



Volume 13, Issue 1 (2025)
Health Educ Health Promot 2025, 13(1): 1-6 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mashudi M, Masyitah D, Fahmi I, Dahrizal D, Idramsyah I. Impact of the TB SEHAT Application on Medication Adherence in Pulmonary Tuberculosis Patients at Putri Ayu Health Center, Jambi City. Health Educ Health Promot 2025; 13 (1) :1-6
URL: http://hehp.modares.ac.ir/article-5-77780-en.html
URL: http://hehp.modares.ac.ir/article-5-77780-en.html
1- Department of Nursing, Health Polytechnic of Jambi, Jambi, Indonesia
2- Department of Nursing, Health Polytechnic of Bengkulu, Bengkulu, Indonesia
2- Department of Nursing, Health Polytechnic of Bengkulu, Bengkulu, Indonesia
Keywords: Tuberculosis, Pulmonary [MeSH], Nursing [MeSH], Mobile Applications [MeSH], Medication Adherence [MeSH]
Full-Text [PDF 575 kb]
(1307 Downloads)
| Abstract (HTML) (917 Views)
Full-Text: (66 Views)
Introduction
Tuberculosis (TB) remains a significant global health challenge, particularly in developing countries [1]. Indonesia ranks third worldwide for the highest TB burden, with a treatment success rate of only around 50% [2]. Successful TB treatment requires a prolonged duration, and factors, such as drug side effects, socioeconomic barriers, and social stigma can adversely impact patient adherence to treatment. Ensuring adherence is essential, as it prevents the development of multidrug-resistant tuberculosis (DR-TB), thereby improving cure rates and treatment success and reducing transmission to others [3].
DR-TB presents a significant obstacle to global TB elimination efforts, with a worldwide treatment success rate of just 57%. Loss to follow-up (LTFU) is a primary factor contributing to this low success rate. In Indonesia, the treatment success rate is even lower, at under 50%, partly due to a high LTFU rate of 26% [4].
Indonesia has implemented the DOTS program in line with WHO recommendations; however, DOTS alone has proven insufficient, as challenges with patient adherence to TB medication persist [5]. Traditional direct supervision has had limited success in addressing these adherence issues, highlighting the need for innovative approaches that utilize electronic and communication media to support medication supervision by health workers. Research on the effectiveness of digital health solutions to improve medication adherence among TB patients remains limited in Indonesia [6].
Mobile health (M-Health) applications, particularly those that are Android-based, represent an innovative approach in the healthcare sector aimed at facilitating behavioral change and promoting health management outside traditional hospital settings. Technology-based services offer the potential for efficient, effective, and high-quality care. By utilizing technology, patients are empowered to actively engage in self-screening and treatment, fostering greater self-care awareness and optimizing health outcomes [7-9].
M-Health is advancing rapidly and has been applied across a wide range of disease areas. TB, one of the leading causes of death from infectious diseases globally, stands to benefit significantly from M-Health applications, which contribute meaningfully to enhancing TB treatment outcomes [10, 11]. Specifically, applications that support dose individualization, adherence monitoring, or provide targeted information and education about the disease serve as effective tools for preventing drug-resistant TB and disease relapse. M-Health holds substantial promise for addressing key challenges in TB treatment. Although mobile technology has shown a positive impact on adherence and treatment outcomes, further clinical evidence is needed to confirm its benefits for individualized dosing, patient education, and diagnostic support [6, 12].
M-Health, which leverages smartphones as a platform, is highly accessible and widely adopted within communities [13]. Community nurses, especially those in primary healthcare settings, can apply M-Health effectively. Given the challenges of managing large service areas with limited human resources, M-Health offers a valuable alternative for delivering remote nursing care and monitoring patients who require supervision [10, 14].
Research relevant to the Lung TB Treatment Monitoring Application includes the study titled “Design of TB Treatment Compliance Application” [15], which highlights the importance of adherence to treatment. Additionally, Iribarren et al. [16] demonstrate that self-management of pulmonary TB through SMS can significantly enhance treatment adherence and patient awareness regarding follow-up examinations.
Building on the insights gained from the TB Treatment Adherence Application Design, the researchers developed an Android-based Oral Anti-Tuberculosis (OAT) Adherence Application featuring a more comprehensive set of tools. Notable enhancements include educational components covering TB infection prevention, the importance of adhering to OAT, nutritional management, and stress management, along with features, such as a calendar, notifications, and consultation options. This application specifically targets the needs of TB patients and their families.
Data from the Putri Ayu Health Center indicate a rising trend in pulmonary TB cases and a persistently high dropout rate among patients. Accordingly, this study aimed to evaluate the impact of the TB SEHAT application on medication adherence among pulmonary TB patients in Jambi City.
Materials and Methods
Study design
This research employed a one-group pre-test-post-test design with a control group using prospective data collection.
Participants
This study was conducted in the service area of the Putri Ayu Health Center in Jambi City, Indonesia, from May to July 2024. Respondents, selected through simple random sampling, were categorized into two groups; the intervention group, which received education and medication reminders through the TB SEHAT app, and the control group, which received standard care from medication supervisors. The subjects included adult TB patients aged 17 years and older who had been undergoing treatment for at least one month, were receiving first-line OAT medication, and were accompanied by their families while using the Android application. Exclusion criteria included patients with mental disorders, those undergoing directly observed treatment, short-course (DOTS), patients who did not consistently attend follow-up appointments, and those who had dropped out of treatment.
Sample size
To achieve a power of 0.80 at an alpha level of 0.05, adequate sample size was estimated using the formula for the “mean of the two groups” [17]. The effect size was determined based on the findings from the study by Hoffman et al. [18], which assessed the effectiveness of the TB SEHAT app in enhancing medication adherence. Utilizing Cohen’s formula, the effect size (d) was calculated to be 0.20 (p<0.05). Furthermore, Cohen’s guidelines were employed to estimate the sample size based on the specified significance criteria (α=0.05, power=0.80) considering µ1=42.1, µ2=49.9, SD1=11, and SD2=11.3. This yielded a minimum required sample size of 31 participants per group. To accommodate potential dropouts, an additional 20% was added to each group, resulting in a final sample size of 37 participants per group.
Data collection
OAT medication adherence refers to the respondents’ compliance with health workers’ recommendations regarding the intake of OAT drugs. This was evaluated using the Tuberculosis Medication Adherence Scale (TBMAS) consisting of ten items, with scores ranging from 10 to 100. Adherence was categorized into two objective criteria; compliant if the respondent’s score was ≥60, and non-compliant if the score was <60.
The “TB SEHAT” application served as the intervention and independent parameter. The pre-test and initial intervention using the mobile application were conducted on day one, followed by a second intervention and post-test on day 30. The pre-test and post-test assessments focused on OAT medication adherence, which was measured by comparing the time of medication intake with the scheduled alarm time. TB patients were considered compliant if the time difference between taking the medication and the alarm schedule was no more than two hours; they were deemed non-compliant if this difference exceeded two hours. Medication adherence was monitored using a QR code found on the medication box, which was linked to the “TB SEHAT” application.
Statistical analysis
A descriptive analysis was conducted to characterize the respondents’ demographics. Descriptive statistics summarize the data using measures, such as mean, maximum, minimum, median, and standard deviation. To compare medication adherence between the group using the TB SEHAT application and the control group, an analysis of covariance (ANCOVA) was employed. Data analysis was performed using SPSS version 23.0. A 95% confidence interval not including the value of one indicated statistical significance.
Findings
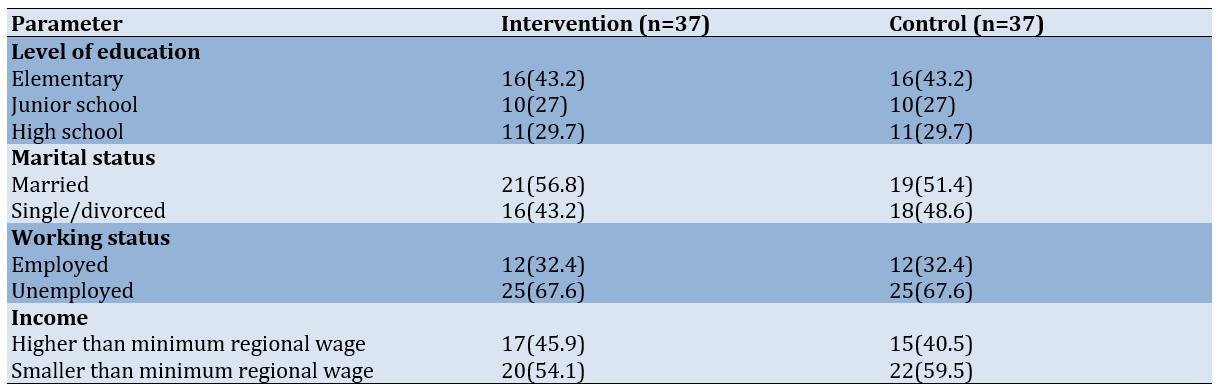
The mean age of participants in the intervention group was 43.76±16.31 years, while the control group had a mean age of 45.62±16.15 years. The ages of respondents ranged from 18 to 73 years. A higher proportion of male respondents was observed, with 27 males (72.97%) in the intervention group and 23 males (62.16%) in the control group. The educational levels of respondents were comparable between groups, and the majority were married. Additionally, there were more respondents who were unemployed compared to those who were employed, with most reporting an income below the minimum wage (Table 1).
Table 1. Demographic characteristics of the respondents
A significant difference was observed in adherence to OAT medication adherence between the intervention and control groups (p=0.001). The mean compliance score before using the TB SEHAT application was 121.16±6.19, while the mean compliance score after using the application increased to 127.30±5.22. In contrast, the mean compliance score for respondents undergoing standardized treatment monitoring remained unchanged, with a score of 121.41±6.38 before and 121.41±6.43 after monitoring, indicating no improvement in adherence.
Discussion
This study aimed to evaluate the impact of the TB SEHAT application on medication adherence among pulmonary TB patients in Jambi City. The majority of respondents were male, totaling 50 individuals. The average age of participants in both groups was similar, both of which fall within the productive age category. This demographic trend may be attributed to the higher mobility of men in their productive years, which increases their likelihood of exposure to TB pathogens. Moreover, after puberty, the body’s capacity to prevent disease transmission through the bloodstream improves, yet its ability to guard against respiratory infections diminishes significantly. This decline is linked to the reduced functionality of the thymus gland, which plays a crucial role in the immune defense system during childhood [19]. These findings are consistent with previous research [20-22], indicating that men are more susceptible to TB, with a prevalence of 55.18% compared to 44.82% in women. Contributing factors include unhealthy lifestyle choices among men, such as smoking and alcohol consumption, which compromise the immune system and increase vulnerability to pulmonary TB infection [23].
There was a significant difference in the average compliance of respondents, as measured by the TBMAS, before and after using the SEHAT TB application in the intervention group, with an increase of 6.14 points. In contrast, the control group showed no change in the average adherence score. Further statistical analysis revealed that the TB SEHAT application significantly enhanced adherence to OAT. These findings suggest a notable difference in the effectiveness of medication supervision through digital technology compared to that provided by directly observed therapy (DOT) by the drug-taking supervisors (PMO).
The TB SEHAT application has proven effective in enhancing the knowledge and compliance of TB patients regarding their treatment. It features four key components that represent a novel advancement over previous applications, including education, consultation, calendar, and notifications. The education section includes animated videos on infection prevention, the importance of adhering to TB medication, nutritional management, and stress management techniques, including progressive muscle relaxation (PMR). This educational content is designed to enhance patient understanding of lung TB management, thereby promoting adherence to OAT medication.
In contrast, the control group, which received supervision from the PMO, demonstrated lower effectiveness in promoting adherence. It is hypothesized that this may be attributed to the PMO’s busy schedules in meeting family obligations, potentially leading to lapses in reminders for patients to take their OAT medication.
Our findings align with research conducted by Fuadiati et al. [24], indicating that animated videos are favored by patients over the age of 18 as a compelling form of media. This preference is attributed to the dynamic presentation of motion, images, and sound, which effectively captures attention. In contrast, counseling that utilizes printed media often involves direct verbal instruction and written content, which may convey a more formal tone. While printed materials can be informative, they tend to be perceived as less engaging compared to animated videos, making the latter a more appealing choice for counseling purposes [19].
Furthermore, medication monitoring through mHealth applications based on Android technology represents a significant innovation in the healthcare sector, aimed at facilitating behavioral changes and enhancing health management beyond traditional hospital settings. By leveraging technology, healthcare services can be delivered efficiently and effectively, ultimately improving the quality of care. Additionally, such technology empowers patients to take an active role in their health management, fostering self-screening and increasing awareness of self-care practices to optimize health outcomes [25, 26].
This study is consistent with research conducted by Iribarren et al. [16], indicating that self-management of pulmonary TB through SMS communication can significantly enhance treatment adherence and patient awareness regarding their examinations. Furthermore, findings from Wijayanti et al. [27] support this notion, demonstrating that the use of social media platforms, such as BBM, Line, and Twitter can positively influence individual behaviors.
The observed increase in medication adherence among pulmonary TB patients in the intervention group can be attributed to the ongoing interactions between the researchers and the respondents. This continuous engagement fosters social interaction and cultivates a reciprocal influence, ultimately enhancing the management strategies employed by each individual. Such relationships are critical in promoting adherence and improving health outcomes for patients undergoing treatment for pulmonary TB.
The sample size was limited to just 74 respondents, encompassing both the intervention and control groups. As a result, the generalizability of the findings to a broader population may be compromised. A small sample size can diminish statistical power, increasing the risk of Type I or Type II errors.
Additionally, the relatively short duration of the study may not adequately capture long-term changes in patient adherence following the implementation of the TB SEHAT app. Consequently, further research with a larger sample size and an extended timeframe is warranted to better assess the app’s sustained impact on medication adherence among patients.
The implications of this study for the field of health are significant. The TB SEHAT app notably improved medication adherence, positioning it as an essential tool in TB management programs. This application offers valuable support for patients in maintaining optimal adherence to treatment protocols.
Furthermore, these results could stimulate the development of technology-based health applications for various other diseases, thereby enhancing the scope and effectiveness of digital interventions. Additionally, the findings may heighten awareness among healthcare professionals regarding the critical role of technological approaches in improving patient adherence, which could lead to better health outcomes and a reduction in TB-related complications. Lastly, this study provides a foundation for future research aimed at exploring additional factors that influence medication adherence and the utilization of health apps within the context of chronic diseases. Consequently, the implementation of the TB SEHAT app is recommended as an essential component of TB management strategies and serves as a model for the future development of similar health applications.
Conclusion
The TB SEHAT application effectively improves adherence to anti-tuberculosis drugs in patients with pulmonary tuberculosis.
Acknowledgments: We extend our heartfelt gratitude to everyone who contributed to this research. In particular, we would like to acknowledge the Head of the Health Polytechnic of Jambi and the Health Polytechnic of Bengkulu for their invaluable support and guidance throughout this project. We are also grateful to the application development team for their insightful input during the research process.
Ethical Permissions: This study received ethical approval from the Health Research Ethics Commission of the Ministry of Health, Jambi, under protocol number LB.02.06/5/162/2024. All procedures adhered to established research ethics standards, ensuring the protection of participants’ rights and privacy.
Conflicts of Interests: The authors reported no conflicts of interests.
Authors' Contribution: Mashudi M (First Author), Introduction Writer/Main Researcher/Methodologist/Discussion Writer/Statistical Analyst (40%); Masyitah D (Second Author), Assistance Researcher/Discussion Writer (20%); Fahmi I (Third Author), Introduction Writer/Assistance Researcher/Discussion Writer (20%); Dahrizal D (Fourth Author), Introduction Writer/Assistance Researcher/Discussion Writer (10%); Idramsyah I (Fifth Author), Introduction Writer/Assistance Researcher/Discussion Writer (10%)
Funding/Support: This research was funded by a grant from the Indonesian Ministry of Health.
Tuberculosis (TB) remains a significant global health challenge, particularly in developing countries [1]. Indonesia ranks third worldwide for the highest TB burden, with a treatment success rate of only around 50% [2]. Successful TB treatment requires a prolonged duration, and factors, such as drug side effects, socioeconomic barriers, and social stigma can adversely impact patient adherence to treatment. Ensuring adherence is essential, as it prevents the development of multidrug-resistant tuberculosis (DR-TB), thereby improving cure rates and treatment success and reducing transmission to others [3].
DR-TB presents a significant obstacle to global TB elimination efforts, with a worldwide treatment success rate of just 57%. Loss to follow-up (LTFU) is a primary factor contributing to this low success rate. In Indonesia, the treatment success rate is even lower, at under 50%, partly due to a high LTFU rate of 26% [4].
Indonesia has implemented the DOTS program in line with WHO recommendations; however, DOTS alone has proven insufficient, as challenges with patient adherence to TB medication persist [5]. Traditional direct supervision has had limited success in addressing these adherence issues, highlighting the need for innovative approaches that utilize electronic and communication media to support medication supervision by health workers. Research on the effectiveness of digital health solutions to improve medication adherence among TB patients remains limited in Indonesia [6].
Mobile health (M-Health) applications, particularly those that are Android-based, represent an innovative approach in the healthcare sector aimed at facilitating behavioral change and promoting health management outside traditional hospital settings. Technology-based services offer the potential for efficient, effective, and high-quality care. By utilizing technology, patients are empowered to actively engage in self-screening and treatment, fostering greater self-care awareness and optimizing health outcomes [7-9].
M-Health is advancing rapidly and has been applied across a wide range of disease areas. TB, one of the leading causes of death from infectious diseases globally, stands to benefit significantly from M-Health applications, which contribute meaningfully to enhancing TB treatment outcomes [10, 11]. Specifically, applications that support dose individualization, adherence monitoring, or provide targeted information and education about the disease serve as effective tools for preventing drug-resistant TB and disease relapse. M-Health holds substantial promise for addressing key challenges in TB treatment. Although mobile technology has shown a positive impact on adherence and treatment outcomes, further clinical evidence is needed to confirm its benefits for individualized dosing, patient education, and diagnostic support [6, 12].
M-Health, which leverages smartphones as a platform, is highly accessible and widely adopted within communities [13]. Community nurses, especially those in primary healthcare settings, can apply M-Health effectively. Given the challenges of managing large service areas with limited human resources, M-Health offers a valuable alternative for delivering remote nursing care and monitoring patients who require supervision [10, 14].
Research relevant to the Lung TB Treatment Monitoring Application includes the study titled “Design of TB Treatment Compliance Application” [15], which highlights the importance of adherence to treatment. Additionally, Iribarren et al. [16] demonstrate that self-management of pulmonary TB through SMS can significantly enhance treatment adherence and patient awareness regarding follow-up examinations.
Building on the insights gained from the TB Treatment Adherence Application Design, the researchers developed an Android-based Oral Anti-Tuberculosis (OAT) Adherence Application featuring a more comprehensive set of tools. Notable enhancements include educational components covering TB infection prevention, the importance of adhering to OAT, nutritional management, and stress management, along with features, such as a calendar, notifications, and consultation options. This application specifically targets the needs of TB patients and their families.
Data from the Putri Ayu Health Center indicate a rising trend in pulmonary TB cases and a persistently high dropout rate among patients. Accordingly, this study aimed to evaluate the impact of the TB SEHAT application on medication adherence among pulmonary TB patients in Jambi City.
Materials and Methods
Study design
This research employed a one-group pre-test-post-test design with a control group using prospective data collection.
Participants
This study was conducted in the service area of the Putri Ayu Health Center in Jambi City, Indonesia, from May to July 2024. Respondents, selected through simple random sampling, were categorized into two groups; the intervention group, which received education and medication reminders through the TB SEHAT app, and the control group, which received standard care from medication supervisors. The subjects included adult TB patients aged 17 years and older who had been undergoing treatment for at least one month, were receiving first-line OAT medication, and were accompanied by their families while using the Android application. Exclusion criteria included patients with mental disorders, those undergoing directly observed treatment, short-course (DOTS), patients who did not consistently attend follow-up appointments, and those who had dropped out of treatment.
Sample size
To achieve a power of 0.80 at an alpha level of 0.05, adequate sample size was estimated using the formula for the “mean of the two groups” [17]. The effect size was determined based on the findings from the study by Hoffman et al. [18], which assessed the effectiveness of the TB SEHAT app in enhancing medication adherence. Utilizing Cohen’s formula, the effect size (d) was calculated to be 0.20 (p<0.05). Furthermore, Cohen’s guidelines were employed to estimate the sample size based on the specified significance criteria (α=0.05, power=0.80) considering µ1=42.1, µ2=49.9, SD1=11, and SD2=11.3. This yielded a minimum required sample size of 31 participants per group. To accommodate potential dropouts, an additional 20% was added to each group, resulting in a final sample size of 37 participants per group.
Data collection
OAT medication adherence refers to the respondents’ compliance with health workers’ recommendations regarding the intake of OAT drugs. This was evaluated using the Tuberculosis Medication Adherence Scale (TBMAS) consisting of ten items, with scores ranging from 10 to 100. Adherence was categorized into two objective criteria; compliant if the respondent’s score was ≥60, and non-compliant if the score was <60.
The “TB SEHAT” application served as the intervention and independent parameter. The pre-test and initial intervention using the mobile application were conducted on day one, followed by a second intervention and post-test on day 30. The pre-test and post-test assessments focused on OAT medication adherence, which was measured by comparing the time of medication intake with the scheduled alarm time. TB patients were considered compliant if the time difference between taking the medication and the alarm schedule was no more than two hours; they were deemed non-compliant if this difference exceeded two hours. Medication adherence was monitored using a QR code found on the medication box, which was linked to the “TB SEHAT” application.
Statistical analysis
A descriptive analysis was conducted to characterize the respondents’ demographics. Descriptive statistics summarize the data using measures, such as mean, maximum, minimum, median, and standard deviation. To compare medication adherence between the group using the TB SEHAT application and the control group, an analysis of covariance (ANCOVA) was employed. Data analysis was performed using SPSS version 23.0. A 95% confidence interval not including the value of one indicated statistical significance.
Findings
The mean age of participants in the intervention group was 43.76±16.31 years, while the control group had a mean age of 45.62±16.15 years. The ages of respondents ranged from 18 to 73 years. A higher proportion of male respondents was observed, with 27 males (72.97%) in the intervention group and 23 males (62.16%) in the control group. The educational levels of respondents were comparable between groups, and the majority were married. Additionally, there were more respondents who were unemployed compared to those who were employed, with most reporting an income below the minimum wage (Table 1).
Table 1. Demographic characteristics of the respondents
A significant difference was observed in adherence to OAT medication adherence between the intervention and control groups (p=0.001). The mean compliance score before using the TB SEHAT application was 121.16±6.19, while the mean compliance score after using the application increased to 127.30±5.22. In contrast, the mean compliance score for respondents undergoing standardized treatment monitoring remained unchanged, with a score of 121.41±6.38 before and 121.41±6.43 after monitoring, indicating no improvement in adherence.
Discussion
This study aimed to evaluate the impact of the TB SEHAT application on medication adherence among pulmonary TB patients in Jambi City. The majority of respondents were male, totaling 50 individuals. The average age of participants in both groups was similar, both of which fall within the productive age category. This demographic trend may be attributed to the higher mobility of men in their productive years, which increases their likelihood of exposure to TB pathogens. Moreover, after puberty, the body’s capacity to prevent disease transmission through the bloodstream improves, yet its ability to guard against respiratory infections diminishes significantly. This decline is linked to the reduced functionality of the thymus gland, which plays a crucial role in the immune defense system during childhood [19]. These findings are consistent with previous research [20-22], indicating that men are more susceptible to TB, with a prevalence of 55.18% compared to 44.82% in women. Contributing factors include unhealthy lifestyle choices among men, such as smoking and alcohol consumption, which compromise the immune system and increase vulnerability to pulmonary TB infection [23].
There was a significant difference in the average compliance of respondents, as measured by the TBMAS, before and after using the SEHAT TB application in the intervention group, with an increase of 6.14 points. In contrast, the control group showed no change in the average adherence score. Further statistical analysis revealed that the TB SEHAT application significantly enhanced adherence to OAT. These findings suggest a notable difference in the effectiveness of medication supervision through digital technology compared to that provided by directly observed therapy (DOT) by the drug-taking supervisors (PMO).
The TB SEHAT application has proven effective in enhancing the knowledge and compliance of TB patients regarding their treatment. It features four key components that represent a novel advancement over previous applications, including education, consultation, calendar, and notifications. The education section includes animated videos on infection prevention, the importance of adhering to TB medication, nutritional management, and stress management techniques, including progressive muscle relaxation (PMR). This educational content is designed to enhance patient understanding of lung TB management, thereby promoting adherence to OAT medication.
In contrast, the control group, which received supervision from the PMO, demonstrated lower effectiveness in promoting adherence. It is hypothesized that this may be attributed to the PMO’s busy schedules in meeting family obligations, potentially leading to lapses in reminders for patients to take their OAT medication.
Our findings align with research conducted by Fuadiati et al. [24], indicating that animated videos are favored by patients over the age of 18 as a compelling form of media. This preference is attributed to the dynamic presentation of motion, images, and sound, which effectively captures attention. In contrast, counseling that utilizes printed media often involves direct verbal instruction and written content, which may convey a more formal tone. While printed materials can be informative, they tend to be perceived as less engaging compared to animated videos, making the latter a more appealing choice for counseling purposes [19].
Furthermore, medication monitoring through mHealth applications based on Android technology represents a significant innovation in the healthcare sector, aimed at facilitating behavioral changes and enhancing health management beyond traditional hospital settings. By leveraging technology, healthcare services can be delivered efficiently and effectively, ultimately improving the quality of care. Additionally, such technology empowers patients to take an active role in their health management, fostering self-screening and increasing awareness of self-care practices to optimize health outcomes [25, 26].
This study is consistent with research conducted by Iribarren et al. [16], indicating that self-management of pulmonary TB through SMS communication can significantly enhance treatment adherence and patient awareness regarding their examinations. Furthermore, findings from Wijayanti et al. [27] support this notion, demonstrating that the use of social media platforms, such as BBM, Line, and Twitter can positively influence individual behaviors.
The observed increase in medication adherence among pulmonary TB patients in the intervention group can be attributed to the ongoing interactions between the researchers and the respondents. This continuous engagement fosters social interaction and cultivates a reciprocal influence, ultimately enhancing the management strategies employed by each individual. Such relationships are critical in promoting adherence and improving health outcomes for patients undergoing treatment for pulmonary TB.
The sample size was limited to just 74 respondents, encompassing both the intervention and control groups. As a result, the generalizability of the findings to a broader population may be compromised. A small sample size can diminish statistical power, increasing the risk of Type I or Type II errors.
Additionally, the relatively short duration of the study may not adequately capture long-term changes in patient adherence following the implementation of the TB SEHAT app. Consequently, further research with a larger sample size and an extended timeframe is warranted to better assess the app’s sustained impact on medication adherence among patients.
The implications of this study for the field of health are significant. The TB SEHAT app notably improved medication adherence, positioning it as an essential tool in TB management programs. This application offers valuable support for patients in maintaining optimal adherence to treatment protocols.
Furthermore, these results could stimulate the development of technology-based health applications for various other diseases, thereby enhancing the scope and effectiveness of digital interventions. Additionally, the findings may heighten awareness among healthcare professionals regarding the critical role of technological approaches in improving patient adherence, which could lead to better health outcomes and a reduction in TB-related complications. Lastly, this study provides a foundation for future research aimed at exploring additional factors that influence medication adherence and the utilization of health apps within the context of chronic diseases. Consequently, the implementation of the TB SEHAT app is recommended as an essential component of TB management strategies and serves as a model for the future development of similar health applications.
Conclusion
The TB SEHAT application effectively improves adherence to anti-tuberculosis drugs in patients with pulmonary tuberculosis.
Acknowledgments: We extend our heartfelt gratitude to everyone who contributed to this research. In particular, we would like to acknowledge the Head of the Health Polytechnic of Jambi and the Health Polytechnic of Bengkulu for their invaluable support and guidance throughout this project. We are also grateful to the application development team for their insightful input during the research process.
Ethical Permissions: This study received ethical approval from the Health Research Ethics Commission of the Ministry of Health, Jambi, under protocol number LB.02.06/5/162/2024. All procedures adhered to established research ethics standards, ensuring the protection of participants’ rights and privacy.
Conflicts of Interests: The authors reported no conflicts of interests.
Authors' Contribution: Mashudi M (First Author), Introduction Writer/Main Researcher/Methodologist/Discussion Writer/Statistical Analyst (40%); Masyitah D (Second Author), Assistance Researcher/Discussion Writer (20%); Fahmi I (Third Author), Introduction Writer/Assistance Researcher/Discussion Writer (20%); Dahrizal D (Fourth Author), Introduction Writer/Assistance Researcher/Discussion Writer (10%); Idramsyah I (Fifth Author), Introduction Writer/Assistance Researcher/Discussion Writer (10%)
Funding/Support: This research was funded by a grant from the Indonesian Ministry of Health.
Article Type: Original Research |
Subject:
Technology of Health Education
Received: 2024/11/1 | Accepted: 2024/12/16 | Published: 2025/01/21
Received: 2024/11/1 | Accepted: 2024/12/16 | Published: 2025/01/21
References
1. Keutzer L, Wicha SG, Simonsson USH. Mobile health apps for improvement of tuberculosis treatment: Descriptive review. JMIR mHealth uHealth. 2020;8(4):e17246. [] [DOI:10.2196/17246]
2. Cohen A, Mathiasen VD, Schön T, Wejse C. The global prevalence of latent tuberculosis: A systematic review and meta-analysis. Eur Respir J. 2019;54(3):1900655. [Link] [DOI:10.1183/13993003.00655-2019]
3. Novaes MT, Do Prado TN, Delcarro JCS, Rissino SDD, Crepaldi NY, Sanches TLM, et al. Development and content validation of a mobile application for monitoring latent tuberculosis treatment. Rev Soc Bras Med Trop. 2022;55:e0465-2021. [Link] [DOI:10.1590/0037-8682-0465-2021]
4. Soedarsono S, Mertaniasih NM, Kusmiati T, Permatasari A, Juliasih NN, Hadi C, et al. Determinant factors for loss to follow-up in drug-resistant tuberculosis patients: The importance of psycho-social and economic aspects. BMC Pulm Med. 2021;21(1):360. [Link] [DOI:10.1186/s12890-021-01735-9]
5. Ubajaka CF, Azuike EC, Ugoji JO, Nwibo OE, Ejiofor OC, Modebe IA, et al. Adherence to drug medications amongst tuberculosis patients in a tertiary health institution in South East Nigeria. Int J Clin Med. 2015;6(6):399-406. [Link] [DOI:10.4236/ijcm.2015.66052]
6. Mustopa R, Damris D, Syamsurizal S, Emawati MDW. Evaluation of m-health on medication adherence in tuberculosis patients: A systematic review. NSC Nurs. 2023;3(1):1-29. [Link] [DOI:10.32549/OPI-NSC-91]
7. Sehat M, Razzaghi R, Ghamsary M, Ganji MF, Sehat M. Changes in the rate of bacillus tuberculosis infection in health workers in the first year of the COVID-19 epidemic in Kashan-Iran. Heliyon. 2023;9(10):e20560. [Link] [DOI:10.1016/j.heliyon.2023.e20560]
8. Putri SE, Rekawati E, Wati DNK. Effectiveness of self-management on adherence to self-care and on health status among elderly people with hypertension. J Public Health Res. 2021;10(s1):jphr.2021.2406. [Link] [DOI:10.4081/jphr.2021.2406]
9. Supriano A, Katmini K. Analysis of factors affecting druging compliance in lung tuberculosis patients: Theory of health belief model (HBM) in the working area of the health center, Dompu City. J Qual Public Health. 2021;5(1):1-6. [Link] [DOI:10.30994/jqph.v5i1.241]
10. Boonnuddar N, Wuttidittachotti P. Mobile application: Patients' adherence to medicine in-take schedules. Proceedings of the International Conference on Big Data and Internet of Thing. New York: Association for Computing Machinery; 2017. p. 237-41. [Link] [DOI:10.1145/3175684.3175714]
11. Fuad A, Herwanto GB, Pertiwi AAP, Wahyuningtias SD, Harsini H, Maula AW, et al. Design and prototype of TOMO: An app for improving drug resistant TB treatment adherence [version 1; Peer review: 1 approved, 2 approved with reservations]. F1000Research. 2021;10:983. [Link] [DOI:10.12688/f1000research.67212.1]
12. Liu X, Lewis JJ, Zhang H, Lu W, Zhang S, Zheng G, et al. Effectiveness of electronic reminders to improve medication adherence in tuberculosis patients: A cluster-randomised trial. PLoS Med. 2015;12(9):e1001876. [Link] [DOI:10.1371/journal.pmed.1001876]
13. Haase J, Farris KB, Dorsch MP. Mobile applications to improve medication adherence. Telemed J E Health. 2017;23(2):75-9. [Link] [DOI:10.1089/tmj.2015.0227]
14. Haji HA, Rivett U, Suleman H. Improving compliance to tuberculosis treatment: Supporting patients through mobile graphic-based reminders. J Public Health Dev Ctries. 2016;2(3). [Link]
15. Yunita F, Veronica RI, Ratnasari L, Suhendra A, Basuki H. Design a TB treatment compliance application. INFORMATIKA KEDOKTERAN: JURNAL ILMIAH. 2019;2(1):54-69. [Indonesian] [Link]
16. Iribarren SJ, Milligan H, Chirico C, Goodwin K, Schnall R, Telles H, et al. Patient-centered mobile tuberculosis treatment support tools (TB-TSTs) to improve treatment adherence: A pilot randomized controlled trial exploring feasibility, acceptability and refinement needs. Lancet Reg Health Am. 2022;13:100291. [Link] [DOI:10.1016/j.lana.2022.100291]
17. Cohen J. Statistical power analysis for the behavioral sciences. UK: Routledge; 2013. [Link] [DOI:10.4324/9780203771587]
18. Hoffman G, Zhao X. A primer for conducting experiments in human-robot interaction. ACM Transactions on Human-Robot Interaction. 2020;10(1):1-31. [Link] [DOI:10.1145/3412374]
19. Jerene D, Levy J, Van Kalmthout K, Van Rest J, McQuaid CF, Quaife M, et al. Effectiveness of digital adherence technologies in improving tuberculosis treatment outcomes in four countries: A pragmatic cluster randomised trial protocol. BMJ Open. 2023;13(3):e068685. [Link] [DOI:10.1136/bmjopen-2022-068685]
20. Duko B, Bedaso A, Ayano G. The prevalence of depression among patients with tuberculosis: A systematic review and meta-analysis. Ann Gen Psychiatry. 2020;19:30. [Link] [DOI:10.1186/s12991-020-00281-8]
21. Kulchavenya E, Khomyakov V. Male genital tuberculosis in Siberians. World J Urol. 2006;24(1):74-8. [Link] [DOI:10.1007/s00345-005-0048-9]
22. Kaona FAD, Tuba M, Siziya S, Sikaona L. An assessment of factors contributing to treatment adherence and knowledge of TB transmission among patients on TB treatment. BMC Public Health. 2004;4:68. [Link] [DOI:10.1186/1471-2458-4-68]
23. Tesfahuneygn G, Medhin G, Legesse M. Adherence to anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia. BMC Res Notes. 2015;8:503. [Link] [DOI:10.1186/s13104-015-1452-x]
24. Fuadiati LL, Sukartini T, Makhfudli M. The effectiveness of mobile health on medication adherence in tuberculosis patients. J Telenurs. 2023;5(2):1604-13. [Indonesian] [Link] [DOI:10.31539/joting.v5i2.4234]
25. Cinderatama TA, Dianta AF, Efendi FS, Eliyen K. Web and Android-based application for monitoring tuberculosis (TB) patients in Kediri City. Matrix J Technol Inform Manag. 2021;11(1):11-25. [Link] [DOI:10.31940/matrix.v11i1.2331]
26. Arnizant TFS, Bernardi FA, Sanchez TLM, Crepaldi NY, Do Prado TN, Novaes MT, et al. My latent tuberculosis treatment-mobile application to assist in adherence to latent tuberculosis treatment. Procedia Comput Sci. 2022;196:640-6. [Link] [DOI:10.1016/j.procs.2021.12.059]
27. Wijayanti E, Bachtiar A, Achadi A, Rachmawati UA, Sjaaf AC, Eryando T, et al. Mobile application development for improving medication safety in tuberculosis patients: A quasi-experimental study protocol. PLoS One. 2022;17(9):e0272616. [Link] [DOI:10.1371/journal.pone.0272616]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |