



Volume 13, Issue 1 (2025)
Health Educ Health Promot 2025, 13(1): 111-118 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Budiono I, Fauzi L, Kanthawee P, Yasari A, Istighfaroh M. Socio-Demographic, Educational, and Attitudinal Factors Related to Comprehensive Knowledge about HIV/AIDS among Young Indonesian Women. Health Educ Health Promot 2025; 13 (1) :111-118
URL: http://hehp.modares.ac.ir/article-5-78415-en.html
URL: http://hehp.modares.ac.ir/article-5-78415-en.html
1- Department of Nutrition, Faculty of Medicine, Semarang State University, Semarang, Indonesia
2- Department of Public Health, Faculty of Medicine, Semarang State University, Semarang, Indonesia
3- Department of Public Health, School of Health Science, Mae Fah Luang University, Muang, Thailand
2- Department of Public Health, Faculty of Medicine, Semarang State University, Semarang, Indonesia
3- Department of Public Health, School of Health Science, Mae Fah Luang University, Muang, Thailand
Full-Text [PDF 623 kb]
(258 Downloads)
| Abstract (HTML) (419 Views)
Full-Text: (4 Views)
Introduction
Human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) is a significant public health concern globally. Despite substantial advancements in understanding and managing the disease, a definitive cure for HIV infection has yet to be discovered [1]. Data from UNAIDS indicate a persistent increase in the number of People Living with HIV (PLWH) over the years, rising from 27.2 million in 2000 to 32 million in 2010, reaching 36.7 million in 2017, and further increasing to 39.9 million in 2023 [2, 3].
The HIV epidemic in the Asia-Pacific region has a significant impact on key population groups, particularly younger individuals between the ages of 15 and 24, who account for approximately 25% of new HIV infections. In Indonesia, this trend is even more pronounced, with nearly half of all new HIV infections occurring among young people [4]. The number of PLWH in Indonesia has increased significantly over the past decade. In 2005, the estimated number of PLWH was 290,000. This number increased rapidly, reaching 510,000 in 2010 and further increasing to 620,000 by 2016 [2].
There are three types of education: formal, informal, and non-formal. Formal education is conducted in formal educational institutions, such as schools, which are structured and promoted through direct teaching (by teachers, etc.). Non-formal education is similarly structured but occurs outside formal educational settings (field trips, etc.). Informal education describes unstructured forms of learning that are not directly taught and can be accessed by anyone, in any place. In conclusion, the concept of education extends to include access to information through various channels, including other individuals, organizations, printed materials, and mass media as parts of education [5]. Health education can be defined as an activity that aims to provide individuals with information about the nature and causes of health and disease, as well as the individual’s level of risk associated with lifestyle-related behaviors, which motivates individuals to accept the necessary behavioral changes that affect their value systems, beliefs, and attitudes [6]. In this context, information about HIV/AIDS can be accessed through various sources.
Stigma, a complex social phenomenon, encompasses a range of negative attitudes, beliefs, and behaviors directed towards individuals or groups perceived as different or deviant. It involves the process of labeling and marginalizing individuals based on specific characteristics, often leading to discrimination and social exclusion. In the context of HIV/AIDS, stigma manifests in various forms, including fear, prejudice, and discrimination, resulting in devastating consequences such as social isolation, denial and silence, self-blame and guilt, and violence and discrimination. The factors contributing to AIDS stigma are multifaceted, encompassing the nature of transmission, the impact on individuals, societal norms and beliefs, and the accessibility of healthcare services. The stigma associated with AIDS endangers the lives of others [7].
Previous studies have indicated that socio-demographic, educational, and attitudinal factors are associated with comprehensive knowledge about HIV/AIDS [8-12]. This study aimed to determine the association of socio-demographic, educational, and attitudinal factors with knowledge about HIV/AIDS among young women aged 15-24 in Indonesia. It is anticipated that this research will facilitate the Indonesian government’s efforts to address the HIV/AIDS challenge, thereby enabling the realization of government initiatives aimed at achieving an HIV/AIDS-free society by 2030 [13].
Instrument and Methods
Study design and participants
This study was a quantitative research project with an observational analytical and retrospective cohort study design conducted in 2024. The data used were secondary data derived from the 2017 Indonesian Demographic Health Survey (IDHS). The total population was 49,627, derived from the Individual Recode Dataset (IR File), with the unit of study being eligible women aged 15-49.
The first inclusion criterion was young women aged 15-24 years, which comprised 14,766 individuals. After excluding missing data, a defined population of 12,632 participants was obtained for this study (Figure 1).
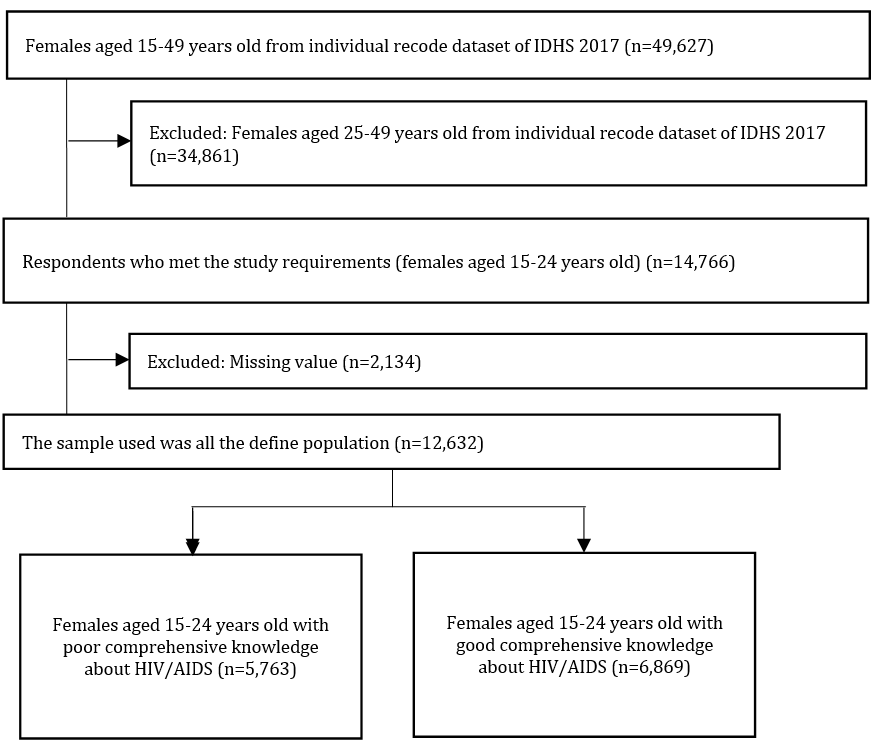
Figure 1. Sampling flowchart
Instrument
The instrument used was a standardized questionnaire from the DHS 2017. It included questions about socio-demographics, education, sources of information about HIV/AIDS, attitudes toward People living with HIV (PLWH), and knowledge about HIV/AIDS.
There were 13 questions regarding sources of information about AIDS. The classification of categories was determined through the calculation of quintiles. The “no information” category indicated that the participant had no information from any source or fewer than two sources of information. The “less information” category indicated that the participant has two sources of information. The “more information” category indicated that the participant has three or more sources of information.
There were nine questions regarding stigmatizing attitudes toward PLWH. The determination of “yes” and “no” was calculated based on the median response. The “yes” category indicated that the participant had a negative stigma and displayed negative behaviors toward PLWH, where the score was less than three for positive attitude responses. Conversely, the “no” category applies if the score was three or more for positive attitude responses.
Regarding knowledge about HIV/AIDS, there were ten questions. The classification of this category was determined by calculating the median. The “bad” category indicated that the participants had poor knowledge about HIV/AIDS, with fewer than eight questions answered correctly. Conversely, the “good” category indicated that the participants answered eight or more questions correctly.
In addition, there were modified parameters, specifically Internet use and contraceptive use. In this study, the categories for Internet use were “yes” and “no.” The “no” category was derived from the following options: 1) “never,” 2) “yes, before the last 12 months,” and 3) “yes, can’t establish when.” The “yes” category was derived from the option “yes, in the last 12 months.” The categories for contraceptive use were also “yes” and “no.” The “no” category was derived from the option “not using,” while the “yes” category was derived from categories other than “not using”.
Data analysis
This study utilized univariate, bivariate, and multivariate tests. The bivariate test employed the Chi-square test, and the multivariate test used binary logistic regression to identify the most influential parameter. SPSS 25 software was used to analyze the data.
Findings
A total of 12,632 young women aged 15-24 years were assessed. The univariate tests showed that participants with poor knowledge of HIV/AIDS accounted for almost half (45.6%) of the total participants. The age groups were nearly balanced, with the age group of 15-19 years comprising 53.1%. The majority of respondents lived in urban areas (58.8%), with the richest economic level dominating at 21.7%, followed by the richer category at 20.6%. The education level was predominantly at the secondary level, comprising 71.5%. Unmarried participants accounted for 77.3%, and 65.6% were not currently working. Most participants owned a mobile phone and used the Internet, at 90.9% and 84.5%, respectively. A total of 87.3% did not use contraception. Regarding information sources, participants had multiple sources of information, with more than three sources (classified as more information) accounting for 36.8%. In terms of stigmatizing attitudes toward PLWH, the majority of participants had a positive attitude toward PLWH (61.9%; Table 1).
Table 1. Frequency of participants’ characteristics from univariate analysis

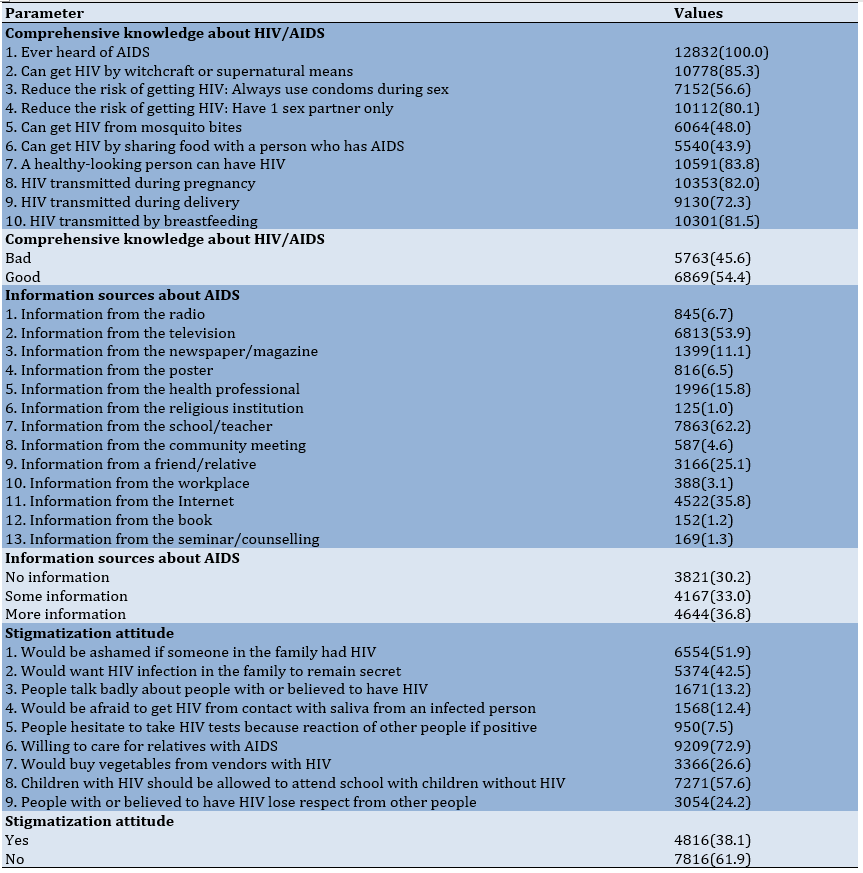
In terms of comprehensive knowledge about HIV/AIDS, the question with the lowest correct response was about whether HIV can be contracted by sharing food with a person who has AIDS, with only 43.9% of participants answering correctly. All participants (100%) had heard about AIDS. Regarding sources of information, most participants obtained AIDS-related information from schools/teachers, television, and the Internet, at 62.2%, 53.9%, and 35.8%, respectively. Meanwhile, the least common sources of information were religious institutions, books, and seminars/counseling, at 1%, 1.2%, and 1.3%, respectively. For stigmatizing attitudes toward PLWH, 72.9% of participants expressed a willingness to care for relatives with AIDS. However, very few individuals were willing to take HIV tests due to concerns about others’ reactions if the results were positive (7.5%), while the remainder were hesitant (92.5%). A total of six out of nine questions were answered with a positive attitude by less than 50% of participants (Table 2).
Table 2. Frequency of correct answers to comprehensive knowledge about HIV/AIDS, sources of information about AIDS, and stigmatization attitudes among females aged 15-24 years in Indonesia
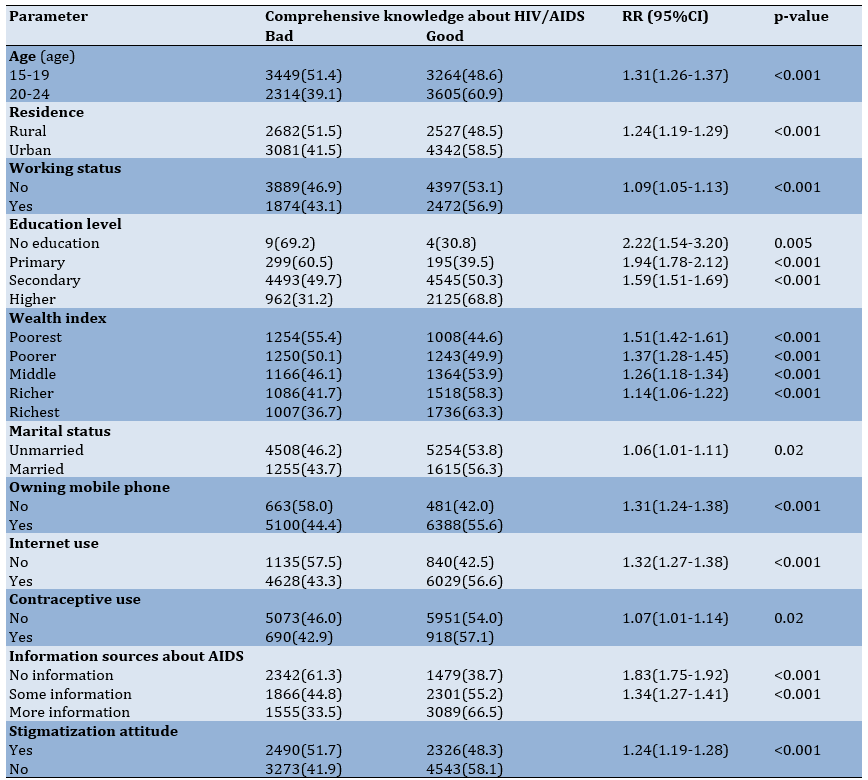
All independent parameters were found to be associated with comprehensive knowledge about HIV/AIDS. Young women aged 15-19 were 1.13 times more likely to have poor knowledge about HIV/AIDS than those aged 20-24. Young women living in villages were 1.24 times more likely to have poor knowledge about HIV/AIDS. Additionally, young women who are not working were 1.09 times more likely to have poor knowledge about HIV/AIDS.
At the education level, individuals with no education, primary education, and secondary education tend to have poorer knowledge about HIV/AIDS compared to those with higher education levels, by factors of 2.22, 1.94, and 1.59 times greater, respectively. Young women with the lowest wealth index had poorer knowledge about HIV/AIDS, with a factor of 1.51 times greater than those with the highest wealth index. Young women who were unmarried and did not use contraceptives exhibited worse knowledge, with factors of 1.06 and 1.07 times, respectively. Not having a mobile phone and not using the internet also increased the likelihood of having poor knowledge about HIV/AIDS by 1.31 and 1.32 times.
In terms of information sources about AIDS, young women who had fewer than two sources of information (classified as no information) were more likely to have poor knowledge about HIV/AIDS, with a factor of 1.83 compared to those with more information, while those with two sources of information (classified as some information) were 1.34 times more likely to have poor knowledge. Negative stigma toward PLWH influenced knowledge about HIV/AIDS, making it 1.24 times worse (Table 3).
Table 3. Relationship between the frequency of socio-demographic, educational, and attitudinal factors and knowledge about HIV/AIDS
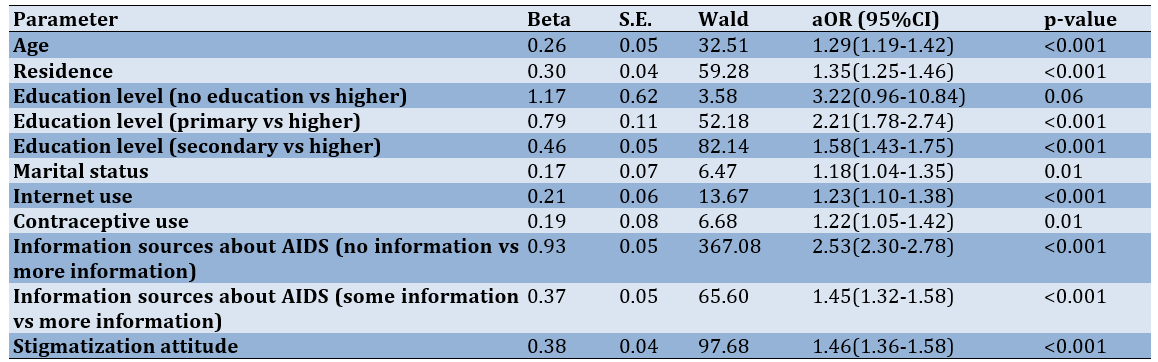
Sources of information about AIDS (no information vs. more information) were found to be the most influential parameter in poor knowledge about HIV/AIDS among young women in Indonesia (Table 4).
Table 4. Multivariate analysis results
Discussion
This study aimed to determine the association of socio-demographic, educational, and attitudinal factors with knowledge about HIV/AIDS among young women aged 15-24 in Indonesia. Socio-demographic, educational, and attitudinal factors are associated with young women’s knowledge about HIV/AIDS in Indonesia. However, regarding knowledge about HIV/AIDS, nearly half (45.5%) of the participants demonstrated a lack of knowledge. This indicates that a significant proportion of young women remain uninformed about HIV/AIDS. Adolescents, particularly those aged 15-19, are especially vulnerable to HIV infection due to the transitional nature of this period, which can lead to increased risky sexual behavior [14, 15]. It is, therefore, important to be informed about HIV/AIDS and the means of preventing it.
Young women aged 15-19 years had a relationship with knowledge about HIV/AIDS, aligning with research conducted in Indonesia using the IDHS 2012, with individuals aged 20 and older, particularly those between 25 and 39, demonstrating superior knowledge compared to the 15-19 age group. This disparity may be attributed to the ongoing education of adolescents aged 15-19, placing them at a lower educational level compared to older individuals. Additionally, limited access to information and educational resources, particularly for those who have dropped out of school, may contribute to this knowledge gap [16]. This finding is also consistent with research conducted in Malawi in 2021 [11].
We explored the relationship between rural residence and young women’s knowledge of HIV/AIDS. Research conducted in low- and middle-income Asian countries has reported similar findings, with individuals residing in rural areas exhibiting lower levels of HIV/AIDS knowledge [9]. This disparity may be attributed to limited access to healthcare services, education, and mass media in rural regions [9, 17, 18].
There was a significant association between working status, marital status, and knowledge about HIV/AIDS. As demonstrated in several previous studies, there is a significant association between respondents’ working status and marital status, and their knowledge about HIV/AIDS [10, 16].
Previous studies have indicated that social factors, including a higher education level and wealth, are associated with increased knowledge about HIV/AIDS [12, 19]. These findings align with our results. This social condition facilitates better access to health information [20]. In the Indonesian formal education system, the curriculum introduced in 2020 at the senior high school level (grade XI) includes instruction on HIV/AIDS [21]. In lower grade levels, typically starting from elementary school, the curriculum generally encompasses only an introduction to reproductive health [22]. At the junior high school level in 2018, an introduction to the anatomy of reproductive organs is typically provided as students enter adolescence and experience puberty [23].
The lack of mobile phone ownership and Internet usage was found to be associated with poor knowledge about HIV/AIDS. According to a study conducted in Ethiopia and Indonesia, there is a statistically significant association between mobile phone ownership and increased knowledge about HIV/AIDS. This is related to Internet use, where ownership of a mobile phone increases the likelihood of exposure to media that can be accessed online [8, 12, 24]. Prior research has demonstrated a significant association between health literacy and internet usage, reporting that many people utilize the Internet for health-related reasons [25]. Mobile technology can facilitate improved communication, easier access to healthcare professionals, enhanced confidentiality, and increased access to information, including reminders [26].
A lack of contraceptive use was associated with poor knowledge about HIV/AIDS. This is consistent with the results of several previous studies conducted in Sub-Saharan Africa, East Africa, Ethiopia, and Bangladesh, which have demonstrated that individuals who use contraceptives tend to have more comprehensive knowledge about HIV/AIDS [8, 18, 27, 28]. Women who use contraceptives are often perceived to have a better understanding of contraceptive methods and their associated health benefits, particularly those with a history of healthcare utilization [27]. Another study indicated that women who utilize contraceptives may possess a higher level of literacy and, consequently, demonstrate a greater receptivity to information than non-users [8].
Media information also played a crucial role in shaping comprehensive knowledge about HIV/AIDS. The more exposure individuals have to HIV/AIDS-related information, the greater their understanding of the disease becomes. We revealed that 61.3% of young women with fewer than two sources of information about HIV/AIDS had inadequate knowledge. This aligns with previous research demonstrating that exposure to a wider range of information sources enhances young women’s knowledge of HIV/AIDS [29-31].
Negative stigma toward PLWH influenced knowledge about HIV/AIDS. Negative stigma toward PLWH has been found to impact the level of knowledge held by individuals regarding HIV transmission, prevention methods, and treatment pathways [32-34]. Previous studies have indicated that negative perceptions and attitudes, which may be shaped by inaccurate knowledge about HIV transmission, can contribute to stigmatization [34].
The study revealed several factors associated with knowledge about HIV/AIDS among young women in Indonesia that require further attention. Any form of education about HIV/AIDS is significant for increasing the knowledge of young women, who are particularly vulnerable to HIV/AIDS infection. This is especially true for individuals with specific sociodemographic characteristics, such as those residing in rural areas, experiencing economic disadvantage, and having limited educational attainment. It is essential to utilize a range of information sources, both online and offline, and to leverage the increasingly sophisticated technology available in the present era to reach all groups. The distribution of health facilities must also be considered to facilitate the delivery of health education. Additionally, it is necessary to address the negative stigma associated with HIV/AIDS and to provide information on how this stigma can be eliminated.
This study had some limitations. The data from 2017 IDHS had missing data in the dataset. Nevertheless, this study still had a large sample size and provided valid evidence of sociodemographic factors associated with comprehensive knowledge about HIV/AIDS among young women in Indonesia. The next limitation was related to the limited number of factors/parameters studied as it depended on the availability of data in the secondary data used in this study.
Conclusion
Several socio-demographic, educational, and attitudinal factors are associated with knowledge about HIV/AIDS among young women in Indonesia.
Acknowledgments: We would like to express our gratitude to the DHS Program for granting us permission to utilize the raw data from the IDHS in the course of this study. We also thank all the insightful editors and reviewers.
Ethical Permissions: This study obtained ethical clearance from the Health Research Ethics Commission, Faculty of Medicine, Universitas Negeri Semarang, Number 422/KEPK/FK/KLE/2024.
Conflicts of Interests: Nothing to be reported.
Authors' Contribution: Budiono I (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer/Statistical Analyst (25%); Fauzi L (Second Author), Introduction Writer/Methodologist/Assistant Researcher/Discussion Writer/Statistical Analyst (25%); Kanthawee Ph (Third Author), Assistant Researcher/Discussion Writer/Statistical Analyst (18%); Yasari AS (Fourth Author), Assistant Researcher/Statistical Analyst (16%); Istighfaroh M (Fifth Author), Assistant Researcher/Statistical Analyst (16%)
Funding/Support: Nothing to be reported.
Human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) is a significant public health concern globally. Despite substantial advancements in understanding and managing the disease, a definitive cure for HIV infection has yet to be discovered [1]. Data from UNAIDS indicate a persistent increase in the number of People Living with HIV (PLWH) over the years, rising from 27.2 million in 2000 to 32 million in 2010, reaching 36.7 million in 2017, and further increasing to 39.9 million in 2023 [2, 3].
The HIV epidemic in the Asia-Pacific region has a significant impact on key population groups, particularly younger individuals between the ages of 15 and 24, who account for approximately 25% of new HIV infections. In Indonesia, this trend is even more pronounced, with nearly half of all new HIV infections occurring among young people [4]. The number of PLWH in Indonesia has increased significantly over the past decade. In 2005, the estimated number of PLWH was 290,000. This number increased rapidly, reaching 510,000 in 2010 and further increasing to 620,000 by 2016 [2].
There are three types of education: formal, informal, and non-formal. Formal education is conducted in formal educational institutions, such as schools, which are structured and promoted through direct teaching (by teachers, etc.). Non-formal education is similarly structured but occurs outside formal educational settings (field trips, etc.). Informal education describes unstructured forms of learning that are not directly taught and can be accessed by anyone, in any place. In conclusion, the concept of education extends to include access to information through various channels, including other individuals, organizations, printed materials, and mass media as parts of education [5]. Health education can be defined as an activity that aims to provide individuals with information about the nature and causes of health and disease, as well as the individual’s level of risk associated with lifestyle-related behaviors, which motivates individuals to accept the necessary behavioral changes that affect their value systems, beliefs, and attitudes [6]. In this context, information about HIV/AIDS can be accessed through various sources.
Stigma, a complex social phenomenon, encompasses a range of negative attitudes, beliefs, and behaviors directed towards individuals or groups perceived as different or deviant. It involves the process of labeling and marginalizing individuals based on specific characteristics, often leading to discrimination and social exclusion. In the context of HIV/AIDS, stigma manifests in various forms, including fear, prejudice, and discrimination, resulting in devastating consequences such as social isolation, denial and silence, self-blame and guilt, and violence and discrimination. The factors contributing to AIDS stigma are multifaceted, encompassing the nature of transmission, the impact on individuals, societal norms and beliefs, and the accessibility of healthcare services. The stigma associated with AIDS endangers the lives of others [7].
Previous studies have indicated that socio-demographic, educational, and attitudinal factors are associated with comprehensive knowledge about HIV/AIDS [8-12]. This study aimed to determine the association of socio-demographic, educational, and attitudinal factors with knowledge about HIV/AIDS among young women aged 15-24 in Indonesia. It is anticipated that this research will facilitate the Indonesian government’s efforts to address the HIV/AIDS challenge, thereby enabling the realization of government initiatives aimed at achieving an HIV/AIDS-free society by 2030 [13].
Instrument and Methods
Study design and participants
This study was a quantitative research project with an observational analytical and retrospective cohort study design conducted in 2024. The data used were secondary data derived from the 2017 Indonesian Demographic Health Survey (IDHS). The total population was 49,627, derived from the Individual Recode Dataset (IR File), with the unit of study being eligible women aged 15-49.
The first inclusion criterion was young women aged 15-24 years, which comprised 14,766 individuals. After excluding missing data, a defined population of 12,632 participants was obtained for this study (Figure 1).
Figure 1. Sampling flowchart
Instrument
The instrument used was a standardized questionnaire from the DHS 2017. It included questions about socio-demographics, education, sources of information about HIV/AIDS, attitudes toward People living with HIV (PLWH), and knowledge about HIV/AIDS.
There were 13 questions regarding sources of information about AIDS. The classification of categories was determined through the calculation of quintiles. The “no information” category indicated that the participant had no information from any source or fewer than two sources of information. The “less information” category indicated that the participant has two sources of information. The “more information” category indicated that the participant has three or more sources of information.
There were nine questions regarding stigmatizing attitudes toward PLWH. The determination of “yes” and “no” was calculated based on the median response. The “yes” category indicated that the participant had a negative stigma and displayed negative behaviors toward PLWH, where the score was less than three for positive attitude responses. Conversely, the “no” category applies if the score was three or more for positive attitude responses.
Regarding knowledge about HIV/AIDS, there were ten questions. The classification of this category was determined by calculating the median. The “bad” category indicated that the participants had poor knowledge about HIV/AIDS, with fewer than eight questions answered correctly. Conversely, the “good” category indicated that the participants answered eight or more questions correctly.
In addition, there were modified parameters, specifically Internet use and contraceptive use. In this study, the categories for Internet use were “yes” and “no.” The “no” category was derived from the following options: 1) “never,” 2) “yes, before the last 12 months,” and 3) “yes, can’t establish when.” The “yes” category was derived from the option “yes, in the last 12 months.” The categories for contraceptive use were also “yes” and “no.” The “no” category was derived from the option “not using,” while the “yes” category was derived from categories other than “not using”.
Data analysis
This study utilized univariate, bivariate, and multivariate tests. The bivariate test employed the Chi-square test, and the multivariate test used binary logistic regression to identify the most influential parameter. SPSS 25 software was used to analyze the data.
Findings
A total of 12,632 young women aged 15-24 years were assessed. The univariate tests showed that participants with poor knowledge of HIV/AIDS accounted for almost half (45.6%) of the total participants. The age groups were nearly balanced, with the age group of 15-19 years comprising 53.1%. The majority of respondents lived in urban areas (58.8%), with the richest economic level dominating at 21.7%, followed by the richer category at 20.6%. The education level was predominantly at the secondary level, comprising 71.5%. Unmarried participants accounted for 77.3%, and 65.6% were not currently working. Most participants owned a mobile phone and used the Internet, at 90.9% and 84.5%, respectively. A total of 87.3% did not use contraception. Regarding information sources, participants had multiple sources of information, with more than three sources (classified as more information) accounting for 36.8%. In terms of stigmatizing attitudes toward PLWH, the majority of participants had a positive attitude toward PLWH (61.9%; Table 1).
Table 1. Frequency of participants’ characteristics from univariate analysis
In terms of comprehensive knowledge about HIV/AIDS, the question with the lowest correct response was about whether HIV can be contracted by sharing food with a person who has AIDS, with only 43.9% of participants answering correctly. All participants (100%) had heard about AIDS. Regarding sources of information, most participants obtained AIDS-related information from schools/teachers, television, and the Internet, at 62.2%, 53.9%, and 35.8%, respectively. Meanwhile, the least common sources of information were religious institutions, books, and seminars/counseling, at 1%, 1.2%, and 1.3%, respectively. For stigmatizing attitudes toward PLWH, 72.9% of participants expressed a willingness to care for relatives with AIDS. However, very few individuals were willing to take HIV tests due to concerns about others’ reactions if the results were positive (7.5%), while the remainder were hesitant (92.5%). A total of six out of nine questions were answered with a positive attitude by less than 50% of participants (Table 2).
Table 2. Frequency of correct answers to comprehensive knowledge about HIV/AIDS, sources of information about AIDS, and stigmatization attitudes among females aged 15-24 years in Indonesia
All independent parameters were found to be associated with comprehensive knowledge about HIV/AIDS. Young women aged 15-19 were 1.13 times more likely to have poor knowledge about HIV/AIDS than those aged 20-24. Young women living in villages were 1.24 times more likely to have poor knowledge about HIV/AIDS. Additionally, young women who are not working were 1.09 times more likely to have poor knowledge about HIV/AIDS.
At the education level, individuals with no education, primary education, and secondary education tend to have poorer knowledge about HIV/AIDS compared to those with higher education levels, by factors of 2.22, 1.94, and 1.59 times greater, respectively. Young women with the lowest wealth index had poorer knowledge about HIV/AIDS, with a factor of 1.51 times greater than those with the highest wealth index. Young women who were unmarried and did not use contraceptives exhibited worse knowledge, with factors of 1.06 and 1.07 times, respectively. Not having a mobile phone and not using the internet also increased the likelihood of having poor knowledge about HIV/AIDS by 1.31 and 1.32 times.
In terms of information sources about AIDS, young women who had fewer than two sources of information (classified as no information) were more likely to have poor knowledge about HIV/AIDS, with a factor of 1.83 compared to those with more information, while those with two sources of information (classified as some information) were 1.34 times more likely to have poor knowledge. Negative stigma toward PLWH influenced knowledge about HIV/AIDS, making it 1.24 times worse (Table 3).
Table 3. Relationship between the frequency of socio-demographic, educational, and attitudinal factors and knowledge about HIV/AIDS
Sources of information about AIDS (no information vs. more information) were found to be the most influential parameter in poor knowledge about HIV/AIDS among young women in Indonesia (Table 4).
Table 4. Multivariate analysis results
Discussion
This study aimed to determine the association of socio-demographic, educational, and attitudinal factors with knowledge about HIV/AIDS among young women aged 15-24 in Indonesia. Socio-demographic, educational, and attitudinal factors are associated with young women’s knowledge about HIV/AIDS in Indonesia. However, regarding knowledge about HIV/AIDS, nearly half (45.5%) of the participants demonstrated a lack of knowledge. This indicates that a significant proportion of young women remain uninformed about HIV/AIDS. Adolescents, particularly those aged 15-19, are especially vulnerable to HIV infection due to the transitional nature of this period, which can lead to increased risky sexual behavior [14, 15]. It is, therefore, important to be informed about HIV/AIDS and the means of preventing it.
Young women aged 15-19 years had a relationship with knowledge about HIV/AIDS, aligning with research conducted in Indonesia using the IDHS 2012, with individuals aged 20 and older, particularly those between 25 and 39, demonstrating superior knowledge compared to the 15-19 age group. This disparity may be attributed to the ongoing education of adolescents aged 15-19, placing them at a lower educational level compared to older individuals. Additionally, limited access to information and educational resources, particularly for those who have dropped out of school, may contribute to this knowledge gap [16]. This finding is also consistent with research conducted in Malawi in 2021 [11].
We explored the relationship between rural residence and young women’s knowledge of HIV/AIDS. Research conducted in low- and middle-income Asian countries has reported similar findings, with individuals residing in rural areas exhibiting lower levels of HIV/AIDS knowledge [9]. This disparity may be attributed to limited access to healthcare services, education, and mass media in rural regions [9, 17, 18].
There was a significant association between working status, marital status, and knowledge about HIV/AIDS. As demonstrated in several previous studies, there is a significant association between respondents’ working status and marital status, and their knowledge about HIV/AIDS [10, 16].
Previous studies have indicated that social factors, including a higher education level and wealth, are associated with increased knowledge about HIV/AIDS [12, 19]. These findings align with our results. This social condition facilitates better access to health information [20]. In the Indonesian formal education system, the curriculum introduced in 2020 at the senior high school level (grade XI) includes instruction on HIV/AIDS [21]. In lower grade levels, typically starting from elementary school, the curriculum generally encompasses only an introduction to reproductive health [22]. At the junior high school level in 2018, an introduction to the anatomy of reproductive organs is typically provided as students enter adolescence and experience puberty [23].
The lack of mobile phone ownership and Internet usage was found to be associated with poor knowledge about HIV/AIDS. According to a study conducted in Ethiopia and Indonesia, there is a statistically significant association between mobile phone ownership and increased knowledge about HIV/AIDS. This is related to Internet use, where ownership of a mobile phone increases the likelihood of exposure to media that can be accessed online [8, 12, 24]. Prior research has demonstrated a significant association between health literacy and internet usage, reporting that many people utilize the Internet for health-related reasons [25]. Mobile technology can facilitate improved communication, easier access to healthcare professionals, enhanced confidentiality, and increased access to information, including reminders [26].
A lack of contraceptive use was associated with poor knowledge about HIV/AIDS. This is consistent with the results of several previous studies conducted in Sub-Saharan Africa, East Africa, Ethiopia, and Bangladesh, which have demonstrated that individuals who use contraceptives tend to have more comprehensive knowledge about HIV/AIDS [8, 18, 27, 28]. Women who use contraceptives are often perceived to have a better understanding of contraceptive methods and their associated health benefits, particularly those with a history of healthcare utilization [27]. Another study indicated that women who utilize contraceptives may possess a higher level of literacy and, consequently, demonstrate a greater receptivity to information than non-users [8].
Media information also played a crucial role in shaping comprehensive knowledge about HIV/AIDS. The more exposure individuals have to HIV/AIDS-related information, the greater their understanding of the disease becomes. We revealed that 61.3% of young women with fewer than two sources of information about HIV/AIDS had inadequate knowledge. This aligns with previous research demonstrating that exposure to a wider range of information sources enhances young women’s knowledge of HIV/AIDS [29-31].
Negative stigma toward PLWH influenced knowledge about HIV/AIDS. Negative stigma toward PLWH has been found to impact the level of knowledge held by individuals regarding HIV transmission, prevention methods, and treatment pathways [32-34]. Previous studies have indicated that negative perceptions and attitudes, which may be shaped by inaccurate knowledge about HIV transmission, can contribute to stigmatization [34].
The study revealed several factors associated with knowledge about HIV/AIDS among young women in Indonesia that require further attention. Any form of education about HIV/AIDS is significant for increasing the knowledge of young women, who are particularly vulnerable to HIV/AIDS infection. This is especially true for individuals with specific sociodemographic characteristics, such as those residing in rural areas, experiencing economic disadvantage, and having limited educational attainment. It is essential to utilize a range of information sources, both online and offline, and to leverage the increasingly sophisticated technology available in the present era to reach all groups. The distribution of health facilities must also be considered to facilitate the delivery of health education. Additionally, it is necessary to address the negative stigma associated with HIV/AIDS and to provide information on how this stigma can be eliminated.
This study had some limitations. The data from 2017 IDHS had missing data in the dataset. Nevertheless, this study still had a large sample size and provided valid evidence of sociodemographic factors associated with comprehensive knowledge about HIV/AIDS among young women in Indonesia. The next limitation was related to the limited number of factors/parameters studied as it depended on the availability of data in the secondary data used in this study.
Conclusion
Several socio-demographic, educational, and attitudinal factors are associated with knowledge about HIV/AIDS among young women in Indonesia.
Acknowledgments: We would like to express our gratitude to the DHS Program for granting us permission to utilize the raw data from the IDHS in the course of this study. We also thank all the insightful editors and reviewers.
Ethical Permissions: This study obtained ethical clearance from the Health Research Ethics Commission, Faculty of Medicine, Universitas Negeri Semarang, Number 422/KEPK/FK/KLE/2024.
Conflicts of Interests: Nothing to be reported.
Authors' Contribution: Budiono I (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer/Statistical Analyst (25%); Fauzi L (Second Author), Introduction Writer/Methodologist/Assistant Researcher/Discussion Writer/Statistical Analyst (25%); Kanthawee Ph (Third Author), Assistant Researcher/Discussion Writer/Statistical Analyst (18%); Yasari AS (Fourth Author), Assistant Researcher/Statistical Analyst (16%); Istighfaroh M (Fifth Author), Assistant Researcher/Statistical Analyst (16%)
Funding/Support: Nothing to be reported.
Article Type: Descriptive & Survey |
Subject:
Health Education and Health Behavior
Received: 2024/12/11 | Accepted: 2025/01/20 | Published: 2025/02/1
Received: 2024/12/11 | Accepted: 2025/01/20 | Published: 2025/02/1
References
1. WHO. HIV and AIDS [Internet]. Geneva: World Health Organization; 2024 [cited 2024 May 15]. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids?gad_source=1&gclid=CjwKCAjw8rW2BhAgEiwAoRO5rBnHoGKk_ka0upux9qOgU6xQY9YL3LEMY10zeVDrS---ciaw3Wev1BoCMmoQAvD_BwE. [Link]
2. UNAIDS. UNAIDS Data 2017. Geneva: Joint United Nations Programme on HIV/AIDS; 2017. [Link]
3. UNAIDS. Fact sheet 2024-Latest global and regional HIV statistics on the status of the AIDS epidemic. Geneva: Joint United Nations Programme on HIV/AIDS; 2024. [Link]
4. UNAIDS. UNAIDS Data 2023. Geneva: Joint United Nations Programme on HIV/AIDS; 2023. [Link]
5. Johnson M, Majewska D. Formal, non-formal, and informal learning: What are they, and how can we research them?. Cambridge: Cambridge University Press & Assessment; 2022. [Link]
6. Whitehead D. Health promotion and health education: Advancing the concepts. J Adv Nurs. 2004;47(3):311-20. [Link] [DOI:10.1111/j.1365-2648.2004.03095.x]
7. Yuh JN, Ellwanger K, Potts L, Ssenyonga J. Stigma among HIV/AIDS patients in Africa: A critical review. Procedia Soc Behav Sci. 2014;140:581-5. [Link] [DOI:10.1016/j.sbspro.2014.04.474]
8. Agegnehu CD, Geremew BM, Sisay MM, Muchie KF, Engida ZT, Gudayu TW, et al. Determinants of comprehensive knowledge of HIV/AIDS among reproductive age (15-49 years) women in Ethiopia: Further analysis of 2016 Ethiopian demographic and health survey. AIDS Res Ther 2020;17(1):51. [Link] [DOI:10.1186/s12981-020-00305-z]
9. Dzadey D, Biswas RK, Bhowmik J. Investigating factors affecting HIV/AIDS knowledge among women in low and middle-income countries in Asia. J Health Psychol. 2023;28(11):1085-98. [Link] [DOI:10.1177/13591053221127531]
10. Gebremedhin SA, Youjie W, Tesfamariam EH. Predictors of HIV/AIDS knowledge and attitude among young women of Nigeria and democratic republic of Congo: Cross-sectional study. J AIDS Clin Res. 2017;8(3). [Link] [DOI:10.4172/2155-6113.1000677]
11. Mandiwa C, Namondwe B, Munthali M. Prevalence and correlates of comprehensive HIV/AIDS knowledge among adolescent girls and young women aged 15-24 years in Malawi: Evidence from the 2015-16 Malawi demographic and health survey. BMC Public Health. 2021;21(1):1508. [Link] [DOI:10.1186/s12889-021-11564-4]
12. Virdausi FD, Efendi F, Kusumaningrum T, Adnani QES, McKenna L, Ramadhan K, et al. Socio-economic and demographic factors associated with knowledge and attitude of HIV/AIDS among women aged 15-49 years old in Indonesia. Healthcare. 2022;10(8):1545. [Link] [DOI:10.3390/healthcare10081545]
13. Regulation of the Minister of Health of the Republic of Indonesia Number 23 of 2022 concerning Overcoming Human Immunodeficiency Virus, Acquired Immuno-Deficiency Syndrome, and Sexually Transmitted Infections. Available from: https://peraturan.bpk.go.id/Details/245543/permenkes-no-23-tahun-2022. [Indonesian] [Link]
14. Keto T, Tilahun A, Mamo A. Knowledge, attitude and practice towards risky sexual behaviors among secondary and preparatory students of Metu town, south western Ethiopia. BMC Public Health. 2020;20(1):1394. [Link] [DOI:10.1186/s12889-020-09371-4]
15. Bakara SM, Lubis ES, Fitriani Y. Adolescent knowledge and perception of HIV/AIDS stigmatization in the Indonesian context. Period Epidemiol J. 2023;11(3):287-94. [Indonesian] [Link] [DOI:10.20473/jbe.V11I32023.287-294]
16. Pradnyani PE, Wibowo A, Mahmudah M. The effects of socio-demographic characteristics on Indonesian women's knowledge of HIV/AIDS: A cross-sectional study. J Prev Med Public Health. 2019;52(2):109-14. [Link] [DOI:10.3961/jpmph.18.256]
17. Ali Khan M, Islam Mondal N, Islam R, Kaikobad S, Mustagir G, Tasneem N. Knowledge about HIV/AIDS among women in Bangladesh: An urban-rural comparison of trend, attitude and determinants. Biom Biostat Int J. 2019;8(5):162-70. [Link] [DOI:10.15406/bbij.2019.08.00285]
18. Sheikh MT, Uddin MN, Khan JR. A comprehensive analysis of trends and determinants of HIV/AIDS knowledge among the Bangladeshi women based on Bangladesh Demographic and Health Surveys, 2007-2014. Arch Public Health. 2017;75:59. [Link] [DOI:10.1186/s13690-017-0228-2]
19. Mude W, Oguoma VM, Gesesew HA, Ameyaw EK, Njue C, Nyanhanda T, et al. HIV/AIDS knowledge and attitudes assessment among women of child-bearing age in South Sudan: Findings from a household survey. PLoS One. 2020;15(12):e0243969. [Link] [DOI:10.1371/journal.pone.0243969]
20. Taylor J, Lamaro Haintz G. Influence of the social determinants of health on access to healthcare services among refugees in Australia. Aust J Prim Health. 2018;24(1):14-28. [Link] [DOI:10.1071/PY16147]
21. Rohiman, M. The Learning Module of Physical Education, Sports, and Health for Senior High School Grade XI: HIV and AIDS. Jakarta: Ministry of Education and Culture of the Republic of Indonesia; 2020. [Indonesian] [Link]
22. Directorate of Elementary Schools, Ministry of Education and Culture of the Republic of Indonesia. Guidebook for Implementing Reproductive Health Education in Elementary Schools. Jakarta: Ministry of Education and Culture of the Republic of Indonesia; 2020. [Indonesian] [Link]
23. Zubaidah S, Mahanal S, Yuliati L, Dasna IW, Pangestuti AA, Puspitasari DR, et al. Natural Sciences for Junior High School Grade IX. Jakarta: Ministry of Education and Culture of the Republic of Indonesia; 2018. [Indonesian] [Link]
24. Gebre MN, Feyasa MB, Dadi TK. Levels of mother-to-child HIV transmission knowledge and associated factors among reproductive-age women in Ethiopia: Analysis of 2016 Ethiopian demographic and health survey data. PLoS One. 2021;16(8):e0256419. [Link] [DOI:10.1371/journal.pone.0256419]
25. Estacio EV, Whittle R, Protheroe J. The digital divide: Examining socio-demographic factors associated with health literacy, access and use of internet to seek health information. J Health Psychol. 2019;24(12):1668-75. [Link] [DOI:10.1177/1359105317695429]
26. Brar MS, Cariappa MP. Exploring the use of mobile phone technology for the enhancement of the prevention of mother-to-child transmission of HIV program in Nyanza, Kenya: A qualitative study. Med J Armed Forces India. 2014;70(3):304. [Link] [DOI:10.1016/j.mjafi.2014.06.010]
27. Terefe B, Jembere MM, Liyew B. Comprehensive knowledge of mother-to-child HIV/AIDS transmission, prevention, and associated factors among reproductive-age women in East Africa: Insights from recent demographic and national health surveys. BMC Womens Health. 2024;24(1):318. [Link] [DOI:10.1186/s12905-024-03173-1]
28. Teshale AB, Yeshaw Y, Alem AZ, Ayalew HG, Liyew AM, Tessema ZT, et al. Comprehensive knowledge about HIV/AIDS and associated factors among women of reproductive age in sub-Saharan Africa: A multilevel analysis using the most recent demographic and health survey of each country. BMC Infect Dis. 2022;22(1):130. [Link] [DOI:10.1186/s12879-022-07124-9]
29. Bozkurt O, Turan DB. Evaluation of the knowledge and stigmatization level of HIV/AIDS and related factors. J Psychiatr Nurs. 2020;11(1):41-8. [Link] [DOI:10.14744/phd.2020.88156]
30. Kene C, Deribe L, Adugna H, Tekalegn Y, Seyoum K, Geta G. HIV/AIDS related knowledge of university students in Southeast Ethiopia: A cross-sectional survey. HIV AIDS. 2021;13:681-90. [Link] [DOI:10.2147/HIV.S300859]
31. Ofori M, Nyarne EA, Eshun I. Students' knowledge and sources of information on HIV/AIDS: Evidence from the lower Manya Krobo municipality of the eastern region of Ghana. Univers J Soc Sci Humanit. 2022;2(4):186-200. [Link] [DOI:10.31586/ujssh.2022.390]
32. Arifin H, Ibrahim K, Rahayuwati L, Herliani YK, Kurniawati Y, Pradipta RO, et al. HIV-related knowledge, information, and their contribution to stigmatization attitudes among females aged 15-24 years: Regional disparities in Indonesia. BMC Public Health. 2022;22(1):637. [Link] [DOI:10.1186/s12889-022-13046-7]
33. Li X, Yuan L, Li X, Shi J, Jiang L, Zhang C, et al. Factors associated with stigma attitude towards people living with HIV among general individuals in Heilongjiang, Northeast China. BMC Infect Dis. 2017;17(1):154. [Link] [DOI:10.1186/s12879-017-2216-0]
34. Ubaka CM, Adibe MO, Ukwe CV. Discriminatory attitudes of pharmacy students and pharmacists against people living with HIV/AIDS. Trop J Pharm Res. 2014;13(2). [Link] [DOI:10.4314/tjpr.v13i2.20]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |