



Volume 10, Issue 3 (2022)
Health Educ Health Promot 2022, 10(3): 459-465 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tiryag A, Atiyah M, Khudhair A. Nurses' Knowledge and Attitudes toward Thyroidectomy: A Cross-Sectional Study. Health Educ Health Promot 2022; 10 (3) :459-465
URL: http://hehp.modares.ac.ir/article-5-62784-en.html
URL: http://hehp.modares.ac.ir/article-5-62784-en.html

1- Fundamental of Nursing Department, College of Nursing, University of Basrah, Basrah, Iraq
Full-Text [PDF 499 kb]
(4647 Downloads)
| Abstract (HTML) (2017 Views)
Full-Text: (1811 Views)
Introduction
Thyroidectomy is one of the most frequent neck and endocrine procedures done today. While thyroid surgery mortality and morbidity rates have decreased due to technical developments, certain long-term consequences after thyroidectomy continue to be a health and societal burden [1]. Thyroid disorders such as thyroid cancer, noncancerous thyroid enlargement, and hyperactive thyroid are often treated by head and neck or endocrine surgeons via thyroidectomies [2]. Other reasons for thyroidectomy include a cosmetically enlarged thyroid or a symptomatic blockage that makes it difficult to breathe or swallow [3]. Also, obesity is a risk factor for many cancers, including thyroid cancer [4].
Graves’ disease, autoimmune thyroiditis, is the most common cause of hyperthyroidism. Total thyroidectomy is the treatment of choice when medical therapy by thyrostatic drugs fails to control the disease, and radio-iodine therapy is contraindicated. Surgery is the first-choice therapy for some patients, such as those with severe Graves’ ophthalmopathy, those with Graves’ disease, expecting pregnancy, and drug-induced thyrotoxicosis [5].
Since thyroid nodules are being found more often, thyroidectomy is a procedure that is frequently utilized; 50-70% of adults may have thyroid incidentalomas [6-8].
Over the last several decades, there has been a rise in thyroid cancer worldwide, which has led to an increase in thyroidectomies as a form of therapy [9].
Thyroid surgeries have grown threefold in the last three decades, with 118-166 thousand individuals receiving thyroidectomy annually in the United States for benign or malignant thyroid malignancies [10]. Around 13 thousand thyroid operations are performed annually in England [11]. It is frequently conducted on male and female patients. However, it is more common in females [12].
Between 200 to 800 million individuals worldwide suffer from thyroid illness. Over 20 million Americans get therapy for prevalent thyroid diseases [13].
Nowadays, thyroidectomy is one of the most commonly performed neck and endocrine surgeries due to advancements in the field. Although mortality and morbidity rates are low following thyroidectomy, some long-term complications persist as health and social problems [14]. There are three types of thyroidectomies: 1) total thyroidectomy, which completely removes the thyroid tissue; 2) bilateral subtotal thyroidectomy, which leaves some bilateral thyroid remains; and 3) unilateral total and contralateral subtotal thyroidectomy [15, 16]. When alternative therapies fail in young people, persons with big or suspicious nodules, and those with obstructive symptoms caused by pressure on the esophagus or trachea, surgery is indicated for immediate symptom relief. The most common procedure is a complete thyroidectomy. Enough of the thyroid gland is left after this treatment to create enough thyroid hormone. A complete thyroidectomy is done to treat thyroid cancer, and the patient will need hormone replacement for the rest of their lives [17].
Thyroid carcinoma is the most frequent endocrine disease that requires thyroidectomy and has a favorable result [18].
Surgical complications are classified as either early or late based on whether they arise during the first thirty days after surgery or later [19].
The Clavien-Dindo Classification, which is widely used, divides complications into four severity levels. Minor risk cases that did not necessitate treatment are classified as Grade 1 (with exceptions of analgesic, antipyretic, antiemetic, and antidiarrheal drugs or drugs required for lower urinary tract infection). Grade 2 complications are potentially life-threatening complications requiring surgery or a hospital stay that is more than twice the typical hospitalization time for the same operation. Complications of grade 3 were classified as those that resulted in long-term impairment or organ resection. Grade 4 complications are considered life-threatening, while Grade 5 complications result in a patient's death due to a complication [20].
Neck hematoma, postoperative hypocalcemia due to hypoparathyroidism, vocal cord paresis/paralysis due to damage to the recurrent laryngeal nerves, and postoperative surgical site infection are major complications after thyroid surgery. Patients differ in how seriously these complications affect them. There is an urgent need for treatment since they may be life-threatening in certain individuals, such as acute airway obstruction brought on by a post-operative neck hematoma or bilateral vocal cord paralysis. For example, severe hypocalcemia brought on by hypoparathyroidism or a neck abscess brought on by surgically unintentionally injuring the aerodigestive tracts need intense care in other individuals despite their mild severity [21]. Patients commonly experience uncomfortable neck symptoms, including pain, tension, and pressure, as well as stiffness in the shoulder and restricted range of motion in the neck and shoulder [22].
The incidence of postoperative neck hematoma is between 0.6-2% [23]. Most rebleeding occurs during the first postoperative hours when the patient is observed in the postoperative care unit. Almost 90% of the patients who suffer from this complication bleed within 24 hours of the operation [24].
Postoperative vocal cord palsy occurs due to injury to the recurrent laryngeal nerve. The condition can be unilateral or bilateral, permanent, or transient. The incidence of permanent unilateral vocal cord palsy is 3-5%, whereas bilateral permanent vocal cord palsy is 0.01-0.02% [25]. The recurrent laryngeal nerves course adjacent to the dorsal side of the thyroid gland when entering the vocal muscles on both sides [26].
Postoperative hypocalcemia is a consequence of postoperative hypoparathyroidism. Parathyroid glands are closely attached to the thyroid gland. Hypoparathyroidism occurs when parathyroid glands are removed or injured during surgery. Hypoparathyroidism may be transient or permanent. In large cohort studies, the incidence of transient and permanent postoperative hypoparathyroidism is between 7.6 and 12.5% [27]. Permanent hypoparathyroidism is associated with an increased risk of morbidity and mortality [28, 29].
After thyroid surgery, postoperative surgical site infection is 0.5-2.0% [30]. The infection leads to prolonged thyroid surgery, worsened cosmesis, and increased healthcare costs [31].
A patient's medical history, physical exam findings, and test results all play a role in determining if thyroidectomy is necessary. The most frequent examinations to determine if thyroidectomy is required include a fine needle aspiration biopsy, thyroid scan, thyroid X-ray, ultrasound, X-ray and/or CT scan, and measurement of thyroid hormone levels [32].
The nurse oversees the collection of preoperative screening procedures and reviews the results. Common laboratory studies include a complete blood cell count (CBC), electrolytes, blood urea nitrogen (BUN), and creatinine. Other screening tests that can be obtained in obese patients include a sleep study, upper endoscopy, electrocardiogram (ECG), lipid panel, aspartate aminotransferase (AST), alanine aminotransferase (ALT), glucose, and hemoglobin A1c (HbA1c), as well as iron, vitamin B12, thiamine, and folate [33].
A nurse is essential to the treatment and care of patients and their planning for surgery, informing patients about potential complications following surgery and discharge preparation [34]. Preoperative and postoperative nursing care is critical because poor thyroid surgery preparation and poor postoperative nursing care directly impact patients' recovery, jeopardize their lives, and ultimately harm their quality of life. Observing the patient's condition, aiding and working with the surgeon for treatment, and proactively dealing with severe post-thyroidectomy consequences are all part of nursing care before and after thyroid surgery [35].
Following surgery, the nurse will maintain the patient in the proper posture, splint the incision, provide pain treatment and wound care, educate the patient on how to deal with voice changes, and assist them with neck exercises and nutritional therapy. Additionally, the patient should be aware of the warning signs and symptoms of wound complications and infection. Patients should be advised to seek medical attention if they have any neuromuscular excitability signs or symptoms. The follow-up appointments that include suture and drain removal, voice quality evaluation, calcium status control, and discussion of any relevant difficulties are crucial [36].
This study aimed to assess nurses' knowledge and attitudes about thyroidectomy.
Instrument and Methods
A descriptive cross-sectional study was conducted on nurses’ knowledge and attitudes toward thyroidectomy at all Al-Basrah Governorate Hospitals (Al-Sader Teaching Hospital, Al-Faiha Teaching Hospital, Al-Basrah Teaching Hospital, Abi Al-Khasib General Hospital, Umm Qasr General Hospital, Al-Faw General Hospital, Al-Qurna Hospital, Al-Zubair General Hospital, Al-Shifaa Hospital, and Al-Mawani Teaching Hospital). The study period was extended from the 15th of November 2021 to the 1st of April 2022. The data collection period was extended from the 27th of December 2021 to the 27th of February 2022. A non-probability purposive sample consists of most nurses working in the surgical wards and operating rooms (N=200). Twenty Nurses for the pilot study were excluded from the study.
To accomplish the objectives, the researcher created a questionnaire based on an exhaustive analysis of related literature and previous studies, which was then used to gather data for the study project related to thyroidectomy. It consists of five parts. The study instrument was composed of five parts: the first part consists of the demographic variables of the nurses, the second part consists of knowledge about thyroidectomy (10 items), and the third part: consists of knowledge about complications of thyroidectomy (8 items), fourth part: consist of knowledge about postoperative nursing care (13 items), fifth part: consist of attitudes about thyroidectomy (7 items). Each question in the first four parts assessed involved three items (Know, Uncertain, and Don’t Know) and scored as (3 for “Know” answer, 2 for Uncertain, and 1 for “Don’t Know”). Each question in the fifth part that assesses attitudes involved three items (Yes, No, Don’t Know) and scored as (3 for Yes, 2 for Don’t Know, 1 for No). About 15-20 minutes are given to complete the questionnaire. We use the 3-Points Likert Scale ranging from (1 up to 3). This scale is composed of 39 items, and these items were measured on a three-point Likert scale, which ranged from 1 (Don't know), 2 (Uncertain), and 3 (Know). The level of assessment for each item in the knowledge scales was estimated by calculating the cut-off point for the mean of the score and scored as follows: The researcher determined a 1-1.66 score for poor knowledge, 1.67-2.33 score for moderate knowledge, and 2.34-3 score for the high knowledge. The instrument's reliability was determined through Cronbach’s alpha method for 38 items. The validity of the study instrument was determined through a list of 15 experts. The experts had at least 10 years of experience in their field. These experts were given a copy of the research instrument and asked to review and test it for material clarity and adequacy to investigate the questionnaire's content.
The data analysis used was descriptive statistics and statistical inferential to find the differences between the demographic variables of the nurses and their knowledge and attitudes. Data were analyzed through the use of SPSS application version 26.0. Inferential data analysis includes the Chi-square and Fisher’s exact tests.
Findings
Most nurses were female, 20-29 years old, married, 1-5 years of experience, work in the surgical wards, and had no training course in thyroidectomy (Table 1).
The majority of the nurses had poor knowledge, and attitudes about thyroidectomy (Table 2).
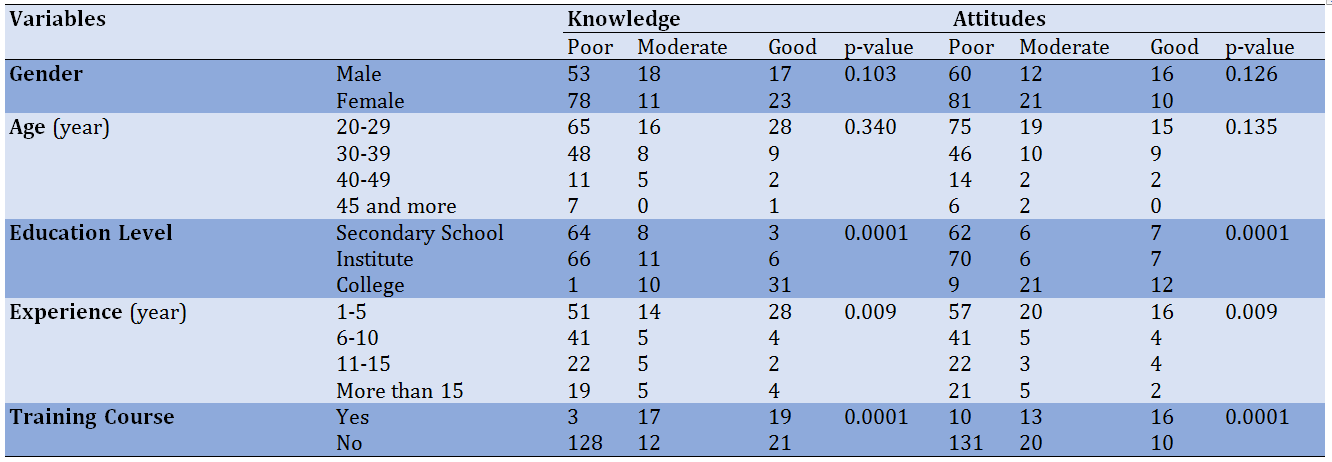
There was a significant relationship between nurses' education level, years of experience, and training courses and their knowledge of thyroidectomy (p<0.05). Also, these findings show no significant relationship between nurses' gender, age, marital status, and place of work and their knowledge about thyroidectomy at a (p>0.05). There was a significant relationship between nurses' (education level, years of experience, and training courses) and their attitudes toward thyroidectomy (p<0.05). Also, the findings show no significant relationship between nurses' gender, age, marital status, and place of work and their attitudes about thyroidectomy (p>0.05; Table 3).
Table 1) Results of nurses demographic data (N=200)
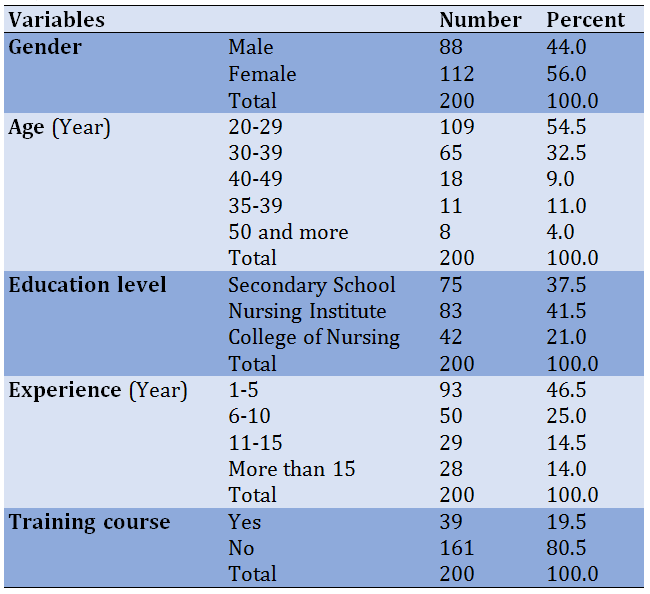
Table 2) Results of nurses' knowledge and attitude toward thyroidectomy
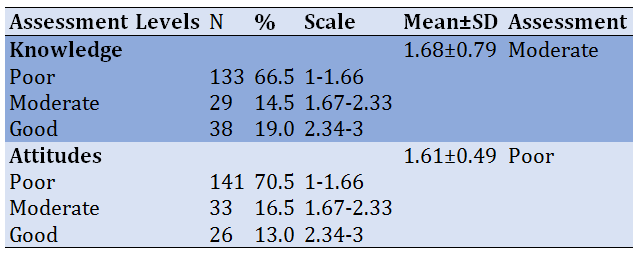
Table 3) Relationships of demographic variables with nurses' knowledge and attitudes
Discussion
The characteristics of the study sample involved in this study Regarding gender, this study shows that more than half of the samples are female and accounted for (56%). This study agreed with the study revealing that most respondents were female [2]. Nurses are mostly female over the globe. In Iraq, females are accepted more often than males into the college of nursing and nursing Institute.
Regarding age in this study, the age group (20-29) years old (54.5%). These results agreed with a study that the majority of the nurses were between (20-29) years old (43%) [2]. The researcher noted that surgical ward and operating room nurses are younger, which is good since they desire to learn more and enhance their skills. Furthermore, this task requires greater muscular effort.
The present study has the highest percentage regarding educational level with the nursing institute (41.5%). The findings of this study agreed with the study in which nursing diploma was the highest proportion (94.4%) [3]. We have a secondary school of nursing, a nursing institute, and a nursing college in Iraq. Nursing graduates from secondary schools and nursing institutes work in practically every ward. College nursing graduates, on the other hand, work in critical wards, and their percentage is less than other nurses.
Regarding years of experience, this study reveals that most nurses who work in the surgical wards were between 1-5 years of experience, with a percentage of 46.5%. These results agree with the study which shows that most of the sample has 1-5 years of experience [2].
Most nurses have no training course (80.5%) concerning training courses. The results of this study are consistent with those which reveal that most nurses do not have a training course [38].
The current study explored the statistics of nurses’ knowledge of thyroidectomy. Nurses’ knowledge statistics are classified into three main domains: Nurses’ knowledge about thyroidectomy, nurses’ knowledge about complications of thyroidectomy, and nurses’ knowledge concerning postoperative nursing care.
According to the findings of this study, the bulk of the nurses (66.5%) have poor knowledge about thyroidectomy.
The researcher believes that nurses’ poor knowledge regarding thyroidectomy might be due to many causes. Nurses did not study enough about thyroidectomy at all nursing education levels. The nurses do not have adequate training courses about thyroidectomy, and the nurses do not update their knowledge continuously. The results of this study agreed with the study [35] that results showed that most nurses have inadequate knowledge (68.3%) toward operative management for patients with thyroidectomy. Also, it agreed with the study [2] that the knowledge level of the 3rd year bachelor in nursing students regarding the management of patients after thyroidectomy was below average.
According to the findings of this study, there is no significant relationship between nurses' knowledge and demographic variables of the study group concerning (gender and age). Other studies have also shown no major differences between demographic variables and nurses' knowledge [35]. This supports the findings of this study and mentions in their results that the nurses' demographic variables did not affect the results.
According to the present study results, most nurses (70.5%) have poor attitudes about thyroidectomy. The results of this study agreed with a study conducted in Bangladesh on nurses' knowledge and attitudes concerning post-thyroidectomy pain management, and their practices reported that nurses had an unsatisfactory level of knowledge and attitudes in post thyroidectomy pain management [39]. Also, it is the opposite of a study conducted in Egypt on nurses’ knowledge, attitude, and practice regarding patients undergoing thyroidectomy. The results show that studied nurses had a high attitude related to thyroidectomy [38].
According to the result of this study, there is a significant relationship between nurses' knowledge and their demographic variables (education level and years of experience). The results agreed with a study [38] that showed a significant relationship between nurses' attitudes, educational levels, and years of experience.
The researcher recommends the following based on the results of this study: Providing education programs for nurses to improve their knowledge about thyroidectomy. Training courses should be provided to these nurses to increase their knowledge about thyroidectomy, complications of thyroidectomy, and pre and postoperative nursing care. Providing booklets for nurses related to thyroidectomy, complications of thyroidectomy, and everything about this surgery (pre and postoperative nursing care). The researcher recommended more studies about thyroidectomy because of the deficit of studies in Iraq. Creating a continued education unit in the surgical ward to help nurses develop their knowledge about thyroidectomy because the curriculum at all levels of nursing doesn't include thyroidectomy, complications of thyroidectomy, and pre and postoperative nursing care. The lack of relevant published literature and research studies and the difficulty to collect all nurses from Al-Basrah Teaching Hospital because this hospital is for COVID-19 patients were limitations.
Conclusion
Most of the nurses who participated in the present study have moderate knowledge and poor attitudes about thyroidectomy.
Acknowledgments: None declared.
Ethical Permissions: None declared.
Conflicts of Interests: None declared.
Authors’ Contributions: Tiryag AM (First Author), Methodologist/Statistical Analyst (40%); Atiyah MA (Second Author), Introduction Writer/Assistant Researcher (30%); Khudhair AA (Third Author), Assistant Researcher/Discussion Writer (30%)
Funding/Support: None declared.
Thyroidectomy is one of the most frequent neck and endocrine procedures done today. While thyroid surgery mortality and morbidity rates have decreased due to technical developments, certain long-term consequences after thyroidectomy continue to be a health and societal burden [1]. Thyroid disorders such as thyroid cancer, noncancerous thyroid enlargement, and hyperactive thyroid are often treated by head and neck or endocrine surgeons via thyroidectomies [2]. Other reasons for thyroidectomy include a cosmetically enlarged thyroid or a symptomatic blockage that makes it difficult to breathe or swallow [3]. Also, obesity is a risk factor for many cancers, including thyroid cancer [4].
Graves’ disease, autoimmune thyroiditis, is the most common cause of hyperthyroidism. Total thyroidectomy is the treatment of choice when medical therapy by thyrostatic drugs fails to control the disease, and radio-iodine therapy is contraindicated. Surgery is the first-choice therapy for some patients, such as those with severe Graves’ ophthalmopathy, those with Graves’ disease, expecting pregnancy, and drug-induced thyrotoxicosis [5].
Since thyroid nodules are being found more often, thyroidectomy is a procedure that is frequently utilized; 50-70% of adults may have thyroid incidentalomas [6-8].
Over the last several decades, there has been a rise in thyroid cancer worldwide, which has led to an increase in thyroidectomies as a form of therapy [9].
Thyroid surgeries have grown threefold in the last three decades, with 118-166 thousand individuals receiving thyroidectomy annually in the United States for benign or malignant thyroid malignancies [10]. Around 13 thousand thyroid operations are performed annually in England [11]. It is frequently conducted on male and female patients. However, it is more common in females [12].
Between 200 to 800 million individuals worldwide suffer from thyroid illness. Over 20 million Americans get therapy for prevalent thyroid diseases [13].
Nowadays, thyroidectomy is one of the most commonly performed neck and endocrine surgeries due to advancements in the field. Although mortality and morbidity rates are low following thyroidectomy, some long-term complications persist as health and social problems [14]. There are three types of thyroidectomies: 1) total thyroidectomy, which completely removes the thyroid tissue; 2) bilateral subtotal thyroidectomy, which leaves some bilateral thyroid remains; and 3) unilateral total and contralateral subtotal thyroidectomy [15, 16]. When alternative therapies fail in young people, persons with big or suspicious nodules, and those with obstructive symptoms caused by pressure on the esophagus or trachea, surgery is indicated for immediate symptom relief. The most common procedure is a complete thyroidectomy. Enough of the thyroid gland is left after this treatment to create enough thyroid hormone. A complete thyroidectomy is done to treat thyroid cancer, and the patient will need hormone replacement for the rest of their lives [17].
Thyroid carcinoma is the most frequent endocrine disease that requires thyroidectomy and has a favorable result [18].
Surgical complications are classified as either early or late based on whether they arise during the first thirty days after surgery or later [19].
The Clavien-Dindo Classification, which is widely used, divides complications into four severity levels. Minor risk cases that did not necessitate treatment are classified as Grade 1 (with exceptions of analgesic, antipyretic, antiemetic, and antidiarrheal drugs or drugs required for lower urinary tract infection). Grade 2 complications are potentially life-threatening complications requiring surgery or a hospital stay that is more than twice the typical hospitalization time for the same operation. Complications of grade 3 were classified as those that resulted in long-term impairment or organ resection. Grade 4 complications are considered life-threatening, while Grade 5 complications result in a patient's death due to a complication [20].
Neck hematoma, postoperative hypocalcemia due to hypoparathyroidism, vocal cord paresis/paralysis due to damage to the recurrent laryngeal nerves, and postoperative surgical site infection are major complications after thyroid surgery. Patients differ in how seriously these complications affect them. There is an urgent need for treatment since they may be life-threatening in certain individuals, such as acute airway obstruction brought on by a post-operative neck hematoma or bilateral vocal cord paralysis. For example, severe hypocalcemia brought on by hypoparathyroidism or a neck abscess brought on by surgically unintentionally injuring the aerodigestive tracts need intense care in other individuals despite their mild severity [21]. Patients commonly experience uncomfortable neck symptoms, including pain, tension, and pressure, as well as stiffness in the shoulder and restricted range of motion in the neck and shoulder [22].
The incidence of postoperative neck hematoma is between 0.6-2% [23]. Most rebleeding occurs during the first postoperative hours when the patient is observed in the postoperative care unit. Almost 90% of the patients who suffer from this complication bleed within 24 hours of the operation [24].
Postoperative vocal cord palsy occurs due to injury to the recurrent laryngeal nerve. The condition can be unilateral or bilateral, permanent, or transient. The incidence of permanent unilateral vocal cord palsy is 3-5%, whereas bilateral permanent vocal cord palsy is 0.01-0.02% [25]. The recurrent laryngeal nerves course adjacent to the dorsal side of the thyroid gland when entering the vocal muscles on both sides [26].
Postoperative hypocalcemia is a consequence of postoperative hypoparathyroidism. Parathyroid glands are closely attached to the thyroid gland. Hypoparathyroidism occurs when parathyroid glands are removed or injured during surgery. Hypoparathyroidism may be transient or permanent. In large cohort studies, the incidence of transient and permanent postoperative hypoparathyroidism is between 7.6 and 12.5% [27]. Permanent hypoparathyroidism is associated with an increased risk of morbidity and mortality [28, 29].
After thyroid surgery, postoperative surgical site infection is 0.5-2.0% [30]. The infection leads to prolonged thyroid surgery, worsened cosmesis, and increased healthcare costs [31].
A patient's medical history, physical exam findings, and test results all play a role in determining if thyroidectomy is necessary. The most frequent examinations to determine if thyroidectomy is required include a fine needle aspiration biopsy, thyroid scan, thyroid X-ray, ultrasound, X-ray and/or CT scan, and measurement of thyroid hormone levels [32].
The nurse oversees the collection of preoperative screening procedures and reviews the results. Common laboratory studies include a complete blood cell count (CBC), electrolytes, blood urea nitrogen (BUN), and creatinine. Other screening tests that can be obtained in obese patients include a sleep study, upper endoscopy, electrocardiogram (ECG), lipid panel, aspartate aminotransferase (AST), alanine aminotransferase (ALT), glucose, and hemoglobin A1c (HbA1c), as well as iron, vitamin B12, thiamine, and folate [33].
A nurse is essential to the treatment and care of patients and their planning for surgery, informing patients about potential complications following surgery and discharge preparation [34]. Preoperative and postoperative nursing care is critical because poor thyroid surgery preparation and poor postoperative nursing care directly impact patients' recovery, jeopardize their lives, and ultimately harm their quality of life. Observing the patient's condition, aiding and working with the surgeon for treatment, and proactively dealing with severe post-thyroidectomy consequences are all part of nursing care before and after thyroid surgery [35].
Following surgery, the nurse will maintain the patient in the proper posture, splint the incision, provide pain treatment and wound care, educate the patient on how to deal with voice changes, and assist them with neck exercises and nutritional therapy. Additionally, the patient should be aware of the warning signs and symptoms of wound complications and infection. Patients should be advised to seek medical attention if they have any neuromuscular excitability signs or symptoms. The follow-up appointments that include suture and drain removal, voice quality evaluation, calcium status control, and discussion of any relevant difficulties are crucial [36].
This study aimed to assess nurses' knowledge and attitudes about thyroidectomy.
Instrument and Methods
A descriptive cross-sectional study was conducted on nurses’ knowledge and attitudes toward thyroidectomy at all Al-Basrah Governorate Hospitals (Al-Sader Teaching Hospital, Al-Faiha Teaching Hospital, Al-Basrah Teaching Hospital, Abi Al-Khasib General Hospital, Umm Qasr General Hospital, Al-Faw General Hospital, Al-Qurna Hospital, Al-Zubair General Hospital, Al-Shifaa Hospital, and Al-Mawani Teaching Hospital). The study period was extended from the 15th of November 2021 to the 1st of April 2022. The data collection period was extended from the 27th of December 2021 to the 27th of February 2022. A non-probability purposive sample consists of most nurses working in the surgical wards and operating rooms (N=200). Twenty Nurses for the pilot study were excluded from the study.
To accomplish the objectives, the researcher created a questionnaire based on an exhaustive analysis of related literature and previous studies, which was then used to gather data for the study project related to thyroidectomy. It consists of five parts. The study instrument was composed of five parts: the first part consists of the demographic variables of the nurses, the second part consists of knowledge about thyroidectomy (10 items), and the third part: consists of knowledge about complications of thyroidectomy (8 items), fourth part: consist of knowledge about postoperative nursing care (13 items), fifth part: consist of attitudes about thyroidectomy (7 items). Each question in the first four parts assessed involved three items (Know, Uncertain, and Don’t Know) and scored as (3 for “Know” answer, 2 for Uncertain, and 1 for “Don’t Know”). Each question in the fifth part that assesses attitudes involved three items (Yes, No, Don’t Know) and scored as (3 for Yes, 2 for Don’t Know, 1 for No). About 15-20 minutes are given to complete the questionnaire. We use the 3-Points Likert Scale ranging from (1 up to 3). This scale is composed of 39 items, and these items were measured on a three-point Likert scale, which ranged from 1 (Don't know), 2 (Uncertain), and 3 (Know). The level of assessment for each item in the knowledge scales was estimated by calculating the cut-off point for the mean of the score and scored as follows: The researcher determined a 1-1.66 score for poor knowledge, 1.67-2.33 score for moderate knowledge, and 2.34-3 score for the high knowledge. The instrument's reliability was determined through Cronbach’s alpha method for 38 items. The validity of the study instrument was determined through a list of 15 experts. The experts had at least 10 years of experience in their field. These experts were given a copy of the research instrument and asked to review and test it for material clarity and adequacy to investigate the questionnaire's content.
The data analysis used was descriptive statistics and statistical inferential to find the differences between the demographic variables of the nurses and their knowledge and attitudes. Data were analyzed through the use of SPSS application version 26.0. Inferential data analysis includes the Chi-square and Fisher’s exact tests.
Findings
Most nurses were female, 20-29 years old, married, 1-5 years of experience, work in the surgical wards, and had no training course in thyroidectomy (Table 1).
The majority of the nurses had poor knowledge, and attitudes about thyroidectomy (Table 2).
There was a significant relationship between nurses' education level, years of experience, and training courses and their knowledge of thyroidectomy (p<0.05). Also, these findings show no significant relationship between nurses' gender, age, marital status, and place of work and their knowledge about thyroidectomy at a (p>0.05). There was a significant relationship between nurses' (education level, years of experience, and training courses) and their attitudes toward thyroidectomy (p<0.05). Also, the findings show no significant relationship between nurses' gender, age, marital status, and place of work and their attitudes about thyroidectomy (p>0.05; Table 3).
Table 1) Results of nurses demographic data (N=200)
Table 2) Results of nurses' knowledge and attitude toward thyroidectomy
Table 3) Relationships of demographic variables with nurses' knowledge and attitudes
Discussion
The characteristics of the study sample involved in this study Regarding gender, this study shows that more than half of the samples are female and accounted for (56%). This study agreed with the study revealing that most respondents were female [2]. Nurses are mostly female over the globe. In Iraq, females are accepted more often than males into the college of nursing and nursing Institute.
Regarding age in this study, the age group (20-29) years old (54.5%). These results agreed with a study that the majority of the nurses were between (20-29) years old (43%) [2]. The researcher noted that surgical ward and operating room nurses are younger, which is good since they desire to learn more and enhance their skills. Furthermore, this task requires greater muscular effort.
The present study has the highest percentage regarding educational level with the nursing institute (41.5%). The findings of this study agreed with the study in which nursing diploma was the highest proportion (94.4%) [3]. We have a secondary school of nursing, a nursing institute, and a nursing college in Iraq. Nursing graduates from secondary schools and nursing institutes work in practically every ward. College nursing graduates, on the other hand, work in critical wards, and their percentage is less than other nurses.
Regarding years of experience, this study reveals that most nurses who work in the surgical wards were between 1-5 years of experience, with a percentage of 46.5%. These results agree with the study which shows that most of the sample has 1-5 years of experience [2].
Most nurses have no training course (80.5%) concerning training courses. The results of this study are consistent with those which reveal that most nurses do not have a training course [38].
The current study explored the statistics of nurses’ knowledge of thyroidectomy. Nurses’ knowledge statistics are classified into three main domains: Nurses’ knowledge about thyroidectomy, nurses’ knowledge about complications of thyroidectomy, and nurses’ knowledge concerning postoperative nursing care.
According to the findings of this study, the bulk of the nurses (66.5%) have poor knowledge about thyroidectomy.
The researcher believes that nurses’ poor knowledge regarding thyroidectomy might be due to many causes. Nurses did not study enough about thyroidectomy at all nursing education levels. The nurses do not have adequate training courses about thyroidectomy, and the nurses do not update their knowledge continuously. The results of this study agreed with the study [35] that results showed that most nurses have inadequate knowledge (68.3%) toward operative management for patients with thyroidectomy. Also, it agreed with the study [2] that the knowledge level of the 3rd year bachelor in nursing students regarding the management of patients after thyroidectomy was below average.
According to the findings of this study, there is no significant relationship between nurses' knowledge and demographic variables of the study group concerning (gender and age). Other studies have also shown no major differences between demographic variables and nurses' knowledge [35]. This supports the findings of this study and mentions in their results that the nurses' demographic variables did not affect the results.
According to the present study results, most nurses (70.5%) have poor attitudes about thyroidectomy. The results of this study agreed with a study conducted in Bangladesh on nurses' knowledge and attitudes concerning post-thyroidectomy pain management, and their practices reported that nurses had an unsatisfactory level of knowledge and attitudes in post thyroidectomy pain management [39]. Also, it is the opposite of a study conducted in Egypt on nurses’ knowledge, attitude, and practice regarding patients undergoing thyroidectomy. The results show that studied nurses had a high attitude related to thyroidectomy [38].
According to the result of this study, there is a significant relationship between nurses' knowledge and their demographic variables (education level and years of experience). The results agreed with a study [38] that showed a significant relationship between nurses' attitudes, educational levels, and years of experience.
The researcher recommends the following based on the results of this study: Providing education programs for nurses to improve their knowledge about thyroidectomy. Training courses should be provided to these nurses to increase their knowledge about thyroidectomy, complications of thyroidectomy, and pre and postoperative nursing care. Providing booklets for nurses related to thyroidectomy, complications of thyroidectomy, and everything about this surgery (pre and postoperative nursing care). The researcher recommended more studies about thyroidectomy because of the deficit of studies in Iraq. Creating a continued education unit in the surgical ward to help nurses develop their knowledge about thyroidectomy because the curriculum at all levels of nursing doesn't include thyroidectomy, complications of thyroidectomy, and pre and postoperative nursing care. The lack of relevant published literature and research studies and the difficulty to collect all nurses from Al-Basrah Teaching Hospital because this hospital is for COVID-19 patients were limitations.
Conclusion
Most of the nurses who participated in the present study have moderate knowledge and poor attitudes about thyroidectomy.
Acknowledgments: None declared.
Ethical Permissions: None declared.
Conflicts of Interests: None declared.
Authors’ Contributions: Tiryag AM (First Author), Methodologist/Statistical Analyst (40%); Atiyah MA (Second Author), Introduction Writer/Assistant Researcher (30%); Khudhair AA (Third Author), Assistant Researcher/Discussion Writer (30%)
Funding/Support: None declared.
Article Type: Original Research |
Subject:
Health Promotion Setting
Received: 2022/04/7 | Accepted: 2022/07/20 | Published: 2022/08/10
Received: 2022/04/7 | Accepted: 2022/07/20 | Published: 2022/08/10
References
1. Christou N, Mathonnet M. Complications after total thyroidectomy. J Visc Surg. 2013;150(4):249-56. [Link] [DOI:10.1016/j.jviscsurg.2013.04.003]
2. Shaama W, M N, Amukugo HJ. Knowledge of the University Of Namibia third year bacherol in nursing students regarding post operative management of patients after thyroidectomy. Int J Med Sci Health Res. 2018;2(04):187-97. [Link]
3. Brunner LS. Brunner & Suddarth's textbook of medical-surgical nursing. Lippincott Williams & Wilkins; 2010. [Link]
4. Tiryag AM, Atiyah HH. Nurses' knowledge toward obesity in al-Basra city. Ann Romanian Socr Cell Biol. 2021;25(5):4667-73. [Link]
5. Smithson M, Asban A, Miller J, Chen H. Considerations for thyroidectomy as a treatment for graves disease. clinical medicine insights. Endocrinology and Diabetes. 2019;12. [Link] [DOI:10.1177/1179551419844523]
6. Dionigi G, Bacuzzi A, Bertocchi V, Carrafiello G, Boni L, Rovera F, et al. Prospectives and surgical usefulness of perioperative parathyroid hormone assay in thyroid surgery. Expert Rev Med Devices. 2008;5(6):699-704. [Link] [DOI:10.1586/17434440.5.6.699]
7. Hallgrimsson P, Nordenström E, Bergenfelz A, Almquist M. Hypocalcaemia after total thyroidectomy for Graves' disease and for benign atoxic multinodular goiter. Langenbecks Arch Surg. 2012;397:1133-7. [Link] [DOI:10.1007/s00423-012-0981-1]
8. Hughes OR, Scott-Coombes DM. Hypocalcaemia following thyroidectomy for treatment of Graves' disease: implications for patient management and cost-effectiveness. J Laryngol Otol. 2011;125(8):849-52. [Link] [DOI:10.1017/S0022215111001332]
9. La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F, et al. Thyroid cancer mortality and incidence: a global overview. Int J Cancer. 2015;136(9):2187-95. [Link] [DOI:10.1002/ijc.29251]
10. Chandrasekhar SS, Randolph GW, Seidman MD, Rosenfeld RM, Angelos P, Barkmeier-Kraemer J, et al. Clinical practice guideline: improving voice outcomes after thyroid surgery. Otolaryngol Head Neck Surg. 2013;148(suppl 6):S1-37. [Link] [DOI:10.1177/0194599813487301]
11. Stedman T, Chew P, Truran P, Lim CB, Balasubramanian SP. Modification, validation, and implementation of a protocol for post-thyroidectomy hypocalcemia. Ann Rl Coll Surg Engl. 2018;100(2):135-9. [Link] [DOI:10.1308/rcsann.2017.0194]
12. Liu ZW, Masterson L, Fish B, Jani P, Chatterjee K. Thyroid surgery for Graves' disease and Graves' ophthalmopathy. Cochrane Database Syst Rev. 2015(11):CD010576. [Link] [DOI:10.1002/14651858.CD010576.pub2]
13. Hassan A, El-Sayed S, Taha M. Impact of a designed educational program on thyroidectomy patients' discharge compliance instructions. J Am Scie. 2012;8(11):1-3. [Link]
14. Solan J, McKiernan J. Thyroidectomy: The ambulatory nurse's role in preventing long-term sequelae. Oncol Nurs Forum. 2007;34(2):515. [Link]
15. Abd-El Mohsen SA, Ahmed NM. Effect of teaching patients neck stretching exercises on neck pain and disability following thyroidectomy. J Nurs Educ Pract. 2018;8(1). [Link] [DOI:10.5430/jnep.v8n1p107]
16. Hashem EM, Mohammed ZA, Ahmed MT, Azer SZ, Abd-Elmohsen SA. Effect of designed nursing guidelines on minimizing postoperative complications for patients undergoing thyroidectomy. Assiut Sci Nurs J. 2018;6(13):29-38. [Link] [DOI:10.21608/asnj.2018.58902]
17. Quérat C, Germain N, Dumollard JM, Estour B, Peoc'h M, Prades JM. Surgical management of hyperthyroidism. Eur Ann Otorhinolaryngol Head Neck Dis. 2015;132(2):63-6. [Link] [DOI:10.1016/j.anorl.2014.04.005]
18. Kandil E, Noureldine SI, Abbas A, Tufano RP. The impact of surgical volume on patient outcomes following thyroid surgery. Surgery. 2013;154(6):1346-53. [Link] [DOI:10.1016/j.surg.2013.04.068]
19. Giordano S. Bariatric and post-bariatric surgery: from metabolic surgery to plastic surgery indications [dissertation]. Turku: University of Turku; 2014. [Finnish] [Link]
20. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-13. [Link] [DOI:10.1097/01.sla.0000133083.54934.ae]
21. Filho JG, Kowalski LP. Surgical complications after thyroid surgery performed in a cancer hospital. Otolaryngol Head Neck Surg. 2005;132(3):490-4. [Link] [DOI:10.1016/j.otohns.2004.09.028]
22. Lewis SM, Dirksen SR, Heitkemper MM, Bucher L, Harding M. Medical-surgical nursing: assessment and management of clinical problems. New York: Mosby; 2013. [Link]
23. Weiss A, Lee KC, Brumund KT, Chang DC, Bouvet M. Risk factors for hematoma after thyroidectomy: results from the nationwide inpatient sample. Surgery. 2014;156(2):399-404. [Link] [DOI:10.1016/j.surg.2014.03.015]
24. Farooq MS, Nouraei R, Kaddour H, Saharay M. Patterns, timing and consequences of post-thyroidectomy hemorrhage. Ann R Coll Surg Engl. 2017;99(1):60-2. [Link] [DOI:10.1308/rcsann.2016.0270]
25. Bergenfelz A, Salem AF, Jacobsson H, Nordenström E, Almquist M, Wallin GW, et al. Risk of recurrent laryngeal nerve palsy in patients undergoing thyroidectomy with and without intraoperative nerve monitoring. J Br Surg. 2016;103(13):1828-38. [Link] [DOI:10.1002/bjs.10276]
26. Mohebati A, Shaha AR. Anatomy of thyroid and parathyroid glands and neurovascular relations. Clin Anat. 2012;25(1):19-31. [Link] [DOI:10.1002/ca.21220]
27. Annebäck M, Hedberg J, Almquist M, Stålberg P, Norlén O. Risk of permanent hypoparathyroidism after total thyroidectomy for benign disease: a nationwide population-based cohort study from Sweden. Ann Surg. 2021;274:e1202-8. [Link] [DOI:10.1097/SLA.0000000000003800]
28. Bergenfelz A, Nordenström E, Almquist M. Morbidity in patients with permanent hypoparathyroidism after total thyroidectomy. Surgery. 2020;167(1):124-8. [Link] [DOI:10.1016/j.surg.2019.06.056]
29. Almquist M, Ivarsson K, Nordenström E, Bergenfelz A. Mortality in patients with permanent hypoparathyroidism after total thyroidectomy. J Br Surg. 2018;105(10):1313-8. [Link] [DOI:10.1002/bjs.10843]
30. Bures C, Zielinski V, Klatte T, Swietek N, Kober F, Tatzgern E, et al. Streptococcal mediastinitis after thyroidectomy. A literature review. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen. 2015;86(12):1145-50. [Link] [DOI:10.1007/s00104-014-2972-y]
31. Urban JA. Cost analysis of surgical site infections. Surg Infect. 2006;7(S1):s19-22. [Link] [DOI:10.1089/sur.2006.7.s1-19]
32. Hassan A. Impact of nursing educational program on patients' outcome among patients undergoing thyroidectomy at general surgical departments el-manial university hospital. Diss. Cairo University. 2012. [Link]
33. Mechanick JI, Youdim A, Jones DB, Garvey WT, Hurley DL, McMahon MM, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient-2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Surg Obes Relat Dis. 2013;9(2):159-91. [Link] [DOI:10.1016/j.soard.2012.12.010]
34. Tiryag AM, Atiyah HH. Nurses' Knowledge toward Bariatric Surgery at Surgical Wards at Teaching Hospitals in Al-Basra City. Ind J Forensic Med Toxicol. 2021;15(3):5153. [Link]
35. Sulaiman AI, Al-Saigh TH. Assessment of nurses knowledge towards post thyroidectomy management in Nineveh Governorate Hospitals. Sch J Mosul Univ. 2020;8(1):25-31. [Link] [DOI:10.33899/mjn.2020.164619]
36. Furtado L. Thyroidectomy: postoperative care and common complications. Nurs Stand. 2011; 25(34):43-52. [Link] [DOI:10.7748/ns2011.04.25.34.43.c8470]
37. Desoky AA, Mohamed MA, Ahmed MT, Ghanem HM. Assessment of nurses' performance for patients undergoing thyroidectomy at Assiut university hospital. AAMJ. 2009;7(2):18-223. [Link]
38. El-Shenawie AE, Aly-Baghdady EG, Mohammed YF. Nurses' knowledge, attitude, and practice regarding patients undergoing thyroidectomy. Int J Novel Res Healthc Nurs. 2021;8(1):781-95. [Link]
39. Basak S. Knowledge and attitudes of nurses and their practices regarding post-operative pain management in Bangladesh [dissertation]. Songkhla: Prince of Songkla University; 2010. [Link]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |