



Volume 10, Issue 3 (2022)
Health Educ Health Promot 2022, 10(3): 433-441 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sklempe Kokic I, Barusic Z, Crnkovic Knezevic M, Benko Mestrovic S, Duvnjak I. Physical Activity and Health-Promoting Behaviours of Nurses and Physiotherapists: a Cross-Sectional Survey. Health Educ Health Promot 2022; 10 (3) :433-441
URL: http://hehp.modares.ac.ir/article-5-62111-en.html
URL: http://hehp.modares.ac.ir/article-5-62111-en.html

1- Faculty of Kinesiology Osijek, Josip Juraj Strossmayer University of Osijek, Osijek, Croatia
2- Community Care Institution Jadranka Pluzaric, Osijek, Croatia
3- Department of Health Studies, College of Applied Sciences, Lavoslav Ruzicka in Vukovar, Vukovar, Croatia
4- Special Hospital for Lung Disease, Zagreb, Croatia
2- Community Care Institution Jadranka Pluzaric, Osijek, Croatia
3- Department of Health Studies, College of Applied Sciences, Lavoslav Ruzicka in Vukovar, Vukovar, Croatia
4- Special Hospital for Lung Disease, Zagreb, Croatia
Full-Text [PDF 492 kb]
(4276 Downloads)
| Abstract (HTML) (2730 Views)
Table 1) Results of participants' characteristics
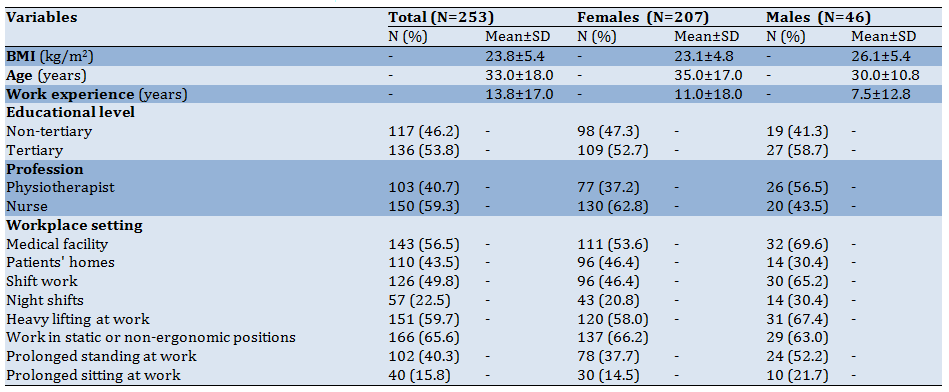
Table 2) Results of HPLP-II (Mean±SD)
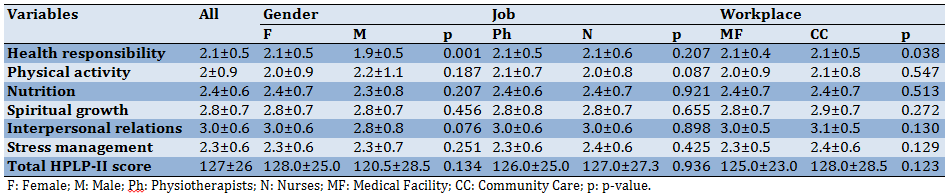
Table 3) Health-related quality of life, EQ-5D-5L (Numbers in parentheses are in percent)

Table 4) Results of physical activity, and sedentary behavior in metabolic equivalents-hours per week (MET-hours/week)

Discussion
Data on physical activity, and health-promoting behaviors of physiotherapists, and nurses in different work settings are limited. To our knowledge, this is the first study that investigates, and compares physiotherapists', and nurses' habits of physical activity, health-promoting behavior, and health-related quality of life, and relationships among them across different work settings, and conditions.
Adequate levels of physical activity including regular exercise, and healthy habits are an essential part of a healthy lifestyle. Healthcare workers, including physiotherapists, and nurses have a chance to actively promote a healthy lifestyle. However, in order to look credible in the eyes of their patients, they should do what they “preach”.
Adoption of health-promoting behaviors is a key factor in health promotion, and disease prevention, and these behaviors are expected from those who educate patients on a healthy lifestyle. Higher rates of work-related stress in healthcare jobs are associated with mental health problems, job dissatisfaction, and decreased levels of healthy lifestyle engagement [18]. Healthy behaviors can enhance the ability of healthcare workers to cope with job-related stress [19]. A recent study showed that healthcare workers adopt better nutrition, more physical activity, and greater health responsibility in comparison to other professions [16]. However, these differences were not found in other sub-scales of the HPLP-II like spiritual growth, interpersonal relations, and stress management.
Our total score on the HPLP-II questionnaire which measures health-promoting behaviors was 127 (average score 2. 4) with no differences by gender, profession, or work setting. This was slightly lower than the scores reported by Kurnat-Thoma et al. [15] where the average score was 2, 9, and Al-Qahtani [14] where it was 2.7. The highest scores were reported in the domains of interpersonal relationships, and spiritual growth, and the lowest score was in the domain of physical activity. This is similar to the results from studies performed on nurses in Saudi Arabia [14], and American nurses in community hospitals [15].
We also found differences between male, and female respondents, but only in the sub-scale health responsibility where females scored higher. This is under a previous study where female students scored higher in that domain in comparison to male students [20]. However, in this study, females also scored higher in the total HPLP-II score and sub-scales nutrition, interpersonal relations, and stress management, which was not the case in our study. Another study performed by Wei et al. [21] found that female respondents had higher scores on sub-scales health responsibility, interpersonal relations, and nutrition than males who scored better on sub-scale physical activity.
In our sample, there was an inverse relationship between age, the total HPLP-II score, and several sub-scales. This was also reported in a recent study performed on community hospital nurses [15]. The finding that the age of health professionals can negatively impact perceptions, and engagement in a healthy lifestyle is very important, and it warrants some concern, and need for action.
Although sub-scale physical activity had the lowest score among HPLP-II sub-scales in our sample, leisure-time physical activity, and walking were in a positive relationship with the total HPLP-II score, and several sub-scales. However, surprisingly, sub-scale interpersonal relationships were in an inverse relationship with the total level of physical activity, and vigorous-intensity physical activity.
There is a positive relationship between health-related quality of life and physical activity which was confirmed by previous studies [22]. While most of our respondents did not report any problems in the majority of the EQ-5D-5L domains, a relatively high percentage reported problems in domains of pain/discomfort, and anxiety, especially female respondents. This could be due to demand, and stressful job conditions in combination with domestic duties, and family obligations. The average score of self-rated health was 85 for the total sample and significantly lower in the subgroup of female respondents which scored 80 on average. Nurses reported more problems with usual activities than physiotherapists, probably due to more difficult working conditions which include heavy lifting, work in static, and non-ergonomic positions, and prolonged standing periods a greater percentage than physiotherapists.
The EQ-VAS positively correlated with the HPLP-II total score, and several sub-scales of HPLP-II: physical activity, spiritual growth, interpersonal relations, and stress management. However, the inverse relationship between age, and work experience could be due to difficult working conditions in healthcare, and burn-out. On the other hand, there was a positive relationship between EQ-VAS and leisure-time physical activity. A previous study also reported a positive relationship between health-related quality of life, and leisure-time physical activity [23].
The reported level of total physical activity in our sample was on average 207 MET-hours/week, which is equivalent to approximately 7 hours of moderate or 3. 5 hours of vigorous physical activity per day. This was considerably higher than the total physical activity among middle-aged employees in Croatia who scored 79 MET-hours/week on average [24]. This means that majority of our respondents exceeded current WHO guidelines which recommend 150 minutes of moderate-intensity aerobic physical activity or at least 75 minutes of vigorous-intensity aerobic activity per week [2]. Indeed, our sample exceeded even the guidelines for physical activity needed to gain additional health benefits which recommend at least 300 minutes of moderate-intensity or 150 minutes of vigorous-intensity physical activity per week. However, most of the physical activity was accumulated within the work domain, and only 18 MET-hours/week were accumulated in the domain of leisure, which is equivalent to approximately 0.6 hours of moderate-intensity or 0.3 hours of vigorous-intensity physical activity.
These results are similar to the study performed on Polish nurses, and midwives [25] where average levels of total physical activity were 262 MET-hours/week among those who work rotating night shifts, and 207 MET-hours/week among those who work only day shifts. Likewise, their levels of leisure-time physical activity were a bit lower than our results, ranging from 11.7 to 13. 2 MET-hours/week. Peplonska et al. [25] also reported lower levels of leisure-time physical activity among nurses and midwives working night shifts which we confirmed in our results not only for leisure-time physical activity, but also for total physical activity, walking, moderate-, and vigorous-intensity physical activity.
Other workplace characteristics which could be considered difficult working conditions like heavy lifting, working in static or non-ergonomic positions, or prolonged standing were also in inverse relationship with levels of physical activity. Another study performed on Danish female nurses also found a significantly lower average number of hours spent on sports activities (2.8 vs. 4.2) among nurses who worked after midnight in comparison to those who never work after midnight [26]. Jurakic et al. [24] found that leisure-time physical activity was not related to work characteristics among middle-aged employees, but another previous study has shown that stressful work increases the likelihood of physical inactivity in leisure time [27].
Interestingly, physiotherapists reported lower levels of total, moderate-, and vigorous-intensity physical activity than nurses. It was hypothesized that physiotherapists will score higher than nurses since they have extensive knowledge, and education regarding the importance of exercise, and physical activity, and their main role is to prescribe those to the patients. The inverse relationship between age and levels of physical activity was another surprising finding. This was contrary to the results of Hallal et al. [28], however, following the results obtained by Jurakic et al. [29] on a sample of the Croatian population where physical activity scores increased with advancing age.
A comparison of physical activity levels by gender revealed that men are considerably more active than women in work, and leisure domains, and men have higher scores for total, and vigorous-intensity physical activity. This is under some previous studies which reported the same [24, 30].
The strength of our study is the use of valid, and reliable questionnaires which allows the comparison of our results with other studies. The IPAQ-L questionnaire covers all important domains of physical activity, and it has proven validity and reliability. The HPLP-II and EQ-5D-5L are also well-known, valid, and reliable survey tools. Furthermore, this study is the first to investigate patterns of physical activity among physiotherapists, and nurses, and their relationship with health-promoting behaviors, and health-related quality of life. Considering that improvements in the adoption of healthy habits among healthcare workers could directly influence the adoption of healthy habits by their patients in a positive way, the results of this study could help to plan worksite interventions aimed at healthcare workers to adopt healthy habits and physical activity.
The main study limitations include cross-sectional nature and convenience sample which precluded establishing any causal relationships among the observed variables. Also, there is a possibility of self-report bias. Another limitation may apply to the study regarding its generalization to populations other than nurses, physiotherapists, and in other countries. Our study was conducted from September to January, so another limitation may arise from the assumption that the level of physical activity varied between autumn and winter. Due to low levels of leisure-time physical activity, and the positive relationship to a healthy lifestyle, and quality of life, it is recommended to take measures among healthcare workers to increase the levels of leisure-time physical activity.
Conclusion
The results demonstrated high levels of physical activity among nurses, and physiotherapists irrespective of their work setting, but relatively low levels of active transportation, and leisure-time physical activity. There is a positive relationship between leisure-time physical activity, health-related quality of life, and health-promoting behaviors. Further research should use objective methods of determining levels of physical activity to avoid over-, and under-reporting, and include other groups of healthcare professionals.
Acknowledgments: The authors are grateful to all the participants for their involvement in the study.
Ethical Permissions: The study was approved by the Ethics Committee of Community Care Institution Jadranka Pluzaric, Osijek, Croatia, and the Ethics Committee of County General Hospital Vinkovci, Vinkovci, Croatia.
Conflicts of Interests: The authors declared no potential conflicts of interest for the research, authorship, and/or publication of this article.
Authors' Contribution: Sklempe Kokic I (First Author), Main Researcher/Statistical Analyst (30%); Barusic, Z (Second Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%); Crnkovic Knezevic M (Third Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%); Benko Mestrovic S (Fourth Author), Introduction Writer/Discussion Writer/Methodologist (15%); Duvnjak I (Fifth Author), Introduction Writer/Methodologist/Discussion Writer (15%)
Funding/Support: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Full-Text: (568 Views)
Introduction
Low levels of physical activity, obesity, and a sedentary lifestyle are of great concern worldwide. These are major contributors to the prevalence of many chronic diseases and premature mortality. Physical inactivity is the fourth leading risk factor for global mortality (6% of deaths globally) after high blood pressure (13%); high blood glucose (6%), overweightness, and obesity (5%); which are all associated with physical inactivity [1, 2].
Heart disease, stroke, hypertension, type 2 diabetes, dementia, depression, postpartum depression, excessive weight gain, falls with injuries among the elderly, and several types of cancer are less common among physically active individuals, along with reduced risks of mortality, and of developing or progression of other chronic diseases or conditions [3]. Physical activity also improves physical function, and quality of life, while prolonged sedentary time is independently associated with poor health outcomes [3].
Physical activity is bodily movement produced by skeletal muscles that result in energy expenditure, while exercise represents a physical activity that is planned, structured, repetitive, and designed to improve or maintain physical fitness, physical performance, or health [4]. Sedentary behavior is any waking behavior characterized by an energy expenditure of 1. 5 or less metabolic equivalents of task (MET) while sitting, reclining, or lying [3]. Health-promoting lifestyle is a multidimensional pattern of self-initiated perceptions, and actions aimed to maintain or improve the individual's wellness [5].
In the adult population, physical activity includes recreational or leisure-time physical activity, active transportation, occupational, and household activities [2]. Adults aged 18-64 years should do at least 150 minutes of moderate-intensity aerobic physical activity, at least 75 minutes of vigorous-intensity aerobic physical activity, or the equivalent combination of moderate-, and vigorous-intensity activity throughout the week in bouts of at least 10 minutes duration, e. g. 500 to 1000 MET-minutes of moderate-to-vigorous physical activity [2, 3]. This should include muscle-strengthening activities involving major muscle groups on at least 2 days a week. Additional health benefits can be gained by increasing moderate, and vigorous-intensity aerobic physical activities to 300, and 150 minutes per week, respectively. Worldwide, 1 in 4 adults does not currently meet the global recommendations for physical activity set by World Health Organization (WHO) [6]. In Croatia, 30.5% of the adult population is considered physically inactive [7].
The workplace has been recognized internationally as an appropriate setting for health promotion, and disease prevention, which should be further stimulated by advocating a healthy diet, and physical activity among workers [8]. Furthermore, health practitioners including nurses and physiotherapists could have an important role in the promotion of physical activity, and health-promoting behaviors among co-workers, and patients, and they are expected to act as role models.
A recent study showed that healthcare workers believe that they should serve as role models for the promotion of healthy behaviors and that they should practice a healthy lifestyle [9]. Also, physiotherapists, physiotherapy assistants, and students of physiotherapy reported higher rates of physical activity than health-diagnosing professionals, and the general adult population [10]. Healthcare workers are expected to have more knowledge about the importance of physical activity, healthy behaviors, and their long-term consequences than the general population.
However, there is still limited data related to physical activity, and health-promoting behaviors of nurses, and physiotherapists in different work settings. We were unable to find published studies documenting differences in physical activity habits, health-promoting behaviors, and health-related quality of life between physiotherapists, and nurses.
The objective of this study was to investigate and compare health-promoting behaviors, levels of physical activity, and health-related quality of life among nurses, and physiotherapists working in two different work settings –medical facilities, and community care. The secondary objective was to explore associations between health-related quality of life, levels of physical activity, and health-promoting behaviors in these two groups of healthcare professionals. We hypothesized that physiotherapists and those working in community care will accumulate higher levels of physical activity and that those with higher levels of physical activity, and health-promoting behaviors will report better health-related quality of life.
Instrument and Methods
In this cross-sectional survey study, we collected data from a convenience sample of nurses, and physiotherapists employed in three county general hospitals, one inpatient rehabilitation facility, and two institutions registered for community healthcare in continental Croatia. Individuals aged 18-65 years currently employed as physiotherapists or nurses were eligible to participate. Potential participants were excluded if they were retired or unemployed or if they had contraindications to moderate-to-vigorous intensity physical activity. The sample size was estimated using several possible calculation methods. We took into account the proportion of nurses, and physiotherapists in Croatia, and calculated the sample size for the known population with the formula for z-values, and margin of error. Additionally, we used Minitab software (Minitab LLC, State College, PA, USA) and, considering the study design, performed an a priori analysis for the sample size estimation. For the significance level of 0.05, and desired statistical power of 0.95, the minimum sample size was calculated to be N=202, with a margin of error of 0.05.
Demographic information collected by the questionnaires included data on age, gender, body height, body mass, educational level, profession, professional experience, work setting, and work conditions. Body mass index (BMI) was calculated according to a standard equation from self-reports of body height, and body mass.
- Physical activity was assessed using International Physical Activity Questionnaire -Long Form (IPAQ-L) (Croatian version) [11, 12]. This physical activity questionnaire is publicly available, and free to use without permission. The IPAQ-L requires respondents to recall their physical activity from the previous 7-day period. It consists of 27 questions about frequency, duration, and intensity of activity on weekdays, and weekends in four different domains: occupation, transportation, domestic, and leisure. Furthermore, IPAQ also includes three questions regarding sedentary time. For each domain-specific MET values are assigned: walking (3. 3), moderate activity (3.0-4.0), cycling (6.0), and vigorous activity (5. 5-8.0). One MET is the rate of energy expenditure while sitting at rest, which, for most people approximates an oxygen uptake of 3. 5 milliliters per kilogram per minute [3]. Data were processed according to established guidelines [13] and presented as MET-hours per week.
- Health Promoting Lifestyle Profile II (HPLP-II) was used for the assessment of health-promoting behaviors. It is a validated 52-item questionnaire used for the measurement of health behaviors of workers in different occupations [14-16] comprising six components of a healthy lifestyle: health responsibility, physical activity, nutrition, spiritual growth, interpersonal relations, and stress management [5]. Respondents are asked to report on the frequency of health-promoting behaviors on a 4-point Likert scale ranging from never (1) to routinely (4). The HPLP-II was translated to Croatian with the author's permission, and following accepted standards, using the back-translation technique for assuring linguistic validity. The total HPLP-II score ranges from 52 to 208, with higher scores indicating a higher presence of health-promoting behaviors. To calculate the subscale scores, the scores for each item in each subscale were added and then divided by the number of items in that subscale.
- Health-related quality of life was measured using the new five-level version of the EQ-5D (EQ-5D-5L) questionnaire, the Croatian version. It is a self-report, valid, and reliable tool designed by the EuroQol Research Foundation, which includes five dimensions of health: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, and a visual analog scale (VAS) designed to give an overall, self-report summary evaluation of an individual’s health status [17]. We registered the use of the questionnaire with the EuroQol Research Foundation and obtained their permission. The respondents chose five levels of severity (1, no problem; 2, slight problem; 3, moderate problem; 4, severe problem, and 5, unable to/extreme problem) in five dimensions, and rated their overall health status via the EuroQol-visual analog scale (EQ-VAS) by selecting a point on a continuous scale from 0 (worst state) to 100 (best state). Participants were categorized into two groups: those reporting no problems at all versus those reporting problems of any severity in any of the five dimensions of health.
Participants were recruited through e-mail, social networking, and word-of-mouth. Participation was voluntary and anonymous, and all participants gave their written consent. We obtained ethical approval for our study from the relevant research ethics boards in institutions where we performed data collection. Data were collected between September 2017, and January 2018 using paper-based survey questionnaires which included demographic information, self-reported physical activity levels, health-promoting behaviors, and health-related quality of life.
Statistical analyses were performed using SPSS 19.0 (IBM, Armonk, NY, USA). The level of significance was set at p<0.05. The Shapiro-Wilk test was performed to check for normality of data and showed non-normal distribution for all variables. Values for continuous variables were presented as medians, and inter-quartile ranges and categorical variables were summarized by frequencies and percentages. Fisher's Exact Test was used to test for differences between gender, profession, and work setting for categorical variables. Due to non-normal distribution, the Mann-Whitney U test was used for continuous variables. Spearman's correlation (rs) analyses were performed to examine the association across different domains, intensities of physical activity, scores of the HPLP-II questionnaire, EQ-VAS, and continuous variables of demographic characteristics. Point-biserial correlation coefficient (rpbi) was calculated to assess for an association between specific working conditions (shift work, night work, and difficult working conditions), and continuous variables.
Findings
Two hundred fifty-three participants were included in our analysis (median age of 33±18, 81.8% females, 59. 3% nurses, and 56. 5% working in a medical facility). The BMI for the total sample (23.8±5.4 kg/m2), and all subgroups were within the normal range except for the male participants who can be classified as overweight (26.1±5.4kg/m2). Almost half of the participants worked in shifts (49.8%), and almost a quarter worked night shifts (22.5%). Most of the participants had reported difficult working conditions, 59.7% reported heavy lifting at work, and 65. 6% work in static or non-ergonomic positions. Less than half of the participants reported prolonged standing at work (40.3%), and only 15. 8% reported prolonged periods of sitting at work (Table 1).
Table 2 shows the scores of the HPLP-II questionnaire for the total sample, and by gender, profession, and work setting. The average total score was 127.0±26.0, and there were no differences between female, and male participants, nor by profession or work setting. The highest average score on the sub-scales of the HPLP-II was for interpersonal relationships followed by spiritual growth, while the lowest average score was for physical activity. The only differences in HPLP-II scores were found for the sub-scale health responsibility between female, and male participants (p<0.001), and between those working in a medical facility, and those working in community care (p=0.038). Female participants reported higher values than males. Furthermore, although median values by work setting were the same for the two subgroups, those working in community care had higher mean scores than the subgroup working in a medical facility.
We found weak, but negative significant correlations between age, and work experience, and subscales of physical activity (p=0.005, rs=-0.177; p=0.009, rs=-0.164), spiritual growth (p<0.001, rs=-0.304; p<0.001, rs=-0.259), interpersonal relations (p<0.001, rs=-0.242; p<0.001, rs=-0.231), and the total HPLP-II score (p<0.001, rs=-0.229; p=0.001, rs=-0.213). Furthermore, BMI was also negatively associated with the sub-scale physical activity (p<0.049, rs=-0.124), and the total HPLP-II score (p<0.048, rs=-0.124). A weak but significant negative correlation was found between HPLP-II total score, and working night shifts (p=0.026, rpbi=-0.140).
EQ-5D-5L results for the total sample, and by gender, profession, and work setting are presented in Table 3. While the majority of respondents did not report any problems in mobility; self-care, and usual activities, a substantial percentage of respondents reported slight or more severe problems in the dimensions of pain/discomfort and anxiety. The EQ-VAS average score was 85±16. 5 for the total sample. While there were no differences regarding work setting we found differences between females, and males, physiotherapists, and nurses in several EQ-5D-5L dimensions. While no male respondent reported problems in usual activities, 13. 8% of female respondents reported slight or more severe problems in that dimension (p=0.001). Furthermore, a higher percentage of female respondents reported problems in the pain/discomfort dimension. The EQ-VAS was higher for male respondents. The only difference between physiotherapists and nurses was in the dimension of usual activities. Nurses reported problems during usual activities in a higher percentage than physiotherapists.
The EQ-VAS positively correlated with the HPLP-II total score (p<0.001, rs=0.231), and several sub-scales: physical activity (p=0.001, rs=0.208), spiritual growth (p<0.001, rs=0.273), interpersonal relations (p=0.002, rs=0.189), and stress management (p=0.044, rs=0.127). Furthermore, it was negatively associated with age (p<0.001, rs=-0.244), BMI (p=0.044, rs=-0.127), and work experience (p=<0.001, rs=-0.243).
The median total physical activity which included domains of work, transport, domestic, garden, and leisure for the total sample was 207. 1±293. 5 MET-hours/week. Most physical activities were accumulated in the domain of work followed by domestic, and garden activities, and the least physical activity was accumulated in the domain of transport followed by leisure. Male respondents accumulated higher levels of physical activity in the work domain in comparison to females. This was also the case for the domain of leisure, and total levels of physical activity. Furthermore, male respondents accumulated higher levels of vigorous-intensity physical activity. Nurses accumulated higher levels of total physical activity than physiotherapists. Likewise, nurses accumulated higher levels of moderate-intensity physical activity and vigorous-intensity physical activity. Respondents working in community care reported higher levels of physical activity in the domain of transport in comparison with those working in a medical facility (Table 4).
There was a positive relationship between age, and work experience, and physical activity in domains of work (p=0.001, rs=0.207; p<0.001, rs=0.218), and domestic (p<0.001, rs=0.232; p<0.001, rs=0.233), and total levels of physical activity (p<0.001, rs=0.222; p<0.001, rs=0.238), moderate-intensity physical activity (p<0.001, rs=0.247; p<0.001, rs=0.262), and vigorous-intensity physical activity (p=0.006, rs=0.173; p=0.001, rs=0.204). Furthermore, BMI was associated with levels of physical activity in the work domain (p<0.001, rs=0.227), total levels of physical activity (p=0.010, rs=0.161), moderate-, and vigorous-intensity physical activity (p=0.016, rs=0.151; p=0.003, rs=0.185). Physical activity in the domain leisure was positively correlated with total HPLP-II score (p<0.001, rs=0.299), and several subscales: health responsibility (p=0.004, rs=0.181), physical activity (p<0.001, rs=0.445), nutrition (p=0.002, rs=0.194), and stress management (p=0.001, rs=0.209).
Levels of total physical activity were negatively correlated with HPLP-II sub-scale interpersonal relations (p=0.044, rs=-0.127). Walking positively correlated with total HPLP-II score (p=0.040, rs=0.129), and sub-scales for physical activity (p=0.026, rs=0.140), and nutrition (p=0.032, rs=0.135). Vigorous-intensity physical activity negatively correlated with HPLP-II sub-scale interpersonal relations (p=0.037, rs=-0.131), and sedentary activity negatively correlated with sub-scale nutrition (p=0.019, rs=-0.148). There was a positive relationship between EQ-VAS, and levels of physical activity in the domain of leisure (p=0.047, rs=0.125).
There was a negative relationship between working nights, and levels of physical activity in the domain of leisure (p=0.001, rpbi=-0.210), total physical activity (p<0.001, rpbi=-0.276), walking (P=0.007, rpbi=-0.169), moderate-intensity, and vigorous-intensity physical activity (p<0.001, rpbi=-0.248; p<0.001, rpbi=-0.242). Levels of total physical activity were also negatively correlated with heavy lifting at work (p<0.001, rpbi=-0.329), work in static or non-ergonomic positions (p<0.001, rpbi=-0.250), and prolonged standing at work (p=0.001, rpbi=-0.216). Physical activity in the domain of leisure was also negatively associated with prolonged standing at work (p=0.028, rpbi=-0.138). There was a negative relationship between levels of moderate-, and vigorous-intensity physical activity, and heavy lifting at work (p<0.001, rpbi=-0.222); p<0.001, rpbi=-0.349), work in static, and non-ergonomic positions (p=0.003, rpbi=-0.186; p<0.001, rpbi=-0.281), and prolonged standing at work (p<0.001, rpbi=-0.231; p=0.002, rpbi=-0.196). Furthermore, walking was negatively associated with heavy lifting at work (p=0.002, rpbi=-0.190).
Low levels of physical activity, obesity, and a sedentary lifestyle are of great concern worldwide. These are major contributors to the prevalence of many chronic diseases and premature mortality. Physical inactivity is the fourth leading risk factor for global mortality (6% of deaths globally) after high blood pressure (13%); high blood glucose (6%), overweightness, and obesity (5%); which are all associated with physical inactivity [1, 2].
Heart disease, stroke, hypertension, type 2 diabetes, dementia, depression, postpartum depression, excessive weight gain, falls with injuries among the elderly, and several types of cancer are less common among physically active individuals, along with reduced risks of mortality, and of developing or progression of other chronic diseases or conditions [3]. Physical activity also improves physical function, and quality of life, while prolonged sedentary time is independently associated with poor health outcomes [3].
Physical activity is bodily movement produced by skeletal muscles that result in energy expenditure, while exercise represents a physical activity that is planned, structured, repetitive, and designed to improve or maintain physical fitness, physical performance, or health [4]. Sedentary behavior is any waking behavior characterized by an energy expenditure of 1. 5 or less metabolic equivalents of task (MET) while sitting, reclining, or lying [3]. Health-promoting lifestyle is a multidimensional pattern of self-initiated perceptions, and actions aimed to maintain or improve the individual's wellness [5].
In the adult population, physical activity includes recreational or leisure-time physical activity, active transportation, occupational, and household activities [2]. Adults aged 18-64 years should do at least 150 minutes of moderate-intensity aerobic physical activity, at least 75 minutes of vigorous-intensity aerobic physical activity, or the equivalent combination of moderate-, and vigorous-intensity activity throughout the week in bouts of at least 10 minutes duration, e. g. 500 to 1000 MET-minutes of moderate-to-vigorous physical activity [2, 3]. This should include muscle-strengthening activities involving major muscle groups on at least 2 days a week. Additional health benefits can be gained by increasing moderate, and vigorous-intensity aerobic physical activities to 300, and 150 minutes per week, respectively. Worldwide, 1 in 4 adults does not currently meet the global recommendations for physical activity set by World Health Organization (WHO) [6]. In Croatia, 30.5% of the adult population is considered physically inactive [7].
The workplace has been recognized internationally as an appropriate setting for health promotion, and disease prevention, which should be further stimulated by advocating a healthy diet, and physical activity among workers [8]. Furthermore, health practitioners including nurses and physiotherapists could have an important role in the promotion of physical activity, and health-promoting behaviors among co-workers, and patients, and they are expected to act as role models.
A recent study showed that healthcare workers believe that they should serve as role models for the promotion of healthy behaviors and that they should practice a healthy lifestyle [9]. Also, physiotherapists, physiotherapy assistants, and students of physiotherapy reported higher rates of physical activity than health-diagnosing professionals, and the general adult population [10]. Healthcare workers are expected to have more knowledge about the importance of physical activity, healthy behaviors, and their long-term consequences than the general population.
However, there is still limited data related to physical activity, and health-promoting behaviors of nurses, and physiotherapists in different work settings. We were unable to find published studies documenting differences in physical activity habits, health-promoting behaviors, and health-related quality of life between physiotherapists, and nurses.
The objective of this study was to investigate and compare health-promoting behaviors, levels of physical activity, and health-related quality of life among nurses, and physiotherapists working in two different work settings –medical facilities, and community care. The secondary objective was to explore associations between health-related quality of life, levels of physical activity, and health-promoting behaviors in these two groups of healthcare professionals. We hypothesized that physiotherapists and those working in community care will accumulate higher levels of physical activity and that those with higher levels of physical activity, and health-promoting behaviors will report better health-related quality of life.
Instrument and Methods
In this cross-sectional survey study, we collected data from a convenience sample of nurses, and physiotherapists employed in three county general hospitals, one inpatient rehabilitation facility, and two institutions registered for community healthcare in continental Croatia. Individuals aged 18-65 years currently employed as physiotherapists or nurses were eligible to participate. Potential participants were excluded if they were retired or unemployed or if they had contraindications to moderate-to-vigorous intensity physical activity. The sample size was estimated using several possible calculation methods. We took into account the proportion of nurses, and physiotherapists in Croatia, and calculated the sample size for the known population with the formula for z-values, and margin of error. Additionally, we used Minitab software (Minitab LLC, State College, PA, USA) and, considering the study design, performed an a priori analysis for the sample size estimation. For the significance level of 0.05, and desired statistical power of 0.95, the minimum sample size was calculated to be N=202, with a margin of error of 0.05.
Demographic information collected by the questionnaires included data on age, gender, body height, body mass, educational level, profession, professional experience, work setting, and work conditions. Body mass index (BMI) was calculated according to a standard equation from self-reports of body height, and body mass.
- Physical activity was assessed using International Physical Activity Questionnaire -Long Form (IPAQ-L) (Croatian version) [11, 12]. This physical activity questionnaire is publicly available, and free to use without permission. The IPAQ-L requires respondents to recall their physical activity from the previous 7-day period. It consists of 27 questions about frequency, duration, and intensity of activity on weekdays, and weekends in four different domains: occupation, transportation, domestic, and leisure. Furthermore, IPAQ also includes three questions regarding sedentary time. For each domain-specific MET values are assigned: walking (3. 3), moderate activity (3.0-4.0), cycling (6.0), and vigorous activity (5. 5-8.0). One MET is the rate of energy expenditure while sitting at rest, which, for most people approximates an oxygen uptake of 3. 5 milliliters per kilogram per minute [3]. Data were processed according to established guidelines [13] and presented as MET-hours per week.
- Health Promoting Lifestyle Profile II (HPLP-II) was used for the assessment of health-promoting behaviors. It is a validated 52-item questionnaire used for the measurement of health behaviors of workers in different occupations [14-16] comprising six components of a healthy lifestyle: health responsibility, physical activity, nutrition, spiritual growth, interpersonal relations, and stress management [5]. Respondents are asked to report on the frequency of health-promoting behaviors on a 4-point Likert scale ranging from never (1) to routinely (4). The HPLP-II was translated to Croatian with the author's permission, and following accepted standards, using the back-translation technique for assuring linguistic validity. The total HPLP-II score ranges from 52 to 208, with higher scores indicating a higher presence of health-promoting behaviors. To calculate the subscale scores, the scores for each item in each subscale were added and then divided by the number of items in that subscale.
- Health-related quality of life was measured using the new five-level version of the EQ-5D (EQ-5D-5L) questionnaire, the Croatian version. It is a self-report, valid, and reliable tool designed by the EuroQol Research Foundation, which includes five dimensions of health: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, and a visual analog scale (VAS) designed to give an overall, self-report summary evaluation of an individual’s health status [17]. We registered the use of the questionnaire with the EuroQol Research Foundation and obtained their permission. The respondents chose five levels of severity (1, no problem; 2, slight problem; 3, moderate problem; 4, severe problem, and 5, unable to/extreme problem) in five dimensions, and rated their overall health status via the EuroQol-visual analog scale (EQ-VAS) by selecting a point on a continuous scale from 0 (worst state) to 100 (best state). Participants were categorized into two groups: those reporting no problems at all versus those reporting problems of any severity in any of the five dimensions of health.
Participants were recruited through e-mail, social networking, and word-of-mouth. Participation was voluntary and anonymous, and all participants gave their written consent. We obtained ethical approval for our study from the relevant research ethics boards in institutions where we performed data collection. Data were collected between September 2017, and January 2018 using paper-based survey questionnaires which included demographic information, self-reported physical activity levels, health-promoting behaviors, and health-related quality of life.
Statistical analyses were performed using SPSS 19.0 (IBM, Armonk, NY, USA). The level of significance was set at p<0.05. The Shapiro-Wilk test was performed to check for normality of data and showed non-normal distribution for all variables. Values for continuous variables were presented as medians, and inter-quartile ranges and categorical variables were summarized by frequencies and percentages. Fisher's Exact Test was used to test for differences between gender, profession, and work setting for categorical variables. Due to non-normal distribution, the Mann-Whitney U test was used for continuous variables. Spearman's correlation (rs) analyses were performed to examine the association across different domains, intensities of physical activity, scores of the HPLP-II questionnaire, EQ-VAS, and continuous variables of demographic characteristics. Point-biserial correlation coefficient (rpbi) was calculated to assess for an association between specific working conditions (shift work, night work, and difficult working conditions), and continuous variables.
Findings
Two hundred fifty-three participants were included in our analysis (median age of 33±18, 81.8% females, 59. 3% nurses, and 56. 5% working in a medical facility). The BMI for the total sample (23.8±5.4 kg/m2), and all subgroups were within the normal range except for the male participants who can be classified as overweight (26.1±5.4kg/m2). Almost half of the participants worked in shifts (49.8%), and almost a quarter worked night shifts (22.5%). Most of the participants had reported difficult working conditions, 59.7% reported heavy lifting at work, and 65. 6% work in static or non-ergonomic positions. Less than half of the participants reported prolonged standing at work (40.3%), and only 15. 8% reported prolonged periods of sitting at work (Table 1).
Table 2 shows the scores of the HPLP-II questionnaire for the total sample, and by gender, profession, and work setting. The average total score was 127.0±26.0, and there were no differences between female, and male participants, nor by profession or work setting. The highest average score on the sub-scales of the HPLP-II was for interpersonal relationships followed by spiritual growth, while the lowest average score was for physical activity. The only differences in HPLP-II scores were found for the sub-scale health responsibility between female, and male participants (p<0.001), and between those working in a medical facility, and those working in community care (p=0.038). Female participants reported higher values than males. Furthermore, although median values by work setting were the same for the two subgroups, those working in community care had higher mean scores than the subgroup working in a medical facility.
We found weak, but negative significant correlations between age, and work experience, and subscales of physical activity (p=0.005, rs=-0.177; p=0.009, rs=-0.164), spiritual growth (p<0.001, rs=-0.304; p<0.001, rs=-0.259), interpersonal relations (p<0.001, rs=-0.242; p<0.001, rs=-0.231), and the total HPLP-II score (p<0.001, rs=-0.229; p=0.001, rs=-0.213). Furthermore, BMI was also negatively associated with the sub-scale physical activity (p<0.049, rs=-0.124), and the total HPLP-II score (p<0.048, rs=-0.124). A weak but significant negative correlation was found between HPLP-II total score, and working night shifts (p=0.026, rpbi=-0.140).
EQ-5D-5L results for the total sample, and by gender, profession, and work setting are presented in Table 3. While the majority of respondents did not report any problems in mobility; self-care, and usual activities, a substantial percentage of respondents reported slight or more severe problems in the dimensions of pain/discomfort and anxiety. The EQ-VAS average score was 85±16. 5 for the total sample. While there were no differences regarding work setting we found differences between females, and males, physiotherapists, and nurses in several EQ-5D-5L dimensions. While no male respondent reported problems in usual activities, 13. 8% of female respondents reported slight or more severe problems in that dimension (p=0.001). Furthermore, a higher percentage of female respondents reported problems in the pain/discomfort dimension. The EQ-VAS was higher for male respondents. The only difference between physiotherapists and nurses was in the dimension of usual activities. Nurses reported problems during usual activities in a higher percentage than physiotherapists.
The EQ-VAS positively correlated with the HPLP-II total score (p<0.001, rs=0.231), and several sub-scales: physical activity (p=0.001, rs=0.208), spiritual growth (p<0.001, rs=0.273), interpersonal relations (p=0.002, rs=0.189), and stress management (p=0.044, rs=0.127). Furthermore, it was negatively associated with age (p<0.001, rs=-0.244), BMI (p=0.044, rs=-0.127), and work experience (p=<0.001, rs=-0.243).
The median total physical activity which included domains of work, transport, domestic, garden, and leisure for the total sample was 207. 1±293. 5 MET-hours/week. Most physical activities were accumulated in the domain of work followed by domestic, and garden activities, and the least physical activity was accumulated in the domain of transport followed by leisure. Male respondents accumulated higher levels of physical activity in the work domain in comparison to females. This was also the case for the domain of leisure, and total levels of physical activity. Furthermore, male respondents accumulated higher levels of vigorous-intensity physical activity. Nurses accumulated higher levels of total physical activity than physiotherapists. Likewise, nurses accumulated higher levels of moderate-intensity physical activity and vigorous-intensity physical activity. Respondents working in community care reported higher levels of physical activity in the domain of transport in comparison with those working in a medical facility (Table 4).
There was a positive relationship between age, and work experience, and physical activity in domains of work (p=0.001, rs=0.207; p<0.001, rs=0.218), and domestic (p<0.001, rs=0.232; p<0.001, rs=0.233), and total levels of physical activity (p<0.001, rs=0.222; p<0.001, rs=0.238), moderate-intensity physical activity (p<0.001, rs=0.247; p<0.001, rs=0.262), and vigorous-intensity physical activity (p=0.006, rs=0.173; p=0.001, rs=0.204). Furthermore, BMI was associated with levels of physical activity in the work domain (p<0.001, rs=0.227), total levels of physical activity (p=0.010, rs=0.161), moderate-, and vigorous-intensity physical activity (p=0.016, rs=0.151; p=0.003, rs=0.185). Physical activity in the domain leisure was positively correlated with total HPLP-II score (p<0.001, rs=0.299), and several subscales: health responsibility (p=0.004, rs=0.181), physical activity (p<0.001, rs=0.445), nutrition (p=0.002, rs=0.194), and stress management (p=0.001, rs=0.209).
Levels of total physical activity were negatively correlated with HPLP-II sub-scale interpersonal relations (p=0.044, rs=-0.127). Walking positively correlated with total HPLP-II score (p=0.040, rs=0.129), and sub-scales for physical activity (p=0.026, rs=0.140), and nutrition (p=0.032, rs=0.135). Vigorous-intensity physical activity negatively correlated with HPLP-II sub-scale interpersonal relations (p=0.037, rs=-0.131), and sedentary activity negatively correlated with sub-scale nutrition (p=0.019, rs=-0.148). There was a positive relationship between EQ-VAS, and levels of physical activity in the domain of leisure (p=0.047, rs=0.125).
There was a negative relationship between working nights, and levels of physical activity in the domain of leisure (p=0.001, rpbi=-0.210), total physical activity (p<0.001, rpbi=-0.276), walking (P=0.007, rpbi=-0.169), moderate-intensity, and vigorous-intensity physical activity (p<0.001, rpbi=-0.248; p<0.001, rpbi=-0.242). Levels of total physical activity were also negatively correlated with heavy lifting at work (p<0.001, rpbi=-0.329), work in static or non-ergonomic positions (p<0.001, rpbi=-0.250), and prolonged standing at work (p=0.001, rpbi=-0.216). Physical activity in the domain of leisure was also negatively associated with prolonged standing at work (p=0.028, rpbi=-0.138). There was a negative relationship between levels of moderate-, and vigorous-intensity physical activity, and heavy lifting at work (p<0.001, rpbi=-0.222); p<0.001, rpbi=-0.349), work in static, and non-ergonomic positions (p=0.003, rpbi=-0.186; p<0.001, rpbi=-0.281), and prolonged standing at work (p<0.001, rpbi=-0.231; p=0.002, rpbi=-0.196). Furthermore, walking was negatively associated with heavy lifting at work (p=0.002, rpbi=-0.190).
Table 1) Results of participants' characteristics
Table 2) Results of HPLP-II (Mean±SD)
Table 3) Health-related quality of life, EQ-5D-5L (Numbers in parentheses are in percent)
Table 4) Results of physical activity, and sedentary behavior in metabolic equivalents-hours per week (MET-hours/week)
Discussion
Data on physical activity, and health-promoting behaviors of physiotherapists, and nurses in different work settings are limited. To our knowledge, this is the first study that investigates, and compares physiotherapists', and nurses' habits of physical activity, health-promoting behavior, and health-related quality of life, and relationships among them across different work settings, and conditions.
Adequate levels of physical activity including regular exercise, and healthy habits are an essential part of a healthy lifestyle. Healthcare workers, including physiotherapists, and nurses have a chance to actively promote a healthy lifestyle. However, in order to look credible in the eyes of their patients, they should do what they “preach”.
Adoption of health-promoting behaviors is a key factor in health promotion, and disease prevention, and these behaviors are expected from those who educate patients on a healthy lifestyle. Higher rates of work-related stress in healthcare jobs are associated with mental health problems, job dissatisfaction, and decreased levels of healthy lifestyle engagement [18]. Healthy behaviors can enhance the ability of healthcare workers to cope with job-related stress [19]. A recent study showed that healthcare workers adopt better nutrition, more physical activity, and greater health responsibility in comparison to other professions [16]. However, these differences were not found in other sub-scales of the HPLP-II like spiritual growth, interpersonal relations, and stress management.
Our total score on the HPLP-II questionnaire which measures health-promoting behaviors was 127 (average score 2. 4) with no differences by gender, profession, or work setting. This was slightly lower than the scores reported by Kurnat-Thoma et al. [15] where the average score was 2, 9, and Al-Qahtani [14] where it was 2.7. The highest scores were reported in the domains of interpersonal relationships, and spiritual growth, and the lowest score was in the domain of physical activity. This is similar to the results from studies performed on nurses in Saudi Arabia [14], and American nurses in community hospitals [15].
We also found differences between male, and female respondents, but only in the sub-scale health responsibility where females scored higher. This is under a previous study where female students scored higher in that domain in comparison to male students [20]. However, in this study, females also scored higher in the total HPLP-II score and sub-scales nutrition, interpersonal relations, and stress management, which was not the case in our study. Another study performed by Wei et al. [21] found that female respondents had higher scores on sub-scales health responsibility, interpersonal relations, and nutrition than males who scored better on sub-scale physical activity.
In our sample, there was an inverse relationship between age, the total HPLP-II score, and several sub-scales. This was also reported in a recent study performed on community hospital nurses [15]. The finding that the age of health professionals can negatively impact perceptions, and engagement in a healthy lifestyle is very important, and it warrants some concern, and need for action.
Although sub-scale physical activity had the lowest score among HPLP-II sub-scales in our sample, leisure-time physical activity, and walking were in a positive relationship with the total HPLP-II score, and several sub-scales. However, surprisingly, sub-scale interpersonal relationships were in an inverse relationship with the total level of physical activity, and vigorous-intensity physical activity.
There is a positive relationship between health-related quality of life and physical activity which was confirmed by previous studies [22]. While most of our respondents did not report any problems in the majority of the EQ-5D-5L domains, a relatively high percentage reported problems in domains of pain/discomfort, and anxiety, especially female respondents. This could be due to demand, and stressful job conditions in combination with domestic duties, and family obligations. The average score of self-rated health was 85 for the total sample and significantly lower in the subgroup of female respondents which scored 80 on average. Nurses reported more problems with usual activities than physiotherapists, probably due to more difficult working conditions which include heavy lifting, work in static, and non-ergonomic positions, and prolonged standing periods a greater percentage than physiotherapists.
The EQ-VAS positively correlated with the HPLP-II total score, and several sub-scales of HPLP-II: physical activity, spiritual growth, interpersonal relations, and stress management. However, the inverse relationship between age, and work experience could be due to difficult working conditions in healthcare, and burn-out. On the other hand, there was a positive relationship between EQ-VAS and leisure-time physical activity. A previous study also reported a positive relationship between health-related quality of life, and leisure-time physical activity [23].
The reported level of total physical activity in our sample was on average 207 MET-hours/week, which is equivalent to approximately 7 hours of moderate or 3. 5 hours of vigorous physical activity per day. This was considerably higher than the total physical activity among middle-aged employees in Croatia who scored 79 MET-hours/week on average [24]. This means that majority of our respondents exceeded current WHO guidelines which recommend 150 minutes of moderate-intensity aerobic physical activity or at least 75 minutes of vigorous-intensity aerobic activity per week [2]. Indeed, our sample exceeded even the guidelines for physical activity needed to gain additional health benefits which recommend at least 300 minutes of moderate-intensity or 150 minutes of vigorous-intensity physical activity per week. However, most of the physical activity was accumulated within the work domain, and only 18 MET-hours/week were accumulated in the domain of leisure, which is equivalent to approximately 0.6 hours of moderate-intensity or 0.3 hours of vigorous-intensity physical activity.
These results are similar to the study performed on Polish nurses, and midwives [25] where average levels of total physical activity were 262 MET-hours/week among those who work rotating night shifts, and 207 MET-hours/week among those who work only day shifts. Likewise, their levels of leisure-time physical activity were a bit lower than our results, ranging from 11.7 to 13. 2 MET-hours/week. Peplonska et al. [25] also reported lower levels of leisure-time physical activity among nurses and midwives working night shifts which we confirmed in our results not only for leisure-time physical activity, but also for total physical activity, walking, moderate-, and vigorous-intensity physical activity.
Other workplace characteristics which could be considered difficult working conditions like heavy lifting, working in static or non-ergonomic positions, or prolonged standing were also in inverse relationship with levels of physical activity. Another study performed on Danish female nurses also found a significantly lower average number of hours spent on sports activities (2.8 vs. 4.2) among nurses who worked after midnight in comparison to those who never work after midnight [26]. Jurakic et al. [24] found that leisure-time physical activity was not related to work characteristics among middle-aged employees, but another previous study has shown that stressful work increases the likelihood of physical inactivity in leisure time [27].
Interestingly, physiotherapists reported lower levels of total, moderate-, and vigorous-intensity physical activity than nurses. It was hypothesized that physiotherapists will score higher than nurses since they have extensive knowledge, and education regarding the importance of exercise, and physical activity, and their main role is to prescribe those to the patients. The inverse relationship between age and levels of physical activity was another surprising finding. This was contrary to the results of Hallal et al. [28], however, following the results obtained by Jurakic et al. [29] on a sample of the Croatian population where physical activity scores increased with advancing age.
A comparison of physical activity levels by gender revealed that men are considerably more active than women in work, and leisure domains, and men have higher scores for total, and vigorous-intensity physical activity. This is under some previous studies which reported the same [24, 30].
The strength of our study is the use of valid, and reliable questionnaires which allows the comparison of our results with other studies. The IPAQ-L questionnaire covers all important domains of physical activity, and it has proven validity and reliability. The HPLP-II and EQ-5D-5L are also well-known, valid, and reliable survey tools. Furthermore, this study is the first to investigate patterns of physical activity among physiotherapists, and nurses, and their relationship with health-promoting behaviors, and health-related quality of life. Considering that improvements in the adoption of healthy habits among healthcare workers could directly influence the adoption of healthy habits by their patients in a positive way, the results of this study could help to plan worksite interventions aimed at healthcare workers to adopt healthy habits and physical activity.
The main study limitations include cross-sectional nature and convenience sample which precluded establishing any causal relationships among the observed variables. Also, there is a possibility of self-report bias. Another limitation may apply to the study regarding its generalization to populations other than nurses, physiotherapists, and in other countries. Our study was conducted from September to January, so another limitation may arise from the assumption that the level of physical activity varied between autumn and winter. Due to low levels of leisure-time physical activity, and the positive relationship to a healthy lifestyle, and quality of life, it is recommended to take measures among healthcare workers to increase the levels of leisure-time physical activity.
Conclusion
The results demonstrated high levels of physical activity among nurses, and physiotherapists irrespective of their work setting, but relatively low levels of active transportation, and leisure-time physical activity. There is a positive relationship between leisure-time physical activity, health-related quality of life, and health-promoting behaviors. Further research should use objective methods of determining levels of physical activity to avoid over-, and under-reporting, and include other groups of healthcare professionals.
Acknowledgments: The authors are grateful to all the participants for their involvement in the study.
Ethical Permissions: The study was approved by the Ethics Committee of Community Care Institution Jadranka Pluzaric, Osijek, Croatia, and the Ethics Committee of County General Hospital Vinkovci, Vinkovci, Croatia.
Conflicts of Interests: The authors declared no potential conflicts of interest for the research, authorship, and/or publication of this article.
Authors' Contribution: Sklempe Kokic I (First Author), Main Researcher/Statistical Analyst (30%); Barusic, Z (Second Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%); Crnkovic Knezevic M (Third Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%); Benko Mestrovic S (Fourth Author), Introduction Writer/Discussion Writer/Methodologist (15%); Duvnjak I (Fifth Author), Introduction Writer/Methodologist/Discussion Writer (15%)
Funding/Support: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Article Type: Descriptive & Survey |
Subject:
Healthy Life Style
Received: 2022/05/9 | Accepted: 2022/07/21 | Published: 2022/08/10
Received: 2022/05/9 | Accepted: 2022/07/21 | Published: 2022/08/10
References
1. World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva: World Health Organization Press; 2009. [Link]
2. World Health Organization. Global recommendations on physical activity for health. Geneva: World Health Organization Press; 2010. [Link]
3. 2018 Physical Activity Guidelines Advisory Committee. Physical activity guidelines advisory committee scientific report. Washington: U. S. Department of Health and Human Services; 2018. [Link]
4. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126-31. [Link]
5. Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: development and psychometric characteristics. Nurs Res. 1987;36(2):76-81. [Link] [DOI:10.1097/00006199-198703000-00002]
6. World Health Organization. Global action plan on physical activity 2018-2030: more active people for a healthier world. Geneva: World Health Organization Press; 2018. [Link]
7. Milosevic M, Golubic R, Mustajbegovic J, Doko Jelinic J, Janev HolcerN, Kern J. Regional pattern of physical inactivity in Croatia. Coll Antropol. 2009;33 suppl 1:35-8. [Link]
8. World Health Organization. WHO Global Plan of Action on Workers' Health (2008-2017): Baseline for Implementation Global Country Survey 2008/2009Executive Summary and Survey Findings. Geneva: World Health Organization Press2013 [cited 2022 Jun 1]. Available from: [Link]
9. Black B, Marcoux BC, Stiller C, Qu X, Gellish R. Personal health behaviors and role-modeling attitudes of physical therapists and physical therapist students: A cross-sectional study. Phys Ther. 2012;92(11):1419-36. [Link] [DOI:10.2522/ptj.20110037]
10. Chevan J, Haskvitz EM. Do as I do: exercise habits of physical therapists, physical therapist assistants, and student physical therapists. Phys Ther. 2010;90(5):726-34. [Link] [DOI:10.2522/ptj.20090112]
11. Craig CL, Marshal, AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sport Exerc. 2003;35(8):1381-95. [Link] [DOI:10.1249/01.MSS.0000078924.61453.FB]
12. Pedisic Z, Jurakic D, Rakovac M, Hodak D, Dizdar D. Reliability of the croatian long version of the international physical activity questionnaire. Kinesiology. 2011;43:185-91. [Sažetak] [Link]
13. IPAQ Group. Guidelines for the data processing and analysis of the international physical activity questionnaire: short and long forms; 2005 [cited 2022 Jun 1]. Available from: https://sites.google.com/site/theipaq/scoring-protocol [Link]
14. Al-Qahtani MF. Health-promoting lifestyle beaviors among nurses in private hospitals in Al-Khobar, Saudi Arabia. J Egypt Public Health Assoc. 2015;90(1):29-34. [Link] [DOI:10.1097/01.EPX.0000461325.97703.8a]
15. Kurnat-Thoma E, El-Banna M, Oakcrum M, Tyroler J. Nurses' health promoting lifestyle behaviours in a community hospital. Appl Nurs Res. 2017;35:77-81. [Link] [DOI:10.1016/j.apnr.2017.02.012]
16. Profis M, Simon-Tuval T. The influence of healthcare workers' occupation on health promoting lifestyle profile. Ind Health. 2016;54(5):439-47. [Link] [DOI:10.2486/indhealth.2015-0187]
17. Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P, Parkin D et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-36. [Link] [DOI:10.1007/s11136-011-9903-x]
18. Melnyk B, Hrabe DP, Szalacha LA. Relationship among work stress, job satisfaction, mental health, and healthy lifestyle behaviors among new graduate nurses attending the nurse athlete program: a call to action for nursing leaders. Nurs Adm Q. 2013;37(4):278-85. [Link] [DOI:10.1097/NAQ.0b013e3182a2f963]
19. Wright K. Alleviating stress in the workplace: advice for nurses. Nurs Stand. 2014;28(20):37-42. [Link] [DOI:10.7748/ns2014.01.28.20.37.e8391]
20. Can G, Ozdilli K, Ero, O, Unsar S, Tulek Z, Savaser S et al. Comparison of the health-promoting lifestyles of nursing and non-nursing students in Istanbul, Turkey. Nurs Health Sci. 2008;10(4):273-80. [Link] [DOI:10.1111/j.1442-2018.2008.00405.x]
21. Wei CN, Harada K, Ueda K, Fukumoto K, Minamoto K, Ueda A.(2012). Assessment of health-promoting lifestyle profile in Japanese university students. Environ Health Prev Med. 2012;17(3):222-7. [Link] [DOI:10.1007/s12199-011-0244-8]
22. Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: a systematic review. Prev Med. 2007;45(6):401-15. [Link] [DOI:10.1016/j.ypmed.2007.07.017]
23. Vuillemin A, Boini S, Bertrais S, Tessier S, Oppert JM, Hercberg S, et al. Leisure time physical activity and health-related quality of life. Prev Med. 2005;41(2):562-9. [Link] [DOI:10.1016/j.ypmed.2005.01.006]
24. Jurakic D, Golubic A, Pedisic Z, Pori M. Patterns and correlates of physical activity among middle-aged employees: a population-based, cross-sectional study. Int J Occup Med Environ Health. 2014;27(3):487-97. [Link] [DOI:10.2478/s13382-014-0282-8]
25. Peplonska B, Bukowska A, Sobala W. Rotating night shift work and physical activity of nurses and midwives in the cross-sectional study in Lodz, Poland. Chronobio Int. 2014;31(10):1152-9. [Link] [DOI:10.3109/07420528.2014.957296]
26. Hansen J, Stevens RG. Case-control study of shift-work and breast cancer risk in Danish nurses: impact of shift systems. Eur J Cancer. 2012;48(11):1722-9. [Link] [DOI:10.1016/j.ejca.2011.07.005]
27. Fransson EI, Heikkilä K, Nyberg ST, Zins M, Westerlund H, Westerholm P, et al. Job strain as a risk factor for leisure-time physical inactivity: an individual-participant meta-analysis of up to 170,000 men and women: The IPD-Work Consortium. Am J Epidemiol. 2012;176(12):1078-89. [Link] [DOI:10.1093/aje/kws336]
28. Hallal PC, Victora CG, Wells JC, Lima RC. Physical inactivity: prevalence and associated variables in Brazilian adults. Med Sci Sport Exerc. 2003;35(11):1894-900. [Link] [DOI:10.1249/01.MSS.0000093615.33774.0E]
29. Jurakic D, Pedisic Z, Andrijasevic M. Physical activity of Croatian population: cross-sectional study using international physical activity questionnaire. Croat Med J. 2009;50(2):165-73. [Link] [DOI:10.3325/cmj.2009.50.165]
30. Kim HK, Kim MJ, Park CG, Kim HO. Gender differences in physical activity and its determinants in rural adults in Korea. J Clin Nurs. 2010;19(5-6):876-83. [Link] [DOI:10.1111/j.1365-2702.2009.03054.x]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |