



Volume 11, Issue 3 (2023)
Health Educ Health Promot 2023, 11(3): 477-483 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rahimi Z, Zarvekanloo S, Arab Borzu Z, Shirzadi S. Health Promoting Behaviors and Their Determinants in Iranian Postmenopausal Women; a Cross-Sectional Study. Health Educ Health Promot 2023; 11 (3) :477-483
URL: http://hehp.modares.ac.ir/article-5-70498-en.html
URL: http://hehp.modares.ac.ir/article-5-70498-en.html
1- Students Research Committee, Neyshabur University of Medical Sciences, Neyshabur, Iran
2- Department of Biostatistics and Epidemiology, School of Health, Zahedan University of Medical Sciences, Zahedan, Iran
3- Healthy Ageing Research Centre, Neyshabur University of Medical Sciences, Neyshabur, Iran
2- Department of Biostatistics and Epidemiology, School of Health, Zahedan University of Medical Sciences, Zahedan, Iran
3- Healthy Ageing Research Centre, Neyshabur University of Medical Sciences, Neyshabur, Iran
Full-Text [PDF 770 kb]
(408 Downloads)
| Abstract (HTML) (304 Views)
Full-Text: (24 Views)
Introduction
In today's world, as a modern life period, having a healthy lifestyle is one of the basic needs in human societies, and the way to achieve it is through health-promoting behaviors (HPBs) [1].
HPBs encompass all dimensions of health, including healthy eating, regular exercise, avoiding harmful behaviors and substance abuse, protection against events and incidents, early diagnosis of diseases, emotional and mental control, coping with stress and psychological problems, compatibility and modification of interpersonal relationships. According to Pender's theory, health-promoting behaviors include any measures to increase or maintain an individual's or group's health and self-actualization. These behaviors include six dimensions of spiritual growth (SG), health responsibility (HR), physical activity (PA), nutrition (Nut), interpersonal relationships (IR), and stress management (SM) [2].
One of the health promotion goals is to empower individuals and groups so that they can have control over the determinants of their quality of life and choose healthy lifestyles. Given the selectivity of behavior in lifestyle, it is essential to consider the empowerment of individuals [3]. This necessity is particularly important in relation to gender-related issues and diseases [4]. Women of all age groups make up a significant portion of the population, and due to natural changes in their physiological state, they face certain issues and crises. Menopause is one of the most important reproductive health issues of women. Because of rising life expectancy, women may expect to spend more than a third of their lives after menopause. Aging and changes caused by menopause, such as hormonal changes, can increase the risk of developing chronic diseases [4, 5]. The disorders of metabolic syndromes, encompassing cardiovascular diseases and type 2 diabetes, may arise from a myriad of lipid metabolic disorders brought about by hormonal fluctuations, namely, diminished levels of estrogens and augmented levels of circulating androgens [6]. Cardiovascular disease is the leading cause of death in women, who have a significant increase in the risk for this disease after menopause [7]. Most menopausal women experience menopausal vasomotor symptoms, often described as hot flushes or night sweats, chills, sleep disruption, and palpitations. They also experience psychological symptoms such as mood changes, anxiety, and depression [8]. Other conditions occur after menopause, including decreased bone density, energy changes, decreased sexual function, vaginal dryness/dyspareunia, obesity, and more. All of these conditions can affect the quality of life of postmenopausal women. Therefore, it is necessary to use strategies and planning to improve the quality of life during menopause [4, 5].
A healthy lifestyle is an important factor in postmenopausal women's health, and various studies have shown a relationship between HPBs and menopausal symptoms and women's health [9-11]. Studies have shown the effect of lifestyle modification programs in reducing menopausal symptoms [12-14]. A study conducted among Finnish middle-aged women, athletes, and nonalcoholic women experienced fewer menopause symptoms than nonathletic and alcoholic postmenopausal women [15].
Since women have basic roles in family and society, coping with these roles and duties requires physical and mental health. Therefore, it is necessary and beneficial that postmenopausal women be familiar with HPBs and be informed of their roles in health promotion and controlling of menopause symptoms. An unhealthy lifestyle in the long term will be a serious threat to postmenopausal women, and they will face health problems in old age. Therefore, because of its importance, this study was conducted to determine HPBs and their individual-social factors in postmenopausal women living in Neyshabur City, Iran.
Instrument and Methods
This cross-sectional study was conducted among Iranian postmenopausal women sampled from Neyshabur County, Razavi Khorasan Province, Iran, in 2022. The general population, which was covered by the regional healthcare centers in urban areas, was the sampling frame. To determine the sample size, the primary information was obtained from a previous study [16]. We estimated sample size using the formula, where α=0.05, B=90%, R=-0.404. Considering about 20% attrition, the sample size was increased to 300.
According to this, 300 women from 45 to 60 years old experience menopause after 45 years of age, not having abnormal menopause (hysterectomy surgery, chemotherapy and …), no hormone therapy in the last 6 months, at least 12 months have passed since the last menstrual period were selected for the study. Individuals with a physical or mental disability, experienced unfortunate events and incidents in the last 6 months, and using tobacco and alcoholic beverages were not selected. Regarding the sample size, the stratified sampling method was used to select the participants. To this end, the researcher first identified the total number of women covered in healthcare centers. Then the healthcare centers with more women had a larger sample size proportionate to its size.
A self-administered questionnaire was used for data collection. It consists of two sections:
Socio-demographic Variables: This includes age, employment status, educational status, marital status, number of children, menopausal age, family structure, economic status, spouse's educational status, and having a chronic disease.
Health-Promoting Lifestyle Profile-ll (HPLP-ll): This scale was designed by Walker et al. in 1987 to measure health-promoting behaviors [2]. the Persian version of HPLP-II, validated by Mohammadi Zeidi et al., was used [17]. Fifty-two health-promoting lifestyle behaviors are measured on a four-point Likert scale (1=never, 2=frequently, 3=almost, and 4=always). The HPLP-II includes six subscales: health responsibility (9 items), physical activity (8 items), nutrition (9 items), spiritual growth (9 items), interpersonal relationships (9 items), and stress management (8 items). The overall score of the instrument ranges from 52 to 208, where each domain has its separate score, and higher scores indicate a better adherence to health-promoting behavior. In this way, scores 52-145 mean a low level of adherence to these behaviors, and scores 146-160 and above 160 imply a moderate and high level, respectively.
Informed consent was obtained verbally from all study participants before completing the survey instrument. A survey questionnaire was used for data collection. Trained interviewers collected the data from the respondents, and those women who were illiterate were assisted in completing the questionnaire. Additionally, participants were free to withdraw or remain in the study during data collection.
We performed all the analyses using SPSS 22 software. The statistical description of the sociodemographic variables was performed by applying frequencies, means, and standard deviations (SDs). We used a T-test and one-way analysis of variance to analyze the differences between HPBs by sociodemographic characteristics. To determine the effect size, the effect size values greater than 0.45 have high effect size, values between 0.25-0.1 are medium effect size, and values less than 0.1 are weak effect size. Multivariate linear regression was used to determine the independent predictor variables of HPB. The level of significance was set to be <0.05.
Findings
The mean age and menopausal age were 56.4±4.1 and 49.4±3.3 years, respectively. The majority of the menopausal women were married (75%) and housewives (88%), had three or more children (80%) and suffered from at least one chronic disease (65.7%). Also, the economic status of 67.3% of individuals was moderate.
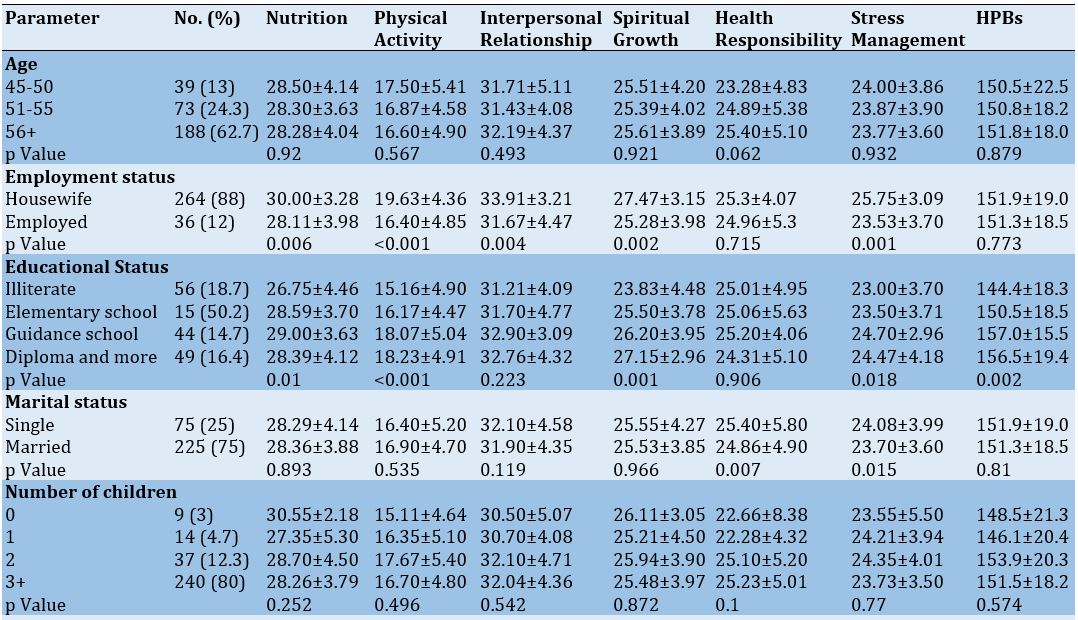
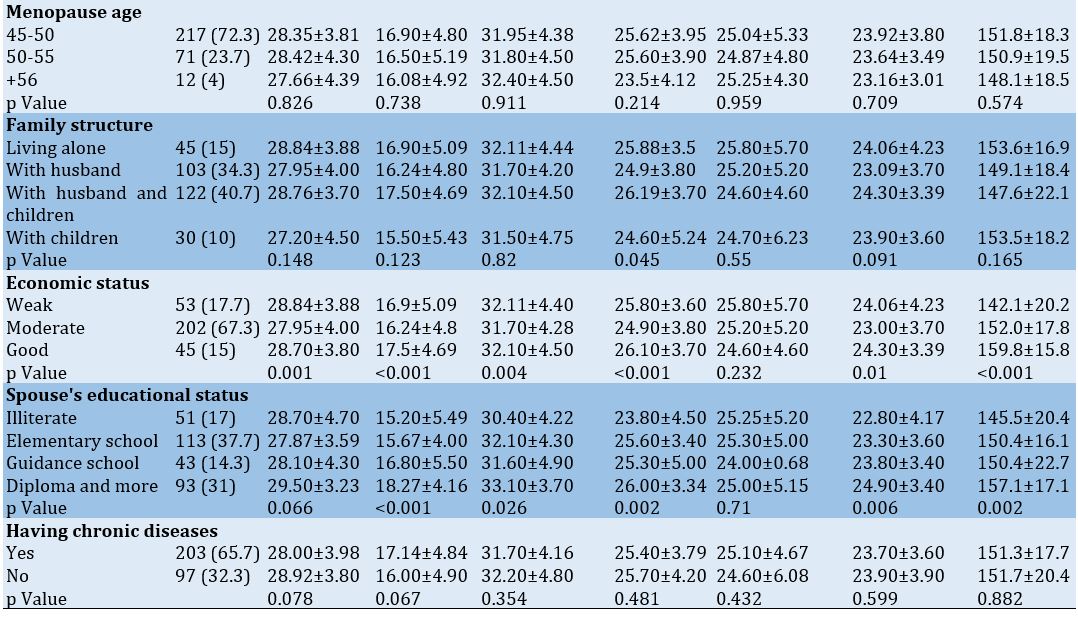
The mean of HPBs in postmenopausal women was 151.5±18.6, and the highest score of HPB was related to interpersonal relationships (31.9±4.4), and the lowest score was related to physical activity (16.8±4.9). There were significant statistical relationships (p<0.05) between educational level, economic status, spouse's education level, and HPBs (Table 1).
Table 1. Relationships between demographic characteristics with HPBs and their diminution score in postmenopausal women
The multivariate linear regression test results showed that employment and economic status were significantly independent predictors for HPBs (≤0.001; Table 2).
Table 2. The relationship between demographic characteristics and HPBs in postmenopausal women based on a multivariate linear regression test (Adjusted R2=0.095)

Discussion
This study aimed to explore HPBs and their related factors among postmenopausal women in Neyshabur City, Iran. Our results provide an insight into the lifestyle of Iranian postmenopausal women.
The overall mean score for HPBs among postmenopausal women was moderate, consistent with the findings of other studies [10, 16, 18, 19]. This finding highlights the importance of health promotion planning, emphasizing empowerment to develop a healthy lifestyle among postmenopausal women. Previous studies also demonstrate the positive impact of HPBs on menopausal symptoms. So, after implementing the educational intervention, menopausal symptoms have decreased in postmenopausal women [14, 20, 21].
Regarding HPBs subscales, postmenopausal women obtained the highest mean score in interpersonal relations, consistent with some studies conducted among menopausal women [22, 23]. However, other studies have shown results that differ from ours [10, 11, 16, 24, 25]. lose interpersonal relationships play a significant role in health behaviors and adapting to the changes in psychosomatic functioning during menopause. Rejection, loneliness, and lack of intimacy in relationships can deepen and prolong menopausal symptoms, while feeling loved, important, understood, and cared for can contribute to well-being and more effective coping [26]. Interpersonal connections and social capital have been found to positively correlate with increased physical activity and decreased depressive symptoms [27, 28].
In our study, the majority of participants had high interpersonal relations. Therefore, it can be said that they have the capacity to seek support and participate in support activities. This potential can be utilized to promote healthy behaviors such as physical activity, stress management, and health responsibility, provided healthcare providers design and implement health promotion programs targeting postmenopausal women.
In this study, postmenopausal women obtained the lowest mean score in physical activity, which is similar to other previous studies conducted in Iranian [10, 14, 23, 29], Korean [24, 25], Turkish [22], and Egyptian postmenopausal women [16]. However, numerous studies have shown that physical activity improves the symptoms of menopause and increases the quality of life. So, Women with high and moderate physical activity levels had less severe menopausal symptoms than inactive women [30, 31]. Our findings are alarming and show that postmenopausal women have a sedentary lifestyle. Some reasons may be noted for such a low level of physical activity, including lack of exercise facilities in the community, lack of social support and a PA partner, lack of time and knowledge, insufficient safe outdoor playgrounds, low self-efficacy on exercise, and lack of walking tracks in most of the cities, particularly, for females—another reason for the low level of physical.
Thus, community and cultural-based health promotion planning is necessary to motivate postmenopausal women to engage in regular physical activity to promote health and prevent diseases.
In this study, 65.7% of women had chronic diseases, but there was no significant correlation between HPBs and a history of chronic disease. This suggests that postmenopausal women in this study are not sensitive to their health, even with a chronic disease. Menopause is a critical period for women's health, as it marks the onset of several chronic diseases that can significantly impact their quality and quantity of life [4, 32]. Therefore, prevention strategies at menopause should include screening and assessment for risk factors, lifestyle management, a healthy diet, moderate exercise, and mentally stimulating activities.
According to our study, stress management was the second-lowest mean score of the HPB dimensions. Postmenopausal women in this study did not use stress management techniques or find enough time to relax. Stress management can offer an alternative approach to managing menopausal symptoms. Studies have shown that the stress reduction program and structured education program incorporating deep breathing, progressive muscle relaxation, and guided visualization could effectively manage menopausal symptoms [33, 34]. Therefore, educating and providing opportunities to apply stress management techniques, such as getting enough sleep, relaxing, and focusing on pleasant thoughts, may be helpful for postmenopausal women.
In this study, economic status was one of the effective factors in health-promoting behaviors; women with favorable economic status had higher mean scores in whole HPBs, NUT, PA, IR, SG, and SM. The empirical evidence has amply demonstrated the inverse associations between socioeconomic status and unhealthy lifestyle practices [16, 35, 36]. Class distinction and social motives may influence the adoption of certain health behaviors. Comparisons of the determinants of behaviors may offer new insights into pursuing a healthy lifestyle. There is a need for multilevel interventions to enhance the health of all individuals, particularly disadvantaged groups, to reduce and eliminate health inequities [35].
According to this study, housewives had significantly higher mean scores in NUT, PA, SG, IR, and SM, which is different from the results of studies conducted by Enjezab [29], Abo-Ali [16], and Sehhatie [10]. The household responsibilities and workplace environment strongly correlate to women's work-life conflict [37]. Therefore, employed women should be aware of the potential health risks of unhealthy lifestyles and take steps to manage their work-life balance effectively. Policymakers can use these findings to inform regulations and policies related to maintaining and improving the health of employed women, ensuring that they prioritize employee health and safety. In addition, it is essential to provide programs that target employed women, such as periodic assessments of mental and physical health, providing PA services and facilities in the workplace, and allocating leave for medical checkups.
Also, it was found that there is a significant relationship between educational levels and whole HPBs, Nut, PA, SG, and SM dimensions; in other words, menopausal women with a low education level had a lower mean score of the mentioned variables, which was in accordance with other studies [16, 38]. Our finding can be considered as an additional document that training and awareness of menopausal women regarding HPBs should be considered a universal issue, and education and counseling regarding HPBs are recommended for them by HCPs.
In the present study, the married women scored significantly higher on NUT, while the single/divorced/widowed women scored significantly higher on HR and SM. In a study by Abo Ali, married PMW had a better HPB score compared to divorced and widowed [16]. However, in studies by Sehhatie [10], Enjezab [29], and Kim JH [25], there was no significant relationship between marital status and HPBs.
This could be explained by the fact that married women have various routine responsibilities, such as taking care of children, cleaning the house, cooking, etc., which makes women prioritize everything else first, often at the expense of their self-care. Additionally, as married women have different responsibilities and are the foundation of family care, they must be familiar with stress management techniques.
Based on the results, a higher level of education of women's husbands was accompanied by higher mean scores in whole HPBs, PA, SG, IR, and SM dimensions. In a study by Shabani Asrami et al., the results showed a positive significant relationship between women's health-promoting lifestyle behaviors and their spouse's level of education [11]. The findings regarding these relationships may be considered a noteworthy issue in this study. Especially in low- and middle-income settings, men could be decision-makers in issues related to women's health [39, 40], and their role must be kept in mind in policies related to the health promotion of their wives. Less educated men appear to require more careful training and planning.
Additionally, it was found that women who lived with their children and husbands had a significantly higher score of SG. Although our finding does not follow studies conducted among PMWs [11, 16], Family spirituality can strengthen family health by fostering family commitment, improving emotional well-being, developing new healthy behaviors, and providing healing experiences [41]. It can be considered as additional evidence that a cohesive family can promote spirituality among family members and improve women's health.
The current study faced several limitations. Firstly, the cross-sectional design of this study does not establish causation and changes over time in HPBs among postmenopausal women. Therefore, the generalization of the findings should be done with caution. Future studies can be conducted to discover and confirm the association between HPBs and different factors. Secondly, as all information collected in this study was based on self-reporting, it is possible that the answers have a socially desirable response bias. Thirdly, this study was conducted on women admitted to healthcare centers, and its results are, therefore, only applicable to this group of women. Future studies should be conducted through population-based design research to visit postmenopausal women in their residences.
Conclusion
Postmenopausal women's HPB status in Neyshabur City is moderate. It is necessary to promote HPBs, with a particular focus on physical activity.
Acknowledgments: The authors would like to thank the officials of Neyshabur Healthcare Centers for their cooperation, the postmenopausal women, and the Neyshabur Students Research Committee.
Ethical Permission: This study was approved by the Neyshabur University of Medical Sciences (with the ethics code of IR.NUMS.REC.1401.005).
Conflict of Interests: The authors declare no conflict of interest.
Authors’ Contribution: Rahimi Z (First Author), Introduction Writer/Main Researcher/Discussion Writer (30%); Zarvekanloo S (Second Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%); Arab Borzu Z (Third Author), Assistant Researcher/Statistical Analyst (10%); Shirzadi S (Fourth Author), Introduction Writer/Methodologist/Main Researcher/Statistical Analyst (40%)
Funding/Support: This study was supported by the Neyshabur University of Medical Sciences (Students Research Committee; grant number: 140).
In today's world, as a modern life period, having a healthy lifestyle is one of the basic needs in human societies, and the way to achieve it is through health-promoting behaviors (HPBs) [1].
HPBs encompass all dimensions of health, including healthy eating, regular exercise, avoiding harmful behaviors and substance abuse, protection against events and incidents, early diagnosis of diseases, emotional and mental control, coping with stress and psychological problems, compatibility and modification of interpersonal relationships. According to Pender's theory, health-promoting behaviors include any measures to increase or maintain an individual's or group's health and self-actualization. These behaviors include six dimensions of spiritual growth (SG), health responsibility (HR), physical activity (PA), nutrition (Nut), interpersonal relationships (IR), and stress management (SM) [2].
One of the health promotion goals is to empower individuals and groups so that they can have control over the determinants of their quality of life and choose healthy lifestyles. Given the selectivity of behavior in lifestyle, it is essential to consider the empowerment of individuals [3]. This necessity is particularly important in relation to gender-related issues and diseases [4]. Women of all age groups make up a significant portion of the population, and due to natural changes in their physiological state, they face certain issues and crises. Menopause is one of the most important reproductive health issues of women. Because of rising life expectancy, women may expect to spend more than a third of their lives after menopause. Aging and changes caused by menopause, such as hormonal changes, can increase the risk of developing chronic diseases [4, 5]. The disorders of metabolic syndromes, encompassing cardiovascular diseases and type 2 diabetes, may arise from a myriad of lipid metabolic disorders brought about by hormonal fluctuations, namely, diminished levels of estrogens and augmented levels of circulating androgens [6]. Cardiovascular disease is the leading cause of death in women, who have a significant increase in the risk for this disease after menopause [7]. Most menopausal women experience menopausal vasomotor symptoms, often described as hot flushes or night sweats, chills, sleep disruption, and palpitations. They also experience psychological symptoms such as mood changes, anxiety, and depression [8]. Other conditions occur after menopause, including decreased bone density, energy changes, decreased sexual function, vaginal dryness/dyspareunia, obesity, and more. All of these conditions can affect the quality of life of postmenopausal women. Therefore, it is necessary to use strategies and planning to improve the quality of life during menopause [4, 5].
A healthy lifestyle is an important factor in postmenopausal women's health, and various studies have shown a relationship between HPBs and menopausal symptoms and women's health [9-11]. Studies have shown the effect of lifestyle modification programs in reducing menopausal symptoms [12-14]. A study conducted among Finnish middle-aged women, athletes, and nonalcoholic women experienced fewer menopause symptoms than nonathletic and alcoholic postmenopausal women [15].
Since women have basic roles in family and society, coping with these roles and duties requires physical and mental health. Therefore, it is necessary and beneficial that postmenopausal women be familiar with HPBs and be informed of their roles in health promotion and controlling of menopause symptoms. An unhealthy lifestyle in the long term will be a serious threat to postmenopausal women, and they will face health problems in old age. Therefore, because of its importance, this study was conducted to determine HPBs and their individual-social factors in postmenopausal women living in Neyshabur City, Iran.
Instrument and Methods
This cross-sectional study was conducted among Iranian postmenopausal women sampled from Neyshabur County, Razavi Khorasan Province, Iran, in 2022. The general population, which was covered by the regional healthcare centers in urban areas, was the sampling frame. To determine the sample size, the primary information was obtained from a previous study [16]. We estimated sample size using the formula, where α=0.05, B=90%, R=-0.404. Considering about 20% attrition, the sample size was increased to 300.
According to this, 300 women from 45 to 60 years old experience menopause after 45 years of age, not having abnormal menopause (hysterectomy surgery, chemotherapy and …), no hormone therapy in the last 6 months, at least 12 months have passed since the last menstrual period were selected for the study. Individuals with a physical or mental disability, experienced unfortunate events and incidents in the last 6 months, and using tobacco and alcoholic beverages were not selected. Regarding the sample size, the stratified sampling method was used to select the participants. To this end, the researcher first identified the total number of women covered in healthcare centers. Then the healthcare centers with more women had a larger sample size proportionate to its size.
A self-administered questionnaire was used for data collection. It consists of two sections:
Socio-demographic Variables: This includes age, employment status, educational status, marital status, number of children, menopausal age, family structure, economic status, spouse's educational status, and having a chronic disease.
Health-Promoting Lifestyle Profile-ll (HPLP-ll): This scale was designed by Walker et al. in 1987 to measure health-promoting behaviors [2]. the Persian version of HPLP-II, validated by Mohammadi Zeidi et al., was used [17]. Fifty-two health-promoting lifestyle behaviors are measured on a four-point Likert scale (1=never, 2=frequently, 3=almost, and 4=always). The HPLP-II includes six subscales: health responsibility (9 items), physical activity (8 items), nutrition (9 items), spiritual growth (9 items), interpersonal relationships (9 items), and stress management (8 items). The overall score of the instrument ranges from 52 to 208, where each domain has its separate score, and higher scores indicate a better adherence to health-promoting behavior. In this way, scores 52-145 mean a low level of adherence to these behaviors, and scores 146-160 and above 160 imply a moderate and high level, respectively.
Informed consent was obtained verbally from all study participants before completing the survey instrument. A survey questionnaire was used for data collection. Trained interviewers collected the data from the respondents, and those women who were illiterate were assisted in completing the questionnaire. Additionally, participants were free to withdraw or remain in the study during data collection.
We performed all the analyses using SPSS 22 software. The statistical description of the sociodemographic variables was performed by applying frequencies, means, and standard deviations (SDs). We used a T-test and one-way analysis of variance to analyze the differences between HPBs by sociodemographic characteristics. To determine the effect size, the effect size values greater than 0.45 have high effect size, values between 0.25-0.1 are medium effect size, and values less than 0.1 are weak effect size. Multivariate linear regression was used to determine the independent predictor variables of HPB. The level of significance was set to be <0.05.
Findings
The mean age and menopausal age were 56.4±4.1 and 49.4±3.3 years, respectively. The majority of the menopausal women were married (75%) and housewives (88%), had three or more children (80%) and suffered from at least one chronic disease (65.7%). Also, the economic status of 67.3% of individuals was moderate.
The mean of HPBs in postmenopausal women was 151.5±18.6, and the highest score of HPB was related to interpersonal relationships (31.9±4.4), and the lowest score was related to physical activity (16.8±4.9). There were significant statistical relationships (p<0.05) between educational level, economic status, spouse's education level, and HPBs (Table 1).
Table 1. Relationships between demographic characteristics with HPBs and their diminution score in postmenopausal women
The multivariate linear regression test results showed that employment and economic status were significantly independent predictors for HPBs (≤0.001; Table 2).
Table 2. The relationship between demographic characteristics and HPBs in postmenopausal women based on a multivariate linear regression test (Adjusted R2=0.095)
Discussion
This study aimed to explore HPBs and their related factors among postmenopausal women in Neyshabur City, Iran. Our results provide an insight into the lifestyle of Iranian postmenopausal women.
The overall mean score for HPBs among postmenopausal women was moderate, consistent with the findings of other studies [10, 16, 18, 19]. This finding highlights the importance of health promotion planning, emphasizing empowerment to develop a healthy lifestyle among postmenopausal women. Previous studies also demonstrate the positive impact of HPBs on menopausal symptoms. So, after implementing the educational intervention, menopausal symptoms have decreased in postmenopausal women [14, 20, 21].
Regarding HPBs subscales, postmenopausal women obtained the highest mean score in interpersonal relations, consistent with some studies conducted among menopausal women [22, 23]. However, other studies have shown results that differ from ours [10, 11, 16, 24, 25]. lose interpersonal relationships play a significant role in health behaviors and adapting to the changes in psychosomatic functioning during menopause. Rejection, loneliness, and lack of intimacy in relationships can deepen and prolong menopausal symptoms, while feeling loved, important, understood, and cared for can contribute to well-being and more effective coping [26]. Interpersonal connections and social capital have been found to positively correlate with increased physical activity and decreased depressive symptoms [27, 28].
In our study, the majority of participants had high interpersonal relations. Therefore, it can be said that they have the capacity to seek support and participate in support activities. This potential can be utilized to promote healthy behaviors such as physical activity, stress management, and health responsibility, provided healthcare providers design and implement health promotion programs targeting postmenopausal women.
In this study, postmenopausal women obtained the lowest mean score in physical activity, which is similar to other previous studies conducted in Iranian [10, 14, 23, 29], Korean [24, 25], Turkish [22], and Egyptian postmenopausal women [16]. However, numerous studies have shown that physical activity improves the symptoms of menopause and increases the quality of life. So, Women with high and moderate physical activity levels had less severe menopausal symptoms than inactive women [30, 31]. Our findings are alarming and show that postmenopausal women have a sedentary lifestyle. Some reasons may be noted for such a low level of physical activity, including lack of exercise facilities in the community, lack of social support and a PA partner, lack of time and knowledge, insufficient safe outdoor playgrounds, low self-efficacy on exercise, and lack of walking tracks in most of the cities, particularly, for females—another reason for the low level of physical.
Thus, community and cultural-based health promotion planning is necessary to motivate postmenopausal women to engage in regular physical activity to promote health and prevent diseases.
In this study, 65.7% of women had chronic diseases, but there was no significant correlation between HPBs and a history of chronic disease. This suggests that postmenopausal women in this study are not sensitive to their health, even with a chronic disease. Menopause is a critical period for women's health, as it marks the onset of several chronic diseases that can significantly impact their quality and quantity of life [4, 32]. Therefore, prevention strategies at menopause should include screening and assessment for risk factors, lifestyle management, a healthy diet, moderate exercise, and mentally stimulating activities.
According to our study, stress management was the second-lowest mean score of the HPB dimensions. Postmenopausal women in this study did not use stress management techniques or find enough time to relax. Stress management can offer an alternative approach to managing menopausal symptoms. Studies have shown that the stress reduction program and structured education program incorporating deep breathing, progressive muscle relaxation, and guided visualization could effectively manage menopausal symptoms [33, 34]. Therefore, educating and providing opportunities to apply stress management techniques, such as getting enough sleep, relaxing, and focusing on pleasant thoughts, may be helpful for postmenopausal women.
In this study, economic status was one of the effective factors in health-promoting behaviors; women with favorable economic status had higher mean scores in whole HPBs, NUT, PA, IR, SG, and SM. The empirical evidence has amply demonstrated the inverse associations between socioeconomic status and unhealthy lifestyle practices [16, 35, 36]. Class distinction and social motives may influence the adoption of certain health behaviors. Comparisons of the determinants of behaviors may offer new insights into pursuing a healthy lifestyle. There is a need for multilevel interventions to enhance the health of all individuals, particularly disadvantaged groups, to reduce and eliminate health inequities [35].
According to this study, housewives had significantly higher mean scores in NUT, PA, SG, IR, and SM, which is different from the results of studies conducted by Enjezab [29], Abo-Ali [16], and Sehhatie [10]. The household responsibilities and workplace environment strongly correlate to women's work-life conflict [37]. Therefore, employed women should be aware of the potential health risks of unhealthy lifestyles and take steps to manage their work-life balance effectively. Policymakers can use these findings to inform regulations and policies related to maintaining and improving the health of employed women, ensuring that they prioritize employee health and safety. In addition, it is essential to provide programs that target employed women, such as periodic assessments of mental and physical health, providing PA services and facilities in the workplace, and allocating leave for medical checkups.
Also, it was found that there is a significant relationship between educational levels and whole HPBs, Nut, PA, SG, and SM dimensions; in other words, menopausal women with a low education level had a lower mean score of the mentioned variables, which was in accordance with other studies [16, 38]. Our finding can be considered as an additional document that training and awareness of menopausal women regarding HPBs should be considered a universal issue, and education and counseling regarding HPBs are recommended for them by HCPs.
In the present study, the married women scored significantly higher on NUT, while the single/divorced/widowed women scored significantly higher on HR and SM. In a study by Abo Ali, married PMW had a better HPB score compared to divorced and widowed [16]. However, in studies by Sehhatie [10], Enjezab [29], and Kim JH [25], there was no significant relationship between marital status and HPBs.
This could be explained by the fact that married women have various routine responsibilities, such as taking care of children, cleaning the house, cooking, etc., which makes women prioritize everything else first, often at the expense of their self-care. Additionally, as married women have different responsibilities and are the foundation of family care, they must be familiar with stress management techniques.
Based on the results, a higher level of education of women's husbands was accompanied by higher mean scores in whole HPBs, PA, SG, IR, and SM dimensions. In a study by Shabani Asrami et al., the results showed a positive significant relationship between women's health-promoting lifestyle behaviors and their spouse's level of education [11]. The findings regarding these relationships may be considered a noteworthy issue in this study. Especially in low- and middle-income settings, men could be decision-makers in issues related to women's health [39, 40], and their role must be kept in mind in policies related to the health promotion of their wives. Less educated men appear to require more careful training and planning.
Additionally, it was found that women who lived with their children and husbands had a significantly higher score of SG. Although our finding does not follow studies conducted among PMWs [11, 16], Family spirituality can strengthen family health by fostering family commitment, improving emotional well-being, developing new healthy behaviors, and providing healing experiences [41]. It can be considered as additional evidence that a cohesive family can promote spirituality among family members and improve women's health.
The current study faced several limitations. Firstly, the cross-sectional design of this study does not establish causation and changes over time in HPBs among postmenopausal women. Therefore, the generalization of the findings should be done with caution. Future studies can be conducted to discover and confirm the association between HPBs and different factors. Secondly, as all information collected in this study was based on self-reporting, it is possible that the answers have a socially desirable response bias. Thirdly, this study was conducted on women admitted to healthcare centers, and its results are, therefore, only applicable to this group of women. Future studies should be conducted through population-based design research to visit postmenopausal women in their residences.
Conclusion
Postmenopausal women's HPB status in Neyshabur City is moderate. It is necessary to promote HPBs, with a particular focus on physical activity.
Acknowledgments: The authors would like to thank the officials of Neyshabur Healthcare Centers for their cooperation, the postmenopausal women, and the Neyshabur Students Research Committee.
Ethical Permission: This study was approved by the Neyshabur University of Medical Sciences (with the ethics code of IR.NUMS.REC.1401.005).
Conflict of Interests: The authors declare no conflict of interest.
Authors’ Contribution: Rahimi Z (First Author), Introduction Writer/Main Researcher/Discussion Writer (30%); Zarvekanloo S (Second Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%); Arab Borzu Z (Third Author), Assistant Researcher/Statistical Analyst (10%); Shirzadi S (Fourth Author), Introduction Writer/Methodologist/Main Researcher/Statistical Analyst (40%)
Funding/Support: This study was supported by the Neyshabur University of Medical Sciences (Students Research Committee; grant number: 140).
Article Type: Descriptive & Survey |
Subject:
Healthy Life Style
Received: 2023/07/13 | Accepted: 2023/09/2 | Published: 2023/10/1
Received: 2023/07/13 | Accepted: 2023/09/2 | Published: 2023/10/1
References
1. Fortunka KB. Factors affecting human health in the modern world. J Educ Health and Sport. 2020;10(4):75-81. [Link] [DOI:10.12775/JEHS.2020.10.04.009]
2. Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: development and psychometric characteristics. Nurs Res. 1987;36(2):76-81. [Link] [DOI:10.1097/00006199-198703000-00002]
3. Tengland PA. Behavior change or empowerment: On the ethics of health-promotion goals. Health Care Anal. 2016;24(1):24-46. [Link] [DOI:10.1007/s10728-013-0265-0]
4. Lobo RA, Davis SR, De Villiers T, Gompel A, Henderson VW, Hodis HN, et al. Prevention of diseases after menopause. Climacteric. 2014;17(5):540-56. [Link] [DOI:10.3109/13697137.2014.933411]
5. Al-Azzawi F, Palacios S. Hormonal changes during menopause. Maturitas. 2009;63(2):135-7. [Link] [DOI:10.1016/j.maturitas.2009.03.009]
6. Ko SH, Kim HS. Menopause-associated lipid metabolic disorders and foods beneficial for postmenopausal women. Nutrients. 2020;12(1):202. [Link] [DOI:10.3390/nu12010202]
7. El Khoudary SR, Aggarwal B, Beckie TM, Hodis HN, Johnson AE, Langer RD, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: A scientific statement from the American Heart Association. Circulation. 2020;142(25):e506-32. [Link] [DOI:10.1161/CIR.0000000000000912]
8. Cramer H, Peng W, Lauche R. Yoga for menopausal symptoms-A systematic review and meta-analysis. Maturitas. 2018;109:13-25. [Link] [DOI:10.1016/j.maturitas.2017.12.005]
9. Alaeenejad A, Farahaninia M, Janmohammadi S, Haghani H. Relationship between health-promoting behaviors and quality of life in postmenopausal women. J Client Centered Nurs Care. 2017;3(4):269-76. [Link] [DOI:10.32598/jccnc.3.4.269]
10. Sehhatie F, Mirghafourvand M, Momeni K. Health promoting behaviors among postmenopausal women in langroud city, Iran. Tabriz Univ Med Sci Knowl Repository. 2015;3(3):158-62. [Link] [DOI:10.15296/ijwhr.2015.33]
11. Asrami FS, Hamzehgardeshi Z, Shahhosseini Z. Health promoting lifestyle behaviors in menopausal women: A cross-sectional study. Glob J Health Sci. 2016;8(8):128-34. [Link] [DOI:10.5539/gjhs.v8n8p128]
12. Rathnayake N, Alwis G, Lenora J, Lekamwasam S. Impact of health-promoting lifestyle education intervention on health-promoting behaviors and health status of postmenopausal women: A quasi-experimental study from Sri-Lanka. BioMed Res Int. 2019;2019:4060426. [Link] [DOI:10.1155/2019/4060426]
13. Malik E, Sheoran P, Siddiqui A. Health-promoting behaviors and menopausal symptoms: an interventional study in rural India. J Midlife Health. 2018;9(4):200-6. [Link] [DOI:10.4103/jmh.JMH_96_18]
14. Nazari M, Farmani S, Kaveh MH, Ghaem H. The effectiveness of lifestyle educational program in health promoting behaviors and menopausal symptoms in 45-60-year-old women in Marvdasht, Iran. Glob J Health Sci. 2016;8(10):55414. [Link] [DOI:10.5539/gjhs.v8n10p34]
15. Moilanen J, Aalto AM, Hemminki E, Aro AR, Raitanen J, Luoto R. Prevalence of menopause symptoms and their association with lifestyle among Finnish middle-aged women. Maturitas. 2010;67(4):368-74. [Link] [DOI:10.1016/j.maturitas.2010.08.007]
16. Abo Ali EA, Oka AA. Menopausal symptoms and health-promoting lifestyle behaviors among women in Tanta, Egypt: An analytic cross-sectional study. Egypt Family Med J. 2021;5(1):125-40. [Link] [DOI:10.21608/efmj.2021.34033.1037]
17. Mohammadi Zeidi I, Pakpour Hajiagha A, Mohammadi Zeidi B. Reliability and validity of Persian version of the health-promoting lifestyle profile. J Mazandaran Univ Med Sci. 2011;20(1):102-13. [Persian] [Link]
18. Moudi A, Dashtgard A, Salehiniya H, Katebi MS, Razmara MR, Jani MR. The relationship between health-promoting lifestyle and sleep quality in postmenopausal women. Biomedicine. 2018;8(2):11. [Link] [DOI:10.1051/bmdcn/2018080211]
19. Park S. Mediating effect of a health-promoting lifestyle in the relationship between menopausal symptoms, resilience, and depression in middle-aged women. Health Care Women Int. 2020;41(9):967-83. [Link] [DOI:10.1080/07399332.2019.1685524]
20. Anderson D, Seib C, McGuire A, Porter-Steele J. Decreasing menopausal symptoms in women undertaking a web-based multi-modal lifestyle intervention: The women's wellness program. Maturitas. 2015;81(1):69-75. [Link] [DOI:10.1016/j.maturitas.2015.02.263]
21. Shafaie FS, Mirghafourvand M, Jafari M. Effect of education through support group on early symptoms of menopause: A randomized controlled trial. J Caring Sci. 2014;3(4):247-56. [Link]
22. Ozcan H. Healthy life style behaviors and quality of life at menopause. Int J Caring Sci. 2019;12(1):492-500. [Link]
23. Azhari S, Ghorbani M, Esmaeili H. Evaluation of the relationship between lifestyle and quality of sleep in postmenopausal women. Iran J Obstet Gynecol Infertil. 2014;17(112):7-14. [Persian] [Link]
24. Hong E, Kang YS, Ha Y. Factors affecting on health promoting behaviors among teachers with middle-aged women experiencing menopause. Korean J Occupational Health Nurs. 2013:66-74. [Link] [DOI:10.5807/kjohn.2013.22.1.66]
25. Kim JH, Oh PJ. Menopause symptoms and perceived cognitive decline in menopausal women: The mediating effect of health promotion behavior. Korean J Adult Nurs. 2017;29(2):200-10. [Link] [DOI:10.7475/kjan.2017.29.2.200]
26. Jarecka K, Bielawska-Batorowicz E. Quality of the relationship and menopausal symptoms of menopausal women. Health Psychol Rep. 2017;5(1):55-66. [Link] [DOI:10.5114/hpr.2017.62522]
27. Naworska B, Brzęk A, Bąk-Sosnowska M. The relationship between health status and social activity of perimenopausal and postmenopausal women (Health status and social relationships in menopause). Int J Environ Res Public Health. 2020;17(22):8388. [Link] [DOI:10.3390/ijerph17228388]
28. Converso D, Viotti S, Sottimano I, Loera B, Molinengo G, Guidetti G. The relationship between menopausal symptoms and burnout: A cross-sectional study among nurses. BMC Womens Health. 2019;19(1):1-12. [Link] [DOI:10.1186/s12905-019-0847-6]
29. Enjezab B, Farajzadegan Z, Taleghani F, Aflatoonian A, Morowatisharifabad MA. Health promoting behaviors in a population-based sample of middle-aged women and its relevant factors in Yazd, Iran. Int J Preventive Med. 2012;3(Suppl1):S191-8. [Link]
30. Kim MJ, Cho J, Ahn Y, Yim G, Park HY. Association between physical activity and menopausal symptoms in perimenopausal women. BMC Womens Health. 2014;14:122. [Link] [DOI:10.1186/1472-6874-14-122]
31. Dąbrowska-Galas M, Dąbrowska J, Ptaszkowski K, Plinta R. High physical activity level may reduce menopausal symptoms. Medicina. 2019;55(8):466. [Link] [DOI:10.3390/medicina55080466]
32. Stachowiak G, Pertyński T, Pertyńska-Marczewska M. Metabolic disorders in menopause. Prz Menopauzalny. 2015;14(1):59-64. [Link] [DOI:10.5114/pm.2015.50000]
33. Augoulea A, Palaiologou A, Christidi F, Armeni E, Soureti A, Alexandrou A, et al. Assessing the efficacy of a structured stress management program in reducing stress and climacteric symptoms in peri-and postmenopausal women. Arch Womens Ment Health. 2021;24(5):727-35. [Link] [DOI:10.1007/s00737-021-01106-7]
34. Wong C, Yip BHK, Gao T, Lam KYY, Woo DMS, Yip ALK, et al. Mindfulness-based stress reduction (MBSR) or psychoeducation for the reduction of menopausal symptoms: A randomized, controlled clinical trial. Sci Rep. 2018;8(1):6609. [Link] [DOI:10.1038/s41598-018-24945-4]
35. Pampel FC, Krueger PM, Denney JT. Socioeconomic disparities in health behaviors. Annu Rev Sociol. 2010;36:349-70. [Link] [DOI:10.1146/annurev.soc.012809.102529]
36. Ghorbani M, Azhari S, Esmaeili H, Alighanbari B. The survey of relationship between health promotion behaviors and vasomotor's symptoms in menopausal women in Mashhad, Iran. Iran J Nurs Midwifery Res. 2012;15(39):23-30. [Link]
37. Shakil Ahmad M, Fakhr Z, Ahmed J. Working women work‐life conflict. Bus Strategy Ser. 2011;12(6):289-302. [Link] [DOI:10.1108/17515631111185923]
38. Wang J, Geng L. Effects of socioeconomic status on physical and psychological health: Lifestyle as a mediator. Int J Environ Res Public Health. 2019;16(2):281. [Link] [DOI:10.3390/ijerph16020281]
39. Bohren MA, Hunter EC, Munthe-Kaas HM, Souza JP, Vogel JP, Gülmezoglu AM. Facilitators and barriers to facility-based delivery in low-and middle-income countries: a qualitative evidence synthesis. Reproductive Health. 2014;11(1):71. [Link] [DOI:10.1186/1742-4755-11-71]
40. Shirzadi S, Allahverdipour H, Sharma M, Hasankhani H. Perceived barriers to mammography adoption among women in Iran: A qualitative study. Korean J Fam Med. 2020;41(1):20. [Link] [DOI:10.4082/kjfm.18.0054]
41. Kim SS, Kim-Godwin YS, Koenig HG. Family spirituality and family health among Korean-American elderly couples. J Relig Health. 2016;55(2):729-46. [Link] [DOI:10.1007/s10943-015-0107-5]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |