



Volume 12, Issue 2 (2024)
Health Educ Health Promot 2024, 12(2): 347-356 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Babaei M, Simbar M, Alavi Majd H, Nahidi F. Promoting Sexual and Reproductive Health among Married Women of Reproductive Age in Sanandaj City, Iran. Health Educ Health Promot 2024; 12 (2) :347-356
URL: http://hehp.modares.ac.ir/article-5-75308-en.html
URL: http://hehp.modares.ac.ir/article-5-75308-en.html
1- Department of Reproductive Health and Midwifery, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Department of Biostatistics, Faculty of Paramedical Sciences, Shahid Beheshti Medical University, Tehran, Iran
2- Department of Biostatistics, Faculty of Paramedical Sciences, Shahid Beheshti Medical University, Tehran, Iran
Full-Text [PDF 682 kb]
(2904 Downloads)
| Abstract (HTML) (988 Views)
Full-Text: (285 Views)
Introduction
Improvement of women's health is a comprehensive approach that significantly impacts a country's long-term development strategies and economic progress [1]. Reproductive and sexual health is crucial for women's overall well-being. It ensures healthy sexual lives, reproductive capabilities, and informed decisions. Improving SRH (Sexual and Reproductive Health) supports sustainable development goals, particularly in achieving gender equality and enhancing health and well-being for all [2, 3].
Globally, reproductive and sexual health issues among women represent a substantial proportion of health-related challenges. Enhancing these aspects of health not only empowers women to gain greater control over their well-being but also addresses underlying factors that influence health outcomes [4, 5]. Promoting sexual health involves empowering individuals to manage and enhance their sexual well-being [6]. This can help prevent sexually transmitted diseases, avoid unintended pregnancies, and improve sexual performance [7]. Furthermore, sexual and reproductive health promotion extends beyond clinical aspects to include a wide range of choices, behaviors, and social impacts [8]. It seems that there are multiple individual and interpersonal factors that can influence the adoption of behaviors promoting reproductive and sexual health [9, 10]. In Abedi et al.'s study, a significant relationship was observed between various dimensions of a health-promoting lifestyle, such as responsibility, interpersonal relationships, and stress management, and all aspects of sexual functioning in women of reproductive age [11]. Family responsibilities, environmental pressures, financial pressures, family and social support networks, and inadequate communication are among the barriers that can affect the promotion of sexual and reproductive health [12].
In a study conducted in Iran, women took measures to improve their reproductive health by making informed decisions, engaging in self-care behaviors, having satisfactory sexual relationships through discussing their needs and desires, and striving to resolve sexual issues. Effective communication between couples and joint decision-making were also identified as actions that prevent unwanted pregnancies and enhance women's reproductive health [13]. In another study, the use of condoms, traditional medicine, antibiotics, and disinfecting and cleaning oneself after sexual intercourse were among the preventive behaviors identified for maintaining reproductive and sexual health and preventing sexually transmitted infections [14]. In the study by Cipres et al., it was observed that women used various strategies to reduce the risk of sexually transmitted infections, including condom use, asking partners about STIs (Sexually Transmitted Infections), frequent STI screening, and inquiring about their partners' other sexual partners. It also appears that another factor influencing the incidence of sexually transmitted infections in women is related to power inequities in sexual partnerships [15]. Married women face multiple roles and responsibilities, and the nature of their marital relationship can greatly influence their reproductive and sexual health [16]. Numerous studies have been conducted on health-promoting lifestyles among women of reproductive age in Iran and around the world. However, there has not been a study specifically examining health-promoting reproductive and sexual behaviors in the particular group of married women of reproductive age.
Differences in healthy behaviors across cultures highlight the significant impact of cultural and religious contexts on women's reproductive and sexual health. Context is critical for understanding health behavior, and its importance is emphasized for planning behavior change interventions and policies [17]. Each society's unique value system influences these behaviors, underscoring the need for qualitative studies to understand women's perspectives. Such studies are crucial for developing tailored health services and interventions. The absence of qualitative research on married women of reproductive age in Iran, despite their vital role in family and community health, motivated this study to explore their experiences regarding health-promoting sexual and reproductive behaviors.
Participants and Methods
The current research was conducted between December 2019 and March 2022 in Sanandaj, the capital of Kurdistan province in western Iran.
The qualitative study utilized a conventional content analysis approach to gain deeper insights into the experiences of married women regarding promotion behaviors related to sexual and reproductive health. Sampling took place at two health centers with high visitor numbers, located in distinct regions characterized by various social and economic levels. The research population comprised women attending urban healthcare centers in Sanandaj. Sampling was purposeful, aiming for maximum diversity in age, education levels of both women and their spouses, family income status, occupations of both women and their spouses, number of children, and place of residence. Sampling continued until data saturation was achieved. The inclusion criteria encompassed women aged 15-49 years, Iranian nationality, ability to communicate effectively with the researcher, not being pregnant, and willingness to participate in the study.
The study's exit conditions encompass any distinct physical or psychological ailment that hinders the participant's involvement in the research including pregnancy. The interviews were conducted solely by the first author, who possesses extensive expertise in qualitative research. A total of 23 interviews were conducted, and to ensure comprehensive coverage, three additional participants were interviewed once data saturation was reached. Additionally, to enrich the insights gleaned from participant interviews, discussions were held with 6 specialists. The participants were interviewed at specific locations and times as arranged. Due to the widespread occurrence of COVID-19, interviews took place in various settings such as parks, open areas, and occasionally at the participants' homes. Key informant interviews were conducted using online methods. Information was collected through semi-structured and comprehensive interviews with women. Field notes were taken, and audio recording was conducted with participants' consent. Additionally, insights were derived from participants' nonverbal cues. Occasionally, participants requested to temporarily pause the recording during the interview to share information more comfortably. In such cases, the interviews were paused, and the details were transcribed. These transcribed sections were promptly reviewed and edited. At the start of the interview, a series of broad and open-ended inquiries were employed. The interview started with a general and open question.
Search engine queries were used as needed to ask detailed questions, including seeking further elaboration, clarification, specific details, examples, and consideration of additional factors related to discussed behaviors. Participants were also encouraged to share any additional insights they wished to offer and invited to address any questions not asked. Permission for future interviews was obtained. Participants freely expressed viewpoints through unbiased inquiries, with opportunities to share experiences. Interviews lasted 40 to 90 minutes, allowing broad perspectives to emerge.
Data analysis
This study utilized content analysis following the steps proposed by Graneheim & Lundman [18]. After each interview, the researcher listened to the recordings multiple times for comprehension, transcribed the data manually, and then typed them. Analysis was conducted using MAXQDA10 software (version 10). Initial categorization occurred concurrently with interviews, with units of meaning condensed into codes, organized based on commonalities and distinctions, resulting in subcategories. These subcategories were grouped into categories, and fundamental themes were identified.
To ensure data accuracy and robustness, Guba & Lincoln's fourfold criteria were applied, focusing on dependability, transferability, credibility, and confirmability [19]. To boost data credibility, the first author used three methods over a year: Extensive data work, cross-checking notes with participants for alignment, and verifying codes and categories with the research team. A mixed data collection approach was employed, including interviews, observations, and written materials.
When participants couldn't review texts due to literacy or time constraints, segments needing clarification were revisited through various means. Texts were reviewed and modified if necessary. Sample diversity was ensured to enhance data credibility. Reliability was ensured by recording interviews in audio and handwritten forms, with a 2-week gap for comparison. Identical questions were asked to all participants, validated by two qualitative researchers.
Confirmability was maintained through review by two faculty members, extending to data analysis procedures. For transferability, the research methodology provided comprehensive descriptions of the study population and contextual details.
The datasets generated and/or analyzed during the current study are not publicly available due to privacy protection of the participants but are available from the corresponding author on reasonable request.
Findings
The age of the women ranged from 18 to 45 years. Women had varying levels of education, ranging from being illiterate to holding a master's degree (Tables 1 & 2).
Table 1. Demographic characteristics of participants
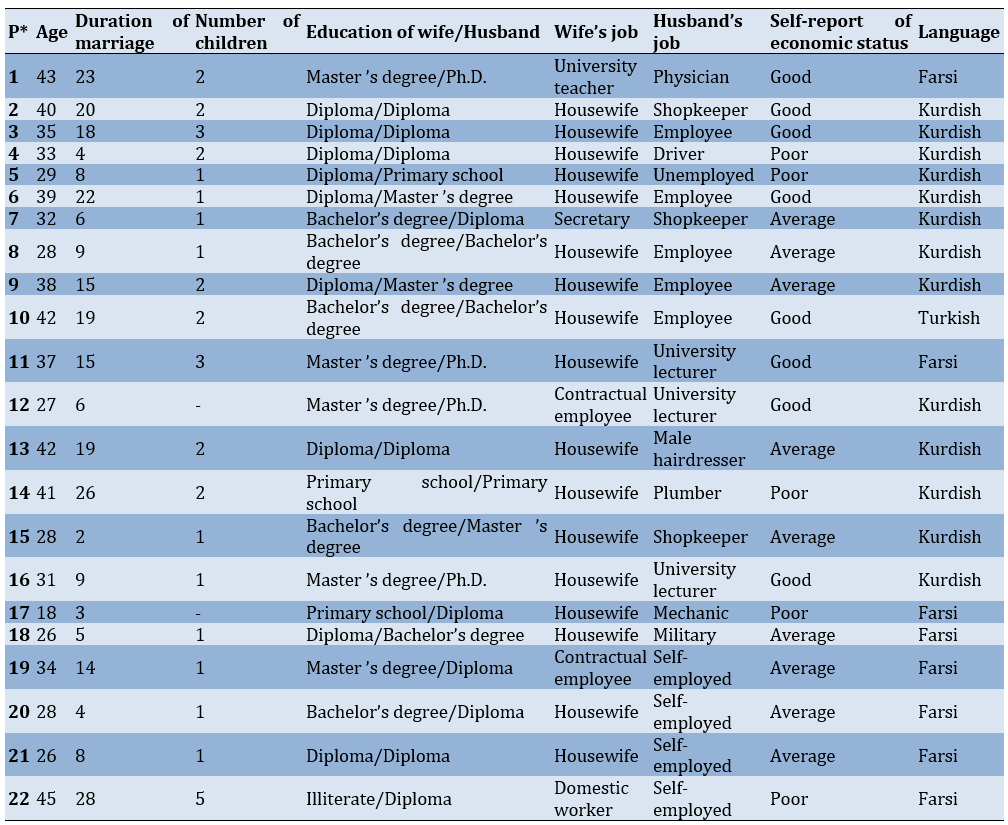
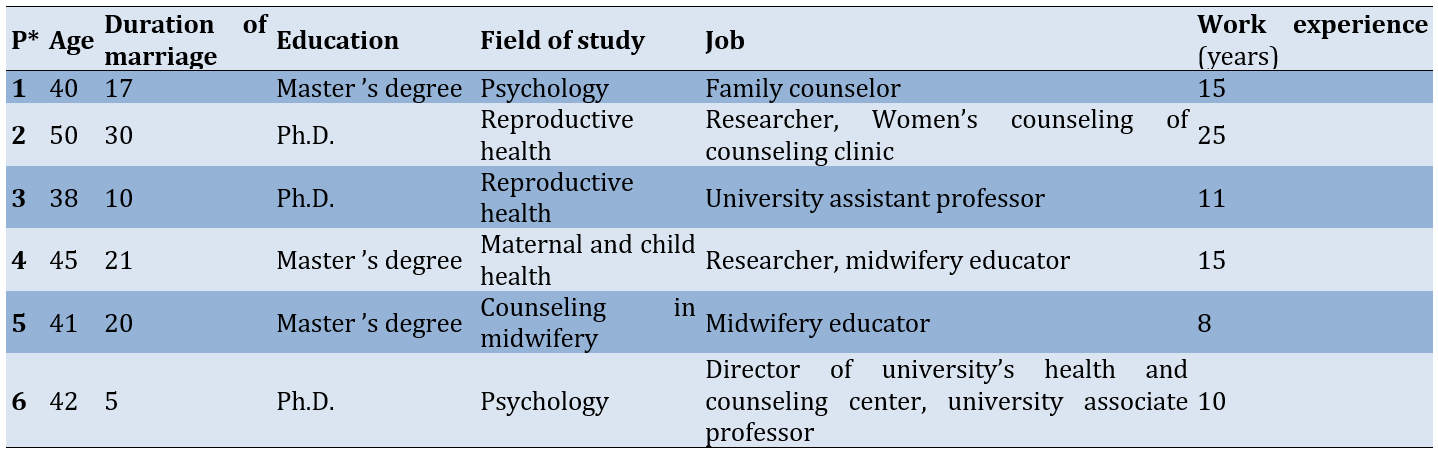
Table 2. Demographic characteristics of specialists
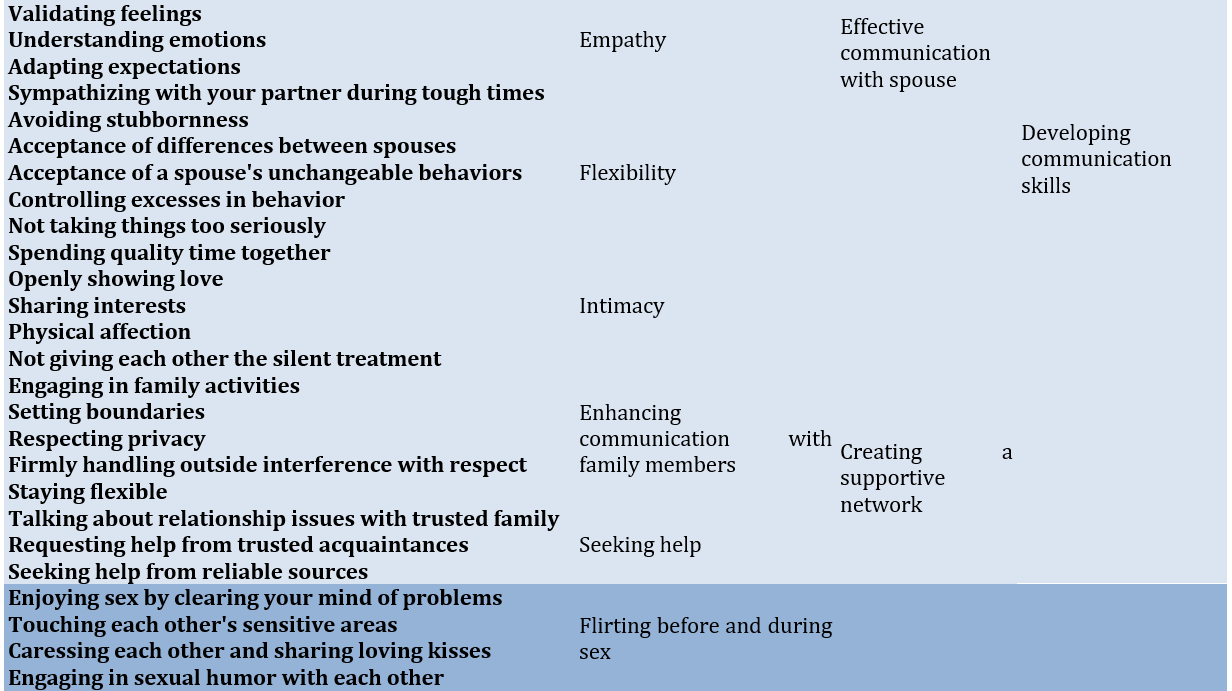
After analyzing the qualitative data, 2650 semantic unit were identified. Through the process of combining overlapping phrases and eliminating similar and duplicate codes, a final set of 76 codes, 23 subcategories, 6 categories and 3 themes were detected which all could be categorized under the umbrella of personal empowerment (Table 3).
Table 3. Promoting behavior of sexual and reproductive health in married woman
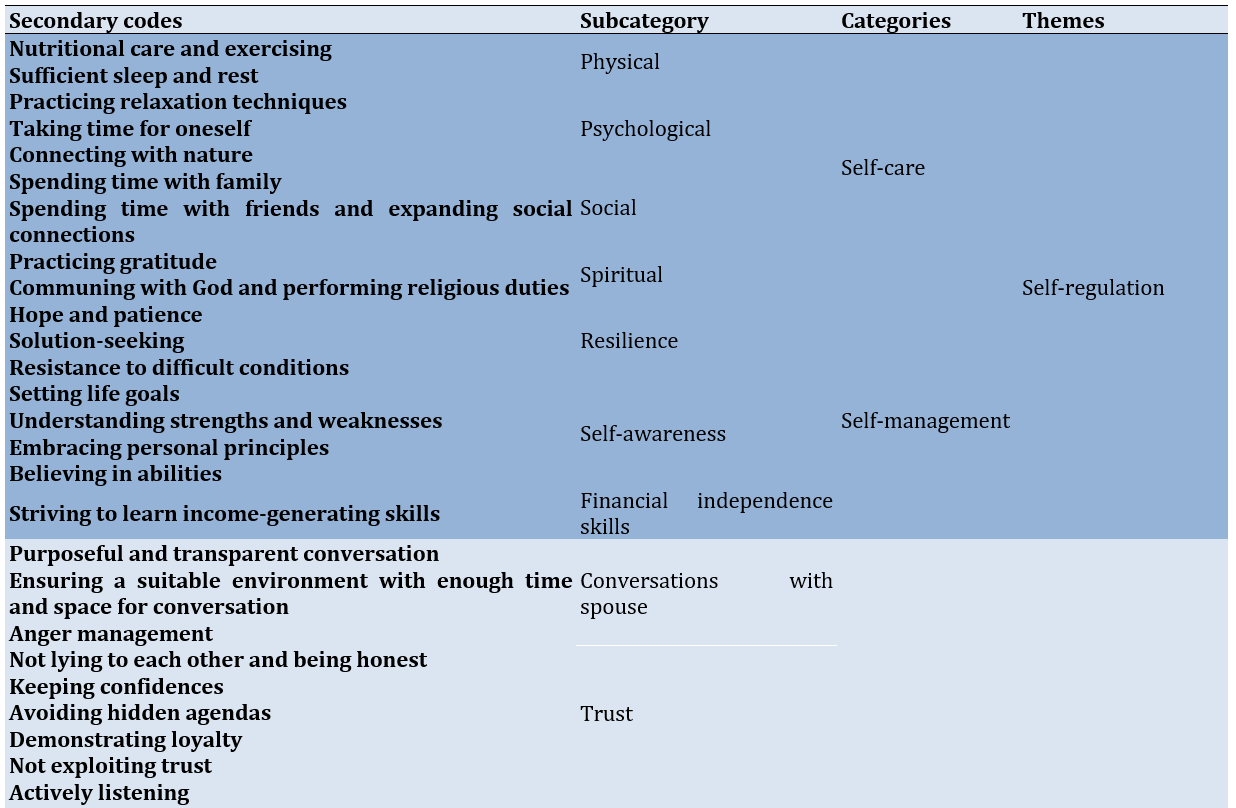
Personal empowerment
This theme was classified in 3 main categories, namely Self-regulation, developing communication skills and the healthy sex life extracted from 7 subcategories.
Self-regulation
Self-regulation encompasses women's focus on self-care and management, empowering them with greater control over their lives for enhanced reproductive and sexual health.
Self-care: Self-care involves routines to maintain physical and mental health, including physical, psychological, social, and spiritual aspects.
Certain women enhanced self-satisfaction and tranquility by maintaining proper nutrition, exercising, getting adequate sleep, grooming well, and practicing good hygiene. Additionally, many people alleviated stress, cleared their minds, and managed anger through soothing music and dance, nature, hobbies, crying, warm showers, positive affirmations, and deep breathing exercises.
This quote reflects it:
“When I sleep well, I engage in my daily walks and follow my special diet, which is "no sugar". It makes me a more positive thinker, happier, and kinder. I also have more energy in my relationship with my spouse”. (participant 11, 37 years old, married for 15 years)
Some participants found serenity and resilience through gratitude, nature, and faith. Others achieved joy and tranquility by avoiding pessimistic people, following motivational content, avoiding self-blame for their spouse's unchangeable actions, and spending quality time with loved ones.
The following quote reflects this:
“Every day, I engage in prayer, expressing gratitude to God for all aspects of my life, and I humbly request His blessing of patience, which brings me a profound sense of peace”. (participant 8, 28 years old, married for 9 years)
Self-management: The self-management category suggests that by actively promoting resilience, self-awareness, and acquiring financial independence skills, women can strengthen their marital relationships and make informed decisions together.
Some women emphasized resilience in reducing tension with their husbands through hope, patience, solution-seeking, and resistance to difficult conditions for marital harmony. They also discovered that self-awareness, including setting life goals, understanding strengths and weaknesses, embracing personal principles, and believing in abilities, boosts self-confidence. Additionally, they viewed involvement in family financial planning and skill development for financial independence as vital for making joint decisions and maintaining individual autonomy effectively.
The following quotes reflects this:
“At times during my marriage, I felt confined and burdened by significant stress from my partner's painful behaviors and my responsibilities toward our children and family. Leaving wasn't an option; I had to find a viable resolution, work hard, and believe that things would improve”. (participant 22, 45 years old, married for 28 years)
“In the past, my rights were entirely under my husband's authority. However, I have now taken control of my finances and gained the freedom to decide how to use my money. This change has led to a heightened sense of self-reliance and ease”. (participant 1, 43 years old, married for 23 years)
Developing communication skills
This main theme includes behaviors aimed at improving relationships with your spouse and those around you, which can enhance decision-making and effectively improve women's sexual health.
Effective communication with spouse: Effective communication between spouses involves conversations with spouse, trust, empathy, flexibility, and intimacy.
Spousal communication involves clear, purposeful conversations, avoiding past hurts, seeking forgiveness, respecting opinions, being open to perspectives, expressing appreciation, actively listening, avoiding arguments, managing emotions, and ensuring a suitable environment with enough time and space for discussions. This quote reflects it:
“I refrain from discussing important matters with my husband during moments when he's tired or when the children are awake because I anticipate that it will inevitably lead to disagreements and conflicts”. (participant 14, 41 years old, married for 26 years)
Trust is built on honesty, confidentiality, avoiding hidden agendas, demonstrating loyalty, and not exploiting trust. These actions alleviate tension, strengthen bonds, and help couples navigate life effectively. A participant's statement exemplifying this concept goes like this:
“I have complete control over my husband's finances due to his unwavering trust in me and confidence that I will handle this responsibility responsibly and without misuse”. (participant 11, 37 years old, married for 15 years)
Demonstrating empathy involves actively listening, validating feelings, understanding emotions, adapting expectations, and sympathizing with your partner during tough times.
“I understand my spouse well. When they come home exhausted and irritable, it's tough, but after eating and sipping tea, they become more tender and compassionate". (participant 18, 26 years old, married for 5 years)
Improving relationships and reducing tension involves a flexible approach: Not overreacting, letting go, avoiding stubbornness, acknowledging differences, and accepting unchangeable behaviors. A sample quote from participants is provided below:
“My partner says I have a binary perspective, seeing things as either completely right or wrong, causing frustration and arguments. I'm working on being more adaptable and open-minded”. (participant 16, 31 years old, married for 9 years)
Participants believe that spending quality time, openly showing love, sharing interests, and physical affection contribute to a nurturing relationship, enhancing closeness, affection, and the bond with one's spouse.
The following statements indicate it:
“Despite struggling to express emotions, I consistently seek moments of tenderness by asking my spouse for a kiss, driven by a strong urge for closeness”. (participant 17, 18 years old, married for 3 years)
Creating a supportive network: Building a robust support system can help reduce tensions, manage daily life problems, control spousal violence, and significantly improve women's sexual health. This involves enhancing communication with family members and seeking help during crucial moments.
Fostering respect, engaging in family activities, setting boundaries, respecting privacy, resisting external interference, staying flexible, and seeking support during difficult times effectively reduce marital stress and prevent spousal violence. One participant stated:
“I've always made it a priority to build a strong bond with my spouse's family by showing them the utmost respect. This effort has fostered their affection for me, which has greatly strengthened my connection with my spouse as well”. (participant 20, 28 years old, married for 4 years)
Some individuals believe that confiding in trustworthy people, informing family members about spousal violence, and seeking help from reliable sources are effective strategies to protect themselves from their spouse's anger and prevent related negative consequences.
“Years ago, my spouse injured me with a knife, but I kept it secret. When he struck me again, causing bruises, I confided in my family. Together, we sought help from a legal clinic and initiated a case against him. As a result, he stopped all violent behavior”. (participant 9, 38 years old, married for 15 years)
Healthy sex life
Behaviors and actions that people take in dealing with their spouses and also individually to improve their sexual performance, prevent unwanted pregnancy and sexually transmitted diseases.
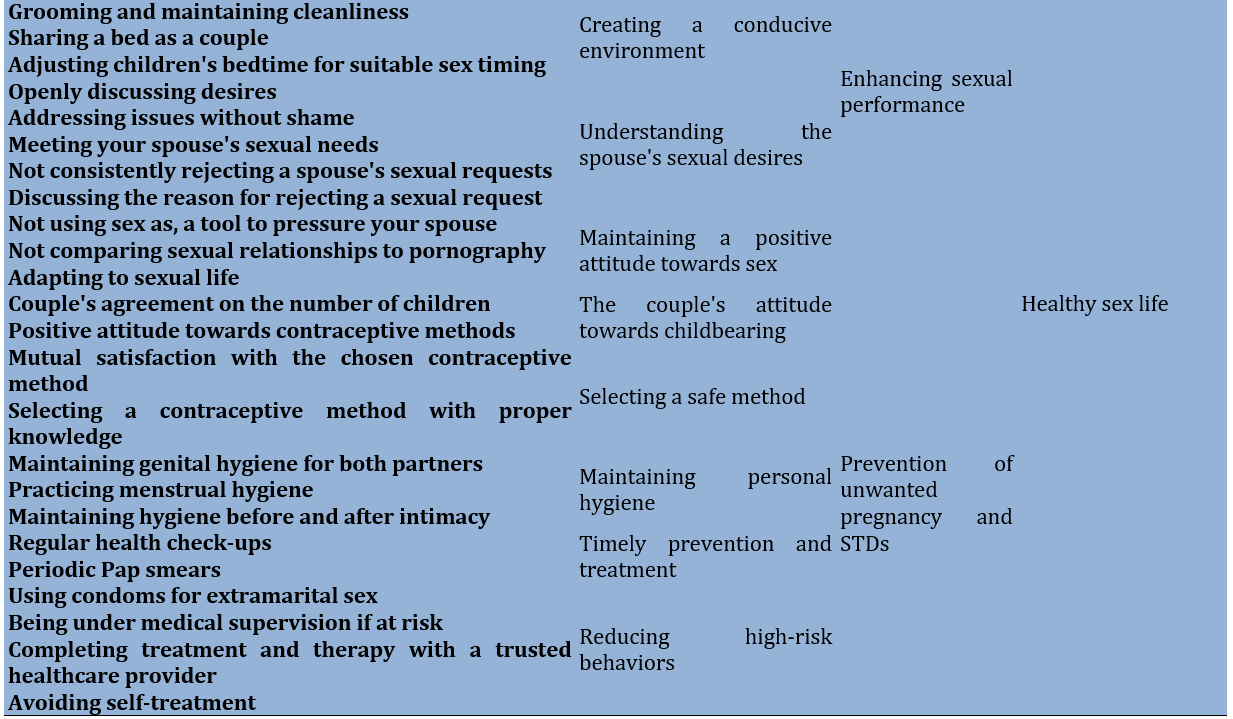
Enhancing sexual performance: Enhancing sexual performance category include flirting before and during sex, creating a conducive environment, understanding the spouse's sexual desires, and maintaining a positive attitude towards sex while being aware of the dynamics of couples' first sexual encounters.
Participants engage in pre-sex banter, caressing, romantic gestures, stimulation, lubrication use, stress relief, enhancing desire, and fully enjoying the experience.
Some participants enhanced self-satisfaction and confidence by grooming and maintaining cleanliness. Others prioritized intimacy by sleeping together and adjusting children's bedtime for suitable sex timing. Here are comments from two participants:
"We schedule sex around the children's sleep. It's not feasible during the day with my husband at work or the children at home”. (participant 10, 38 years old, married for 15 years)
"I quickly change clothes to avoid sweat smells and shower daily. I spray perfume in my hair as my husband likes it. I don't want distance due to hygiene". (participant 1, 43 years old, married for 20 years)
Participants focused on meeting their spouse's sexual needs by understanding their mental states, openly discussing desires, and addressing issues without shame. They viewed sex and communication as vital for enhancing performance and preventing violence.
"I'm not shy about my sexual desires. I openly discuss them with my husband, which greatly improves our sexual relationship”. (participant 11, 42 years old, married for 19 years)
Some participants viewed behaviors like not constantly refusing sexual requests and discussing rejections respectfully as means to maintain closeness with their spouse, fostering peace, and preventing sexual violence and coercion. One participant stated:
“During a period of low mood in my youth, I consistently declined my husband's sexual advances. One day, when I refused again, he became violent, beating me until I struggled to breathe. At that time, I didn't realize this was wrong”. (participant 23, 45 years old, married for 28 years)
Participants noted harmful behaviors like comparing sex to porn, substance use, prolonged abstinence, frequent masturbation, and using sex as pressure on the spouse. These actions decrease self-confidence, increase dissatisfaction, and risk sexual violence.
"I've been hurt in my marriage by my husband's excessive interest in masturbation. It's upsetting and I don't enjoy it". (participant 7, 39 years old, married for 22 years)
Some participants viewed maintaining a positive attitude towards sex and being adaptable as key to fostering intimacy, love, relaxation, and enjoyment in couples.
Participants emphasized the importance of choosing a suitable, tension-free time and place for the couple's first sexual encounter. They advocated discussing marriage desires and sexual needs beforehand to enhance intimacy and manage fears associated with first-time sex.
"On our wedding night, my husband forced sex, causing severe vaginal injury. Stress overwhelmed us, with people waiting outside like spies, making it feel out of our control". (participant 7, 39 years old, married for 22 years)
Prevention of unwanted pregnancy and STDs: Effective preventative measures for both preventing unwanted pregnancy and STDs involved the couple's attitude towards childbearing, selecting a safe method suited to their circumstances, maintaining personal hygiene, timely prevention and treatment, and reducing high-risk behaviors.
Some participants opt for reliable contraception after thorough consideration of factors like cost, availability, ease of use, and satisfaction for both partners.
"Honestly, we tried all the methods, but now everything is expensive and we can't afford It ... because of that, even though I had several unwanted pregnancies and had to have an abortion, the natural method is the best method for us ... It doesn't cost us anything and it's convenient ..." (participant 15, 41 years old, married for 26 years, 4 unwanted pregnancies)
Some participants viewed the couple's decision to not have children, along with maintaining a positive attitude towards contraceptive methods, as effective in preventing unwanted pregnancies.
"My husband is completely against having too many children and if I want to think about a third child, he will divorce me, because of that we are rigidly preventing" (participant 3, 40 years old, married for 20 years)
Some participants believed that maintaining genital hygiene for both men and women, as well as practicing cleanliness during intercourse and menstruation, can help prevent sexually transmitted diseases.
Some participants found periodic checkups and pap smears effective in preventing sexually transmitted diseases and cervical cancer.
"We have to do a pap smear test periodically ... I found out that I have the first stage of cervical cancer during a pap smear" (participant 10, 38 years old, married for 15 years)
Some participants said using condoms in extramarital sexual encounters and seeking professional treatment when feeling at risk of infection, rather than self-medication, to mitigate the risks of high-risk behaviors.
“I experienced severe infections early in my marriage, prompting my doctor to recommend treatment for my husband as well. I suspect his past, unprotected sexual encounters before our marriage contributed to this issue”. (participant 21, 28 years old, married for 4 years)
Discussion
This qualitative study explored the reproductive and sexual health-promoting behaviors of married women of reproductive age. It identified behaviors adopted by women at various life stages to enhance their reproductive and sexual health. The analysis revealed that the main theme of individual empowerment encompasses three categories: Self-regulation, development of communication skills, and fostering a healthy sex life.
Focusing on self-regulation, women engage in self-care routines and stress management techniques. Spiritual practices and gratitude enhance resilience. This promotes self-awareness, goal-setting, and financial independence, boosting confidence. Some studies have shown that, there is a direct association between increasing women's self-awareness and improving their sexual satisfaction [20].
Self-care fosters conscious reactions, reducing mind wandering, enhancing focus and problem-solving, and lowering perceived stress. While physical care can't prevent stress, it increases tolerance [21], and aids emotional regulation, crucial for satisfactory relationships. Satisfied women exhibit better coping, mental health [22], and cohesion with partners, empowering them to make informed decisions.
Developing communication skills is essential for personal empowerment, enhancing marital relationships, and improving sexual health. Effective communication involves clear conversations, trust, empathy, flexibility, and intimacy, fostering a supportive environment and reducing conflicts.
Improving the relationship with a spouse and enhancing negotiation skills can empower women in fertility decision, self-control, and access to health services, including fertility decisions, contraception use, and sexual lives [23, 24]. Effective communication and negotiation with a spouse can be challenging and require patience and practice. If needed, learning these skills from a counselor or therapist can be beneficial [25].
Effective marital relationships are influenced by various factors, including personality traits, age, marriage duration, education, employment status, and economic stability. Traits like conscientiousness and agreeableness promote positive relationships and harmony. Strong communication and conflict management skills enhance satisfaction, trust, mutual control, and affection [26, 27]. Additionally, the balance of decision-making authority and financial power affects communication. Imbalances can make one partner feel unheard or afraid to express themselves. Creating an environment of mutual respect, equality, and joint decision-making can help. Cultural differences can also impact communication, leading to misunderstandings and conflicts [28, 29].
Effective anger management is crucial for a healthy marital relationship. Uncontrolled anger can hinder communication, leading to shouting, blaming, defensiveness, and even physical violence. It disrupts problem-solving and decision-making abilities, making it harder to find solutions [30, 31]. Effective communication improves reproductive and sexual health in married women by fostering understanding, addressing contraceptive use, preventing violence, and enhancing sexual performance.
In the context of personal empowerment, fostering a healthy sex life was crucial for improving sexual performance, preventing unwanted pregnancies, and avoiding sexually transmitted diseases. Women enhance their sexual experiences through behaviors such as flirting, romantic gestures, maintaining a positive attitude towards sex. Women who view sex positively are more likely to experience desire and satisfaction, while those who see it negatively may face dysfunction and understanding their spouse's desires [32, 33]. Observing personal hygiene [34] creating conducive environments for intimacy also play significant roles. Effective communication about sexual needs and preferences helps prevent conflicts and violence. Participants highlighted the importance of contraception, genital hygiene, and periodic medical checkups for overall sexual health [35, 36]. Additionally, seeking family planning counseling at health centers enhances awareness and effectiveness of contraceptive methods [37].
Behaviors that prevent sexually transmitted diseases (STDs) were vital for a healthy sex life in women. Seeking information about STDs reduces risky behaviors. Using condoms during intercourse, though uncommon in Iranian society due to cultural attitudes and lack of awareness, is effective in prevention [38]. Negative cultural views and taboos around sexual discussion hinder condom use, especially outside marriage, increasing STD risk.
Limitations of the study
However, these individual behaviors alone are not sufficient to promote the fertility and sexual health of women. This study primarily examines the behaviors that promote fertility and sexual health of women at the individual level. Although attempts have been made in this research to consider the influential factors on the occurrence of behaviors, the actions of husbands, environmental and cultural factors, as well as individual living conditions play a determining role in achieving the enhancement of their fertility and sexual health.
In the current study, four married women under the age of 25 who met the study criteria were included in the study. However, due to their young age and short duration of marriage, the researcher was unable to extract behaviors promoting fertility and sexual health from the interviews conducted with them. Therefore, they were excluded from the interviews. As typical in qualitative studies, findings have limited generalizability, particularly as the study focused on a small sample of women in Kurdistan. Therefore, caution is advised when extending these findings to other women.
Conclusion
Women adopt various behaviors to enhance their fertility and sexual health. These behaviors include self-regulation, improved communication with spouses and relatives, and maintaining a healthy sexual life. Additionally, empowering behaviors and positive interpersonal relationships increases satisfaction with married life and improve women's sexual performance.
Acknowledgments: The authors would like to express their gratitude to all the participants who took part in the study.
Ethical Permissions: After introducing the study, the objectives were explained to the participants, and they were assured that all data would be kept confidential. All participants signed the informed consent forms. informed consent was obtained from all subjects. Code of Ethics received from Shahid Beheshti University of Medical Sciences: IR.SBMU.PHARMACY.REC.1399.201. Approval statement is “The project was found to be in accordance with the ethical principles and the national norms and standards for conducting medical research in Iran”.
Conflicts of Interests: The authors declare no conflict of interest.
Authors' Contribution: Babaei M (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer/Statistical Analyst (55%); Simbar M (Second Author), Introduction Writer/Methodologist/Discussion Writer/Statistical Analyst (20%); Alavi Majd H (Third Author), Statistical Analyst (5%); Nahidi F (Fourth Author), Introduction Writer/Methodologist/Discussion Writer/Statistical Analyst (20%)
Funding/Support: Shahid Beheshti University of Medical Sciences.
Improvement of women's health is a comprehensive approach that significantly impacts a country's long-term development strategies and economic progress [1]. Reproductive and sexual health is crucial for women's overall well-being. It ensures healthy sexual lives, reproductive capabilities, and informed decisions. Improving SRH (Sexual and Reproductive Health) supports sustainable development goals, particularly in achieving gender equality and enhancing health and well-being for all [2, 3].
Globally, reproductive and sexual health issues among women represent a substantial proportion of health-related challenges. Enhancing these aspects of health not only empowers women to gain greater control over their well-being but also addresses underlying factors that influence health outcomes [4, 5]. Promoting sexual health involves empowering individuals to manage and enhance their sexual well-being [6]. This can help prevent sexually transmitted diseases, avoid unintended pregnancies, and improve sexual performance [7]. Furthermore, sexual and reproductive health promotion extends beyond clinical aspects to include a wide range of choices, behaviors, and social impacts [8]. It seems that there are multiple individual and interpersonal factors that can influence the adoption of behaviors promoting reproductive and sexual health [9, 10]. In Abedi et al.'s study, a significant relationship was observed between various dimensions of a health-promoting lifestyle, such as responsibility, interpersonal relationships, and stress management, and all aspects of sexual functioning in women of reproductive age [11]. Family responsibilities, environmental pressures, financial pressures, family and social support networks, and inadequate communication are among the barriers that can affect the promotion of sexual and reproductive health [12].
In a study conducted in Iran, women took measures to improve their reproductive health by making informed decisions, engaging in self-care behaviors, having satisfactory sexual relationships through discussing their needs and desires, and striving to resolve sexual issues. Effective communication between couples and joint decision-making were also identified as actions that prevent unwanted pregnancies and enhance women's reproductive health [13]. In another study, the use of condoms, traditional medicine, antibiotics, and disinfecting and cleaning oneself after sexual intercourse were among the preventive behaviors identified for maintaining reproductive and sexual health and preventing sexually transmitted infections [14]. In the study by Cipres et al., it was observed that women used various strategies to reduce the risk of sexually transmitted infections, including condom use, asking partners about STIs (Sexually Transmitted Infections), frequent STI screening, and inquiring about their partners' other sexual partners. It also appears that another factor influencing the incidence of sexually transmitted infections in women is related to power inequities in sexual partnerships [15]. Married women face multiple roles and responsibilities, and the nature of their marital relationship can greatly influence their reproductive and sexual health [16]. Numerous studies have been conducted on health-promoting lifestyles among women of reproductive age in Iran and around the world. However, there has not been a study specifically examining health-promoting reproductive and sexual behaviors in the particular group of married women of reproductive age.
Differences in healthy behaviors across cultures highlight the significant impact of cultural and religious contexts on women's reproductive and sexual health. Context is critical for understanding health behavior, and its importance is emphasized for planning behavior change interventions and policies [17]. Each society's unique value system influences these behaviors, underscoring the need for qualitative studies to understand women's perspectives. Such studies are crucial for developing tailored health services and interventions. The absence of qualitative research on married women of reproductive age in Iran, despite their vital role in family and community health, motivated this study to explore their experiences regarding health-promoting sexual and reproductive behaviors.
Participants and Methods
The current research was conducted between December 2019 and March 2022 in Sanandaj, the capital of Kurdistan province in western Iran.
The qualitative study utilized a conventional content analysis approach to gain deeper insights into the experiences of married women regarding promotion behaviors related to sexual and reproductive health. Sampling took place at two health centers with high visitor numbers, located in distinct regions characterized by various social and economic levels. The research population comprised women attending urban healthcare centers in Sanandaj. Sampling was purposeful, aiming for maximum diversity in age, education levels of both women and their spouses, family income status, occupations of both women and their spouses, number of children, and place of residence. Sampling continued until data saturation was achieved. The inclusion criteria encompassed women aged 15-49 years, Iranian nationality, ability to communicate effectively with the researcher, not being pregnant, and willingness to participate in the study.
The study's exit conditions encompass any distinct physical or psychological ailment that hinders the participant's involvement in the research including pregnancy. The interviews were conducted solely by the first author, who possesses extensive expertise in qualitative research. A total of 23 interviews were conducted, and to ensure comprehensive coverage, three additional participants were interviewed once data saturation was reached. Additionally, to enrich the insights gleaned from participant interviews, discussions were held with 6 specialists. The participants were interviewed at specific locations and times as arranged. Due to the widespread occurrence of COVID-19, interviews took place in various settings such as parks, open areas, and occasionally at the participants' homes. Key informant interviews were conducted using online methods. Information was collected through semi-structured and comprehensive interviews with women. Field notes were taken, and audio recording was conducted with participants' consent. Additionally, insights were derived from participants' nonverbal cues. Occasionally, participants requested to temporarily pause the recording during the interview to share information more comfortably. In such cases, the interviews were paused, and the details were transcribed. These transcribed sections were promptly reviewed and edited. At the start of the interview, a series of broad and open-ended inquiries were employed. The interview started with a general and open question.
Search engine queries were used as needed to ask detailed questions, including seeking further elaboration, clarification, specific details, examples, and consideration of additional factors related to discussed behaviors. Participants were also encouraged to share any additional insights they wished to offer and invited to address any questions not asked. Permission for future interviews was obtained. Participants freely expressed viewpoints through unbiased inquiries, with opportunities to share experiences. Interviews lasted 40 to 90 minutes, allowing broad perspectives to emerge.
Data analysis
This study utilized content analysis following the steps proposed by Graneheim & Lundman [18]. After each interview, the researcher listened to the recordings multiple times for comprehension, transcribed the data manually, and then typed them. Analysis was conducted using MAXQDA10 software (version 10). Initial categorization occurred concurrently with interviews, with units of meaning condensed into codes, organized based on commonalities and distinctions, resulting in subcategories. These subcategories were grouped into categories, and fundamental themes were identified.
To ensure data accuracy and robustness, Guba & Lincoln's fourfold criteria were applied, focusing on dependability, transferability, credibility, and confirmability [19]. To boost data credibility, the first author used three methods over a year: Extensive data work, cross-checking notes with participants for alignment, and verifying codes and categories with the research team. A mixed data collection approach was employed, including interviews, observations, and written materials.
When participants couldn't review texts due to literacy or time constraints, segments needing clarification were revisited through various means. Texts were reviewed and modified if necessary. Sample diversity was ensured to enhance data credibility. Reliability was ensured by recording interviews in audio and handwritten forms, with a 2-week gap for comparison. Identical questions were asked to all participants, validated by two qualitative researchers.
Confirmability was maintained through review by two faculty members, extending to data analysis procedures. For transferability, the research methodology provided comprehensive descriptions of the study population and contextual details.
The datasets generated and/or analyzed during the current study are not publicly available due to privacy protection of the participants but are available from the corresponding author on reasonable request.
Findings
The age of the women ranged from 18 to 45 years. Women had varying levels of education, ranging from being illiterate to holding a master's degree (Tables 1 & 2).
Table 1. Demographic characteristics of participants
Table 2. Demographic characteristics of specialists
After analyzing the qualitative data, 2650 semantic unit were identified. Through the process of combining overlapping phrases and eliminating similar and duplicate codes, a final set of 76 codes, 23 subcategories, 6 categories and 3 themes were detected which all could be categorized under the umbrella of personal empowerment (Table 3).
Table 3. Promoting behavior of sexual and reproductive health in married woman
Personal empowerment
This theme was classified in 3 main categories, namely Self-regulation, developing communication skills and the healthy sex life extracted from 7 subcategories.
Self-regulation
Self-regulation encompasses women's focus on self-care and management, empowering them with greater control over their lives for enhanced reproductive and sexual health.
Self-care: Self-care involves routines to maintain physical and mental health, including physical, psychological, social, and spiritual aspects.
Certain women enhanced self-satisfaction and tranquility by maintaining proper nutrition, exercising, getting adequate sleep, grooming well, and practicing good hygiene. Additionally, many people alleviated stress, cleared their minds, and managed anger through soothing music and dance, nature, hobbies, crying, warm showers, positive affirmations, and deep breathing exercises.
This quote reflects it:
“When I sleep well, I engage in my daily walks and follow my special diet, which is "no sugar". It makes me a more positive thinker, happier, and kinder. I also have more energy in my relationship with my spouse”. (participant 11, 37 years old, married for 15 years)
Some participants found serenity and resilience through gratitude, nature, and faith. Others achieved joy and tranquility by avoiding pessimistic people, following motivational content, avoiding self-blame for their spouse's unchangeable actions, and spending quality time with loved ones.
The following quote reflects this:
“Every day, I engage in prayer, expressing gratitude to God for all aspects of my life, and I humbly request His blessing of patience, which brings me a profound sense of peace”. (participant 8, 28 years old, married for 9 years)
Self-management: The self-management category suggests that by actively promoting resilience, self-awareness, and acquiring financial independence skills, women can strengthen their marital relationships and make informed decisions together.
Some women emphasized resilience in reducing tension with their husbands through hope, patience, solution-seeking, and resistance to difficult conditions for marital harmony. They also discovered that self-awareness, including setting life goals, understanding strengths and weaknesses, embracing personal principles, and believing in abilities, boosts self-confidence. Additionally, they viewed involvement in family financial planning and skill development for financial independence as vital for making joint decisions and maintaining individual autonomy effectively.
The following quotes reflects this:
“At times during my marriage, I felt confined and burdened by significant stress from my partner's painful behaviors and my responsibilities toward our children and family. Leaving wasn't an option; I had to find a viable resolution, work hard, and believe that things would improve”. (participant 22, 45 years old, married for 28 years)
“In the past, my rights were entirely under my husband's authority. However, I have now taken control of my finances and gained the freedom to decide how to use my money. This change has led to a heightened sense of self-reliance and ease”. (participant 1, 43 years old, married for 23 years)
Developing communication skills
This main theme includes behaviors aimed at improving relationships with your spouse and those around you, which can enhance decision-making and effectively improve women's sexual health.
Effective communication with spouse: Effective communication between spouses involves conversations with spouse, trust, empathy, flexibility, and intimacy.
Spousal communication involves clear, purposeful conversations, avoiding past hurts, seeking forgiveness, respecting opinions, being open to perspectives, expressing appreciation, actively listening, avoiding arguments, managing emotions, and ensuring a suitable environment with enough time and space for discussions. This quote reflects it:
“I refrain from discussing important matters with my husband during moments when he's tired or when the children are awake because I anticipate that it will inevitably lead to disagreements and conflicts”. (participant 14, 41 years old, married for 26 years)
Trust is built on honesty, confidentiality, avoiding hidden agendas, demonstrating loyalty, and not exploiting trust. These actions alleviate tension, strengthen bonds, and help couples navigate life effectively. A participant's statement exemplifying this concept goes like this:
“I have complete control over my husband's finances due to his unwavering trust in me and confidence that I will handle this responsibility responsibly and without misuse”. (participant 11, 37 years old, married for 15 years)
Demonstrating empathy involves actively listening, validating feelings, understanding emotions, adapting expectations, and sympathizing with your partner during tough times.
“I understand my spouse well. When they come home exhausted and irritable, it's tough, but after eating and sipping tea, they become more tender and compassionate". (participant 18, 26 years old, married for 5 years)
Improving relationships and reducing tension involves a flexible approach: Not overreacting, letting go, avoiding stubbornness, acknowledging differences, and accepting unchangeable behaviors. A sample quote from participants is provided below:
“My partner says I have a binary perspective, seeing things as either completely right or wrong, causing frustration and arguments. I'm working on being more adaptable and open-minded”. (participant 16, 31 years old, married for 9 years)
Participants believe that spending quality time, openly showing love, sharing interests, and physical affection contribute to a nurturing relationship, enhancing closeness, affection, and the bond with one's spouse.
The following statements indicate it:
“Despite struggling to express emotions, I consistently seek moments of tenderness by asking my spouse for a kiss, driven by a strong urge for closeness”. (participant 17, 18 years old, married for 3 years)
Creating a supportive network: Building a robust support system can help reduce tensions, manage daily life problems, control spousal violence, and significantly improve women's sexual health. This involves enhancing communication with family members and seeking help during crucial moments.
Fostering respect, engaging in family activities, setting boundaries, respecting privacy, resisting external interference, staying flexible, and seeking support during difficult times effectively reduce marital stress and prevent spousal violence. One participant stated:
“I've always made it a priority to build a strong bond with my spouse's family by showing them the utmost respect. This effort has fostered their affection for me, which has greatly strengthened my connection with my spouse as well”. (participant 20, 28 years old, married for 4 years)
Some individuals believe that confiding in trustworthy people, informing family members about spousal violence, and seeking help from reliable sources are effective strategies to protect themselves from their spouse's anger and prevent related negative consequences.
“Years ago, my spouse injured me with a knife, but I kept it secret. When he struck me again, causing bruises, I confided in my family. Together, we sought help from a legal clinic and initiated a case against him. As a result, he stopped all violent behavior”. (participant 9, 38 years old, married for 15 years)
Healthy sex life
Behaviors and actions that people take in dealing with their spouses and also individually to improve their sexual performance, prevent unwanted pregnancy and sexually transmitted diseases.
Enhancing sexual performance: Enhancing sexual performance category include flirting before and during sex, creating a conducive environment, understanding the spouse's sexual desires, and maintaining a positive attitude towards sex while being aware of the dynamics of couples' first sexual encounters.
Participants engage in pre-sex banter, caressing, romantic gestures, stimulation, lubrication use, stress relief, enhancing desire, and fully enjoying the experience.
Some participants enhanced self-satisfaction and confidence by grooming and maintaining cleanliness. Others prioritized intimacy by sleeping together and adjusting children's bedtime for suitable sex timing. Here are comments from two participants:
"We schedule sex around the children's sleep. It's not feasible during the day with my husband at work or the children at home”. (participant 10, 38 years old, married for 15 years)
"I quickly change clothes to avoid sweat smells and shower daily. I spray perfume in my hair as my husband likes it. I don't want distance due to hygiene". (participant 1, 43 years old, married for 20 years)
Participants focused on meeting their spouse's sexual needs by understanding their mental states, openly discussing desires, and addressing issues without shame. They viewed sex and communication as vital for enhancing performance and preventing violence.
"I'm not shy about my sexual desires. I openly discuss them with my husband, which greatly improves our sexual relationship”. (participant 11, 42 years old, married for 19 years)
Some participants viewed behaviors like not constantly refusing sexual requests and discussing rejections respectfully as means to maintain closeness with their spouse, fostering peace, and preventing sexual violence and coercion. One participant stated:
“During a period of low mood in my youth, I consistently declined my husband's sexual advances. One day, when I refused again, he became violent, beating me until I struggled to breathe. At that time, I didn't realize this was wrong”. (participant 23, 45 years old, married for 28 years)
Participants noted harmful behaviors like comparing sex to porn, substance use, prolonged abstinence, frequent masturbation, and using sex as pressure on the spouse. These actions decrease self-confidence, increase dissatisfaction, and risk sexual violence.
"I've been hurt in my marriage by my husband's excessive interest in masturbation. It's upsetting and I don't enjoy it". (participant 7, 39 years old, married for 22 years)
Some participants viewed maintaining a positive attitude towards sex and being adaptable as key to fostering intimacy, love, relaxation, and enjoyment in couples.
Participants emphasized the importance of choosing a suitable, tension-free time and place for the couple's first sexual encounter. They advocated discussing marriage desires and sexual needs beforehand to enhance intimacy and manage fears associated with first-time sex.
"On our wedding night, my husband forced sex, causing severe vaginal injury. Stress overwhelmed us, with people waiting outside like spies, making it feel out of our control". (participant 7, 39 years old, married for 22 years)
Prevention of unwanted pregnancy and STDs: Effective preventative measures for both preventing unwanted pregnancy and STDs involved the couple's attitude towards childbearing, selecting a safe method suited to their circumstances, maintaining personal hygiene, timely prevention and treatment, and reducing high-risk behaviors.
Some participants opt for reliable contraception after thorough consideration of factors like cost, availability, ease of use, and satisfaction for both partners.
"Honestly, we tried all the methods, but now everything is expensive and we can't afford It ... because of that, even though I had several unwanted pregnancies and had to have an abortion, the natural method is the best method for us ... It doesn't cost us anything and it's convenient ..." (participant 15, 41 years old, married for 26 years, 4 unwanted pregnancies)
Some participants viewed the couple's decision to not have children, along with maintaining a positive attitude towards contraceptive methods, as effective in preventing unwanted pregnancies.
"My husband is completely against having too many children and if I want to think about a third child, he will divorce me, because of that we are rigidly preventing" (participant 3, 40 years old, married for 20 years)
Some participants believed that maintaining genital hygiene for both men and women, as well as practicing cleanliness during intercourse and menstruation, can help prevent sexually transmitted diseases.
Some participants found periodic checkups and pap smears effective in preventing sexually transmitted diseases and cervical cancer.
"We have to do a pap smear test periodically ... I found out that I have the first stage of cervical cancer during a pap smear" (participant 10, 38 years old, married for 15 years)
Some participants said using condoms in extramarital sexual encounters and seeking professional treatment when feeling at risk of infection, rather than self-medication, to mitigate the risks of high-risk behaviors.
“I experienced severe infections early in my marriage, prompting my doctor to recommend treatment for my husband as well. I suspect his past, unprotected sexual encounters before our marriage contributed to this issue”. (participant 21, 28 years old, married for 4 years)
Discussion
This qualitative study explored the reproductive and sexual health-promoting behaviors of married women of reproductive age. It identified behaviors adopted by women at various life stages to enhance their reproductive and sexual health. The analysis revealed that the main theme of individual empowerment encompasses three categories: Self-regulation, development of communication skills, and fostering a healthy sex life.
Focusing on self-regulation, women engage in self-care routines and stress management techniques. Spiritual practices and gratitude enhance resilience. This promotes self-awareness, goal-setting, and financial independence, boosting confidence. Some studies have shown that, there is a direct association between increasing women's self-awareness and improving their sexual satisfaction [20].
Self-care fosters conscious reactions, reducing mind wandering, enhancing focus and problem-solving, and lowering perceived stress. While physical care can't prevent stress, it increases tolerance [21], and aids emotional regulation, crucial for satisfactory relationships. Satisfied women exhibit better coping, mental health [22], and cohesion with partners, empowering them to make informed decisions.
Developing communication skills is essential for personal empowerment, enhancing marital relationships, and improving sexual health. Effective communication involves clear conversations, trust, empathy, flexibility, and intimacy, fostering a supportive environment and reducing conflicts.
Improving the relationship with a spouse and enhancing negotiation skills can empower women in fertility decision, self-control, and access to health services, including fertility decisions, contraception use, and sexual lives [23, 24]. Effective communication and negotiation with a spouse can be challenging and require patience and practice. If needed, learning these skills from a counselor or therapist can be beneficial [25].
Effective marital relationships are influenced by various factors, including personality traits, age, marriage duration, education, employment status, and economic stability. Traits like conscientiousness and agreeableness promote positive relationships and harmony. Strong communication and conflict management skills enhance satisfaction, trust, mutual control, and affection [26, 27]. Additionally, the balance of decision-making authority and financial power affects communication. Imbalances can make one partner feel unheard or afraid to express themselves. Creating an environment of mutual respect, equality, and joint decision-making can help. Cultural differences can also impact communication, leading to misunderstandings and conflicts [28, 29].
Effective anger management is crucial for a healthy marital relationship. Uncontrolled anger can hinder communication, leading to shouting, blaming, defensiveness, and even physical violence. It disrupts problem-solving and decision-making abilities, making it harder to find solutions [30, 31]. Effective communication improves reproductive and sexual health in married women by fostering understanding, addressing contraceptive use, preventing violence, and enhancing sexual performance.
In the context of personal empowerment, fostering a healthy sex life was crucial for improving sexual performance, preventing unwanted pregnancies, and avoiding sexually transmitted diseases. Women enhance their sexual experiences through behaviors such as flirting, romantic gestures, maintaining a positive attitude towards sex. Women who view sex positively are more likely to experience desire and satisfaction, while those who see it negatively may face dysfunction and understanding their spouse's desires [32, 33]. Observing personal hygiene [34] creating conducive environments for intimacy also play significant roles. Effective communication about sexual needs and preferences helps prevent conflicts and violence. Participants highlighted the importance of contraception, genital hygiene, and periodic medical checkups for overall sexual health [35, 36]. Additionally, seeking family planning counseling at health centers enhances awareness and effectiveness of contraceptive methods [37].
Behaviors that prevent sexually transmitted diseases (STDs) were vital for a healthy sex life in women. Seeking information about STDs reduces risky behaviors. Using condoms during intercourse, though uncommon in Iranian society due to cultural attitudes and lack of awareness, is effective in prevention [38]. Negative cultural views and taboos around sexual discussion hinder condom use, especially outside marriage, increasing STD risk.
Limitations of the study
However, these individual behaviors alone are not sufficient to promote the fertility and sexual health of women. This study primarily examines the behaviors that promote fertility and sexual health of women at the individual level. Although attempts have been made in this research to consider the influential factors on the occurrence of behaviors, the actions of husbands, environmental and cultural factors, as well as individual living conditions play a determining role in achieving the enhancement of their fertility and sexual health.
In the current study, four married women under the age of 25 who met the study criteria were included in the study. However, due to their young age and short duration of marriage, the researcher was unable to extract behaviors promoting fertility and sexual health from the interviews conducted with them. Therefore, they were excluded from the interviews. As typical in qualitative studies, findings have limited generalizability, particularly as the study focused on a small sample of women in Kurdistan. Therefore, caution is advised when extending these findings to other women.
Conclusion
Women adopt various behaviors to enhance their fertility and sexual health. These behaviors include self-regulation, improved communication with spouses and relatives, and maintaining a healthy sexual life. Additionally, empowering behaviors and positive interpersonal relationships increases satisfaction with married life and improve women's sexual performance.
Acknowledgments: The authors would like to express their gratitude to all the participants who took part in the study.
Ethical Permissions: After introducing the study, the objectives were explained to the participants, and they were assured that all data would be kept confidential. All participants signed the informed consent forms. informed consent was obtained from all subjects. Code of Ethics received from Shahid Beheshti University of Medical Sciences: IR.SBMU.PHARMACY.REC.1399.201. Approval statement is “The project was found to be in accordance with the ethical principles and the national norms and standards for conducting medical research in Iran”.
Conflicts of Interests: The authors declare no conflict of interest.
Authors' Contribution: Babaei M (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer/Statistical Analyst (55%); Simbar M (Second Author), Introduction Writer/Methodologist/Discussion Writer/Statistical Analyst (20%); Alavi Majd H (Third Author), Statistical Analyst (5%); Nahidi F (Fourth Author), Introduction Writer/Methodologist/Discussion Writer/Statistical Analyst (20%)
Funding/Support: Shahid Beheshti University of Medical Sciences.
Article Type: Qualitative Research |
Subject:
Sexual Health Education/Promotion
Received: 2024/05/26 | Accepted: 2024/08/11 | Published: 2024/08/30
Received: 2024/05/26 | Accepted: 2024/08/11 | Published: 2024/08/30
References
1. Joulaei H, Maharlouei N, Lankarani KB, Razzaghi A, Akbari M. Narrative review of women's health in Iran: Challenges and successes. Int J Equity Health. 2016;15:25. [Link] [DOI:10.1186/s12939-016-0316-x]
2. Edwards WM, Coleman E. Defining sexual health: A descriptive overview. Arch Sex Behav. 2004;33(3):189-95. [Link] [DOI:10.1023/B:ASEB.0000026619.95734.d5]
3. Mohamad Taghvaee V, Assari Arani A, Nodehi M, Khodaparast Shirazi J, Agheli L, Neshat Ghojogh HM, et al. Sustainable development goals: Transportation, health and public policy. Rev Econ Polit Sci. 2023;8(2):134-61. [Link] [DOI:10.1108/REPS-12-2019-0168]
4. Bacchus LJ, Colombini M, Pearson I, Gevers A, Stöckl H, Guedes AC. Interventions that prevent or respond to intimate partner violence against women and violence against children: A systematic review. Lancet Public Health. 2024;9(5):e326-38. [Link] [DOI:10.1016/S2468-2667(24)00048-3]
5. Pender NJ, Murdaugh CL, Parsons MA. Health promotion in nursing practice. Hoboken: Prentice Hall; 2006. [Link]
6. Eisenberg ME, Bernat DH, Bearinger LH, Resnick MD. Support for comprehensive sexuality education: Perspectives from parents of school-age youth. J Adolesc Health. 2008;42(4):352-9. [Link] [DOI:10.1016/j.jadohealth.2007.09.019]
7. PAHO. Promoting sexual health: Recommendations for action. Washington, DC: Pan American Health Organization; 2000. [Link]
8. Leekuan P, Kane R, Sukwong P, Kulnitichai W. Understanding sexual and reproductive health from the perspective of late adolescents in Northern Thailand: A phenomenological study. Reprod Health. 2022;19(1):230. [Link] [DOI:10.1186/s12978-022-01528-1]
9. Morowatisharifabad MA, Rahimi T, Farajkhoda T, Fallahzadeh H, Mohebi S. Exploring the feelings of Iranian women of reproductive age about health care seeking behavior: A qualitative study. Health Promot Perspect. 2018;8(1):71-8. [Link] [DOI:10.15171/hpp.2018.09]
10. Maryam B, Fatemeh S, Nourossadat K, Saeideh N, Giti O. Women's awareness of ovarian cancer risk factors and symptoms in Western Iran in 2020-2021. BMC Womens Health. 2022;22(1):192. [Link] [DOI:10.1186/s12905-022-01779-x]
11. Abedi P, Jorfi M, Afshari P, Fakhri A. How does health-promoting lifestyle relate to sexual function among women of reproductive age in Iran?. Glob Health Promot. 2018;25(3):15-21. [Link] [DOI:10.1177/1757975917706831]
12. Darebo TD, Spigt M, Teklewold B, Badacho AS, Mayer N, Teklewold M. The sexual and reproductive healthcare challenges when dealing with female migrants and refugees in low and middle-income countries (a qualitative evidence synthesis). BMC Public Health. 2024;24(1):520. [Link] [DOI:10.1186/s12889-024-17916-0]
13. Bakht R, Dolatian M, Hajian S, Montazeri A, Majd HA, Zare E. Women's reproductive health literacy: A qualitative study. Int J Womens Health Reprod Sci. 2023;11(1):16-24. [Link] [DOI:10.15296/ijwhr.2023.04]
14. Fauziah M, Rabbany NN. Behavioral prevention of sexual transmitted infections in female sexual workers in Puncak, Bogor. Int J Healthc Res. 2018;1(2):50-8. [Link] [DOI:10.12928/ijhr.v1i2.754]
15. Cipres D, Rodriguez A, Alvarez J, Stern L, Steinauer J, Seidman D. Racial/ethnic differences in young women's health-promoting strategies to reduce vulnerability to sexually transmitted infections. J Adolesc Health. 2017;60(5):556-62. [Link] [DOI:10.1016/j.jadohealth.2016.11.024]
16. Lim S, Raymo JM. Marriage and women's health in Japan. J Marriage Fam. 2016;78(3):780-96. [Link] [DOI:10.1111/jomf.12298]
17. Perski O, Keller J, Kale D, Asare BY, Schneider V, Powell D, et al. Understanding health behaviours in context: A systematic review and meta-analysis of ecological momentary assessment studies of five key health behaviours. Health Psychol Rev. 2022;16(4):576-601. [Link] [DOI:10.1080/17437199.2022.2112258]
18. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105-12. [Link] [DOI:10.1016/j.nedt.2003.10.001]
19. Guba EG, Lincoln YS. Competing paradigms in qualitative research. In: Handbook of qualitative research. Washington DC: Sage Publications; 1994. p. 105-17. [Link]
20. Moodi S, Mehrbakhsh Z, Amtaeh F, Moghasemi S. Comparing the self-awareness and problem-solving skills training on sexual desire of newly married women: A field trial study. J Educ Health Promot. 2023;12:226. [Link] [DOI:10.4103/jehp.jehp_739_22]
21. Bernstein EE, McNally RJ. Exercise as a buffer against difficulties with emotion regulation: A pathway to emotional wellbeing. Behav Res Ther. 2018;109:29-36. [Link] [DOI:10.1016/j.brat.2018.07.010]
22. Afshani AR, ShiriMohammadabad H. The study of relationship between life satisfaction and social health of Yazd city women. Tolooe Behdasht. 2016;15(2):34-44. [Persian] [Link]
23. Osamor PE, Grady C. Women's autonomy in health care decision-making in developing countries: A synthesis of the literature. Int J Womens Health. 2016;8:191-202. [Link] [DOI:10.2147/IJWH.S105483]
24. Kariman N, Simbar M, Ahmadi F, Vedadhir AA. Socioeconomic and emotional predictors of decision making for timing motherhood among Iranian women in 2013. Iran Red Crescent Med J. 2014;16(2):e13629. [Link] [DOI:10.5812/ircmj.13629]
25. Mataji Amirroud M, Ghaffari M, Ramezankhani A, Soori H. Barriers to empowering assertive behavior in dealing with spousal violence in Iranian married women: A qualitative approach. J Aggress Maltreatment Trauma. 2024;33(4):451-71. [Link] [DOI:10.1080/10926771.2023.2240249]
26. Soltani Ramezan Zadeh M, Rasoulian M, Mohammadsadeghi H, Ahmadzad-Asl M, Nohesara S, Soraya S, et al. The effect of communication skills training and conflict resolution tactics on marital satisfaction of married women in Kermanshah. J Iran Med Counc. 2020;3(2):79-88. [Link]
27. Abolghasemi J, Jafari F, Samani LN, Rimaz S. Predictors of marital satisfaction among reproductive-age women based on personality traits: A study in Iran. Cureus. 2024;16(5):e59610. [Link] [DOI:10.7759/cureus.59610]
28. Etemadifrd S. Decision-making patterns among Iranian family members. OIDA Int J Sustain Dev. 2015;8(10):21-8. [Link]
29. Vizheh M, Zurynski Y, Braithwaite J, Moghadam ZB, Rapport F. Impact of agency on Iranian women's access to and utilisation of reproductive healthcare services: A qualitative study. Sex Res Soc Policy. 2024;21:676-89. [Link] [DOI:10.1007/s13178-024-00938-z]
30. Taherkhani S, Negarandeh R, Simbar M, Ahmadi F. Barriers to seeking help among abused Iranian women. J Adult Protect. 2017;19(5):261-73. [Link] [DOI:10.1108/JAP-03-2017-0007]
31. Aghakhani N, Lopez V, Parizad N, Baghaei R. "It was like nobody cared about what I said?" Iranian women committed self-immolation: A qualitative study. BMC Womens Health. 2021;21(1):75. [Link] [DOI:10.1186/s12905-021-01221-8]
32. Soltani F, Azizi R, Sourinegad H, Shayan A, Mohammadi Y, Khodakarami B. Sexual knowledge and attitude as predictors of female sexual satisfaction. Biomed Res Ther. 2017;4(12):1874-84. [Link] [DOI:10.15419/bmrat.v4i12.398]
33. Nejad SH, Bokaie M, Ardekani SM. Effectiveness of sexual health counseling based on mindfulness approach on sexual satisfaction in women suffering from infertility: An RCT. Int J Reprod Biomed. 2023;21(2):147-58. [Link] [DOI:10.18502/ijrm.v21i2.12805]
34. Mariani A, Seweng A, Ruseng SS, Moedjiono AI, Abdullah T, Anshary A, et al. The relationship between knowledge and personal hygiene and the occurrence of sexually transmitted diseases at the Community Health Center Talise, Palu. Gaceta Sanitaria. 2021;35(Suppl 2):S164-7. [Link] [DOI:10.1016/j.gaceta.2021.10.016]
35. Rossetto KR, Tollison AC. Feminist agency, sexual scripts, and sexual violence: Developing a model for postgendered family communication. Fam Relat. 2017;66(1):61-74. [Link] [DOI:10.1111/fare.12232]
36. Barrow RY, Ahmed F, Bolan GA, Workowski KA. Recommendations for providing quality sexually transmitted diseases clinical services, 2020. MMWR Recomm Rep. 2020;68(RR-5):1-20. [Link] [DOI:10.15585/mmwr.rr6805a1]
37. Cheraghi P, Poorolajal J, Moeini B, Cheraghi Z. Predictors of unintended pregnancy among married women in Hamadan, Western Iran: A case-control study. Iran J Public Health. 2013;42(8):854-9. [Link]
38. Asadisarvestani K, Leng Khoo S, Malek NM, Yasin SM, Ahmadi A. Determinants of contraceptive usage among married women in Shiraz, Iran. J Midwifery Reprod Health. 2017;5(4):1041-52. [Link] [DOI:10.17795/whb-38928]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |