the purpose of the study. Finally, the educational content was developed and implemented in the experimental group by reviewing relevant texts, including reference books, theses, published papers, experts' and research teams' opinions. A total of 180min of interpersonal communication skills training for the caregivers and the elderly experimental group were conducted separately during four weeks. According to the conditions of the elderly and at the request of the participants, training sessions were held in the house of one of them. But no training was provided for the control group. The caregiver and the elderly experimental group received information with identical explanations in two separate sessions to increase awareness. To develop communication skills and transform the content of theory into practical skills, eliminate wrong inferences, and answering the questions, the method of presentation, group discussion, and consultation for the experimental group were used. The outline of the first and second training sessions included familiarizing the elderly and caregivers with how to conduct research, the concept of communication, the importance and purpose of communication skills, communication obstacles, different communication personalities and styles, and effective tips on facilitating communication. The outline of the third and fourth training sessions included acquaintance of the elderly and caregivers with verbal and nonverbal communication skills, interpersonal communication skills, interpersonal communication obstacles, opposition, and non-opposition management and interpersonal communication skills, key points of how to communicate with the elderly (caregivers) effectively, the ability to manage the pressures of care and prevent the effect on interpersonal relations (caregivers) and key points on how to communicate effectively with caregivers to express their needs and problems (the elderly) held in a lecture with a presentation for the elderly and their caregivers separately. These sessions also included topics such as starting a hello greeting, making eye contact, speaking at a modest pace, simplifying and using common words, prioritizing what to discuss and emphasizing key points, repeating key points, the elderly and caregivers' participation, encourage them to ask questions. Also, during training, participants improved communication so that participants better accept recommendations and training and understand the content presented. The experimental group was also asked not to share the educational content with others until the end of the study. 2 months after the training, the questionnaires were completed again by both the experimental and control groups.
Scores of each questionnaire were recorded using SPSS 25 software. The descriptive statistics, mean±SD were used to describe the state of the subjects, and for data analysis, at a significance level 0.05, Mann-Whitney, Kolmogorov–Smirnov, Wilcoxon, and Spearman tests were used. The normal distribution of data was controlled by the Kolmogorov-Smirnov test. The Mann-Whitney test was applied to compare demographic data of the intervention and control groups before the intervention. Wilcoxon test was used to compare the pre-test and post-test scores. Spearman test was used to show the correlation between elderly and caregivers’ communication skills variables with elderly lifestyle variables.
Findings
The mean age of the caregivers of the elderly in the experimental and control groups were 55.01±6.38 and 54.44±6.22 years, respectively. Moreover, the mean age of the elderly in the experimental and control groups were 66.39±6.16 and 66.47±6.41 years (Table 1). No statistically significant difference was found between the experimental and control groups of the elderly and caregivers in terms of demographic variables for performing the intervention (p>0.05).
Table 1) Frequency distribution of individual variables in the elderly and their caregiver
The study results showed that communication skills training significantly increased the experimental group of caregivers and the elderly (Tables 2 and 3).
The mean±SD score of communication skills and lifestyle for the elderly were 90.56±4.00 and 107.34±9.14, respectively (Tables 3 and 4). The total score of lifestyle in both experimental and control groups of the elderly (Table 4) and the total score of communication skills in both experimental and control groups of the elderly (Table 3) and their caregivers (Table 2) were at the same level before the intervention. They were not significantly different (p>0.05), but two months after the training intervention, this difference was significant (p<0.001).
No significant difference was observed in the mean score of the spiritual dimension between the experimental and control groups before and after two months of the intervention (p>0.05). According to the obtained results, implementation of educational intervention did not affect the spiritual dimension of the elderly (p>0.05); but it was effective on other dimensions of their healthy lifestyle (p<0.001; Table 4).
Table 2) Comparison of the mean±SD score of the total communication skills and its dimensions between the experimental and control groups of the caregivers before and after two months of the educational intervention
Table 3) Comparison of the mean±SD score of the total communication skills and its dimensions between the experimental and control groups of the elderly before and after two months of the educational intervention
Table 4) Comparison of the mean±SD lifestyle score and its different dimensions between the experimental and control elderly groups before and after two months of the educational intervention
Discussion
The present study results showed that the mean lifestyle score of the elderly according to the Walker questionnaire before the intervention was at the mean level, which is consistent with the results of other studies [23, 24]. While in the other studies, the mean lifestyle score was at a desirable status [25, 26]. It can be predicted that the geographic location and ethnic, economic, cultural, and social differences can affect their lifestyle. Also, in the present study, the mean score of communication skills of the elderly according to the Queendam questionnaire before the intervention was at the moderate level like Siamian's study [27]. In some studies, the mean score of communication skills was weak [28, 29]. While in a study by Mojadam et al., the level of communication skills of the elderly was well reported [30]. It seems that these differences are due to the method of completing the questionnaire, questionnaire type, age of the studied population, cultural and social differences, and other demographic characteristics of the research community.
This study tries to investigate the effect of the caregiver and elderly communication skills training on the lifestyle of the elderly. Diagnosis of communication skills in the elderly is necessary because communication skills are very important in interpersonal relationships. Furthermore, the elderly's communication functions change in normal aging at different rates, and it is important to notify
the elderly's family about these changes. Accordingly, the main issues here concern communication difficulties in elderly relations and their determinants [14]. According to the results, communication skills training significantly increased the communication skills of the experimental group of caregivers and the elderly. The results of the present study are consistent with the results of the study done by Sprangers et al. [31], Heidari et al. [32], and Basiri et al. [33] but inconsistent with the results of the study done by Rask et al. [34] The cause of the existing difference can be attributed to the type of skills training and follow-up after the intervention. Therefore, communication skills training is a tool for helping the elderly and their caregivers to communicate effectively so that by changing inappropriate behaviors, they can prevent destructive interactions and help the elderly participate in social activities and avoid loneliness [35].
The effect of the training intervention on the total score of lifestyle and its dimensions in the elderly experimental group is another result of this intervention consistent with other studies [15, 24, 36]. Therefore, the elderly should be provided with the necessary knowledge to engage in healthy behaviors through basic training to enjoy a longer life without disabilities.
According to the obtained results, no significant difference was observed in the mean score of the spiritual dimension between the experimental and control groups before and after two months of the intervention. Implementation of educational intervention did not affect the spiritual dimension of the elderly, but it was effective on other dimensions of their healthy lifestyle. This could mean this educational intervention alone could not positively affect all dimensions of the lifestyle of the elderly.
The present study results are consistent with the results of the study done by Movahedi et al. [37] but inconsistent with the results of the study done by Sobhani et al. [38].
It seems that the spiritual health of the elderly depends on various factors such as religion [39], demographic, family factors, levels of worry about death, coping with problems, personal life events, having physical and mental health, levels of social activity, and purposefulness in life [40]. Regarding the difference in the level of spirituality of individuals in different settings, it is suggested that future interventions for the development of care and education programs should consider the above to improve the spiritual health of the elderly. The limitations of the present study include the low literacy of most participants and the time required to complete the two questionnaires, which resulted in wasting time so the sampling process lasted more until the sample size was sufficient enough to be able to perform the first stage of the study.
Conclusion
Communication skills training for caregivers and the elderly positively correlates with the level of the lifestyle of the elderly. This training improves the level of lifestyle and its dimensions (except spiritual growth) in the elderly group and the level of total communication skills and its dimensions in the caregiver and the elderly. Observing a healthy lifestyle, receiving health promotion training, and improving social relationships have a significant effect on improving health and increasing life expectancy in the elderly, and failure to observe the lifestyle indicators can aggravate the aging process.
Acknowledgments: The authors express their gratitude to the research deputy of Tarbiat Modares University, and they would like to express their gratitude and appreciation to elderlies and their caregivers because of their sincere cooperation.
Ethical Permissions: This article is part of the MSc thesis on health education and health promotion with the number 2017.662 in Tarbiat Modares University's ethics committee: TR.TMU.REC.2017.662.
Conflicts of Interests: The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Authors’ Contribution: Marjan Bagheri (First author), Introduction author/Methodologist/Original researcher/Statistical analyst/Discussion author (40%); Shamsaddin Niknami (Second author), Methodologist/Assistant/Discussion author (30%); Fatemeh Rahmati Najarkolaei (Third author), Methodologist/Assistant/Discussion author (30%).
Funding/Support: This article is part of MSc thesis on health education and health promotion with the number 2017.662 in Tarbiat Modarres University's ethics committee.
Article Type: Original Research |
Subject:
Healthy Life Style
Received: 2020/10/7 | Accepted: 2021/02/27 | Published: 2021/05/20
Received: 2020/10/7 | Accepted: 2021/02/27 | Published: 2021/05/20
References
1. Kushkestani M, Parvani M, Moghadassi M, Ebrahimpour Nosrani S. Investigation of life expectancy in community-dwelling elderly men in iran and its related factors. J Aging Sci. 2020;8(4):1-10. [Link] [DOI:10.17265/2332-7839/2020.02.005]
2. Knoops KTB, De Groot LCPGM, Kromhout D, Perrin AE, Moreiras-Varela O, Menotti A, et al. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA. 2004;292(12):1433-9. [Link] [DOI:10.1001/jama.292.12.1433] [PMID]
3. Li J, Yu J, Chen X, Quan X, Zhou L. Correlations between health-promoting lifestyle and health-related quality of life among elderly people with hypertension in Hengyang, Hunan, China. Medicine. 2018;97(25):10937. [Link] [DOI:10.1097/MD.0000000000010937] [PMID] [PMCID]
4. Mohammadi M, Ramezankhani A, Mohammadi S, Zahed S, Khabiri F, Khodakarim S, et al. The predictors of metabolic syndrome based on Walker health-promoting lifestyle in Iran 2016. Diabetes Metab Syndr. 2017;11 Suppl 2:745-9. [Link] [DOI:10.1016/j.dsx.2017.05.009] [PMID]
5. Kitaoka M, Mitoma J, Asakura H, Anyenda OE, Nguyen TTT, Hamagishi T, et al. The relationship between hypertension and health-related quality of life: Adjusted by chronic pain, chronic diseases, and life habits in the general middle-aged population in Japan. Environ Health Prev Med. 2016;21(4):193-214.
https://doi.org/10.1007/s12199-016-0525-3 [Link] [DOI:10.1007/s12199-016-0514-6] [PMCID]
6. Morowatisharifabad MA, Fallah Z, Bidaki R, Hashemian Z, Fallahzadeh H, Rafatifard M, et al. The prevalence of Alzheimer's disease preventive behaviors in elderly people, Yazd, Iran. Elder Health J. 2017;3(1):16-22. [Persian] [Link]
7. Meihan L, Chung-Ngok W. Validation of the psychometric properties of the health-promoting lifestyle profile in a sample of Taiwanese women. Qual Life Res. 2011;20(4):523-8. [Link] [DOI:10.1007/s11136-010-9790-6] [PMID] [PMCID]
8. Habibi Sola A, Nikpoor S, Rezaei M, Haghani H. Health promotion behaviours and level of activities of daily living and instrumental activities of daily living among elderly people in west region of Tehran: A cross sectional survey. SALMAND. 2007;2(3):331-9. [Persian] [Link]
9. Moatamedy A. A desirable lifestyle based on the communicative view (man's relationship with himself, God, others and nature). Cult Consult Psychother. 2013;4(13):125-42. [Persian] [Link]
10. Sechilariu M, Wang BC, Locment F, Jouglet A. DC microgrid power flow optimization by multi-layer supervision control, design and experimental validation. Energy Convers Manag. 2014;82:1-10. [Link] [DOI:10.1016/j.enconman.2014.03.010]
11. Yousefi F. The relationship between emotional intelligence and communication skills in university students. Dev Psychol. 2006;3(9):5-13. [Persian] [Link]
12. Freedman A, Nicolle J. Social isolation and loneliness: The new geriatric giants: Approach for primary care. Can Fam Physician. 2020;66(3):176-82. [Link]
13. Managheb SE, Jaafarian J, Firouzi H. The effect of communication skills training based on Calgary-Cambridge guideline on knowledge, attitude and practice of family physician of Jahrom university of medical sciences 2007. J Jahrom Univ Med Sci. 2008;6(3):74-84. [Persian] [Link] [DOI:10.29252/jmj.6.3.4.74]
14. Daniluk B, Borkowska AR. Pragmatic aspects of verbal communication in elderly people: A study of Polish seniors. Int J Lang Commun Disord. 2020;55(4):493-505. [Link] [DOI:10.1111/1460-6984.12532] [PMID]
15. Visser M, Wijnhoven HAH, Comijs HC, Thomese F, Twisk JWR, Deeg DJ. A healthy lifestyle in old age and prospective change in four domains of functioning. J Aging Health. 2019;31(7):1297-314. [Link] [DOI:10.1177/0898264318774430] [PMID] [PMCID]
16. Palmer AD, Newsom JT, Rook KS. How does difficulty communicating affect the social relationships of older adults? an exploration using data from a national survey. J Commun Disord. 2016;62:131-46. [Link] [DOI:10.1016/j.jcomdis.2016.06.002] [PMID] [PMCID]
17. Ruben RJ. Redefining the survival of the fittest: Communication disorders in the 21st century. Laryngoscope. 2000;110(2 Pt 1):241-5. [Link] [DOI:10.1097/00005537-200002010-00010] [PMID]
18. Yorkston KM, Bourgeois MS, Baylor CR. Communication and aging. Phys Med Rehabil Clin N Am. 2010;21(2):309-19. [Link] [DOI:10.1016/j.pmr.2009.12.011] [PMID] [PMCID]
19. Khavoshi N, Tol A, Shojaeizade D, Shamshiri A. Effect of educational intervention on the lifestyle of elderly people referred to clinical centers of Eslamshahr, Iran: Application of health belief model. J Nurs Educ. 2015;3(4):19-28. [Persian] [Link]
20. Hosseinechari M, Fadakaredavarani MM. Studying the Impact of University on Communication Skills Based on Comparison of Students and Students. Daneshvar Behav. 2005;12(15):21-32. [Persian] [Link]
21. Walker SN, Hill-Polerecky DM. Psychometric evaluation of the health-promoting lifestyle profile II. Univ Nebraska Med Center. 1996. [Link]
22. Mohammadi Zeidi I, Pakpour Hajiagha A, Mohammadi Zeidi B. Reliability and validity of Persian version of the health-promoting lifestyle profile. J Mazandaran Univ Med Sci. 2012;21(1):103-13. [Persian] [Link]
23. Ataie Z, Allahverdi A, Dehnoalian A, Orooji A. The relationship between lifestyle and general health among elderly people in Neyshabur. Iran J Nurs. 2018;31(111):10-9. [Persian] [Link] [DOI:10.29252/ijn.31.111.10]
24. Tahmasebi H, Maddah Sadat SB, Dalvandi A, Ghasemi S, Rahgozar M. The effect of educational program on health promotion behaviors on elderly life style. Iran J Rehabil Res Nurs. 2019;5(2):47-54. [Persian] [Link]
25. Brojeni SA, Ilali ES, Taraghi Z, Mousavinasab N. Lifestyle and its related factors in elderly. J Nurs Midwifery Sci. 2019;6(1):32-7. [Persian] [Link] [DOI:10.4103/JNMS.JNMS_39_18]
26. Alaee N, Jafari R, Heravi-Karmooi M, Arsang S. Investigation of Lifestyle and its related factors in the elderly population in Qom city, 2017 (Iran). Qom Univ Med Sci J. 2018;12(8):69-77. [Persian] [Link] [DOI:10.29252/qums.12.8.69]
27. Siamian H, Bagheri-Nesami M, Nia RD, Reza Nezhad F, Akbari H, Balaghafari A, et al. Assessment of interpersonal communication skills among sari health centers' staff. Mater Sociomed. 2014;26(5):324-8. [Link] [DOI:10.5455/msm.2014.26.324-328] [PMID] [PMCID]
28. Mirzaei-Alavijeh M, Motlagh MI, Hosseini SN, Jalilian F. Nursing students communication skills with patients in Kermanshah university of medical sciences. Res Med Educ. 2017;9(3):47-54. [Persian] [Link] [DOI:10.29252/rme.9.3.54]
29. Javaher AA, Khaghanizade M, Ebadi A. Study of communication skills in nursing students and its association with demographic characteristics. Iran J Med Educ. 2014;14(1):23-31. [Persian] [Link]
30. Mojadam M, Eshghizadeh M, Johari Naeimi A. Assessing interpersonal communication skills of elderly in Gonabad city. J Geriatr Nurs. 2015;2(1):29-38. [Persian] [Link]
31. Sprangers S, Dijkstra K, Romijn-Luijten A. Communication skills training in a nursing home: Effects of a brief intervention on residents and nursing aides. Clin Interv Aging. 2015;10:311-9. [Link] [DOI:10.2147/CIA.S73053] [PMID] [PMCID]
32. Heidari H, Masoudi R, Noorian K, Jamali S. The design, implementation, and evaluation of a communication skills program for the nursing students of Shahrekord university of medical sciences (Iran). J Clin Nurs Midwifery. 2020;8(4):553-9. [Persian] [Link]
33. Basiri M, Karimy M, Shahnazi H. Effect of educational intervention on communication skills and self-efficacy of primary healthcare workers (Behvarz). J Educ Community Health. 2019;6(2):71-7. [Persian] [Link] [DOI:10.29252/jech.6.2.71]
34. Rask MT, Jensen ML, Andersen J, Zachariae R. Effects of an intervention aimed at improving nurse-patient communication in an oncology outpatient clinic. Cancer Nurs. 2009;32(1):1-11. [Link] [DOI:10.1097/01.NCC.0000343365.13871.12] [PMID]
35. Rustan E, Hasriani H. Communication pattern between nurses and elderly patients through a neuro-linguistic programming approach. J Stud Komun. 2020;4(1):75-89. [Link] [DOI:10.25139/jsk.v4i1.2180]
36. Eriksen AK, Hansen RD, Borre M, Larsen RG, Jensen JM, Overgaard K, et al. A lifestyle intervention among elderly men on active surveillance for non-aggressive prostate cancer: A randomized feasibility study with whole-grain rye and exercise. Trials. 2017;18(1):20. [Link] [DOI:10.1186/s13063-016-1734-1] [PMID] [PMCID]
37. Movahedi M, Khamseh F, Ebadi A, Haji Amini Z. The impact of healthy lifestyle multimedia education on elderly life promotion. J Gerontol. 2019;4(2):45-52. [Persian] [Link] [DOI:10.29252/joge.4.1.45]
38. Sobhani A, Shahnazi H, Mostafavi F. The efficiency of theory-based education on mental health subscales in elders: Application of theory of planned behavior. Iran J Health Educ Health Promot. 2018;6(4):367-75. [Persian] [Link] [DOI:10.30699/acadpub.ijhehp.6.4.367]
39. Guerrero-Castaneda RF, De Oliva Menezes TM, Do Prado ML, Galindo-Soto JA. Spirituality and religiosity for the transcendence of the elderly being. Rev Braz Enferm. 2019;72 Suppl 2:259-65. [Link] [DOI:10.1590/0034-7167-2018-0840] [PMID]
40. Solaimanizadeh F, Mohammadinia N, Solaimanizadeh L. The relationship between spiritual health and religious coping with death anxiety in the elderly. J Relig Health. 2020;59(4):1925-32. [Link] [DOI:10.1007/s10943-019-00906-7] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |