



Volume 13, Issue 2 (2025)
Health Educ Health Promot 2025, 13(2): 305-313 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Adil Z, AL-Sarray A, Luma H. Awareness and Understanding of Waterborne Diseases among Healthcare Providers in Al-Karkh District, Baghdad. Health Educ Health Promot 2025; 13 (2) :305-313
URL: http://hehp.modares.ac.ir/article-5-81326-en.html
URL: http://hehp.modares.ac.ir/article-5-81326-en.html
1- Department of Community Health, College of Health and Medical Techniques, Middle Technical University, Baghdad, Iraq
Keywords: Waterborne Diseases [MeSH], Public Health [MeSH], Hygiene [MeSH], Iraq [MeSH], Cross-Sectional Study [MeSH]
Full-Text [PDF 640 kb]
(106 Downloads)
| Abstract (HTML) (174 Views)
Full-Text: (6 Views)
Introduction
Water-related infectious diseases are a major cause of mortality and morbidity worldwide, and the effects of climate change will exacerbate the challenges for the public health sector regarding both foodborne and waterborne diseases. Human exposure to waterborne infections occurs through contact with contaminated drinking water, recreational water, or food. Waterborne and foodborne diseases are linked to the ingestion of pathogens via contaminated water or food, while vector-borne diseases are linked to infections transmitted by arthropods, such as mosquitoes. Therefore, climate change and climate variability will affect the burden of climate-sensitive infectious diseases, particularly waterborne and foodborne diseases [1].
Risks associated with deficiencies in water, sanitation, and hygiene contribute to infectious diseases to humans through polluted water. These include cholera, Shigella, typhoid, hepatitis A and E, and poliomyelitis. These diseases account for about 1.5 million deaths annually and represent an estimated 3.6% of the global burden of disease in terms of disability-adjusted life years [2]. Poor water quality continues to pose a major threat to human health. Diarrheal disease alone accounts for an estimated 4.1% of the total disability adjusted life year (DALY) global burden of disease and is responsible for the deaths of 2 million people every year. It is estimated that 88% of that burden is attributable to unsafe water supply, sanitation, and hygiene, with the majority concentrated among children in developing countries [3].
According to estimates from the World Health Organization (2007), environmental modifications, such as initiatives to enhance sanitation and hygiene practices and to expand access to clean drinking water, can prevent 94% of waterborne diarrheal infections [4]. Moreover, a 2005 systematic review determined that diarrheal episodes are reduced by 25% through improved water supply, 32% through proper sanitation, 45% through hand washing, and by 39% through household water treatment and safe storage. Other interventions to decrease waterborne diseases include improvements in drinking water, hygiene practices, and sanitation facilities in less developed countries [5].
Waterborne diseases can be acquired during water-related recreational activities, such as swimming, boating, or other water sports. Many epidemiological studies conducted at both marine and freshwater bathing beaches have shown a significant increase in the incidence of illness, including gastrointestinal, respiratory, ear, ocular, and skin or wound infections among those who engage in water-based recreational activities [6].
Waterborne infections can still affect the most immunocompromised patients, even with proper monitoring and additional disinfection of the water distribution system. Comprehensive epidemiological data can be obtained through whole-genome sequencing to assess such transmissions. For the most vulnerable patients, point-of-use filters could be used as a last resort. In addition to technological solutions, patients and their families should report any issues with water quality or hygiene, and healthcare staff should receive training on strict hand hygiene guidelines and how to prevent contamination of the water system [7]. This study aimed to evaluate the awareness of healthcare providers in the Al-Karkh District of Baghdad regarding the prevention and management of waterborne diseases.
Instrument and Methods
Study design
The current cross-sectional descriptive study assessed the knowledge of healthcare providers regarding waterborne diseases in six hospitals and 25 healthcare centers located in the Al-Karkh side of Baghdad from January 2025 to March 2025.
Sample size
The sample included 550 medical staff and healthcare workers who were randomly selected from among the healthcare providers working in the hospitals and healthcare centers in the Al-Karkh district of Baghdad. Required data were collected on the healthcare providers’ knowledge about waterborne diseases. All eligible participants filled out a consent form and completed the research tool in written format.
Study tolls
The questionnaire aimed to collect data on the “definition of waterborne diseases, their modes of transmission, symptoms, affected age groups, and examples of such diseases.” It consisted of 45 questions. The structure of the questionnaire included four parts.
Part I: Respondent demographics
This section included seven elements addressing age, gender, educational level, professional level, years of experience, health institution, and involvement in training courses or workshops related to waterborne diseases [8].
Part II: Knowledge module
This section consisted of 45 questions that tested the participants’ understanding of general information, symptoms, consequences, mechanisms of transmission, and prevention strategies related to waterborne infections [9].
Part III: Attitudes module
This part comprised 13 questions measuring the attitudes of medical and paramedical staff regarding waterborne diseases, including attitudes toward maintaining safe water and clean water containers. These questions were derived from previous studies [10].
Part IV: Practices module
This section contained 15 questions that evaluated the practices of medical and paramedical staff regarding waterborne diseases. These questions provided information on how to keep water sources, water-collecting containers, and storage containers clean, ensuring that water is preserved from the source to the final consumer while being shielded from contamination [11].
A reliability coefficient of 0.93 was found when the questionnaire’s reliability was examined using Cronbach’s alpha.
Statistical analysis
The collected data were coded, input, displayed, and analyzed using SPSS 29. The basic statistics used to display the data included frequency, percentage, mean, standard deviation, and range (minimum-maximum values). The significance of the differences between various means (quantitative data) was tested using the Student’s t-test for calculating the variation between two independent means, the paired t-test for the variation between two observations (or two dependent means), and the ANOVA test for variations among more than two separate means. The Pearson Chi-square test was employed to determine whether the differences in percentages (qualitative data) were significant (χ²-test), applying Yates’ correction or the Fisher Exact test whenever applicable. A p-value was deemed statistically significant if it was equal to or less than 0.05 [8-10].
Findings
The study assessed 550 healthcare providers, with a mean age of 34.0±9.2 years, ranging from 22 to 59 years. The age group of 20-29 years had the highest percentage (40.4%), while the age group of 50-59 years had the lowest percentage (8.9%). Females represented the majority of the sample (72.9%) compared to males (27.1%).
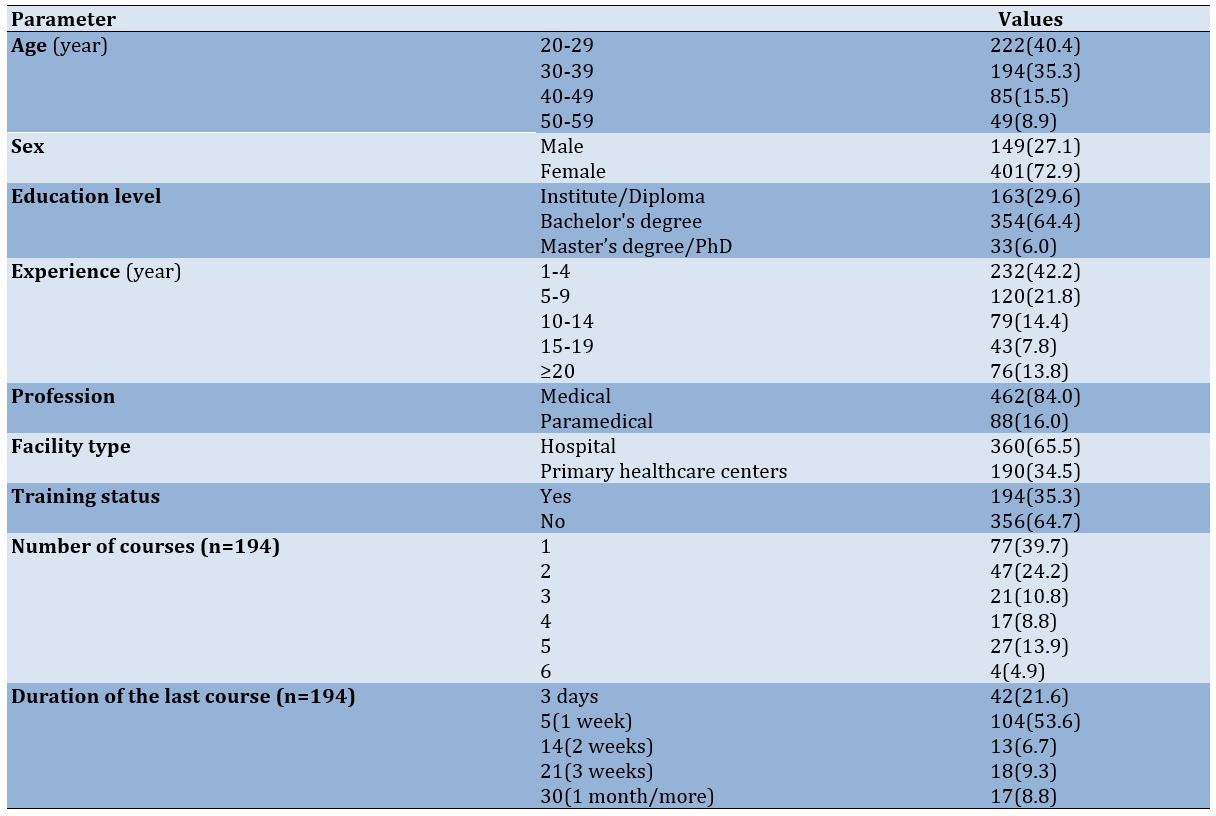
The highest percentage of participants held a bachelor’s degree (64.4%), followed by those with an institute/diploma (29.6%), while the lowest percentage had a master’s/PhD degree (6.0%). Most respondents had 1-4 years of experience (42.2%), and the mean work experience was 9.0±8.5 years, ranging from 1 to 35 years. The majority of healthcare providers were medical professionals (84.0%), while paramedical staff accounted for 16.0%. Most participants worked in hospitals (65.5%) compared to primary healthcare centers (PHCCs; 34.5%). The majority of participants (64.7%) had not received any training on waterborne diseases, while only 35.3% had undergone training. Among those trained, the most common course duration was 5 days (53.6%), followed by 3 days (21.6%; Table 1).
Table 1. Frequency of socio-demographic characteristics of the sample
The vast majority (93.8%) were aware that waterborne diseases are caused by pathogens in contaminated water, while nearly all (92.4%) recognized that outbreaks result in significant mortality in vulnerable communities. About three-quarters of providers (74.7%) correctly identified drinking tap water as a primary transmission route for waterborne diseases. Most respondents (86.5%) knew that these diseases affect both humans and animals. The overwhelming majority recognized poor water quality as a direct indicator (88.5%), and nearly all (90.4%) identified poor sanitation and hygiene as major causes of waterborne diseases (Table 2).
Table 2. Awareness of healthcare providers about waterborne diseases

Most providers (82.0%) correctly identified contamination by human or animal feces as a primary source of waterborne diseases. Similarly, a strong majority (82.7%) recognized improper disposal of industrial waste as a known cause. Nearly three-quarters of providers (73.3%) understood that heavy rains and flooding often lead to increased waterborne diseases. However, knowledge was notably lower (64.2%) regarding the contribution of agricultural runoff to water contamination, with a substantial proportion (23.3%) denying this connection and 12.5% being uncertain (Table 3).
Table 3. Awareness of healthcare providers about waterborne disease transmission routes

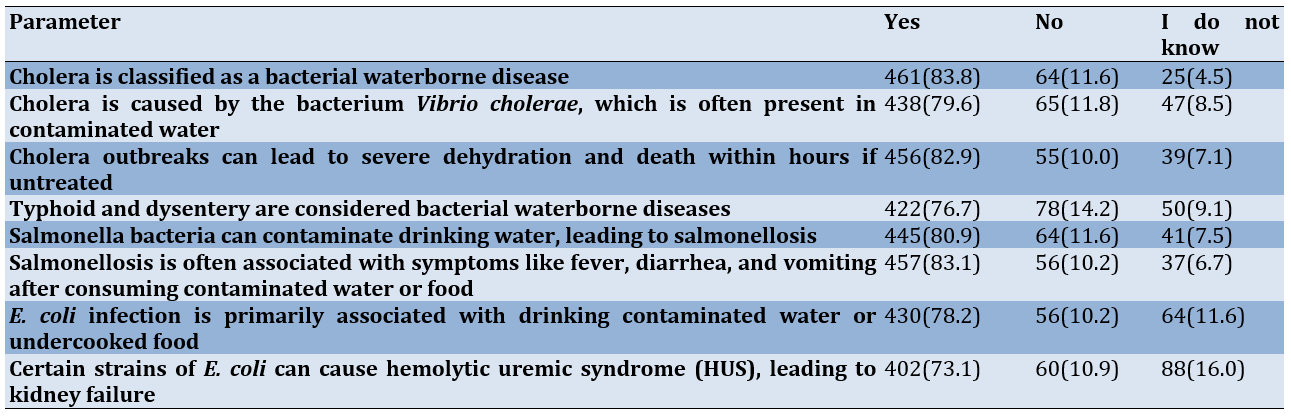
The majority (83.8%) correctly identified cholera as a bacterial waterborne disease, while nearly as many (82.9%) recognized its potential to cause rapid dehydration and death if untreated (Table 4).
Table 4. Awareness of healthcare providers about specific waterborne diseases (bacterial)
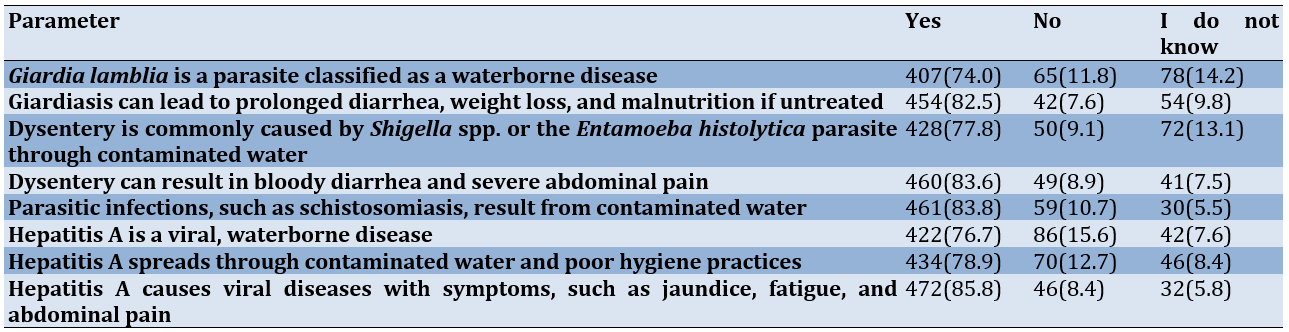
The majority (83.8%) correctly identified schistosomiasis as resulting from contaminated water, while nearly as many (85.8%) recognized hepatitis A symptoms, including jaundice and abdominal pain. Most providers (78.9%) knew that hepatitis A spreads through contaminated water and poor hygiene, and 76.7% correctly classified it as a viral disease. For parasitic infections, 82.5% understood the consequences of giardiasis, though fewer (74.0%) knew that Giardia lamblia is waterborne. Regarding dysentery, 83.6% recognized its symptoms, while 77.8% knew its causes (Shigella spp. or Entamoeba histolytica), with 13.1% answering “Do Not Know” to this question (Table 5).
Table 5. Awareness of healthcare providers of specific waterborne diseases (parasitic & viral)
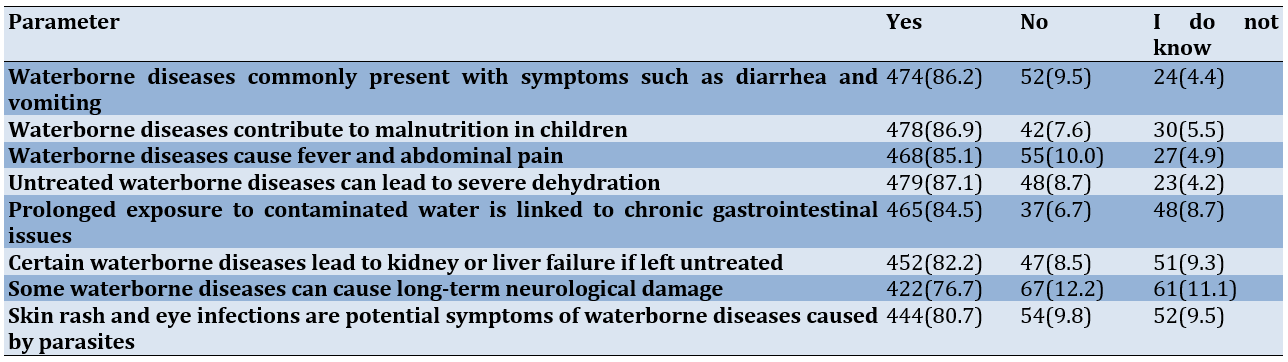
The majority of providers (87.1%) recognized that untreated waterborne diseases can lead to severe dehydration, while nearly as many (86.9%) knew that these diseases contribute to malnutrition in children. Most respondents (86.2%) identified diarrhea and vomiting as common symptoms, and 85.1% acknowledged that fever and abdominal pain are typical manifestations. A significant proportion (84.5%) understood the link between prolonged exposure to contaminated water and chronic gastrointestinal issues. Providers demonstrated good awareness of serious complications, with 82.2% correctly stating that certain waterborne diseases can cause kidney or liver failure if untreated. Skin rashes and eye infections as potential parasitic symptoms were recognized by 80.7% of respondents. Knowledge was slightly lower regarding neurological effects, with 76.7% agreeing that some waterborne diseases can cause long-term neurological damage, while 11.1% answered “Do Not Know” to this question, representing the highest level of uncertainty in this section. The remaining responses for all items showed relatively low proportions of incorrect answers or uncertainty, indicating generally strong awareness of waterborne disease symptoms and complications among healthcare providers (Table 6).
Table 6. Awareness of healthcare providers about symptoms and complications
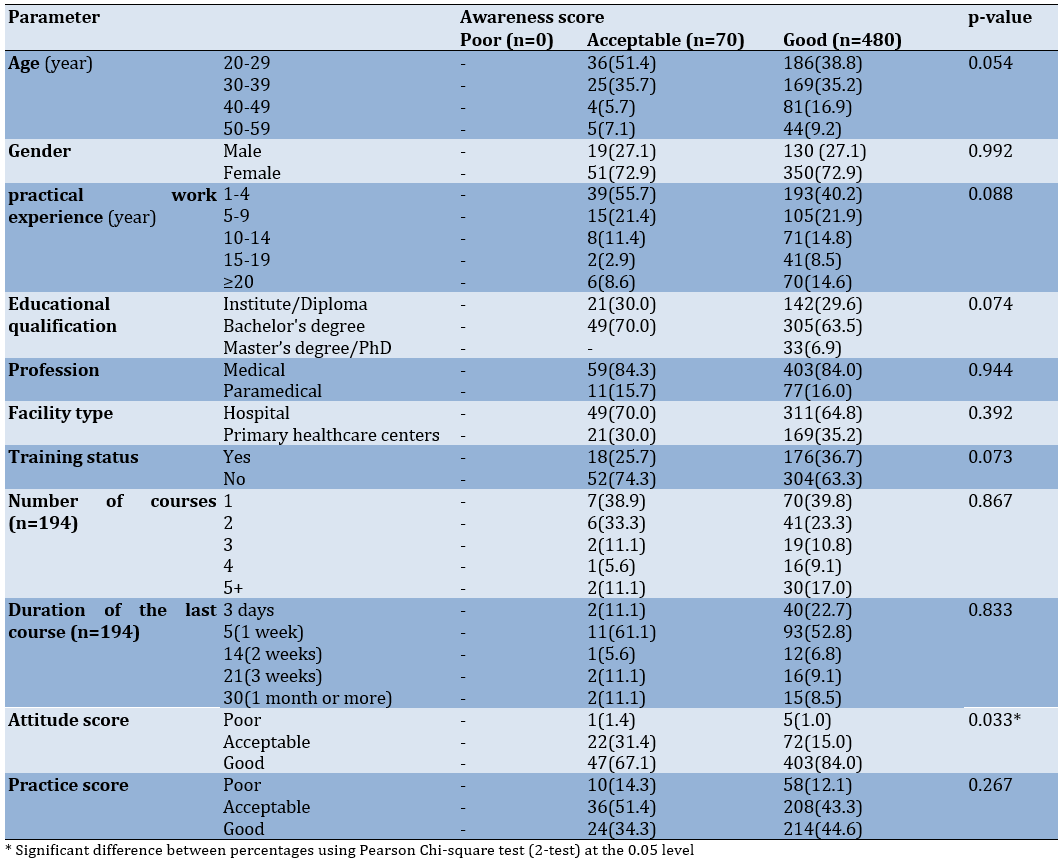
No providers scored in the poor knowledge category, with 70 (12.7%) showing acceptable knowledge and 480 (87.3%) demonstrating good knowledge. A statistically significant association emerged between attitude and knowledge scores (p=0.033), with 84.0% of providers with good attitudes also exhibiting good knowledge, compared to 67.1% with acceptable knowledge.
Age showed a marginal association (p=0.054), with younger providers (20-29 years) comprising 51.4% of the acceptable knowledge group versus 38.8% of the good knowledge group. Training status approached significance (p=0.073), as trained providers represented 36.7% of the good knowledge category compared to 25.7% of the acceptable group. Educational qualifications indicated that no Master’s/PhD holders fell into the acceptable knowledge category, although this difference was not statistically significant (p=0.074).
Other demographic and professional characteristics—including gender, years of experience, profession type, facility type, and practice scores—showed no significant relationships with knowledge levels (all p>0.05). Among trained providers, neither the number of courses taken nor their duration significantly affected knowledge scores. The findings suggest that while positive attitudes strongly correlate with better knowledge, most demographic factors do not significantly influence knowledge levels in this sample (Table 7).
Table 7. Association between healthcare providers' characteristics and their knowledge of waterborne diseases
Discussion
This study aimed to evaluate the awareness of healthcare providers in the Al-Karkh District of Baghdad regarding the prevention and management of waterborne diseases. The majority of participants were female. This finding is consistent with the results of previous research, confirming that the majority of their participants are female. The average age in the current study was 34.0±9.2 years, and the majority of the sample had 1-4 years of work experience. These findings contrast with another study [11], in which the majority of their participants are aged 30-40 years. However, they also differ from another study [12], where most of the sample have 15-35 years of experience, and only a very few have 3-5 years.
Most participants held a bachelor’s degree. This finding contrasts with another study that reported half of their sample are institute graduates, with only a few holding bachelor’s degrees. It also disagrees with another study [13], where more than half of the sample have diplomas, and only a few have higher academic qualifications. In another study [14], a small number of institute graduates is mentioned, which partially supports the lower representation of technical-level education.
More than half of the participants had not received any prior training related to waterborne diseases. This significantly contrasts with Fadhl et al. [8], who reported that 80% of healthcare workers have received either formal or informal training on topics, such as hand hygiene, water treatment, storage, and related diseases.
The vast majority of the sample had a good awareness that waterborne diseases are illnesses caused by water contaminated by pathogens. The transmission routes of waterborne diseases demonstrated that most providers correctly identified contamination by human or animal feces as a primary source. Similarly, a strong majority recognized improper disposal of industrial waste as a known cause. This finding resonates with the studies by Abd Elrazak et al. [15] and Balan et al. [16] in northern Iraq and India, showing that respondents have a good knowledge of waterborne diseases and their causes.
About three-quarters of respondents correctly identified drinking tap water as a primary transmission route for waterborne diseases. This validates the previous study by Balan et al. [16], indicating that these diseases can spread from drinking tap water due to improper maintenance of the pipeline system that transports it. Nearly all our providers identified poor sanitation and hygiene as major causes of waterborne diseases, a finding that corresponds with that of Bennett et al. [17].
Providers demonstrated robust knowledge of high-risk populations, including children under five, infants, and the elderly, which is critical for targeted interventions in vulnerable groups. This is similar to the findings of Ray et al. [18], showing that water can have negative health impacts, such as neurological disorders, gastrointestinal problems, pregnancy complications, and reproductive issues, ultimately affecting the health of infants, pregnant women, the elderly, and those who are already ill and taking medication [8, 19]. These studies demonstrated that a poor water environment is connected to higher maternal mortality, which aligns with the findings of the ongoing study.
Nearly three-quarters of providers understood that heavy rain and flooding often lead to increased waterborne diseases. However, knowledge was notably lower regarding agricultural runoff’s contribution to water contamination [20]. This aligns with our findings, which clearly indicate linkages between waterborne diseases and climate change. Our providers showed high awareness of sanitation and hygiene as causative factors, water quality as a risk indicator, and fecal contamination as a primary source [17].
The study in Tanzania conflicted with the findings of the present study, which indicated that less than half of the participants have adequate knowledge regarding household sanitation and hygiene, while half have inadequate knowledge [21]. This study partially explains that the poor quality of water in in-house storage vessels reflects considerable in-house contamination of drinking water. Risk factors for diarrhea included inadequate water connection and water storage facilities. The association between water quality and diarrhea varied by the level of water availability and the presence or absence of a toilet, which aligns with the concept of the current study. The majority of our samples correctly identified cholera as a bacterial waterborne disease, while nearly as many recognized its potential to cause rapid dehydration and death if untreated. Most providers also know that cholera is caused by Vibrio cholerae in contaminated water [22].
In Yemen, the results were consistent with a recent study, which showed that participants have good knowledge about the infectious agents, vulnerable age groups, main treatments, and disagreements in knowledge about modes of transmission, severity classification, and complications. Current findings indicated that awareness among providers was slightly lower for typhoid and dysentery, both of which are bacterial diseases. Regarding salmonellosis, most understand its link to contaminated water, and a high percentage of the group recognizes its symptoms [23]. This study demonstrated consistency with the current study in terms of providers showing strong awareness of transmission routes, although gaps exist in understanding severity, treatment challenges, and symptoms of typhoid fever [24, 25]. These studies contradict our findings, which showed that participants had less awareness about typhoid, potentially due to inadequate training in waterborne diseases.
The majority correctly identified schistosomiasis as resulting from contaminated water, which is similar to the findings of another study [26]. Many respondents understood the role of contact with contaminated water in transmission. While nearly as many recognized hepatitis A symptoms, including jaundice and abdominal pain, most providers knew that hepatitis A spreads through contaminated water and poor hygiene, and they correctly classified it as a viral disease [27]. This study supports the recent finding that participants had a high level of knowledge about modes of transmission, signs and symptoms, and moderate knowledge about vaccination [28]. This aligns with the outcomes of our study regarding hepatitis A vaccination. A sufficient number of providers recognized that Giardia lamblia is waterborne, which corresponds with Mudavanhu et al. [29], who found that participants have good knowledge; however, Aquino [26] conflicted with our findings, indicating poor awareness, possibly due to inadequate education for the participants about waterborne diseases
A high percentage of providers recognized its symptoms and knew its causes (Shigella Spp. or Entamoeba histolytica). This disagrees with Shamarina et al. [30], who stated that there is inadequate awareness among physicians about amoebiasis. Abd Elrazak et al. [15] agree with our findings. The contrast between the present study and their study may be due to the fact that their study included more detailed questions about amoebiasis and giardiasis.
The majority of providers recognized that untreated waterborne diseases can lead to severe dehydration, while nearly as many knew that these diseases contribute to malnutrition in children. Most respondents identified diarrhea and vomiting as common symptoms and acknowledged that fever and abdominal pain are typical manifestations. A significant proportion understood the link between prolonged exposure to contaminated water and chronic gastrointestinal issues. Providers demonstrated good awareness of serious complications [29]. This study disputes our findings, showing low knowledge about the common causes of diarrhea in children under five years old. However, it agrees that providers have good knowledge about how diarrheal diseases can cause malabsorption and that waterborne diseases can lead to severe diarrhea [24]. It partially disagrees with our finding that participants had moderate knowledge about the meaning of dehydration [31]. This study is inconsistent with our findings, which indicated that participants had low knowledge about the symptoms of diarrhea, suggesting they need more education, potentially due to limited experience.
Overall, healthcare providers demonstrated good knowledge in dealing with waterborne diseases. The providers exhibited a strong understanding in this area. Abd Elrazak et al. [15] and Bennett et al. [17] agree with the current study, attributing knowledge gaps to poor training. In contrast, Galindo et al. [32] disagree with our findings, asserting that participants have good knowledge. Our younger providers comprised half of the group with acceptable knowledge, while only a few belonged to the good knowledge group. Among trained providers, only a few fell into the good knowledge category compared to less than a quarter in the acceptable knowledge group [33-36]. These studies resonate with our findings, revealing considerable differences in healthcare providers’ knowledge and practices concerning waterborne infections based on their age and the relevant training they attended. There is a significant relationship between respondents’ level of awareness and their practices regarding waterborne diseases, influenced by their age and the training they have received [37].
Most medical professionals in Al-Karkh, Baghdad, were well-versed in waterborne illnesses, particularly concerning prevention and symptoms. However, there are still gaps in knowledge regarding certain diseases and environmental factors. Apart from a positive correlation with attitudes, most demographic characteristics did not show any meaningful association with knowledge. We suggest focused training initiatives to address these gaps. The burden of waterborne illnesses can be reduced, and health interventions can be strengthened by increasing awareness through education.
Conclusion
The majority of medical professionals in Al-Karkh, Baghdad, are well-versed in waterborne illnesses, particularly concerning prevention and symptoms.
Acknowledgments: I would like to express my sincere thanks to all health providers across Baghdad Governorate who participated in this research and generously devoted their valuable time.
Ethical Permissions: Participants are fully informed about the research purpose, procedures, risks, and benefits, and they must voluntarily agree to participate.
Conflicts of Interests: The author acknowledges no conflict of interest in this study.
Authors' Contribution: Adil Z (First Author), Introduction Writer/Methodologist/Main Researcher (50%); AL-Sarray AM (Second Author), Assistant Researcher/Statistical Analyst (30%); Luma HA (Third Author), Discussion Writer/Statistical Analyst (20%)
Funding/Support: No funding was received.
Water-related infectious diseases are a major cause of mortality and morbidity worldwide, and the effects of climate change will exacerbate the challenges for the public health sector regarding both foodborne and waterborne diseases. Human exposure to waterborne infections occurs through contact with contaminated drinking water, recreational water, or food. Waterborne and foodborne diseases are linked to the ingestion of pathogens via contaminated water or food, while vector-borne diseases are linked to infections transmitted by arthropods, such as mosquitoes. Therefore, climate change and climate variability will affect the burden of climate-sensitive infectious diseases, particularly waterborne and foodborne diseases [1].
Risks associated with deficiencies in water, sanitation, and hygiene contribute to infectious diseases to humans through polluted water. These include cholera, Shigella, typhoid, hepatitis A and E, and poliomyelitis. These diseases account for about 1.5 million deaths annually and represent an estimated 3.6% of the global burden of disease in terms of disability-adjusted life years [2]. Poor water quality continues to pose a major threat to human health. Diarrheal disease alone accounts for an estimated 4.1% of the total disability adjusted life year (DALY) global burden of disease and is responsible for the deaths of 2 million people every year. It is estimated that 88% of that burden is attributable to unsafe water supply, sanitation, and hygiene, with the majority concentrated among children in developing countries [3].
According to estimates from the World Health Organization (2007), environmental modifications, such as initiatives to enhance sanitation and hygiene practices and to expand access to clean drinking water, can prevent 94% of waterborne diarrheal infections [4]. Moreover, a 2005 systematic review determined that diarrheal episodes are reduced by 25% through improved water supply, 32% through proper sanitation, 45% through hand washing, and by 39% through household water treatment and safe storage. Other interventions to decrease waterborne diseases include improvements in drinking water, hygiene practices, and sanitation facilities in less developed countries [5].
Waterborne diseases can be acquired during water-related recreational activities, such as swimming, boating, or other water sports. Many epidemiological studies conducted at both marine and freshwater bathing beaches have shown a significant increase in the incidence of illness, including gastrointestinal, respiratory, ear, ocular, and skin or wound infections among those who engage in water-based recreational activities [6].
Waterborne infections can still affect the most immunocompromised patients, even with proper monitoring and additional disinfection of the water distribution system. Comprehensive epidemiological data can be obtained through whole-genome sequencing to assess such transmissions. For the most vulnerable patients, point-of-use filters could be used as a last resort. In addition to technological solutions, patients and their families should report any issues with water quality or hygiene, and healthcare staff should receive training on strict hand hygiene guidelines and how to prevent contamination of the water system [7]. This study aimed to evaluate the awareness of healthcare providers in the Al-Karkh District of Baghdad regarding the prevention and management of waterborne diseases.
Instrument and Methods
Study design
The current cross-sectional descriptive study assessed the knowledge of healthcare providers regarding waterborne diseases in six hospitals and 25 healthcare centers located in the Al-Karkh side of Baghdad from January 2025 to March 2025.
Sample size
The sample included 550 medical staff and healthcare workers who were randomly selected from among the healthcare providers working in the hospitals and healthcare centers in the Al-Karkh district of Baghdad. Required data were collected on the healthcare providers’ knowledge about waterborne diseases. All eligible participants filled out a consent form and completed the research tool in written format.
Study tolls
The questionnaire aimed to collect data on the “definition of waterborne diseases, their modes of transmission, symptoms, affected age groups, and examples of such diseases.” It consisted of 45 questions. The structure of the questionnaire included four parts.
Part I: Respondent demographics
This section included seven elements addressing age, gender, educational level, professional level, years of experience, health institution, and involvement in training courses or workshops related to waterborne diseases [8].
Part II: Knowledge module
This section consisted of 45 questions that tested the participants’ understanding of general information, symptoms, consequences, mechanisms of transmission, and prevention strategies related to waterborne infections [9].
Part III: Attitudes module
This part comprised 13 questions measuring the attitudes of medical and paramedical staff regarding waterborne diseases, including attitudes toward maintaining safe water and clean water containers. These questions were derived from previous studies [10].
Part IV: Practices module
This section contained 15 questions that evaluated the practices of medical and paramedical staff regarding waterborne diseases. These questions provided information on how to keep water sources, water-collecting containers, and storage containers clean, ensuring that water is preserved from the source to the final consumer while being shielded from contamination [11].
A reliability coefficient of 0.93 was found when the questionnaire’s reliability was examined using Cronbach’s alpha.
Statistical analysis
The collected data were coded, input, displayed, and analyzed using SPSS 29. The basic statistics used to display the data included frequency, percentage, mean, standard deviation, and range (minimum-maximum values). The significance of the differences between various means (quantitative data) was tested using the Student’s t-test for calculating the variation between two independent means, the paired t-test for the variation between two observations (or two dependent means), and the ANOVA test for variations among more than two separate means. The Pearson Chi-square test was employed to determine whether the differences in percentages (qualitative data) were significant (χ²-test), applying Yates’ correction or the Fisher Exact test whenever applicable. A p-value was deemed statistically significant if it was equal to or less than 0.05 [8-10].
Findings
The study assessed 550 healthcare providers, with a mean age of 34.0±9.2 years, ranging from 22 to 59 years. The age group of 20-29 years had the highest percentage (40.4%), while the age group of 50-59 years had the lowest percentage (8.9%). Females represented the majority of the sample (72.9%) compared to males (27.1%).
The highest percentage of participants held a bachelor’s degree (64.4%), followed by those with an institute/diploma (29.6%), while the lowest percentage had a master’s/PhD degree (6.0%). Most respondents had 1-4 years of experience (42.2%), and the mean work experience was 9.0±8.5 years, ranging from 1 to 35 years. The majority of healthcare providers were medical professionals (84.0%), while paramedical staff accounted for 16.0%. Most participants worked in hospitals (65.5%) compared to primary healthcare centers (PHCCs; 34.5%). The majority of participants (64.7%) had not received any training on waterborne diseases, while only 35.3% had undergone training. Among those trained, the most common course duration was 5 days (53.6%), followed by 3 days (21.6%; Table 1).
Table 1. Frequency of socio-demographic characteristics of the sample
The vast majority (93.8%) were aware that waterborne diseases are caused by pathogens in contaminated water, while nearly all (92.4%) recognized that outbreaks result in significant mortality in vulnerable communities. About three-quarters of providers (74.7%) correctly identified drinking tap water as a primary transmission route for waterborne diseases. Most respondents (86.5%) knew that these diseases affect both humans and animals. The overwhelming majority recognized poor water quality as a direct indicator (88.5%), and nearly all (90.4%) identified poor sanitation and hygiene as major causes of waterborne diseases (Table 2).
Table 2. Awareness of healthcare providers about waterborne diseases
Most providers (82.0%) correctly identified contamination by human or animal feces as a primary source of waterborne diseases. Similarly, a strong majority (82.7%) recognized improper disposal of industrial waste as a known cause. Nearly three-quarters of providers (73.3%) understood that heavy rains and flooding often lead to increased waterborne diseases. However, knowledge was notably lower (64.2%) regarding the contribution of agricultural runoff to water contamination, with a substantial proportion (23.3%) denying this connection and 12.5% being uncertain (Table 3).
Table 3. Awareness of healthcare providers about waterborne disease transmission routes
The majority (83.8%) correctly identified cholera as a bacterial waterborne disease, while nearly as many (82.9%) recognized its potential to cause rapid dehydration and death if untreated (Table 4).
Table 4. Awareness of healthcare providers about specific waterborne diseases (bacterial)
The majority (83.8%) correctly identified schistosomiasis as resulting from contaminated water, while nearly as many (85.8%) recognized hepatitis A symptoms, including jaundice and abdominal pain. Most providers (78.9%) knew that hepatitis A spreads through contaminated water and poor hygiene, and 76.7% correctly classified it as a viral disease. For parasitic infections, 82.5% understood the consequences of giardiasis, though fewer (74.0%) knew that Giardia lamblia is waterborne. Regarding dysentery, 83.6% recognized its symptoms, while 77.8% knew its causes (Shigella spp. or Entamoeba histolytica), with 13.1% answering “Do Not Know” to this question (Table 5).
Table 5. Awareness of healthcare providers of specific waterborne diseases (parasitic & viral)
The majority of providers (87.1%) recognized that untreated waterborne diseases can lead to severe dehydration, while nearly as many (86.9%) knew that these diseases contribute to malnutrition in children. Most respondents (86.2%) identified diarrhea and vomiting as common symptoms, and 85.1% acknowledged that fever and abdominal pain are typical manifestations. A significant proportion (84.5%) understood the link between prolonged exposure to contaminated water and chronic gastrointestinal issues. Providers demonstrated good awareness of serious complications, with 82.2% correctly stating that certain waterborne diseases can cause kidney or liver failure if untreated. Skin rashes and eye infections as potential parasitic symptoms were recognized by 80.7% of respondents. Knowledge was slightly lower regarding neurological effects, with 76.7% agreeing that some waterborne diseases can cause long-term neurological damage, while 11.1% answered “Do Not Know” to this question, representing the highest level of uncertainty in this section. The remaining responses for all items showed relatively low proportions of incorrect answers or uncertainty, indicating generally strong awareness of waterborne disease symptoms and complications among healthcare providers (Table 6).
Table 6. Awareness of healthcare providers about symptoms and complications
No providers scored in the poor knowledge category, with 70 (12.7%) showing acceptable knowledge and 480 (87.3%) demonstrating good knowledge. A statistically significant association emerged between attitude and knowledge scores (p=0.033), with 84.0% of providers with good attitudes also exhibiting good knowledge, compared to 67.1% with acceptable knowledge.
Age showed a marginal association (p=0.054), with younger providers (20-29 years) comprising 51.4% of the acceptable knowledge group versus 38.8% of the good knowledge group. Training status approached significance (p=0.073), as trained providers represented 36.7% of the good knowledge category compared to 25.7% of the acceptable group. Educational qualifications indicated that no Master’s/PhD holders fell into the acceptable knowledge category, although this difference was not statistically significant (p=0.074).
Other demographic and professional characteristics—including gender, years of experience, profession type, facility type, and practice scores—showed no significant relationships with knowledge levels (all p>0.05). Among trained providers, neither the number of courses taken nor their duration significantly affected knowledge scores. The findings suggest that while positive attitudes strongly correlate with better knowledge, most demographic factors do not significantly influence knowledge levels in this sample (Table 7).
Table 7. Association between healthcare providers' characteristics and their knowledge of waterborne diseases
Discussion
This study aimed to evaluate the awareness of healthcare providers in the Al-Karkh District of Baghdad regarding the prevention and management of waterborne diseases. The majority of participants were female. This finding is consistent with the results of previous research, confirming that the majority of their participants are female. The average age in the current study was 34.0±9.2 years, and the majority of the sample had 1-4 years of work experience. These findings contrast with another study [11], in which the majority of their participants are aged 30-40 years. However, they also differ from another study [12], where most of the sample have 15-35 years of experience, and only a very few have 3-5 years.
Most participants held a bachelor’s degree. This finding contrasts with another study that reported half of their sample are institute graduates, with only a few holding bachelor’s degrees. It also disagrees with another study [13], where more than half of the sample have diplomas, and only a few have higher academic qualifications. In another study [14], a small number of institute graduates is mentioned, which partially supports the lower representation of technical-level education.
More than half of the participants had not received any prior training related to waterborne diseases. This significantly contrasts with Fadhl et al. [8], who reported that 80% of healthcare workers have received either formal or informal training on topics, such as hand hygiene, water treatment, storage, and related diseases.
The vast majority of the sample had a good awareness that waterborne diseases are illnesses caused by water contaminated by pathogens. The transmission routes of waterborne diseases demonstrated that most providers correctly identified contamination by human or animal feces as a primary source. Similarly, a strong majority recognized improper disposal of industrial waste as a known cause. This finding resonates with the studies by Abd Elrazak et al. [15] and Balan et al. [16] in northern Iraq and India, showing that respondents have a good knowledge of waterborne diseases and their causes.
About three-quarters of respondents correctly identified drinking tap water as a primary transmission route for waterborne diseases. This validates the previous study by Balan et al. [16], indicating that these diseases can spread from drinking tap water due to improper maintenance of the pipeline system that transports it. Nearly all our providers identified poor sanitation and hygiene as major causes of waterborne diseases, a finding that corresponds with that of Bennett et al. [17].
Providers demonstrated robust knowledge of high-risk populations, including children under five, infants, and the elderly, which is critical for targeted interventions in vulnerable groups. This is similar to the findings of Ray et al. [18], showing that water can have negative health impacts, such as neurological disorders, gastrointestinal problems, pregnancy complications, and reproductive issues, ultimately affecting the health of infants, pregnant women, the elderly, and those who are already ill and taking medication [8, 19]. These studies demonstrated that a poor water environment is connected to higher maternal mortality, which aligns with the findings of the ongoing study.
Nearly three-quarters of providers understood that heavy rain and flooding often lead to increased waterborne diseases. However, knowledge was notably lower regarding agricultural runoff’s contribution to water contamination [20]. This aligns with our findings, which clearly indicate linkages between waterborne diseases and climate change. Our providers showed high awareness of sanitation and hygiene as causative factors, water quality as a risk indicator, and fecal contamination as a primary source [17].
The study in Tanzania conflicted with the findings of the present study, which indicated that less than half of the participants have adequate knowledge regarding household sanitation and hygiene, while half have inadequate knowledge [21]. This study partially explains that the poor quality of water in in-house storage vessels reflects considerable in-house contamination of drinking water. Risk factors for diarrhea included inadequate water connection and water storage facilities. The association between water quality and diarrhea varied by the level of water availability and the presence or absence of a toilet, which aligns with the concept of the current study. The majority of our samples correctly identified cholera as a bacterial waterborne disease, while nearly as many recognized its potential to cause rapid dehydration and death if untreated. Most providers also know that cholera is caused by Vibrio cholerae in contaminated water [22].
In Yemen, the results were consistent with a recent study, which showed that participants have good knowledge about the infectious agents, vulnerable age groups, main treatments, and disagreements in knowledge about modes of transmission, severity classification, and complications. Current findings indicated that awareness among providers was slightly lower for typhoid and dysentery, both of which are bacterial diseases. Regarding salmonellosis, most understand its link to contaminated water, and a high percentage of the group recognizes its symptoms [23]. This study demonstrated consistency with the current study in terms of providers showing strong awareness of transmission routes, although gaps exist in understanding severity, treatment challenges, and symptoms of typhoid fever [24, 25]. These studies contradict our findings, which showed that participants had less awareness about typhoid, potentially due to inadequate training in waterborne diseases.
The majority correctly identified schistosomiasis as resulting from contaminated water, which is similar to the findings of another study [26]. Many respondents understood the role of contact with contaminated water in transmission. While nearly as many recognized hepatitis A symptoms, including jaundice and abdominal pain, most providers knew that hepatitis A spreads through contaminated water and poor hygiene, and they correctly classified it as a viral disease [27]. This study supports the recent finding that participants had a high level of knowledge about modes of transmission, signs and symptoms, and moderate knowledge about vaccination [28]. This aligns with the outcomes of our study regarding hepatitis A vaccination. A sufficient number of providers recognized that Giardia lamblia is waterborne, which corresponds with Mudavanhu et al. [29], who found that participants have good knowledge; however, Aquino [26] conflicted with our findings, indicating poor awareness, possibly due to inadequate education for the participants about waterborne diseases
A high percentage of providers recognized its symptoms and knew its causes (Shigella Spp. or Entamoeba histolytica). This disagrees with Shamarina et al. [30], who stated that there is inadequate awareness among physicians about amoebiasis. Abd Elrazak et al. [15] agree with our findings. The contrast between the present study and their study may be due to the fact that their study included more detailed questions about amoebiasis and giardiasis.
The majority of providers recognized that untreated waterborne diseases can lead to severe dehydration, while nearly as many knew that these diseases contribute to malnutrition in children. Most respondents identified diarrhea and vomiting as common symptoms and acknowledged that fever and abdominal pain are typical manifestations. A significant proportion understood the link between prolonged exposure to contaminated water and chronic gastrointestinal issues. Providers demonstrated good awareness of serious complications [29]. This study disputes our findings, showing low knowledge about the common causes of diarrhea in children under five years old. However, it agrees that providers have good knowledge about how diarrheal diseases can cause malabsorption and that waterborne diseases can lead to severe diarrhea [24]. It partially disagrees with our finding that participants had moderate knowledge about the meaning of dehydration [31]. This study is inconsistent with our findings, which indicated that participants had low knowledge about the symptoms of diarrhea, suggesting they need more education, potentially due to limited experience.
Overall, healthcare providers demonstrated good knowledge in dealing with waterborne diseases. The providers exhibited a strong understanding in this area. Abd Elrazak et al. [15] and Bennett et al. [17] agree with the current study, attributing knowledge gaps to poor training. In contrast, Galindo et al. [32] disagree with our findings, asserting that participants have good knowledge. Our younger providers comprised half of the group with acceptable knowledge, while only a few belonged to the good knowledge group. Among trained providers, only a few fell into the good knowledge category compared to less than a quarter in the acceptable knowledge group [33-36]. These studies resonate with our findings, revealing considerable differences in healthcare providers’ knowledge and practices concerning waterborne infections based on their age and the relevant training they attended. There is a significant relationship between respondents’ level of awareness and their practices regarding waterborne diseases, influenced by their age and the training they have received [37].
Most medical professionals in Al-Karkh, Baghdad, were well-versed in waterborne illnesses, particularly concerning prevention and symptoms. However, there are still gaps in knowledge regarding certain diseases and environmental factors. Apart from a positive correlation with attitudes, most demographic characteristics did not show any meaningful association with knowledge. We suggest focused training initiatives to address these gaps. The burden of waterborne illnesses can be reduced, and health interventions can be strengthened by increasing awareness through education.
Conclusion
The majority of medical professionals in Al-Karkh, Baghdad, are well-versed in waterborne illnesses, particularly concerning prevention and symptoms.
Acknowledgments: I would like to express my sincere thanks to all health providers across Baghdad Governorate who participated in this research and generously devoted their valuable time.
Ethical Permissions: Participants are fully informed about the research purpose, procedures, risks, and benefits, and they must voluntarily agree to participate.
Conflicts of Interests: The author acknowledges no conflict of interest in this study.
Authors' Contribution: Adil Z (First Author), Introduction Writer/Methodologist/Main Researcher (50%); AL-Sarray AM (Second Author), Assistant Researcher/Statistical Analyst (30%); Luma HA (Third Author), Discussion Writer/Statistical Analyst (20%)
Funding/Support: No funding was received.
Article Type: Descriptive & Survey |
Subject:
Healthy Life Style
Received: 2025/05/28 | Accepted: 2025/06/28 | Published: 2025/07/3
Received: 2025/05/28 | Accepted: 2025/06/28 | Published: 2025/07/3
References
1. WHO. Infectious diseases. Geneva: World Health Organization; 2015. [Link]
2. WHO. Diarrhoeal diseases [Internet]. Geneva: World Health Organization; 2017 [cited May 2, 2017]. Available from: https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease. [Link]
3. Chan EYY, Tong KHY, Dubois C, Mc Donnell K, Kim JH, Hung KKC, et al. Narrative review of primary preventive interventions against waterborne diseases: Scientific evidence of health-EDRM in contexts with inadequate safe drinking water. Int J Environ Res Public Health. 2021;18(23):12268. [Link] [DOI:10.3390/ijerph182312268]
4. Garrett V, Ogutu P, Mabonga P, Ombeki S, Mwaki A, Aluoch G, et al. Diarrhoea prevention in a high-risk rural Kenyan population through point-of-use chlorination, safe water storage, sanitation, and rainwater harvesting. Epidemiol Infect. 2008;136(11):1463-71. [Link] [DOI:10.1017/S095026880700026X]
5. Manetu WM, Karanja AM. Waterborne disease risk factors and intervention practices: A review. Open Access Libr J. 2021;8(5):1-11. [Link] [DOI:10.4236/oalib.1107401]
6. Shao GN, Imran S, Jeon SJ, Engole M, Abbas N, Haider MS, et al. Sol-gel synthesis of photoactive zirconia-titania from metal salts and investigation of their photocatalytic properties in the photodegradation of methylene blue. Powder Technol. 2014;258:99-109. [Link] [DOI:10.1016/j.powtec.2014.03.024]
7. Decker BK, Palmore TN. The role of water in healthcare-associated infections. Curr Opin Infect Dis. 2013;26(4):345-51. [Link] [DOI:10.1097/QCO.0b013e3283630adf]
8. Fadhl SA, Ali SI, Ali SM. Knowledge, attitude, and practices of infection control amongst medical staff. THI-QAR Med J. 2023;26(2):106-19. [Link]
9. Shayo GM, Elimbinzi E, Shao GN, Fabian C. Severity of waterborne diseases in developing countries and the effectiveness of ceramic filters for improving water quality. Bull Natl Res Cent. 2023;47(1):113. [Link] [DOI:10.1186/s42269-023-01088-9]
10. Omarova A, Tussupova K, Berndtsson R, Kalishev M, Sharapatova K. Protozoan parasites in drinking water: A system approach for improved water, sanitation and hygiene in developing countries. Int J Environ Res Public Health. 2018;15(3):495. [Link] [DOI:10.3390/ijerph15030495]
11. Mittal GC, Sundar RN, Prashanth A. Knowledge and practices of water and sanitation and prevention of waterborne diseases among the residents of Wabgaon village. Int J Community Med Public Health. 2023;10(2):729. [Link] [DOI:10.18203/2394-6040.ijcmph20230229]
12. Daniel WW, Cross CL. Biostatistics: A foundation for analysis in the health sciences. Hoboken: John Wiley & Sons; 2018. [Link]
13. Moor DS, McCabe GP, Craig BA. Introduction to the practice of statistics. 8th ed. New York: W. H. Freeman; 2014. [Link]
14. Celentano DD, Szklo M. Gordis epidemiology. 6th ed. Amsterdam: Elsevier; 2019. [Link]
15. Abd Elrazak HM, Elkazeh EAEE, Mohamed NM. Effect of the self learning module on knowledge and practices of health team regarding waterborne diseases. Int J Nov Res Healthc Nurs. 2018;5(3):607-27. [Link]
16. Balan V, Galhotra A, Shukla A. Knowledge attitude and practice of healthcare workers about water, sanitation, and hygiene in healthcare facilities in a district of central India. J Pharm Negat Results. 2023;14(2). [Link]
17. Bennett SD, Otieno R, Ayers TL, Odhiambo A, Faith SH, Quick R. Acceptability and use of portable drinking water and hand washing stations in health care facilities and their impact on patient hygiene practices, Western kenya. PLoS One. 2015;10(5):e0126916. [Link] [DOI:10.1371/journal.pone.0126916]
18. Ray S, Kamble S, Gaikwad P. Knowledge regarding selected water borne diseases among the class IV workers working in selected hospitals. Drugs Cell Ther Haematol. 2021;10(1):1061-6. [Link]
19. Samani LP, Mwanga J, Basinda N, Msaki E, Kadigi M. Assessment of knowledge, attitudes, and practices of community health workers on household sanitation and hygiene in rural Tanzania. Int J Trop Dis Health. 2025;46(4):64-83. [Link] [DOI:10.9734/ijtdh/2025/v46i41645]
20. Chaudhary P, Gopal L, Pant K, Pande A. Water borne diseases: Life threatening impact on maternal health. Int J Eng Adv Technol. 2020;8(4s):6-11. [Link] [DOI:10.35940/ijeat.D1002.0484S19]
21. Robertine LF, Payne VK, Honorine NT, Mounchili S, Saturine MM, Manjuh BR, et al. Trends of potential waterborne diseases at different health facilities in Bamboutos division, West region, Cameroon: A retrospective appraisal of routine data from 2013 to 2017. J Water Health. 2021;19(4):616-28. [Link] [DOI:10.2166/wh.2021.027]
22. Benova L, Cumming O, Campbell OM. Systematic review and meta-analysis: Association between water and sanitation environment and maternal mortality. Trop Med Int Health. 2014;19(4):368-87. [Link] [DOI:10.1111/tmi.12275]
23. Sambath V, Narayan S, Kumar P, Kumar P, Pradyumna A. Knowledge, attitudes and practices related to climate change and its health aspects among the healthcare workforce in India-A cross-sectional study. J Clim Change Health. 2022;6:100147. [Link] [DOI:10.1016/j.joclim.2022.100147]
24. Van Der Hoek W, Konradsen F, Ensink JH, Mudasser M, Jensen PK. Irrigation water as a source of drinking water: Is safe use possible?. Trop Med Int Health. 2001;6(1):46-54. [Link] [DOI:10.1046/j.1365-3156.2001.00671.x]
25. Alqato S, Fadhl HAN, Al-Bawah N, Abdulgadir A, Mohamed Amine H, Alsomali RH, et al. Knowledge, attitudes, and practices related to cholera outbreak among medical students in Aemen: A cross-sectional study. Cureus. 2025;17(2):e78885. [Link] [DOI:10.7759/cureus.78885]
26. Aquino RDV. Awareness and practices of barangay health workers to waterborne diseases: Basis for a proposed capability training plan. Puissant. 2024;5:1245-69. [Link]
27. Ray I, Smith KR. Towards safe drinking water and clean cooking for all. Lancet Glob Health. 2021;9(3):e361-5. [Link] [DOI:10.1016/S2214-109X(20)30476-9]
28. Shezad F, Mahsud N, Khan A, Ali J. Knowledge, attitude, and practices towards typhoid among health care professionals working in private clinics of district west Karachi. PalArchs J Archaeol Egypt Egyptol. 2023;20(2):1695-708. [Link]
29. Mudavanhu A, Weeda R, Anyolitho MK, Mlangeni L, Brendonck L, Manyangadze T, et al. Insufficient Water, Sanitation, and Healthcare Facilities Hinder Schistosomiasis Control in Endemic Areas: A Mixed Methods Study. medRxiv. 2024;2024-08.. [Link] [DOI:10.1101/2024.08.30.24312829]
30. Shamarina D, Sluga-O'Callaghan M, Kassianos G, Marijam A, Dave V, Davenport E, et al. Knowledge, attitudes, and practices of European healthcare professionals towards hepatitis a and hepatitis b vaccination in at-risk adults. Vaccines. 2023;11(11):1645. [Link] [DOI:10.3390/vaccines11111645]
31. Iglesias Hernández T, Almannoni SA, Rodríguez ME, Sánchez Valdés L, Pupo DM, Manzur Katrib J, et al. Knowledge, perceptions and practice of dermatologists with respect to Giardia lamblia infection. REVISTA CUBANA DE MEDICINA TROPICAL. 2010;62(1):36-41. [Spanish] [Link]
32. Galindo LF, Valdés LS, De Los Angeles Fernández Ferrer M, Iglesias HM, Goodridge IM, Galindo OF. Knowledge, believes and practices of physicians from Cienfuegos in relation to intestinal amebiasis: Results of an intervention. REVISTA CUBANA DE MEDICINA TROPICAL. 2003;55(3):185-90. [Link]
33. Haston JC, Ford L, Vanden Esschert KL, Plumb ID, Logan N, Francois Watkins LK, et al. Healthcare providers' knowledge and clinical practice surrounding shigellosis-DocStyles survey, 2020. BMC Prim Care. 2023;24(1):267. [Link] [DOI:10.1186/s12875-023-02213-3]
34. Youzbahshi L, Ayash A, Daher N. Assessing acute diarrhea awareness among Syrian private university medical students in Syria: A cross-sectional study. Research Square [Preprint]. 2022 [cited March 01, 2022]. Available from: https://www.researchsquare.com/article/rs-1404547/v1. [Link] [DOI:10.21203/rs.3.rs-1404547/v1]
35. Pandapatan MD, Dofitas MD, Gervasio MD, Dumlao MD. Knowledge, attitudes, and practices of barangay health workers in Marawi city regarding Hansen's disease. ACTA MEDICA PHILIPPINA. 2024;58(17):8-16. [Link] [DOI:10.47895/amp.v58i17.7474]
36. Mohammed S, Othman N, Hussein A, Jalal K. Knowledge, attitude and practice of health care workers in Sulaimani health facilities in relation to medical waste management. Kurd J Appl Res. 2017;2(2):143-50. [Link] [DOI:10.24017/science.2017.2.21]
37. Abu Shomar R, Zeitoun M, Elmanama A. Knowledge and perception of healthcare workers about safe water supplies and antibiotic-resistant bacteria at primary health care facilities in Gaza, Palestine. Israa Univ J Appl Sci. 2023;7(1):27-54. [Link] [DOI:10.52865/NOAN8231]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |