



Volume 13, Issue 2 (2025)
Health Educ Health Promot 2025, 13(2): 205-211 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nuriyah N, Rusdi M, Elfrida S, Effendi M. Effect of ENNOE Information Digitization Intervention on Knowledge and Adherence to HIV Treatment. Health Educ Health Promot 2025; 13 (2) :205-211
URL: http://hehp.modares.ac.ir/article-5-79330-en.html
URL: http://hehp.modares.ac.ir/article-5-79330-en.html
1- Department of Medical, Faculty of Mathematic and Science Programe, Jambi University, Jambi, Indonesia
2- Department of Chemistry Education, Faculty of Teacher Training and Education, Jambi University, Jambi, Indonesia
3- Department of Public Health Sciences, Health Polytechnic Ministry of Health Jambi, Jambi, Indonesia
2- Department of Chemistry Education, Faculty of Teacher Training and Education, Jambi University, Jambi, Indonesia
3- Department of Public Health Sciences, Health Polytechnic Ministry of Health Jambi, Jambi, Indonesia
Keywords: Health Literacy [MeSH], Medication Adherence [MeSH], HIV Infections [MeSH], Patient Education as Topic [MeSH]
Full-Text [PDF 613 kb]
(359 Downloads)
| Abstract (HTML) (624 Views)
Full-Text: (51 Views)
Introduction
Human immunodeficiency virus (HIV) is a pathogen that targets the human immune system and, if left untreated, can progress to acquired immunodeficiency syndrome (AIDS) [1, 2]. The virus replicates by utilizing T cells as host cells, leading to a progressive decline in immune function. Due to its prolonged asymptomatic phase, which can last five to ten years after initial exposure, early diagnosis remains a significant challenge in disease control efforts, underscoring the need for proactive screening and intervention strategies [3].
Globally, the number of individuals living with HIV continues to rise, with approximately 38.4 million people infected as of 2021, including 1.5 million new cases [4]. Epidemiological data indicate that HIV is predominantly concentrated among high-risk groups, such as men who have sex with men (MSM), people who inject drugs, and commercial sex workers [5, 6]. Additionally, geographical factors play a significant role in the spread of HIV, with certain countries and regions exhibiting higher prevalence rates than others [7].
In Indonesia, the number of HIV cases has risen significantly. As of June 2021, there were 303,993 reported HIV cases and 132,995 cases of AIDS. In Jambi Province, by September 2022, the number of HIV cases had reached 2,341, with 820 cases of AIDS [8]. However, the proportion of people living with HIV/AIDS (PLHIV) who remain on antiretroviral therapy (ART) is still relatively low, with only 26% of the total PLHIV actively undergoing treatment. This presents a significant challenge in improving patient adherence to therapy [9, 10].
One of the major barriers to effective HIV treatment is low patient adherence to ongoing ART. Several factors contribute to this issue, including social stigma, limited access to information, fear of drug side effects, and economic and geographical obstacles. Research indicates that many PLHIV face significant challenges in accessing healthcare services due to stigma and discrimination from both the community and healthcare providers. This results in a negative impact on loss to follow-up (LTFU) rates, where patients discontinue their treatment prematurely.
Several previous studies have explored the use of digital technology in health education, including mobile applications and online platforms, to improve ART adherence [11-13]. However, most existing digital interventions focus solely on delivering information without a comprehensive monitoring mechanism. Therefore, this study introduces the ENNOE method (engagement, education, monitoring, and adherence), which integrates digital education with adherence monitoring to provide a more holistic approach to supporting PLHIV.
The ENNOE method differs from previous digital interventions by incorporating four key components, including engagement, to enhance patient involvement in the educational process, education, as a needs-based information delivery tool, monitoring, to track the progress of patient knowledge and behavior, and adherence, which focuses on improving ART compliance. With this approach, ENNOE not only provides a digital education model that is adaptive and responsive to the needs of PLHIV but also contributes to more effective health behavior changes [14, 15].
Using an evidence-based approach, this study not only examined the feasibility and effectiveness of the ENNOE method but also sought to provide practical solutions to support the HIV/AIDS elimination program by 2030, in line with national and global targets. Therefore, this study aimed to analyze the impact of information digitization through the ENNOE method on improving knowledge and treatment adherence among PLHIV.
Materials and Methods
Study design
This study used a research and development (R&D) design, which integrates both qualitative and quantitative approaches. This methodology was used to develop and assess the effectiveness of information digitization based on the ENNOE method in improving knowledge and treatment adherence among PLHIV. The model development follows the ADDIE (analysis, design, development, implementation, and evaluation) framework to ensure the intervention’s effectiveness [16, 17]. During the media evaluation stage, a field trial was conducted using a one-group pre-test-post-test design approach.
Study setting
The research was conducted at four key health centers in Jambi City, including Rawasari Health Center, Simpang Kawat Health Center, Talang Bakung Health Center, and Putri Ayu Health Center, between April and June 2024. These sites were strategically selected based on their central role in providing care and treatment services for PLHIV in the region.
Subjects
The study population consisted of all PLHIV undergoing ART at the Jambi City Health Centers. A random sampling technique was used to select participants, with the sample size determined through power analysis to achieve a statistical power of 0.80 and an alpha level of 0.05, ensuring sufficient sensitivity to detect meaningful differences in knowledge and adherence levels. The inclusion criteria were PLHIV who had been undergoing ART for less than six months and were willing to participate. The exclusion criteria included PLHIV who declined to participate in the study. The field trial involved 30 respondents, who were proportionally selected from each health center in Jambi City. Participants were chosen until the total reached 30, ensuring an equal distribution across health centers to maintain the representativeness of the data.
Instrument
The International Standardized Questionnaire on HIV and AIDS Knowledge (HIV-KQ-18) has demonstrated validity and reliability in assessing HIV/AIDS knowledge across various populations, including those in Indonesia. Research conducted in Yogyakarta indicated that this instrument has a validity coefficient (r-xy) ranging from 0.177 to 0.564, exceeding the r-table value of 0.112, and high reliability, with a KR20 value of 0.763. Furthermore, the adaptation and validation of HIV-KQ-18 for the general Indonesian population have shown Cronbach’s alpha values ranging from 0.75 to 0.89, indicating good internal consistency [18].
The Adherence to Refills and Medications Scale (ARMS) has also proven valid and reliable for assessing patient adherence to medication, including in chronic disease contexts, like HIV. Research has shown that the ARMS performs well, even among patients with low literacy levels [19].
Data collection
The first step was the validation of the Digital Educational Media by Prof. Drs. Damris Muhammad, M.Sc., Ph.D., CIQaR, a conceptual/design expert from the Faculty of Science and Technology at Jambi University. He served as a validator during the expert validation process, assessing the concepts (theory-intervention-impact) in the conceptual paper titled “Digitalization of Information to Increase Knowledge and Adherence to Treatment in People with HIV/AIDS (ODHIV).” Following assessment and revisions, the digital educational media was deemed suitable for use.
Data collection was conducted using two primary approaches, including knowledge assessment and adherence monitoring. To evaluate the knowledge of PLHIV, the HIV-KQ-18, an instrument with established validity and reliability, was used. Knowledge data were gathered through pre- and post-intervention assessments, which aimed to measure changes in HIV/AIDS knowledge following the educational intervention.
Additionally, patient adherence to ART was monitored using a combination of the daily check method and the ARMS. The daily check method records daily medication adherence, while the ARMS measures long-term adherence based on prescription refills and medication compliance. Adherence data were also collected at both pre- and post-test intervals to assess any changes.
To handle missing data, a predefined protocol was established. If a participant missed a response in the questionnaire, multiple imputation was applied to estimate missing values based on the observed data. If a participant failed to complete more than 10% of the total questions, their data were excluded from the final analysis to maintain the validity of the results.
Data analysis
Data normality was assessed using the Shapiro-Wilk test, while homogeneity of variances was evaluated with Levene’s test. Based on the normality assumption test, it was concluded that the data followed a normal distribution and that homogeneity was met, allowing the use of parametric tests for power analysis. Additionally, missing data were handled through multiple imputations to reduce potential biases, and outliers were examined to assess their impact on the overall findings.
Data collected were analyzed using SPSS 23 software. Descriptive analysis was employed to characterize the respondents and assess their levels of knowledge and ART adherence before and after the intervention. Additionally, inferential statistical tests, including the chi-square test, were used to examine the association between risk factors and ART adherence, while paired t-tests were conducted to compare the levels of knowledge and adherence before and after the implementation of the ENNOE method. Cohen’s d analysis was applied to determine the magnitude of the difference in mean knowledge and adherence levels. A p-value of less than 0.05 was considered statistically significant.
Findings
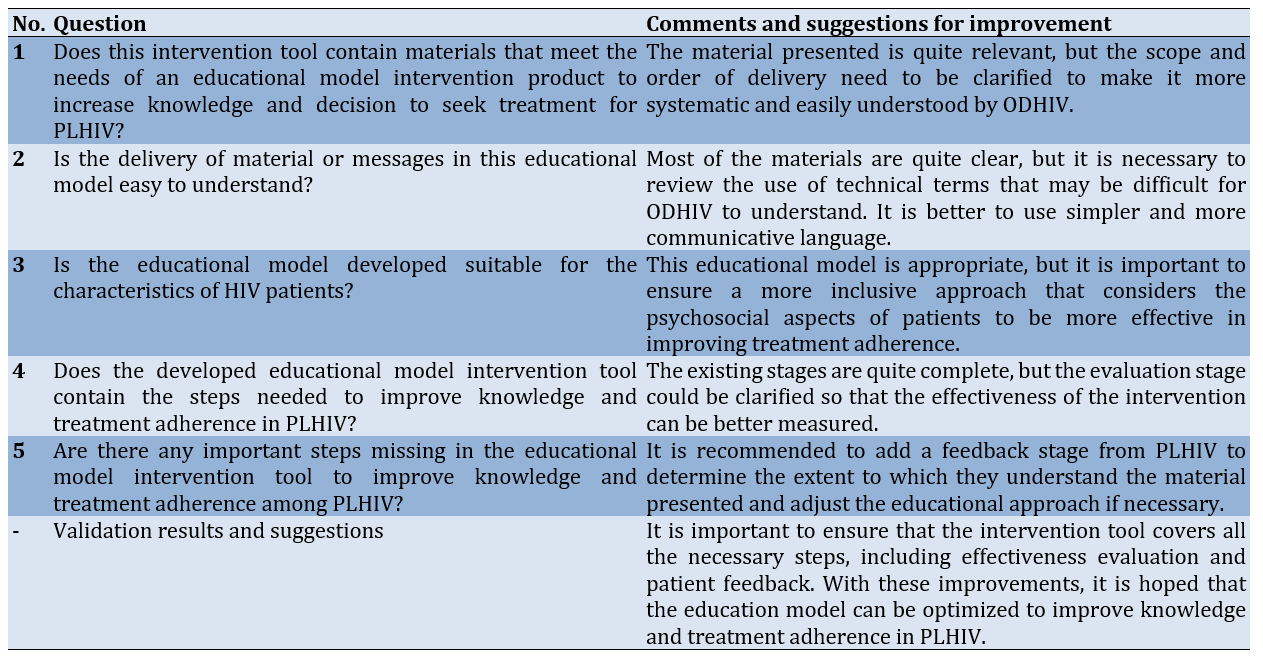
After revision based on expert suggestions to ensure that the intervention tool covered all necessary steps, including effectiveness evaluation and patient feedback, and the educational model was declared valid and is expected to be more effective in improving knowledge and treatment adherence among PLHIV (Tables 1 and 2).
Table 1. Conceptual/design expert responses (theory-intervention-impact) on the information digitization conceptual paper
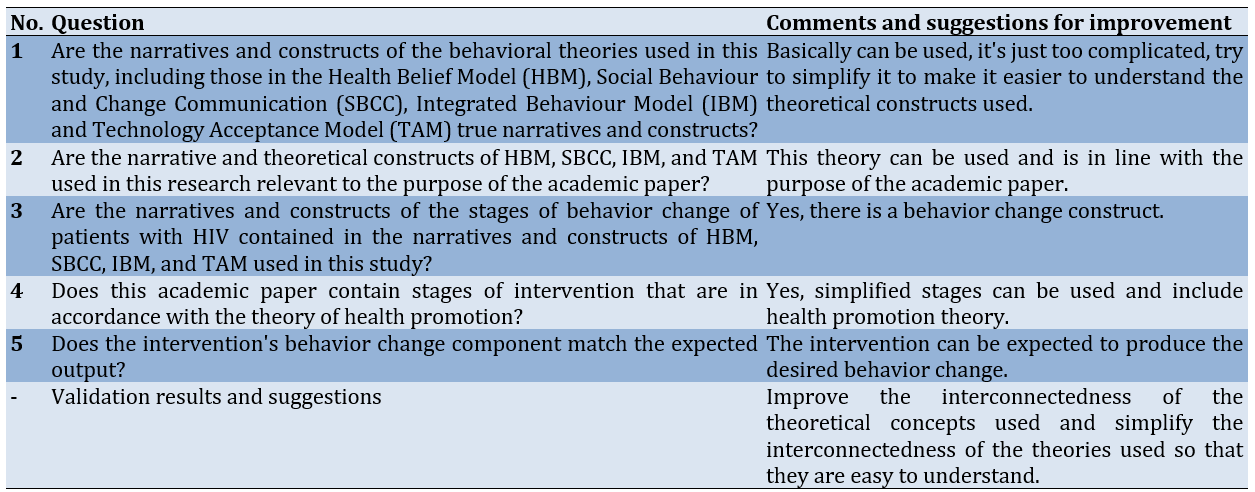
Table 2. Expert responses to public health conceptual (theory-intervention-impact) on the digitization conceptual paper
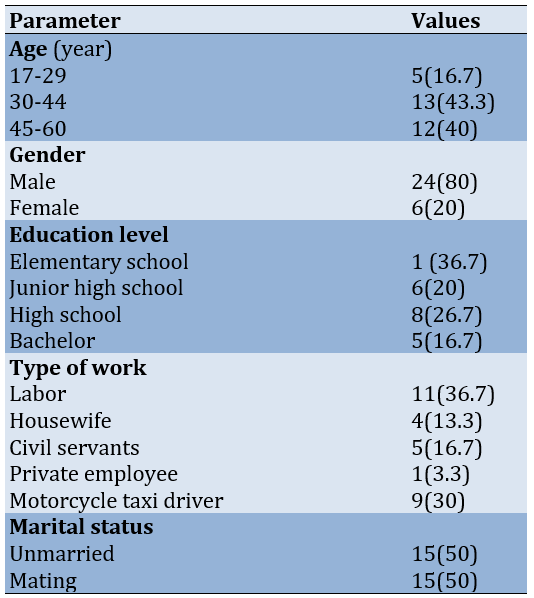
The mean age of subjects was 40.57±10.76 years and most were young to middle-aged males with primary or secondary education. The majority were working as laborers or motorcycle taxi drivers, while fewer were civil/private employees or housewives. Marital status was fairly evenly split between married and unmarried individuals (Table 3).
Table 3. Frequency of respondents’ characteristics
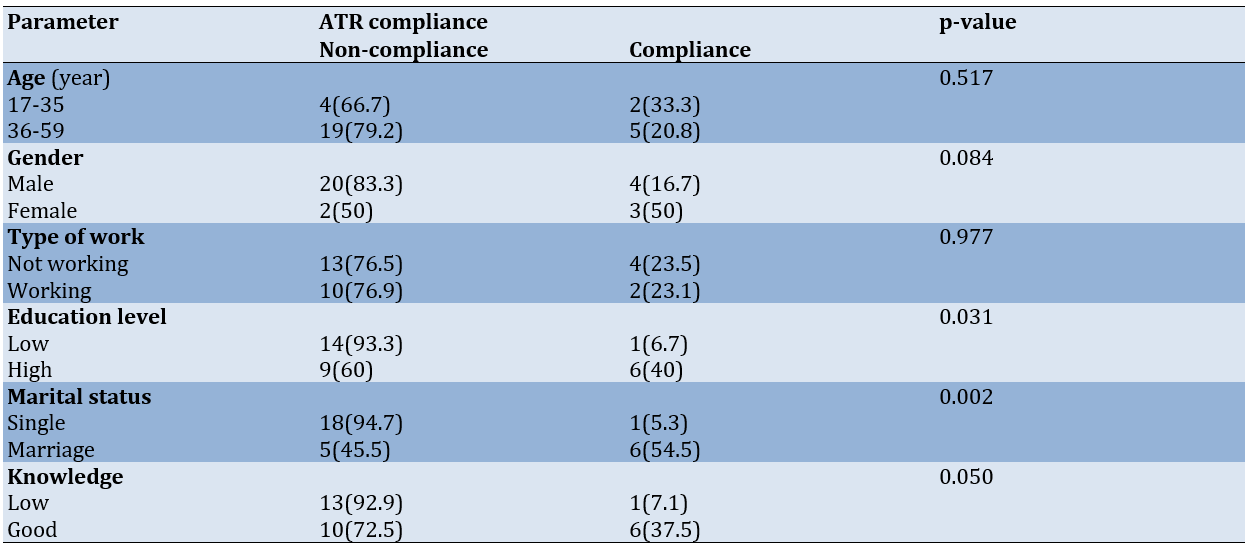
Age, gender, and occupation did not have a significant impact on ART adherence (p>0.05). However, education level emerged as an important factor, with individuals possessing lower education levels generally exhibiting lower adherence rates compared to those with higher education (p<0.05). Marital status also had a significant influence on adherence, with married individuals showing higher adherence rates (p<0.05). Furthermore, knowledge of ART was positively associated with adherence, as patients with a better understanding of the treatment were more likely to remain compliant (p<0.05; Table 4).
Table 4. Results of factor analysis of determinants of antiretroviral therapy (ART) adherence before the ENNOE information digitization intervention
For knowledge, there was a significant improvement between the pre-test and post-test scores, with the mean score increasing from 43 to 60.8. This improvement was statistically significant (p<0.05; Cohen’s d=3.01), reflecting the strong impact of the intervention on enhancing knowledge. Similarly, for medication adherence, a significant improvement was observed, with the mean score rising from 57.7 to 68.5. This change was also statistically significant (p<0.05; Cohen’s d=2.68), signifying a substantial increase in adherence following the intervention. In summary, both knowledge and adherence showed significant improvement, with the intervention producing strong positive effects on both outcomes (Table 5).
Table 5. Mean knowledge and ART medication adherence after the ENNOE information digitization intervention

Discussion
This study aimed to analyze the impact of information digitization through the ENNOE method on improving knowledge and treatment adherence among PLHIV. Analysis of the determinants of ART adherence before the intervention revealed that age, gender, and employment status did not significantly impact adherence. However, education level and marital status showed significant differences. Respondents with lower education levels were more likely to be non-adherent to therapy, with 93.3% not adhering to treatment, while those with higher education demonstrated higher adherence rates, with 40% adhering. This suggests that education may enhance awareness of the importance of medication adherence.
Marital status also played a significant role in ART adherence. Married respondents exhibited higher adherence rates, with 54.5% adhering to treatment, whereas unmarried individuals tended to be more non-adherent, with 94.7% not adhering. This indicates that social support, particularly from a spouse, may contribute to improved treatment adherence. Additionally, knowledge about ART was positively associated with adherence, as those with better knowledge were more likely to adhere to treatment. This underscores the importance of providing comprehensive information to patients to help them better understand and manage their treatment [20, 21].
One of the interesting findings in this study is the stronger influence of education on adherence compared to gender and employment status. One possible explanation is that individuals with higher levels of education may have better health literacy, enabling them to understand medical advice, recognize the risks of non-adherence, and manage their treatment more effectively. In contrast, gender and employment status do not show a significant relationship with adherence. This may be due to the fact that both male and female patients face similar adherence barriers, such as stigma, medication side effects, and forgetting to take their medication, regardless of their type of employment. Further studies are needed to explore whether job stability, income level, or work-related stress may have an indirect effect on ART adherence [22, 23].
In accordance with the study by Jin et al. [24], patient medication adherence is influenced by demographic factors such as higher education, marriage, and adequate knowledge. Patient education plays a crucial role in improving medication adherence. Counseling on the importance of consistent medication is essential for enhancing patient compliance. Some patients may perceive the need for medication as intermittent, leading them to discontinue treatment in an attempt to assess whether it is still necessary. Another study reported that some patients lack understanding of their therapeutic role in treatment [25] and lack knowledge about the disease and the consequences of poor adherence [26, 27].
The effectiveness of the ENNOE information digitization intervention in improving patient knowledge and adherence can be attributed to several key factors. Firstly, digitized information allows for the widespread distribution of educational materials that are easily accessible to patients. In the context of ART, a thorough understanding of the medication’s benefits, mode of action, and the importance of adherence is essential [28]. Through digital platforms, information can be delivered in diverse formats such as text, images, videos, and interactive animations, making it more engaging and easier to comprehend for patients with varying levels of education [29]. This approach helps address the limitations of traditional education methods, which often rely on verbal communication from health workers who have limited time [30].
Secondly, the ENNOE method used in information digitization facilitates a more personalized and patient-centered educational experience. Digital technology enables the delivery of content tailored to the individual’s health condition, level of understanding, and specific needs [31]. For instance, patients with limited knowledge of ART can be provided with simpler, more accessible materials, while those with a higher level of understanding can receive more detailed information. This customization enhances patient engagement in the education process, leading to increased motivation and improved adherence to their treatment [32].
Moreover, digitizing information using the ENNOE method provides patients with the flexibility to access educational materials anytime and anywhere. This feature is particularly beneficial for individuals who face time constraints or challenges in attending in-person education sessions at health facilities [33]. With the ability to access content via electronic devices such as mobile phones or computers, patients can engage with the material at their own pace and convenience. This level of accessibility also addresses geographical barriers, particularly for patients residing in remote areas or those with limited mobility. By offering this ease of access, patients are more likely to stay engaged with their education and gain a deeper understanding of the importance of adhering to ART [34, 35].
The ENNOE digital method further enhances patient engagement through interactive features, such as quizzes, discussion forums, and virtual Q&A sessions with healthcare professionals. These interactive elements not only help patients better grasp the educational content but also provide an opportunity to clarify any confusion or misconceptions about ART. Such active participation aids in information retention and strengthens patient trust in their treatment. Additionally, digital reminders, such as notifications or alarms, can further support patients by helping them stay on track with their medication schedules, thereby improving adherence [36].
Finally, the effectiveness of the ENNOE-based digital intervention is also linked to an increase in patients’ confidence and autonomy in managing their treatment. Access to accurate and easily comprehensible information empowers patients to make informed decisions about their health. Improved education also reduces the fear and stigma often associated with ART, motivating patients to remain consistent with their therapy. In this way, the ENNOE method not only enhances patient knowledge but also fosters positive behavioral changes that contribute to better ART adherence [11].
Although the findings of this study provide valuable insights, several limitations should be considered. First, the relatively small sample size may limit the generalizability of the results to a broader population. A larger sample in future studies would help confirm these findings and enhance the robustness of statistical analyses. Second, this study was conducted in a single urban setting, which may restrict its applicability to rural populations, where access to digital health interventions and healthcare facilities may differ. Further research should compare ART adherence patterns in urban and rural settings to identify unique barriers and opportunities for more effective interventions. Third, potential biases may affect the study results. Social desirability bias may lead participants to report higher adherence than is accurate, while recall bias could impact the accuracy of self-reported knowledge levels. Using more objective adherence measurement methods, such as electronic medication monitoring, could improve data accuracy in future research.
Accordingly, the integration of the ENNOE method into the national digital health policy is recommended as a scalable and cost-effective solution to improve ART adherence and treatment outcomes for PLHIV. This integration should include the implementation of digital training for health educators to enhance patient understanding, funding allocation by policymakers to ensure the accessibility of digital health programs, and the use of ENNOE by patients for self-monitoring and more effective adherence tracking. A digitized educational approach serves as a valuable strategy for improving patients’ understanding of ART and promoting better adherence. This method provides accessible, engaging, and personalized educational content that supports patients in managing their treatment. Given its effectiveness, integrating similar digital interventions into healthcare services can contribute to better treatment outcomes and long-term therapeutic success for individuals living with HIV/AIDS.
Conclusion
The ENNOE information digitization intervention is effective in enhancing patient knowledge and adherence to treatment.
Acknowledgments: Gratitude is expressed to all those who contributed to this research, especially to the Dean of the Faculty of Mathematics and Natural Sciences Education at Jambi University, who provided significant support. We also appreciate the respondents who took the time to provide valuable information in this survey. Additionally, we thank the Puskesmas, private clinics, and independent practicing physicians who facilitated data collection by serving as research locations.
Ethical Permissions: This research obtained a letter of permission to conduct the study from the research ethics committee of Universitas Jambi, Indonesia (Number: 575/UN21.8/PT.01.04/2024), and all participants signed an informed consent form prior to data collection.
Conflicts of Interests: The authors declared no conflicts of interests.
Authors' Contribution: Nuriyah N (First Author), Introduction Writer/Main Researcher/Discussion Writer/Statistical Analyst (40%); Rusdi M (Second Author), Methodologist/Assistant Researcher/Statistical Analyst (20%); Elfrida S (Third Author), Introduction Writer/Methodologist/Assistant Researcher (20%); Effendi MH (Fourth Author), Assistant Researcher/Discussion Writer/Statistical Analyst 20%)
Funding/Support: No funding or financial support was received for the implementation of this activity.
Human immunodeficiency virus (HIV) is a pathogen that targets the human immune system and, if left untreated, can progress to acquired immunodeficiency syndrome (AIDS) [1, 2]. The virus replicates by utilizing T cells as host cells, leading to a progressive decline in immune function. Due to its prolonged asymptomatic phase, which can last five to ten years after initial exposure, early diagnosis remains a significant challenge in disease control efforts, underscoring the need for proactive screening and intervention strategies [3].
Globally, the number of individuals living with HIV continues to rise, with approximately 38.4 million people infected as of 2021, including 1.5 million new cases [4]. Epidemiological data indicate that HIV is predominantly concentrated among high-risk groups, such as men who have sex with men (MSM), people who inject drugs, and commercial sex workers [5, 6]. Additionally, geographical factors play a significant role in the spread of HIV, with certain countries and regions exhibiting higher prevalence rates than others [7].
In Indonesia, the number of HIV cases has risen significantly. As of June 2021, there were 303,993 reported HIV cases and 132,995 cases of AIDS. In Jambi Province, by September 2022, the number of HIV cases had reached 2,341, with 820 cases of AIDS [8]. However, the proportion of people living with HIV/AIDS (PLHIV) who remain on antiretroviral therapy (ART) is still relatively low, with only 26% of the total PLHIV actively undergoing treatment. This presents a significant challenge in improving patient adherence to therapy [9, 10].
One of the major barriers to effective HIV treatment is low patient adherence to ongoing ART. Several factors contribute to this issue, including social stigma, limited access to information, fear of drug side effects, and economic and geographical obstacles. Research indicates that many PLHIV face significant challenges in accessing healthcare services due to stigma and discrimination from both the community and healthcare providers. This results in a negative impact on loss to follow-up (LTFU) rates, where patients discontinue their treatment prematurely.
Several previous studies have explored the use of digital technology in health education, including mobile applications and online platforms, to improve ART adherence [11-13]. However, most existing digital interventions focus solely on delivering information without a comprehensive monitoring mechanism. Therefore, this study introduces the ENNOE method (engagement, education, monitoring, and adherence), which integrates digital education with adherence monitoring to provide a more holistic approach to supporting PLHIV.
The ENNOE method differs from previous digital interventions by incorporating four key components, including engagement, to enhance patient involvement in the educational process, education, as a needs-based information delivery tool, monitoring, to track the progress of patient knowledge and behavior, and adherence, which focuses on improving ART compliance. With this approach, ENNOE not only provides a digital education model that is adaptive and responsive to the needs of PLHIV but also contributes to more effective health behavior changes [14, 15].
Using an evidence-based approach, this study not only examined the feasibility and effectiveness of the ENNOE method but also sought to provide practical solutions to support the HIV/AIDS elimination program by 2030, in line with national and global targets. Therefore, this study aimed to analyze the impact of information digitization through the ENNOE method on improving knowledge and treatment adherence among PLHIV.
Materials and Methods
Study design
This study used a research and development (R&D) design, which integrates both qualitative and quantitative approaches. This methodology was used to develop and assess the effectiveness of information digitization based on the ENNOE method in improving knowledge and treatment adherence among PLHIV. The model development follows the ADDIE (analysis, design, development, implementation, and evaluation) framework to ensure the intervention’s effectiveness [16, 17]. During the media evaluation stage, a field trial was conducted using a one-group pre-test-post-test design approach.
Study setting
The research was conducted at four key health centers in Jambi City, including Rawasari Health Center, Simpang Kawat Health Center, Talang Bakung Health Center, and Putri Ayu Health Center, between April and June 2024. These sites were strategically selected based on their central role in providing care and treatment services for PLHIV in the region.
Subjects
The study population consisted of all PLHIV undergoing ART at the Jambi City Health Centers. A random sampling technique was used to select participants, with the sample size determined through power analysis to achieve a statistical power of 0.80 and an alpha level of 0.05, ensuring sufficient sensitivity to detect meaningful differences in knowledge and adherence levels. The inclusion criteria were PLHIV who had been undergoing ART for less than six months and were willing to participate. The exclusion criteria included PLHIV who declined to participate in the study. The field trial involved 30 respondents, who were proportionally selected from each health center in Jambi City. Participants were chosen until the total reached 30, ensuring an equal distribution across health centers to maintain the representativeness of the data.
Instrument
The International Standardized Questionnaire on HIV and AIDS Knowledge (HIV-KQ-18) has demonstrated validity and reliability in assessing HIV/AIDS knowledge across various populations, including those in Indonesia. Research conducted in Yogyakarta indicated that this instrument has a validity coefficient (r-xy) ranging from 0.177 to 0.564, exceeding the r-table value of 0.112, and high reliability, with a KR20 value of 0.763. Furthermore, the adaptation and validation of HIV-KQ-18 for the general Indonesian population have shown Cronbach’s alpha values ranging from 0.75 to 0.89, indicating good internal consistency [18].
The Adherence to Refills and Medications Scale (ARMS) has also proven valid and reliable for assessing patient adherence to medication, including in chronic disease contexts, like HIV. Research has shown that the ARMS performs well, even among patients with low literacy levels [19].
Data collection
The first step was the validation of the Digital Educational Media by Prof. Drs. Damris Muhammad, M.Sc., Ph.D., CIQaR, a conceptual/design expert from the Faculty of Science and Technology at Jambi University. He served as a validator during the expert validation process, assessing the concepts (theory-intervention-impact) in the conceptual paper titled “Digitalization of Information to Increase Knowledge and Adherence to Treatment in People with HIV/AIDS (ODHIV).” Following assessment and revisions, the digital educational media was deemed suitable for use.
Data collection was conducted using two primary approaches, including knowledge assessment and adherence monitoring. To evaluate the knowledge of PLHIV, the HIV-KQ-18, an instrument with established validity and reliability, was used. Knowledge data were gathered through pre- and post-intervention assessments, which aimed to measure changes in HIV/AIDS knowledge following the educational intervention.
Additionally, patient adherence to ART was monitored using a combination of the daily check method and the ARMS. The daily check method records daily medication adherence, while the ARMS measures long-term adherence based on prescription refills and medication compliance. Adherence data were also collected at both pre- and post-test intervals to assess any changes.
To handle missing data, a predefined protocol was established. If a participant missed a response in the questionnaire, multiple imputation was applied to estimate missing values based on the observed data. If a participant failed to complete more than 10% of the total questions, their data were excluded from the final analysis to maintain the validity of the results.
Data analysis
Data normality was assessed using the Shapiro-Wilk test, while homogeneity of variances was evaluated with Levene’s test. Based on the normality assumption test, it was concluded that the data followed a normal distribution and that homogeneity was met, allowing the use of parametric tests for power analysis. Additionally, missing data were handled through multiple imputations to reduce potential biases, and outliers were examined to assess their impact on the overall findings.
Data collected were analyzed using SPSS 23 software. Descriptive analysis was employed to characterize the respondents and assess their levels of knowledge and ART adherence before and after the intervention. Additionally, inferential statistical tests, including the chi-square test, were used to examine the association between risk factors and ART adherence, while paired t-tests were conducted to compare the levels of knowledge and adherence before and after the implementation of the ENNOE method. Cohen’s d analysis was applied to determine the magnitude of the difference in mean knowledge and adherence levels. A p-value of less than 0.05 was considered statistically significant.
Findings
After revision based on expert suggestions to ensure that the intervention tool covered all necessary steps, including effectiveness evaluation and patient feedback, and the educational model was declared valid and is expected to be more effective in improving knowledge and treatment adherence among PLHIV (Tables 1 and 2).
Table 1. Conceptual/design expert responses (theory-intervention-impact) on the information digitization conceptual paper
Table 2. Expert responses to public health conceptual (theory-intervention-impact) on the digitization conceptual paper
The mean age of subjects was 40.57±10.76 years and most were young to middle-aged males with primary or secondary education. The majority were working as laborers or motorcycle taxi drivers, while fewer were civil/private employees or housewives. Marital status was fairly evenly split between married and unmarried individuals (Table 3).
Table 3. Frequency of respondents’ characteristics
Age, gender, and occupation did not have a significant impact on ART adherence (p>0.05). However, education level emerged as an important factor, with individuals possessing lower education levels generally exhibiting lower adherence rates compared to those with higher education (p<0.05). Marital status also had a significant influence on adherence, with married individuals showing higher adherence rates (p<0.05). Furthermore, knowledge of ART was positively associated with adherence, as patients with a better understanding of the treatment were more likely to remain compliant (p<0.05; Table 4).
Table 4. Results of factor analysis of determinants of antiretroviral therapy (ART) adherence before the ENNOE information digitization intervention
For knowledge, there was a significant improvement between the pre-test and post-test scores, with the mean score increasing from 43 to 60.8. This improvement was statistically significant (p<0.05; Cohen’s d=3.01), reflecting the strong impact of the intervention on enhancing knowledge. Similarly, for medication adherence, a significant improvement was observed, with the mean score rising from 57.7 to 68.5. This change was also statistically significant (p<0.05; Cohen’s d=2.68), signifying a substantial increase in adherence following the intervention. In summary, both knowledge and adherence showed significant improvement, with the intervention producing strong positive effects on both outcomes (Table 5).
Table 5. Mean knowledge and ART medication adherence after the ENNOE information digitization intervention
Discussion
This study aimed to analyze the impact of information digitization through the ENNOE method on improving knowledge and treatment adherence among PLHIV. Analysis of the determinants of ART adherence before the intervention revealed that age, gender, and employment status did not significantly impact adherence. However, education level and marital status showed significant differences. Respondents with lower education levels were more likely to be non-adherent to therapy, with 93.3% not adhering to treatment, while those with higher education demonstrated higher adherence rates, with 40% adhering. This suggests that education may enhance awareness of the importance of medication adherence.
Marital status also played a significant role in ART adherence. Married respondents exhibited higher adherence rates, with 54.5% adhering to treatment, whereas unmarried individuals tended to be more non-adherent, with 94.7% not adhering. This indicates that social support, particularly from a spouse, may contribute to improved treatment adherence. Additionally, knowledge about ART was positively associated with adherence, as those with better knowledge were more likely to adhere to treatment. This underscores the importance of providing comprehensive information to patients to help them better understand and manage their treatment [20, 21].
One of the interesting findings in this study is the stronger influence of education on adherence compared to gender and employment status. One possible explanation is that individuals with higher levels of education may have better health literacy, enabling them to understand medical advice, recognize the risks of non-adherence, and manage their treatment more effectively. In contrast, gender and employment status do not show a significant relationship with adherence. This may be due to the fact that both male and female patients face similar adherence barriers, such as stigma, medication side effects, and forgetting to take their medication, regardless of their type of employment. Further studies are needed to explore whether job stability, income level, or work-related stress may have an indirect effect on ART adherence [22, 23].
In accordance with the study by Jin et al. [24], patient medication adherence is influenced by demographic factors such as higher education, marriage, and adequate knowledge. Patient education plays a crucial role in improving medication adherence. Counseling on the importance of consistent medication is essential for enhancing patient compliance. Some patients may perceive the need for medication as intermittent, leading them to discontinue treatment in an attempt to assess whether it is still necessary. Another study reported that some patients lack understanding of their therapeutic role in treatment [25] and lack knowledge about the disease and the consequences of poor adherence [26, 27].
The effectiveness of the ENNOE information digitization intervention in improving patient knowledge and adherence can be attributed to several key factors. Firstly, digitized information allows for the widespread distribution of educational materials that are easily accessible to patients. In the context of ART, a thorough understanding of the medication’s benefits, mode of action, and the importance of adherence is essential [28]. Through digital platforms, information can be delivered in diverse formats such as text, images, videos, and interactive animations, making it more engaging and easier to comprehend for patients with varying levels of education [29]. This approach helps address the limitations of traditional education methods, which often rely on verbal communication from health workers who have limited time [30].
Secondly, the ENNOE method used in information digitization facilitates a more personalized and patient-centered educational experience. Digital technology enables the delivery of content tailored to the individual’s health condition, level of understanding, and specific needs [31]. For instance, patients with limited knowledge of ART can be provided with simpler, more accessible materials, while those with a higher level of understanding can receive more detailed information. This customization enhances patient engagement in the education process, leading to increased motivation and improved adherence to their treatment [32].
Moreover, digitizing information using the ENNOE method provides patients with the flexibility to access educational materials anytime and anywhere. This feature is particularly beneficial for individuals who face time constraints or challenges in attending in-person education sessions at health facilities [33]. With the ability to access content via electronic devices such as mobile phones or computers, patients can engage with the material at their own pace and convenience. This level of accessibility also addresses geographical barriers, particularly for patients residing in remote areas or those with limited mobility. By offering this ease of access, patients are more likely to stay engaged with their education and gain a deeper understanding of the importance of adhering to ART [34, 35].
The ENNOE digital method further enhances patient engagement through interactive features, such as quizzes, discussion forums, and virtual Q&A sessions with healthcare professionals. These interactive elements not only help patients better grasp the educational content but also provide an opportunity to clarify any confusion or misconceptions about ART. Such active participation aids in information retention and strengthens patient trust in their treatment. Additionally, digital reminders, such as notifications or alarms, can further support patients by helping them stay on track with their medication schedules, thereby improving adherence [36].
Finally, the effectiveness of the ENNOE-based digital intervention is also linked to an increase in patients’ confidence and autonomy in managing their treatment. Access to accurate and easily comprehensible information empowers patients to make informed decisions about their health. Improved education also reduces the fear and stigma often associated with ART, motivating patients to remain consistent with their therapy. In this way, the ENNOE method not only enhances patient knowledge but also fosters positive behavioral changes that contribute to better ART adherence [11].
Although the findings of this study provide valuable insights, several limitations should be considered. First, the relatively small sample size may limit the generalizability of the results to a broader population. A larger sample in future studies would help confirm these findings and enhance the robustness of statistical analyses. Second, this study was conducted in a single urban setting, which may restrict its applicability to rural populations, where access to digital health interventions and healthcare facilities may differ. Further research should compare ART adherence patterns in urban and rural settings to identify unique barriers and opportunities for more effective interventions. Third, potential biases may affect the study results. Social desirability bias may lead participants to report higher adherence than is accurate, while recall bias could impact the accuracy of self-reported knowledge levels. Using more objective adherence measurement methods, such as electronic medication monitoring, could improve data accuracy in future research.
Accordingly, the integration of the ENNOE method into the national digital health policy is recommended as a scalable and cost-effective solution to improve ART adherence and treatment outcomes for PLHIV. This integration should include the implementation of digital training for health educators to enhance patient understanding, funding allocation by policymakers to ensure the accessibility of digital health programs, and the use of ENNOE by patients for self-monitoring and more effective adherence tracking. A digitized educational approach serves as a valuable strategy for improving patients’ understanding of ART and promoting better adherence. This method provides accessible, engaging, and personalized educational content that supports patients in managing their treatment. Given its effectiveness, integrating similar digital interventions into healthcare services can contribute to better treatment outcomes and long-term therapeutic success for individuals living with HIV/AIDS.
Conclusion
The ENNOE information digitization intervention is effective in enhancing patient knowledge and adherence to treatment.
Acknowledgments: Gratitude is expressed to all those who contributed to this research, especially to the Dean of the Faculty of Mathematics and Natural Sciences Education at Jambi University, who provided significant support. We also appreciate the respondents who took the time to provide valuable information in this survey. Additionally, we thank the Puskesmas, private clinics, and independent practicing physicians who facilitated data collection by serving as research locations.
Ethical Permissions: This research obtained a letter of permission to conduct the study from the research ethics committee of Universitas Jambi, Indonesia (Number: 575/UN21.8/PT.01.04/2024), and all participants signed an informed consent form prior to data collection.
Conflicts of Interests: The authors declared no conflicts of interests.
Authors' Contribution: Nuriyah N (First Author), Introduction Writer/Main Researcher/Discussion Writer/Statistical Analyst (40%); Rusdi M (Second Author), Methodologist/Assistant Researcher/Statistical Analyst (20%); Elfrida S (Third Author), Introduction Writer/Methodologist/Assistant Researcher (20%); Effendi MH (Fourth Author), Assistant Researcher/Discussion Writer/Statistical Analyst 20%)
Funding/Support: No funding or financial support was received for the implementation of this activity.
Article Type: Original Research |
Subject:
Technology of Health Education
Received: 2025/01/26 | Accepted: 2025/02/24 | Published: 2025/04/25
Received: 2025/01/26 | Accepted: 2025/02/24 | Published: 2025/04/25
References
1. Prabhu SR, Van Wagoner N. Human immunodeficiency virus infection and acquired immunodeficiency syndrome (HIV/AIDS): An overview. In: Sexually transmissible oral diseases. Hoboken: Wiley Online Library; 2023. p. 51-71. [Link] [DOI:10.1002/9781119826781.ch5]
2. Gillespie SL, Chinen J, Paul ME, Shearer WT. Human immunodeficiency virus infection and acquired immunodeficiency syndrome. In: Clinical immunology. Amsterdam: Elsevier; 2019. p. 545-60. [Link] [DOI:10.1016/B978-0-7020-6896-6.00039-9]
3. Guatelli JC, Siliciano RF, Kuritzkes DR, Richman DD. Human immunodeficiency virus. In: Clinical virology. Hoboken: Wiley Online Library; 2009. p. 737-83. [Link] [DOI:10.1128/9781555815981.ch33]
4. Mwende Wairimu G. The global burden of HIV and progress toward the 2030 UNAIDS targets: A comprehensive review. Res Output J Public Health Med. 2024;3(3):46-51. [Link] [DOI:10.59298/ROJPHM/2024/334651]
5. Papworth E, Ceesay N, An L, Thiam‐Niangoin M, Ky‐Zerbo O, Holland C, et al. Epidemiology of HIV among female sex workers, their clients, men who have sex with men and people who inject drugs in West and Central Africa. J Int AIDS Soc. 2013;16(4 Suppl 3):18751. [Link] [DOI:10.7448/IAS.16.4.18751]
6. Baral SD, Friedman MR, Geibel S, Rebe K, Bozhinov B, Diouf D, et al. Male sex workers: Practices, contexts, and vulnerabilities for HIV acquisition and transmission. Lancet. 2015;385(9964):260-73. [Link] [DOI:10.1016/S0140-6736(14)60801-1]
7. Baral SD, Grosso A, Holland C, Papworth E. The epidemiology of HIV among men who have sex with men in countries with generalized HIV epidemics. Curr Opin HIV AIDS. 2014;9(2):156-67. [Link] [DOI:10.1097/COH.0000000000000037]
8. Kemenkes. 2023 Basic Health Research Report [Internet]. Jakarta: Kemenkes; 2023 [cited 2024, Desember,12]. Available from: https://www.badankebijakan.kemkes.go.id/laporan-hasil-survei/. [Indonesian] [Link]
9. Xuan Tran B, Thanh Nguyen L, Hoang Nguyen N, Van Hoang Q. Determinants of antiretroviral treatment adherence among HIV/AIDS patients: A multisite study. Glob Health Action. 2013;6(1):19570. [Link] [DOI:10.3402/gha.v6i0.19570]
10. Stricker SM, Fox KA, Baggaley R, Negussie E, De Pee S, Grede N, et al. Retention in care and adherence to ART are critical elements of HIV care interventions. AIDS Behav. 2014;18:465-75. [Link] [DOI:10.1007/s10461-013-0598-6]
11. Duthely LM, Sanchez-Covarrubias AP. Digitized HIV/AIDS treatment adherence interventions: A review of recent SMS/texting mobile health applications and implications for theory and practice. Front Commun. 2020;5:530164. [Link] [DOI:10.3389/fcomm.2020.530164]
12. Castano PM, Stockwell MS, Malbon KM. Using digital technologies to improve treatment adherence. Clin Obstet Gynecol. 2013;56(3):434-45. [Link] [DOI:10.1097/GRF.0b013e3182988a3b]
13. Calthorpe RJ, Smith S, Gathercole K, Smyth AR. Using digital technology for home monitoring, adherence and self-management in cystic fibrosis: A state-of-the-art review. Thorax. 2020;75(1):72-7. [Link] [DOI:10.1136/thoraxjnl-2019-213233]
14. Peltzer K, Friend-du Preez N, Ramlagan S, Anderson J. Antiretroviral treatment adherence among HIV patients in KwaZulu-Natal, South Africa. BMC Public Health. 2010;10:111. [Link] [DOI:10.1186/1471-2458-10-111]
15. Youn B, Shireman TI, Lee Y, Galárraga O, Wilson IB. Trends in medication adherence in HIV patients in the US, 2001 to 2012: An observational cohort study. J Int AIDS Soc. 2019;22(8):e25382. [Link] [DOI:10.1002/jia2.25382]
16. Cotter S, Yamamoto J, Stevenson C. A systematic characterization of food safety training interventions using the analyze, design, develop, implement, evaluate (ADDIE) instructional design framework. Food Control. 2023;145:109415. [Link] [DOI:10.1016/j.foodcont.2022.109415]
17. Mdodana-Zide L. Using ADDIE model for scaffolded learning and teaching intervention. Interdiscip J Educ Res. 2024;6:1-15. [Link] [DOI:10.38140/ijer-2024.vol6.28]
18. Arifin B, Rokhman MR, Zulkarnain Z, Perwitasari DA, Manggau M, Rauf S, et al. Adaptation and validation of the HIV knowledge questionnaire-18 for the general population of Indonesia. Health Qual Life Outcomes. 2022;20(1):55. [Link] [DOI:10.1186/s12955-022-01963-5]
19. Kripalani S, Risser J, Gatti ME, Jacobson TA. Development and evaluation of the Adherence to Refills and Medications Scale (ARMS) among low-literacy patients with chronic disease. Value Health. 2009;12(1):118-23. [Link] [DOI:10.1111/j.1524-4733.2008.00400.x]
20. Yusuf AB. Adherence to ART among HIV infected female sex workers in Nigeria [dissertation]. Minneapolis: Walden University; 2019. [Link]
21. Simelane P, Amoateng AY, Soogun AO. Socio-demographic correlates of non-adherence to anti-retroviral therapy (ART) at a health clinic in Mpumalanga province, South Africa. Infect Dis trop Med. 2023;9:e1122. [Link]
22. Campbell LS, Knight L, Masquillier C, Wouters E. Including the household: Individual, community and household factors affecting antiretroviral therapy adherence after ART initiation in Cape town, South Africa. AIDS Behav. 2024;28(11):3733-47. [Link] [DOI:10.1007/s10461-024-04447-3]
23. Simelane TP. Socio-demographic factors affecting adherence to antiretroviral therapy in a wellness centre in South Africa. Potchefstroom: North-West University; 2019. [Link]
24. Jin J, Sklar GE, Min Sen Oh V, Chuen Li S. Factors affecting therapeutic compliance: A review from the patient's perspective. Ther Clin Risk Manag. 2008;4(1):269-86. [Link] [DOI:10.2147/TCRM.S1458]
25. Ponnusankar S, Surulivelrajan M, Anandamoorthy N, Suresh B. Assessment of impact of medication counseling on patients' medication knowledge and compliance in an outpatient clinic in South India. Patient Educ Couns. 2004;54(1):55-60. [Link] [DOI:10.1016/S0738-3991(03)00193-9]
26. Alm-Roijer C, Stagmo M, Udén G, Erhardt L. Better knowledge improves adherence to lifestyle changes and medication in patients with coronary heart disease. Eur J Cardiovasc Nurs. 2004;3(4):321-30. [Link] [DOI:10.1016/j.ejcnurse.2004.05.002]
27. Gascon JJ, Sánchez-Ortuño M, Llor B, Skidmore D, Saturno PJ. Why hypertensive patients do not comply with the treatment: Results from a qualitative study. Fam Pract. 2004;21(2):125-30. [Link] [DOI:10.1093/fampra/cmh202]
28. Whiteley LB, Olsen EM, Haubrick KK, Odoom E, Tarantino N, Brown LK. A review of interventions to enhance HIV medication adherence. Curr HIV/AIDS Rep. 2021;18(5):443-57. [Link] [DOI:10.1007/s11904-021-00568-9]
29. Cao B, Gupta S, Wang J, Hightow-Weidman LB, Muessig KE, Tang W, et al. Social media interventions to promote HIV testing, linkage, adherence, and retention: Systematic review and meta-analysis. J Med Internet Res. 2017;19(11):e394. [Link] [DOI:10.2196/jmir.7997]
30. Yardley L, Morrison L, Bradbury K, Muller I. The person-based approach to intervention development: Application to digital health-related behavior change interventions. J Med Internet Res. 2015;17(1):e30. [Link] [DOI:10.2196/jmir.4055]
31. Wang Z, Zhu Y, Cui L, Qu B. Electronic health interventions to improve adherence to antiretroviral therapy in people living with HIV: Systematic review and meta-analysis. JMIR mHealth uHealth. 2019;7(10):e14404. [Link] [DOI:10.2196/14404]
32. Street RL, Gold WR, Manning TR. Health promotion and interactive technology: Theoretical applications and future directions. London: Routledge; 2013. [Link] [DOI:10.4324/9780203811047]
33. Maloney KM, Bratcher A, Wilkerson R, Sullivan PS. Electronic and other new media technology interventions for HIV care and prevention: A systematic review. J Int AIDS Soc. 2020;23(1):e25439. [Link] [DOI:10.1002/jia2.25439]
34. Haberer JE, Sabin L, Amico KR, Orrell C, Galárraga O, Tsai AC, et al. Improving antiretroviral therapy adherence in resource‐limited settings at scale: A discussion of interventions and recommendations. J Int AIDS Soc. 2017;20(1):21371. [Link] [DOI:10.7448/IAS.20.1.21371]
35. Castel AD, Qasmieh S, Greenberg D, Ellenberger N, Howell TH, Griffith C, et al. Digital gaming to improve adherence among adolescents and young adults living with HIV: Mixed-methods study to test feasibility and acceptability. JMIR Serious Games. 2018;6(4):e10213. [Link] [DOI:10.2196/10213]
36. Daher J, Vijh R, Linthwaite B, Dave S, Kim J, Dheda K, et al. Do digital innovations for HIV and sexually transmitted infections work? Results from a systematic review (1996-2017). BMJ Open. 2017;7(11):e017604. [Link] [DOI:10.1136/bmjopen-2017-017604]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |