



Volume 10, Issue 4 (2022)
Health Educ Health Promot 2022, 10(4): 695-701 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Al-Khafaji A. Microbial Contamination from Mobile Phones of Social Groups at Kufa Technical Institute and Efficiency of Two Disinfections to its Reduction. Health Educ Health Promot 2022; 10 (4) :695-701
URL: http://hehp.modares.ac.ir/article-5-59557-en.html
URL: http://hehp.modares.ac.ir/article-5-59557-en.html
Kufa Technical Institute, Alfurat Alawsat Technical University, 31001 Alkufa Alnajaf, Iraq
Keywords: Mobile Phones [MeSH], Equipment Contamination [MeSH], Aloe vera [MeSH], Disinfectant [MeSH]
Full-Text [PDF 961 kb]
(3426 Downloads)
| Abstract (HTML) (1792 Views)
Full-Text: (511 Views)
Introduction
Since human skin is in constant contact with microbes, it is susceptible to colonization by specific bacteria population. Almost each layer of adult human epidermis is invaded by a variety of microflora and sometimes contaminated with harmful bacteria. During a phone conversation, the mobile phone is in close proximity to the infectious human body regions such as the mouth, nose, and ears [1]. Microbiological hygiene standards are required to maintain a person's health. People frequently believe that microbes are isolated in research labs, institutions, and health centers, creating an erroneous sense of security in other places. Inadequate knowledge of microbial origins may lead to health concerns. Indeed, hand-to-hand touch or contact with other objects transmits around 80% of infections [2].
Mobile phones, sometimes known as "phones", have evolved into one of the most essential tools for both social and professional life [3]. The use of mobile communication technology in healthcare and higher education is increasing [4]. Every day, billions of people use mobile phones (both keypad and smart phone devices), which have become ingrained in modern society. Mobile phone adoption in the community increased dramatically from 10 to 60% between 2011 and 2018 and is predicted to reach 79% by 2025 [5]. Mobile phones are rarely disinfected and cumbersome to clean. As a result, these devices may become contaminated with a variety of bacterial organisms [1].
Zhao et al. studied the relationships between fomite characteristics and human behaviors that affect transmission routes using an Environmental Infection Transmission System (EITS) model. According to the study, tables and benches in commonly touched public places have the highest potential for transmission. The study found that every interior surface of an aircraft, including tray tables, armrests, seat covers, door knobs, and toilet flush buttons, acts as a biothreat source, harboring a variety of potentially dangerous microorganisms, including viruses [6].
The constant use of mobile phones by healthcare workers (HCWs) and the lack of disinfection make them possible routes for transmission of bacterial pathogens, including multi-drug-resistant organisms [7]. Additionally, there are no restrictions on the use of mobile devices in hospitals and the majority of HCWs do not regularly disinfect their mobile devices [8]. Infectious diseases can spread by fomite-mediated transmission in both public and medical settings [9]. Several studies have been conducted to quantify numerous microbial groups in mobile phones, including fungal species, aerobic mesophiles, Enterobacteriaceae coliforms [10] and E. coli. Identifying microbial species may help determine whether mobile phones may operate as reservoirs for microorganisms such as intestinal bacteria, especially when populations of pathogenic and opportunistic microbes are less than extremely low levels. Microbial populations in mobile phones may vary in response to their use in different situations and regions. Regular handling, along with the thermal conduction by the cell phone, creates an ideal habitat for the growth of various bacteria that are naturally present on our skin and in our environment. Due to the frequent interaction of the human epidermis with environmental pathogens, it is prone to colonization by specific microbial species. Given the widespread use and benefits of mobile phones, it is quite simple to avoid the health risks associated with them; this is particularly true given that many users may be concerned about personal hygiene and the number of individuals who may share a phone. This frequent handling by several users exposes the phone to a variety of pathogens, making it an excellent carrier for bacteria that inhabit every square inch of the phone [11].
The aim of this study was to evaluate bacterial contamination and identify all bacterial isolates of mobile phones related to social groups in Kufa Technical Institute and to determine the efficiency of two disinfectants prepared on bacterial species.
Materials and Methods
Study context: Fifty-one swab samples of mobile phones were randomly collected from different people in the social groups of Kufa Technical Institute, including university lecturers, administration staff, restaurant workers, garden workers, and students. All participants in the study completed a questionnaire about mobile phone properties, usage patterns, mobile phone technical parameters, and device cleaning and disinfection practices.
Inoculation of swab samples: Wet swabs were transferred to the microbiological laboratory of the Community Health Department of Kufa Technical Institute, then were cultured on selective and enrichment media and incubated at 37°C for 24 hours.
Isolation and identification of bacterial species: Pure colonies of bacterial isolates appeared in selective media were identified using gram staining and various biochemical tests [12].
Identity confirmation by VITEK-2 Compact System: The kit was applied according to the manufacturer's guidelines. This kit has recently been used for rapid identification of G+ve and G-ve bacteria.
Preparation of disinfectant A: This disinfectant was prepared by adding 20 ml of artificial vinegar (water, 5% acetic acid) to 20 ml of lemon juice, then mixed with a vortex and stored at 37°C until use.
Preparation of disinfectant B: This disinfectant was prepared by adding 20 ml of fresh Aloe vera gel taken from the leaves to 20 ml of lemon juice and 20 grams of NaCl. After filtering the contents through Whatman No. 1 filter paper, it was stored at room temperature until use.
Agar well diffusion technique: Wells with a diameter of 5 mm were cut and swabbed on sterile nutrient agar plates with organism's overnight broth culture. Each of the two wells was filled with about 0.1 ml of disinfectant 1, disinfectant 2 and ethanol alcohol-70% and incubated at 37°C. Following an incubation period (24 hours), the antibacterial activity of the two disinfectants was determined using zones of inhibition (mm). The antagonistic activity of three disinfectants against test organisms was examined.
The inhibition activity of two disinfectant on tested bacteria: The efficiency of two disinfectants was evaluated by determining microbial killing using a spectrophotometer. Microbial suspension of bacteria was prepared after culturing on Nutrient broth at 37°C for 24 hours. 1.5 ml of bacterial suspension with a concentration of 1.5 x 108 cells/ml was prepared with 1.5 ml of disinfectant from the previous one. The tubes were incubated for different time periods (10 min, 1 h, 2 h, 4 h, 8 h, 24 h) at 37°C. The optical density was calculated using a spectrophotometer, taking into account the reading of the results in each period on a wavelength of 600 nanometers, as well as using N. broth medium to zero the device before reading the result.
Statistical analysis: Data were statistically analyzed using appropriate techniques and methods, including SPSS 24 software and one-way analysis of variance at the level of p-value<0.05.
Findings
Table 1 presents the frequency distribution of social group and mobile phone characteristics and the conditions of its use.
All samples were contaminated with bacterial species, so the rate of bacterial contamination was 100%. Ten bacterial species were isolated and identified from mobile phones, which included Staphylococcus aureus in the highest percentage (49%), Staphylococcus epidermidis (12%), Pseudomonas aeruginosa (11%), Staphylococcus haemolyticus (6%), Escherichia vulner (6%), Escherichia coli (4%), Klebsiella pneumoniae (4%), and Bacillus sp (4%). The lowest percentage was related of Pantoea spp and Cronobacter C sakazakii with 2% (Figure 1).
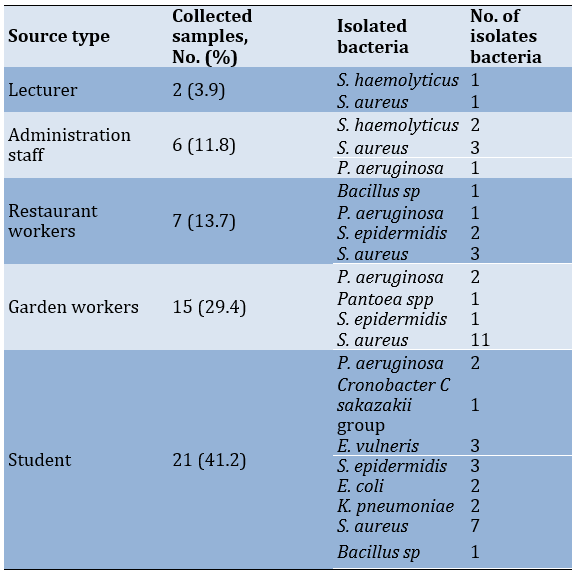
Table 2 shows the frequency distribution of the different types of bacteria isolated from mobile phones, where 23 isolates of Staphylococcus aureus were the dominant organism from mobile phones with any type of source.
Table 1) Frequency distribution of social group and mobile phone characteristics and conditions of its use (n=51)
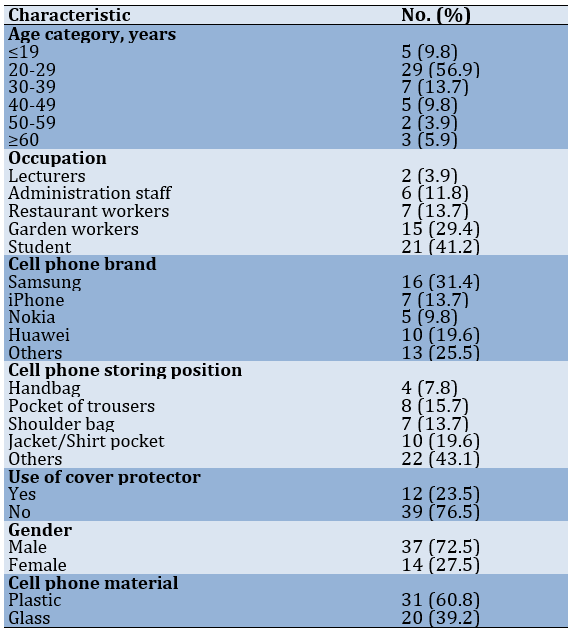
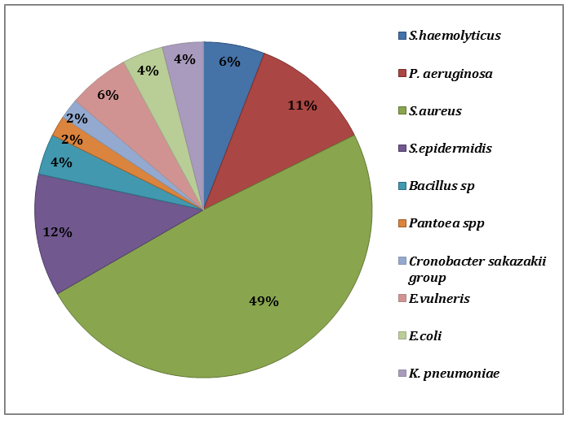
Figure 1) Percentage of bacterial isolates from mobile phones
Table 2) Frequency distribution of different types of bacteria isolated from mobile phones of social groups
Disinfectant 1 had a greater effect on bacterial inhibition compared to disinfectant 2 (p<0.001). There was a significant difference between the two disinfectants for S. aureus, S.epidermidis, E.coli and K. pneumoniae at all times (p<0.001). However, a significant difference was observed between disinfectant 1 and 2 for the inhibition of E. vulneris, Bacillus sp, Cronobacter C sakazakii group, P. aeruginosa, S. haemolyticus, and Pantoea spp, at all times (p<0.001), except 10 minutes (Table 3).
Since human skin is in constant contact with microbes, it is susceptible to colonization by specific bacteria population. Almost each layer of adult human epidermis is invaded by a variety of microflora and sometimes contaminated with harmful bacteria. During a phone conversation, the mobile phone is in close proximity to the infectious human body regions such as the mouth, nose, and ears [1]. Microbiological hygiene standards are required to maintain a person's health. People frequently believe that microbes are isolated in research labs, institutions, and health centers, creating an erroneous sense of security in other places. Inadequate knowledge of microbial origins may lead to health concerns. Indeed, hand-to-hand touch or contact with other objects transmits around 80% of infections [2].
Mobile phones, sometimes known as "phones", have evolved into one of the most essential tools for both social and professional life [3]. The use of mobile communication technology in healthcare and higher education is increasing [4]. Every day, billions of people use mobile phones (both keypad and smart phone devices), which have become ingrained in modern society. Mobile phone adoption in the community increased dramatically from 10 to 60% between 2011 and 2018 and is predicted to reach 79% by 2025 [5]. Mobile phones are rarely disinfected and cumbersome to clean. As a result, these devices may become contaminated with a variety of bacterial organisms [1].
Zhao et al. studied the relationships between fomite characteristics and human behaviors that affect transmission routes using an Environmental Infection Transmission System (EITS) model. According to the study, tables and benches in commonly touched public places have the highest potential for transmission. The study found that every interior surface of an aircraft, including tray tables, armrests, seat covers, door knobs, and toilet flush buttons, acts as a biothreat source, harboring a variety of potentially dangerous microorganisms, including viruses [6].
The constant use of mobile phones by healthcare workers (HCWs) and the lack of disinfection make them possible routes for transmission of bacterial pathogens, including multi-drug-resistant organisms [7]. Additionally, there are no restrictions on the use of mobile devices in hospitals and the majority of HCWs do not regularly disinfect their mobile devices [8]. Infectious diseases can spread by fomite-mediated transmission in both public and medical settings [9]. Several studies have been conducted to quantify numerous microbial groups in mobile phones, including fungal species, aerobic mesophiles, Enterobacteriaceae coliforms [10] and E. coli. Identifying microbial species may help determine whether mobile phones may operate as reservoirs for microorganisms such as intestinal bacteria, especially when populations of pathogenic and opportunistic microbes are less than extremely low levels. Microbial populations in mobile phones may vary in response to their use in different situations and regions. Regular handling, along with the thermal conduction by the cell phone, creates an ideal habitat for the growth of various bacteria that are naturally present on our skin and in our environment. Due to the frequent interaction of the human epidermis with environmental pathogens, it is prone to colonization by specific microbial species. Given the widespread use and benefits of mobile phones, it is quite simple to avoid the health risks associated with them; this is particularly true given that many users may be concerned about personal hygiene and the number of individuals who may share a phone. This frequent handling by several users exposes the phone to a variety of pathogens, making it an excellent carrier for bacteria that inhabit every square inch of the phone [11].
The aim of this study was to evaluate bacterial contamination and identify all bacterial isolates of mobile phones related to social groups in Kufa Technical Institute and to determine the efficiency of two disinfectants prepared on bacterial species.
Materials and Methods
Study context: Fifty-one swab samples of mobile phones were randomly collected from different people in the social groups of Kufa Technical Institute, including university lecturers, administration staff, restaurant workers, garden workers, and students. All participants in the study completed a questionnaire about mobile phone properties, usage patterns, mobile phone technical parameters, and device cleaning and disinfection practices.
Inoculation of swab samples: Wet swabs were transferred to the microbiological laboratory of the Community Health Department of Kufa Technical Institute, then were cultured on selective and enrichment media and incubated at 37°C for 24 hours.
Isolation and identification of bacterial species: Pure colonies of bacterial isolates appeared in selective media were identified using gram staining and various biochemical tests [12].
Identity confirmation by VITEK-2 Compact System: The kit was applied according to the manufacturer's guidelines. This kit has recently been used for rapid identification of G+ve and G-ve bacteria.
Preparation of disinfectant A: This disinfectant was prepared by adding 20 ml of artificial vinegar (water, 5% acetic acid) to 20 ml of lemon juice, then mixed with a vortex and stored at 37°C until use.
Preparation of disinfectant B: This disinfectant was prepared by adding 20 ml of fresh Aloe vera gel taken from the leaves to 20 ml of lemon juice and 20 grams of NaCl. After filtering the contents through Whatman No. 1 filter paper, it was stored at room temperature until use.
Agar well diffusion technique: Wells with a diameter of 5 mm were cut and swabbed on sterile nutrient agar plates with organism's overnight broth culture. Each of the two wells was filled with about 0.1 ml of disinfectant 1, disinfectant 2 and ethanol alcohol-70% and incubated at 37°C. Following an incubation period (24 hours), the antibacterial activity of the two disinfectants was determined using zones of inhibition (mm). The antagonistic activity of three disinfectants against test organisms was examined.
The inhibition activity of two disinfectant on tested bacteria: The efficiency of two disinfectants was evaluated by determining microbial killing using a spectrophotometer. Microbial suspension of bacteria was prepared after culturing on Nutrient broth at 37°C for 24 hours. 1.5 ml of bacterial suspension with a concentration of 1.5 x 108 cells/ml was prepared with 1.5 ml of disinfectant from the previous one. The tubes were incubated for different time periods (10 min, 1 h, 2 h, 4 h, 8 h, 24 h) at 37°C. The optical density was calculated using a spectrophotometer, taking into account the reading of the results in each period on a wavelength of 600 nanometers, as well as using N. broth medium to zero the device before reading the result.
Statistical analysis: Data were statistically analyzed using appropriate techniques and methods, including SPSS 24 software and one-way analysis of variance at the level of p-value<0.05.
Findings
Table 1 presents the frequency distribution of social group and mobile phone characteristics and the conditions of its use.
All samples were contaminated with bacterial species, so the rate of bacterial contamination was 100%. Ten bacterial species were isolated and identified from mobile phones, which included Staphylococcus aureus in the highest percentage (49%), Staphylococcus epidermidis (12%), Pseudomonas aeruginosa (11%), Staphylococcus haemolyticus (6%), Escherichia vulner (6%), Escherichia coli (4%), Klebsiella pneumoniae (4%), and Bacillus sp (4%). The lowest percentage was related of Pantoea spp and Cronobacter C sakazakii with 2% (Figure 1).
Table 2 shows the frequency distribution of the different types of bacteria isolated from mobile phones, where 23 isolates of Staphylococcus aureus were the dominant organism from mobile phones with any type of source.
Table 1) Frequency distribution of social group and mobile phone characteristics and conditions of its use (n=51)
Figure 1) Percentage of bacterial isolates from mobile phones
Table 2) Frequency distribution of different types of bacteria isolated from mobile phones of social groups
Disinfectant 1 had a greater effect on bacterial inhibition compared to disinfectant 2 (p<0.001). There was a significant difference between the two disinfectants for S. aureus, S.epidermidis, E.coli and K. pneumoniae at all times (p<0.001). However, a significant difference was observed between disinfectant 1 and 2 for the inhibition of E. vulneris, Bacillus sp, Cronobacter C sakazakii group, P. aeruginosa, S. haemolyticus, and Pantoea spp, at all times (p<0.001), except 10 minutes (Table 3).
Table 3) Bacterial contamination of mobile phones before and after using disinfectants at different times (10 min, 1, 2, 4, 8, 24 hours)
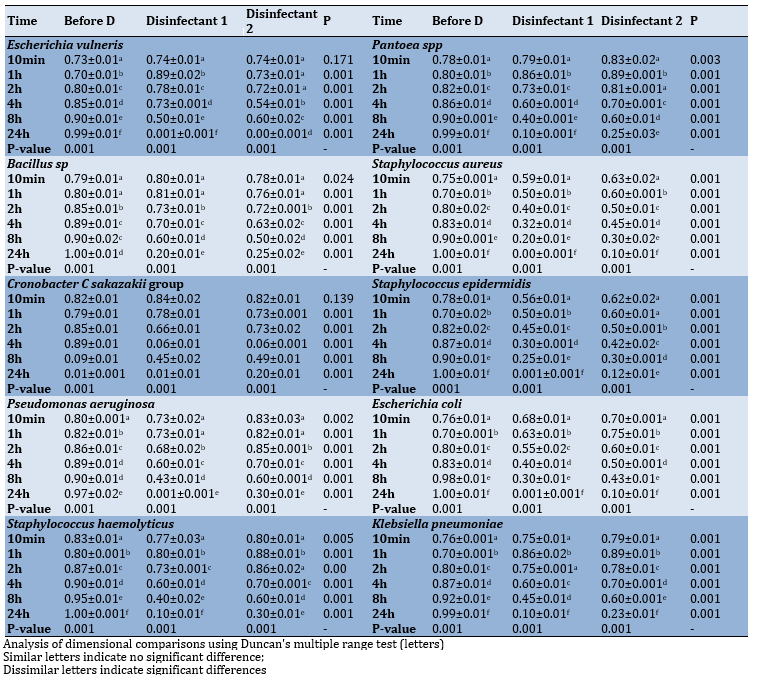
Figure 2 shows that the bacterial inhibition zone caused by disinfectant 1 is higher than that of disinfectant 2, while ethanol alcohol-70% has no inhibition zone
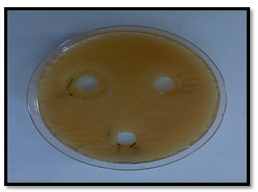
Figure 2) Inhibition zone of Staphylococcus aureus resulted from two disinfectant, and ethanol alcohol-70%. A: Disinfectant 1, B: Disinfectant 2, C: Ethanol alcohol-70%
Discussion
The significant incidence of microbial agents identified from mobile phones has been related to unsanitary and unhygienic behaviors. In general, all 51 mobile phones sampled were completely contaminated with a variety of bacteria. As in healthcare settings, mobile devices in educational institutions may act as a vehicle for microbial transmission and may be contaminated with potentially harmful microbes, which are often components of the human microbiota. Undergraduate students often utilize their mobile phones for academic, recreational, and/or communication purposes regardless of their location. Our data showed that health science students use mobile phones in a microbiology laboratory. Cell phones may act as a storage and source of pathogenic and non-pathogenic organisms in certain environments and increase cross-contamination [13]. A recent study examined both phone surfaces and found no difference in the incidence of bacterial contamination between the two surfaces [14]. This finding is consistent with other studies [15].
According to several studies, women who carry their smartphones in bags are associated with higher bacterial levels, and the heat generated by the phone and the inner surface of the bags may promote the spread of bacteria [16]. As a consequence, it was determined that the female gender is a possible risk factor for bacterial contamination of the phone. Second, after covering (or the inner part of the cover), users clean the back surface of the phone less than the touch screen, which means that viruses remain on the surface. Third, regular cleaning of smartphones may help limit or eliminate bacterial growth on smartphone surfaces. However, all of them have been demonstrated to be associated with bacterial contamination of the posterior surface. Bacterial infections are increasingly spreading in humans as community infections [17].
The study shows that smartphones have a positive effect on university students' academic performance; previous studies have shown similar results [18-20].
According to this study, all mobile phones used by medical workers were contaminated with microorganisms, which is consistent with Chaman et al.'s study [21]. These studies mainly focused on mobile phones with conventional keypads. However, limited studies have concentrated on smartphones, claiming that 20.9–99.2% of them are contaminated in healthcare centers [22, 23]. These bacteria might have entered the phone through the skin or via hand to hand contact. As previously mentioned, these organisms are part of the normal microflora present on the skin [24].
Microorganisms were found on two commonly used household items: cell phones and computer keyboards. Bacteria were found on 92% of mobile devices and 96% of keyboards, showing an ecosystem rich in gram-negative and gram-positive bacteria, as well as harmful and non-pathogenic bacteria. It was shown that 92% of the mobile phones studied were microbiologically contaminated, and Staphylococcus epidermidis was the most common bacteria identified. These bacteria as epiphytes and commensal bacteria may be found in the physiological microbiota of the skin and mucous membranes. Pal et al. found that coagulase-deficient staphylococci were the most common bacteria, accounting for roughly 81% of the total [25]. Based on the findings of this study, which is consistent with our findings, bacteria isolated and identified from mobile phones are the cause of disease in humans.
In the present study, Staphylococcus aureus was the most prevalent bacterial species (49%) that was isolated and identified from mobile phones. According to numerous studies, Staphylococcus aureus is the most common bacteria isolated from personal mobile phones, more than any other bacterial infection. This is a natural result because this bacterium spreads more on the human skin than any other bacterial infection, and it is one of the most bacteria that comes into contact with the surface of the phone screen [26].
The current investigation discovered that Staphylococcus aureus is the most prevalent microbe identified; this bacterium is a significant pathogen that may be transmitted to the general population through mobile phones. This observation is consistent with the findings of other studies [27]. Another study showed that the frequency of E. coli detected from mobile phones was 4%, which is consistent with our findings [28]. The detection of gram-negative bacilli, which are a type of coliform bacteria, indicated that the phone was contaminated with feces. Bacilli are known as decomposing bacteria. When food is prepared or eaten with contaminated hands, food decomposition and contamination increases almost dramatically.
Ulger et al. [13] and Soto et al. [29] revealed the presence of various bacteria on cell phones and reported that contamination occurs mostly through the use of hands, bags, purses, and pockets, as well as through the environment and food residue. Increasing heat and humidity in the phone stimulates microbial development and the formation of biofilm on the surface of the device. The high amount of bacteria recovered from commercial phones in this research may be due to repeated use of mobile phones and exposure to ambient microbes on the hands and skin of users. This is in accordance with previous research [30]. Frequent cleaning of cell phones with disinfectant detergents or hand sanitizers as well as frequent hand washing have been suggested to reduce transmission of microbes [31]. The ability of cell phones to transmit pathogens may be minimized by following proper cleaning and disinfection procedures [32].
Simple control techniques are critical to prevent device infection. Cleaning phones and PCs with alcohol-70% may help reduce the bacterial load [33]. This finding is in consistent with other studies [34]. It was shown that gram-positive bacteria are more sensitive to Aloe vera gel extract than gram-negative bacteria. As found in this study, the ethanolic extract of A. vera gel acts as an antibacterial against pathogens [35]. It was also showed that the inner gel of A. vera significantly reduces that the bacterial biomass due to antibiofilm effect, which is in agreement with the results of Cataldi et al. [36]. Verran performed a simple study in the United Kingdom, cleaning the phone with antimicrobial wipes and comparing the number of colonies present before and after cleaning [37]. This finding is consistent with other studies using chlorhexidine digluconate and triclosan to reduce microbial contamination [38].
Considering the results of the present study, people should use personal hygiene methods such as washing hands before and after handling food and decontamination of phones to prevent bacterial diseases. In the present study, a decrease in bacterial contamination was observed after using disinfectants (1 and 2) on the surface of mobile phones. As a result, it is recommended that mobile phones be sterilized once a week with suitable disinfectants and not used in crowded places and frequent hand washing promoted as a way to prevent disease transmission.
The following are also recommended:
1. Conducting a sensitivity test for bacteria isolated from mobile phone to find out the extent of their contamination with antibiotic-resistant isolates
2. Conducting an extensive study on the presence of other microorganisms on mobile phone
3. Avoid giving mobile phone to children at young ages because the young child lick them, which poses a health risk to him.
5. We must be careful not to place our mobile devices in contaminated places, such as bathrooms, laboratories, etc., to avoid contamination with pathogenic bacteria.
Conclusion
Bacteria colonize cell phones in social groups, and contaminated phones transmit pathogens that can cause serious illnesses. Some of these bacteria are toxic and contribute to illness and death in humans. Using disinfectants reduces bacterial contamination on the surface of the mobile phone.
Acknowledgements: We are grateful to the Kufa Technical Institute, Al-Furat Al-Awsat Technical University for allowing us to conduct this study.
Ethical Permission: This study was approved by Kufa Technical Institute, Alfurat Alawsat Technical University according to the Declaration of Helsinki. All participants signed a written informed consent form. Also, all participants approved the use of their data in the current study.
Conflict of Interests: The authors have no conflicts of interest to declare.
Funding: There was no financial source.
Figure 2 shows that the bacterial inhibition zone caused by disinfectant 1 is higher than that of disinfectant 2, while ethanol alcohol-70% has no inhibition zone
Figure 2) Inhibition zone of Staphylococcus aureus resulted from two disinfectant, and ethanol alcohol-70%. A: Disinfectant 1, B: Disinfectant 2, C: Ethanol alcohol-70%
Discussion
The significant incidence of microbial agents identified from mobile phones has been related to unsanitary and unhygienic behaviors. In general, all 51 mobile phones sampled were completely contaminated with a variety of bacteria. As in healthcare settings, mobile devices in educational institutions may act as a vehicle for microbial transmission and may be contaminated with potentially harmful microbes, which are often components of the human microbiota. Undergraduate students often utilize their mobile phones for academic, recreational, and/or communication purposes regardless of their location. Our data showed that health science students use mobile phones in a microbiology laboratory. Cell phones may act as a storage and source of pathogenic and non-pathogenic organisms in certain environments and increase cross-contamination [13]. A recent study examined both phone surfaces and found no difference in the incidence of bacterial contamination between the two surfaces [14]. This finding is consistent with other studies [15].
According to several studies, women who carry their smartphones in bags are associated with higher bacterial levels, and the heat generated by the phone and the inner surface of the bags may promote the spread of bacteria [16]. As a consequence, it was determined that the female gender is a possible risk factor for bacterial contamination of the phone. Second, after covering (or the inner part of the cover), users clean the back surface of the phone less than the touch screen, which means that viruses remain on the surface. Third, regular cleaning of smartphones may help limit or eliminate bacterial growth on smartphone surfaces. However, all of them have been demonstrated to be associated with bacterial contamination of the posterior surface. Bacterial infections are increasingly spreading in humans as community infections [17].
The study shows that smartphones have a positive effect on university students' academic performance; previous studies have shown similar results [18-20].
According to this study, all mobile phones used by medical workers were contaminated with microorganisms, which is consistent with Chaman et al.'s study [21]. These studies mainly focused on mobile phones with conventional keypads. However, limited studies have concentrated on smartphones, claiming that 20.9–99.2% of them are contaminated in healthcare centers [22, 23]. These bacteria might have entered the phone through the skin or via hand to hand contact. As previously mentioned, these organisms are part of the normal microflora present on the skin [24].
Microorganisms were found on two commonly used household items: cell phones and computer keyboards. Bacteria were found on 92% of mobile devices and 96% of keyboards, showing an ecosystem rich in gram-negative and gram-positive bacteria, as well as harmful and non-pathogenic bacteria. It was shown that 92% of the mobile phones studied were microbiologically contaminated, and Staphylococcus epidermidis was the most common bacteria identified. These bacteria as epiphytes and commensal bacteria may be found in the physiological microbiota of the skin and mucous membranes. Pal et al. found that coagulase-deficient staphylococci were the most common bacteria, accounting for roughly 81% of the total [25]. Based on the findings of this study, which is consistent with our findings, bacteria isolated and identified from mobile phones are the cause of disease in humans.
In the present study, Staphylococcus aureus was the most prevalent bacterial species (49%) that was isolated and identified from mobile phones. According to numerous studies, Staphylococcus aureus is the most common bacteria isolated from personal mobile phones, more than any other bacterial infection. This is a natural result because this bacterium spreads more on the human skin than any other bacterial infection, and it is one of the most bacteria that comes into contact with the surface of the phone screen [26].
The current investigation discovered that Staphylococcus aureus is the most prevalent microbe identified; this bacterium is a significant pathogen that may be transmitted to the general population through mobile phones. This observation is consistent with the findings of other studies [27]. Another study showed that the frequency of E. coli detected from mobile phones was 4%, which is consistent with our findings [28]. The detection of gram-negative bacilli, which are a type of coliform bacteria, indicated that the phone was contaminated with feces. Bacilli are known as decomposing bacteria. When food is prepared or eaten with contaminated hands, food decomposition and contamination increases almost dramatically.
Ulger et al. [13] and Soto et al. [29] revealed the presence of various bacteria on cell phones and reported that contamination occurs mostly through the use of hands, bags, purses, and pockets, as well as through the environment and food residue. Increasing heat and humidity in the phone stimulates microbial development and the formation of biofilm on the surface of the device. The high amount of bacteria recovered from commercial phones in this research may be due to repeated use of mobile phones and exposure to ambient microbes on the hands and skin of users. This is in accordance with previous research [30]. Frequent cleaning of cell phones with disinfectant detergents or hand sanitizers as well as frequent hand washing have been suggested to reduce transmission of microbes [31]. The ability of cell phones to transmit pathogens may be minimized by following proper cleaning and disinfection procedures [32].
Simple control techniques are critical to prevent device infection. Cleaning phones and PCs with alcohol-70% may help reduce the bacterial load [33]. This finding is in consistent with other studies [34]. It was shown that gram-positive bacteria are more sensitive to Aloe vera gel extract than gram-negative bacteria. As found in this study, the ethanolic extract of A. vera gel acts as an antibacterial against pathogens [35]. It was also showed that the inner gel of A. vera significantly reduces that the bacterial biomass due to antibiofilm effect, which is in agreement with the results of Cataldi et al. [36]. Verran performed a simple study in the United Kingdom, cleaning the phone with antimicrobial wipes and comparing the number of colonies present before and after cleaning [37]. This finding is consistent with other studies using chlorhexidine digluconate and triclosan to reduce microbial contamination [38].
Considering the results of the present study, people should use personal hygiene methods such as washing hands before and after handling food and decontamination of phones to prevent bacterial diseases. In the present study, a decrease in bacterial contamination was observed after using disinfectants (1 and 2) on the surface of mobile phones. As a result, it is recommended that mobile phones be sterilized once a week with suitable disinfectants and not used in crowded places and frequent hand washing promoted as a way to prevent disease transmission.
The following are also recommended:
1. Conducting a sensitivity test for bacteria isolated from mobile phone to find out the extent of their contamination with antibiotic-resistant isolates
2. Conducting an extensive study on the presence of other microorganisms on mobile phone
3. Avoid giving mobile phone to children at young ages because the young child lick them, which poses a health risk to him.
5. We must be careful not to place our mobile devices in contaminated places, such as bathrooms, laboratories, etc., to avoid contamination with pathogenic bacteria.
Conclusion
Bacteria colonize cell phones in social groups, and contaminated phones transmit pathogens that can cause serious illnesses. Some of these bacteria are toxic and contribute to illness and death in humans. Using disinfectants reduces bacterial contamination on the surface of the mobile phone.
Acknowledgements: We are grateful to the Kufa Technical Institute, Al-Furat Al-Awsat Technical University for allowing us to conduct this study.
Ethical Permission: This study was approved by Kufa Technical Institute, Alfurat Alawsat Technical University according to the Declaration of Helsinki. All participants signed a written informed consent form. Also, all participants approved the use of their data in the current study.
Conflict of Interests: The authors have no conflicts of interest to declare.
Funding: There was no financial source.
Article Type: Original Research |
Subject:
Technology of Health Education
Received: 2022/02/13 | Accepted: 2022/10/2 | Published: 2022/10/17
Received: 2022/02/13 | Accepted: 2022/10/2 | Published: 2022/10/17
References
1. Elkholy M, Ewees I. Mobile (cellular) phone contamination with nosocomial pathogens in Intensive Care Units. Med J Cairo Univ. 2010;78(2):1-5. [Link]
2. Al-Ghamdi AK, Abdelmalek SMA, Ashshi AM, Faidah H, Shukri H, Jiman-Fatani AA. Bacterial contamination of computer keyboards and mice, elevator buttons, and shopping cards. Afr J Microbiol Res. 2011;5(23):3998-4003. [Link] [DOI:10.5897/AJMR11.770]
3. Bodena D, Teklemariam Z, Balakrishnan S, Tesfa T. Bacterial contamination of mobile phones of health professionals in eastern Ethiopia: antimicrobial susceptibility and associated factors. Trop Med Health. 2019;47:15. [Linkvv] [DOI:10.1186/s41182-019-0144-y]
4. Srivastava TS, Waghmare LS, Jagzape AT, Rawekar, AT, Quazi NZ, Mishra VP. Role of information communication technology in higher education: Learners perspective in rural medical schools. J Clin Diagn Res. 2014;8(6):XC01-6. [Link] [DOI:10.7860/JCDR/2014/8371.4448]
5. Stryjak J, Sivakumaran M. The mobile economy 2019 [Internet]. GSMA Intelligence; 2019 [Cited 2022 May 23]. Available from: https://www.gsmaintelligence.com/research/2019/02/the-mobile-economy-2019/731/ [Link]
6. Zhao B, Dewald C, Hennig M, Bossert J, Bauer M, Pletz, MW. Microorganisms @ materials surfaces in aircraft: potential risks for public health? - A systematic review. Travel Med Infect Dis. 2019;28:6-14. [Link] [DOI:10.1016/j.tmaid.2018.07.011]
7. Banawas S, Abdel-Hadi A, Alaidarous M, Alshehri B, Bin Dukhyil AA, et al. Multidrug-resistant bacteria associated with cell phones of healthcare professionals in selected hospitals in Saudi Arabia. Can J Infect Dis Med Microbiol. 218;2018:6598918. [Link] [DOI:10.1155/2018/6598918]
8. Bhardwaj N, Khatri M, Bhardwaj SK, Sonne C, Deep A, Kim KH. A review on mobile phones as bacterial reservoirs in healthcare environments and potential device decontamination approaches. Environ Res. 2020;186:109569. [Link] [DOI:10.1016/j.envres.2020.109569]
9. Stephens B, Azimi P, Thoemmes MS, Heidarinejad M, Allen JG, Gilbert JA. Microbial exchange via fomites and implications for human health. Curr Pollut Rep. 2019;5(4):198-213. [Link] [DOI:10.1007/s40726-019-00123-6]
10. Ovca A, Rednak B, Torkar K, Jevšnik M, Bauer M. Students' mobile phones - how clean are they? Int J Sanitary Engin Res. 2012;6(1):6-18. [Link]
11. Ibrahim TA, Akenroye OM, Opawale BO, Osabiya OJ. Isolation and identification of bacterial pathogens from mobile phones of volunteered technologists in Rufus Giwa Polytechnic, Owo, Ondo State. J Microbiol Biotech. 2013;3(1):37‐40. [Link] [DOI:10.15580/GJSETR.2013.6.100912104]
12. Patricia T, editor. Bailey & Scott's diagnostic microbiology, 13th Edition. London: Elsevier Health Sciences, Mosby; 2013. [Link]
13. Ulger F, Esen S, Dilek A, Yanik K, Gunaydin M, Leblebicioglu H. Are we aware how contaminated our mobile phones with nosocomial pathogens? Ann Clin Microbiol Antimicrob. 2009;8(1):1-4. [Link] [DOI:10.1186/1476-0711-8-7]
14. Lee YJ, Yoo CG, Lee CT, Chung HS, Kim YW, Han SK et al. Contamination rates between smart cell phones and non-smart cell phones of healthcare workers. J Hosp Med. 2013;8(3):144-7. [Link] [DOI:10.1002/jhm.2011]
15. Farhan MB, Abdulla KK. Isolation and diagnosis of pathogenic bacteria from the upper surface of the cell phone screen and conduct an antibiotic sensitivity test. Int J Drug Deliv Technol. 2019;9(2):222-5. [Link] [DOI:10.25258/ijddt.9.2.17]
16. Bhoonderowa A, Gookool S, Biranjia-Hurdoyal SD. The importance of mobile phones in the possible transmission of bacterial infections in the community. J Community Health. 2014;39(5):965-7. [Link] [DOI:10.1007/s10900-014-9838-6]
17. World Health Organization. Report on the burden of endemic health care-associated infection worldwide [Internet]. Geneva: World Health Organization; 2011 [cited 2022 Apr 11]. Available from: https://www.who.int/publications/i/item/report-on-the-burden-of-endemic-health-care-associated-infection-worldwide. [Link]
18. Qi C. Double-edged sword? Exploring the impact of students' academic usage of mobile devices on technostress and academic performance. Behav Inf Technol. 2019;38:1337-54. [Link] [DOI:10.1080/0144929X.2019.1585476]
19. Hossain SFA, Nurunnabi M, Hussain K, Saha SK. Effects of variety-seeking intention by mobile phone usage on university students' academic performance. Cogent Educ. 2019;6(1):1-18. [Link] [DOI:10.1080/2331186X.2019.1574692]
20. Verma DK, Barasa A, Dara D, W/Medehen H, Asrat H, Demissie N, Tegenaw K, Sendeku W, Berhane N. Isolation and characterization of bacteria from mobile phones of students and employees at University Of Gondar, Ethiopia. Bull Pharm Res. 2015;5(3):96-100. [Link]
21. Chaman R, Nargeseyan S, Jannesar R, Ravangard S, Nikbakht G. Survey of prevalence and types of bacterial contamination of mobile phones of personnel employed in major wards of educational hospitals in Yasuj. J Fundam Appl Sci. 2018;10(2):449-58. [Link]
22. Katsuse KA, Takahashi H, Yoshizawa S, Tateda K, Kaneko A, Kobayashi I. Staphylococcus aureus surface contamination of mobile phones and presence of genetically identical strains on the hands of nursing personnel. Am J Infect Control. 2017;45(8):929-31. [Link] [DOI:10.1016/j.ajic.2017.02.011]
23. Simmonds R, Lee D, Hayhurst E. Mobile phones as fomites for potential pathogens in hospitals: microbiome analysis reveals hidden contaminants. J Hosp Infect. 2020;104(2):207-13. [Link] [DOI:10.1016/j.jhin.2019.09.010]
24. Roth RR, Jenner WD. Microbial ecology of the skin. Annu Rev Microbiol. 1998;42:441- 64. [Link] [DOI:10.1146/annurev.mi.42.100188.002301]
25. Pal S, Juyal D, Adekhandi S, Sharma M, Prakash R, Sharma N, Rana A, Parihar A. Mobile phones: Reservoirs for the transmission of nosocomial pathogens. Adv Biomed Res. 2015;4:144-9. [Link] [DOI:10.4103/2277-9175.161553]
26. Zaman R, Helmi N. Isolation of bacteria from mobile phones before and after decontamination: Study carried out at King Abdulaziz University, Jeddah, Saudi Arabia. Afr J Microbiol Res. 2017;11(35):1371-8. [Link]
27. Al-Abdalall AHA. Isolation and identification of microbes associated with mobile phones in Dammam in eastern Saudi Arabia. J Family Community Med. 2010;17(1):11-4. [Link] [DOI:10.4103/1319-1683.68783]
28. Famurewa O, David OM. Cell phone: A medium of transmission of bacterial pathogens. World Rural Obser. 2009;1(2):69‐72. [Link]
29. Soto RG, Chu LG, Goldman JM, Rampil IJ, Ruskin KJ. Communication in critical care environments, Mobile telephones improve patient cares. Anaesth Analg. 2006;102:534-41. [Link] [DOI:10.1213/01.ane.0000194506.79408.79]
30. Rusin P, Maxwell S, Gerba C. Comparative surface‐to‐hand and fingertip-to-mouth transfer efficiency of gram-positive bacteria, gram‐negative bacteria and phage. J Appl Microbial. 2002;93(4):585‐92. [Link] [DOI:10.1046/j.1365-2672.2002.01734.x]
31. Neely AN, Weber JM, Daviau P, MacGregor A, Miranda C, et al. Computer equipment used in patient care within a multihospital system: Recommendations for cleaning and disinfection. Am J Infect Control. 2005;33(4):233-7. [Link] [DOI:10.1016/j.ajic.2005.03.002]
32. Jeske HC, Tiefenthaler W, Hohlrieder M, Hinterberger G, Benzer A. Bacterial contamination of anesthetists' hands by personal mobile phone and fixed phone use in the operating theatre. Anaesthesia. 2007;62(9):904-6. [Link] [DOI:10.1111/j.1365-2044.2007.05172.x]
33. Neely AN, Sittig DF. Basic microbiologic and infection control information to reduce the potential transmission of pathogens to patients via computer hardware. J Am Med Inform Assoc. 2002;9(5):500-8. [Link] [DOI:10.1197/jamia.M1082]
34. Jamalludeen NM. Efficacy of tap water or tap water and soap on Hand washing to remove hands-contaminated bacteria. Int J Sci Engin Res. 2017;8(7):1519-37. [Link]
35. Agarry OO, Olaleye MT, Bello-Michael CO. Comparative antimicrobial activities of aloe vera gel and leaf. Afr J Biotechnol 2005;4(12):1413-4. [Link]
36. Cataldi V, Di Bartolomeo S, Di Campli E, Nostro A, Cellini L, Di Giulio M. In vitro activity of Aloe vera inner gel against microorganisms grown in planktonic and sessile phases. International Journal of Immunopathology and Pharmacology. 2015;28(4):595-602. [Link] [DOI:10.1177/0394632015600594]
37. Verran J. The microbial contamination of mobile communication devices. J Microbiol Biol Educa. 2012;13(1):59-61. [Link] [DOI:10.1128/jmbe.v13i1.351]
38. Koscova J, Hurnikova Z, Pist J. Degree of bacterial contamination of mobile phone and computer keyboard surfaces and efficacy of disinfection with chlorhexidine digluconate and triclosan to its reduction. Int J Environ Res Public Health. 2018;15(10):2238. [Link] [DOI:10.3390/ijerph15102238]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |