



Volume 12, Issue 2 (2024)
Health Educ Health Promot 2024, 12(2): 309-314 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bahrampour B, Lamyian M, Shahali S. Relationship between Sexual Health Literacy and Sexual Function in Married Women of Reproductive Age. Health Educ Health Promot 2024; 12 (2) :309-314
URL: http://hehp.modares.ac.ir/article-5-73560-en.html
URL: http://hehp.modares.ac.ir/article-5-73560-en.html
Relationship between Sexual Health Literacy and Sexual Function in Married Women of Reproductive Age
1- Department of Reproductive Health and Midwifery, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
Keywords: Sexual Health [MeSH], Married Person [MeSH], Reproductive History [MeSH], Health Literacy [MeSH]
Full-Text [PDF 618 kb]
(2917 Downloads)
| Abstract (HTML) (1231 Views)
Full-Text: (199 Views)
Introduction
Sexual activity is one of the most important aspects of human life and can be influenced by individual characteristics, interpersonal relationships, family and socio-cultural conditions, the environment, the context of sexual activity for both the individual and their partner, as well as physical and mental health [1].
Sexual function is a complex process that encompasses both physical and psychological dimensions, which are related to sexual satisfaction, quality of life, and psychological well-being [2]. Human sexual function involves a combination of different components and requires coordination among the nervous, vascular, and endocrine systems; related disabilities are classified as disorders [3]. The sexual response cycle consists of four stages: sexual desire, arousal, orgasm, and resolution [4]. Among these stages, sexual desire disorder is one of the most common sexual disorders and is strongly associated with negative consequences for quality of life [5].
Sexual dysfunction in women is one of the most common problems worldwide [6]. It is caused by various factors, including biological factors such as chronic diseases, psychological factors such as depression and anxiety, and social factors such as socio-cultural anomalies [7, 8]. Additionally, sexual disorders are closely related to social issues, such as crime, mental illnesses, and divorce. Consequences of failing to satisfy sexual instincts include low quality of life, anxiety, low self-esteem, selfishness, nervousness, inability to concentrate, and even difficulty in performing routine tasks [9]. Studies on sexual dysfunction globally have shown a high prevalence of this disorder, affecting 30% to 50% of women [9]. The prevalence of sexual dysfunction in women ranges from 34% to 90%. This variation is attributed to differing definitions, study protocols, cultural differences, and environmental factors [10]. Research on sexual health in Iran has indicated that the level of sexual dysfunction among Iranian men and women is relatively high, with participating women reporting unfavorable sexual function [11]. In Iran, the prevalence of sexual disorders in women across different age groups has been reported to range from 31% to 72%, with the most common types being orgasm disorders, sexual arousal issues, and decreased sexual desire [12].
Changes in sexual function for various reasons can lead to disturbances in emotional and interpersonal communication, which subsequently affects other functions in women [1]. Numerous studies highlight the special importance of healthy and satisfactory sexual function and its relationship with the quality of sexual life [12]. Evidence has shown that diagnosis, treatment, and education for couples can prevent many problems and improve their quality of life together [13]. Women who report low desire or arousal, difficulty with orgasm, or inadequate sexual stimulation may benefit from normalization, sexual health education, and referral to a sex therapist [14]. Although sexual desires are innate and involuntary, sexual attitudes and behaviors can be learned. There is substantial evidence supporting the importance of sexual health education and addressing women’s sexual dysfunction, which is a significant public health issue [15]. Most women do not discuss their sexual health concerns with healthcare providers but hope that these providers will offer them sexual health education [16].
Sexual health literacy programs provide comprehensive, lifelong information about sex, knowledge, risks, and vulnerabilities related to unhealthy sexual activity, all of which promote sexual health [17]. Having sexual health literacy enhances the ability to understand and assess risks associated with sexual health, delays the onset of the first sexual experience, encourages safe sexual practices, creates appropriate opportunities for fulfilling gender roles, improves the sexual interactions of couples, and ultimately enhances individual sexual health. This, in turn, contributes to the overall health of families and society [18].
Sexual health literacy encompasses a set of skills, abilities, and capacities across different dimensions of sexual health, which can influence sexual function in areas such as access to sexual health information, reading, understanding, evaluation, and analysis [19]. Given that the prevalence of sexual disorders in women is higher than in men [20], and that rural women are among the groups lacking access to sexual health programs, this study assessed the relationship between the level of sexual health literacy and sexual function in married women of reproductive age in rural areas.
Instrument and Methods
Study design
This cross-sectional study was conducted on 200 women in 2021. The statistical population included all married women of reproductive age referring to the health center in the Banaroye sector. Banaroye district is located in Fars province, and the number of women of reproductive age under the comprehensive health service center in this district was 4500 women [21].
Inclusion criteria
Inclusion criteria included being aged 15-45 years, having a marriage history of at least one year, being literate in reading and writing, possessing Iranian citizenship, having a husband who is monogamous and has lived with his wife for the past two months, not being pregnant at the time of the research, not breastfeeding during the research period, having no stressful events in the past month, having no chronic illnesses or mental health disorders, having no addiction to drugs or alcohol, not using medications that affect sexual function, and having no uterine prolapse, cystocele, or rectocele of grade 3 or 4, as well as no urinary tract infection. Participants with education in medical or paramedical fields and those employed in health and treatment centers were excluded from the research.
Sampling
In this study, convenience sampling was employed. The sample size was calculated using PASS software and Cohen’s method [22]. The first and second type errors were set at α=0.05 and β=0.20, and the test power was established at 0.80. The sample size was determined to be at least 157 women, and considering a 20% attrition rate, the final sample size was calculated to be 200 women.
Data collection tools
Three questionnaires were used in this research. A researcher-made questionnaire collected demographic and fertility information (age, occupation, number of pregnancies, education, etc.). The second scale was the Adult Sexual Health Literacy Level Questionnaire (SHELA), which consists of 40 items scoring on a five-point Likert scale ranging from completely agree (5) to completely disagree (1). The scoring range is from 0 to 100 with four insufficient levels, including not very sufficient (0-50), adequate (55.1-66), good (66.1-84), and excellent (84.1-100). The Cronbach’s alpha for all dimensions of this tool is above 0.6, indicating favorable face validity, content validity, and structural validity of the questionnaire. Additionally, the overall Cronbach’s alpha was 0.95, indicating a favorable level of overall internal consistency for the tool [19]. Also, the Female Sexual Function Index (FSFI), which includes 19 questions measured women’s sexual function in six areas of desire, arousal, lubrication, orgasm, sexual satisfaction, and sexual pain. It is scored on a Likert scale and the score of each individual in each section is calculated by summing the scores of the questions related to that area and multiplying the sum by the coefficient for each section. The maximum score for each dimension is six, and the maximum score for the entire scale is 36. A total score of less than 26 is considered indicative of sexual dysfunction. The validity and reliability of this questionnaire in Iran were established by Mohammadi et al., with a Cronbach’s alpha internal consistency coefficient of 0.70. Additionally, the validity of the Persian version demonstrated a significant difference between the average scores of the entire scale and the areas in each case and control group [23].
After assuring the participants of the confidentiality of their information and obtaining written consent from each participant, they were asked to complete the questionnaire. The questionnaires were completed in person and under the supervision of the researcher.
Statistical analysis
After data collection, the data were analyzed using SPSS 21 software. The collected data were analyzed using descriptive statistical methods (frequency, mean, and standard deviation) and analysis of covariance, with a p-value of 0.05 considered significant.
Findings
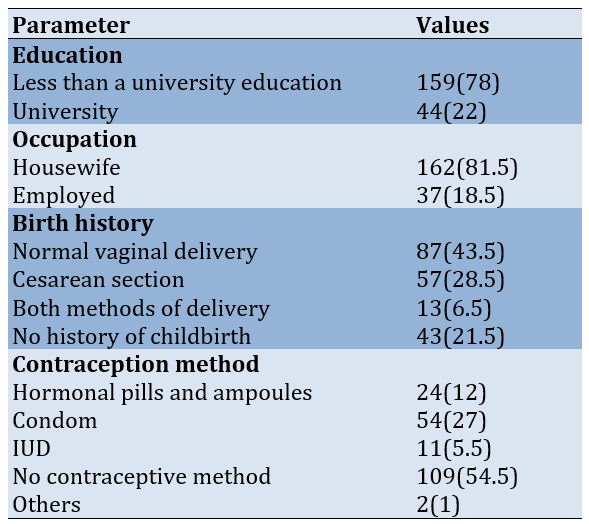
A total of 200 women with an average age of 36.65±5.95 years were included in the study. The average duration of marriage among the women was 12.18±6.65 years, and the average number of children was 1.6±1.1. Eighty percent of the women were housewives, and more than 70% of them did not have a university education (Table 1).
Table 1. Frequency of demographic and fertility characteristics of the participants (n=200)
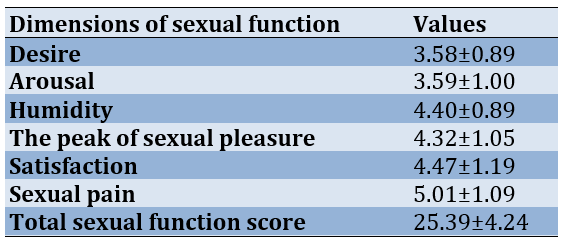
The level of sexual health literacy was favorable in 82.5% of the women. The average sexual function score of the participants was 25.39±4.24 (Table 2).
Table 2. Descriptive indicators of sexual function and its dimensions based on the Female Sexual Function Index (FSFI) (n=200)
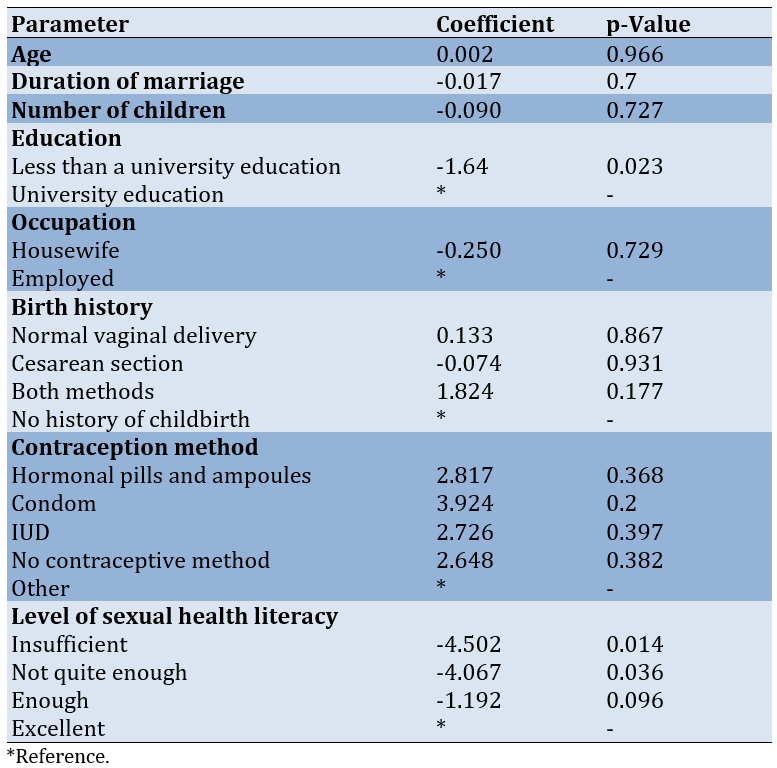
Seventy percent of the participants experienced some degree of sexual dysfunction. The average sexual function score of women with an insufficient level of sexual health literacy was 4.50 points lower than those who had an excellent level of sexual health literacy (p-value=0.014). The average sexual function score of women without a university education was 1.67 points lower than that of those with a university education (p-value=0.023; Table 3).
Table 3. The results of the analysis of covariance between sexual function and the sexual health literacy level and demographic and fertility characteristics of the participants (n=200)
Discussion
This study assessed the relationship between the level of sexual health literacy and sexual function in married women of reproductive age in rural areas. The FSFI was used to measure the sexual function of women. In this questionnaire, women’s sexual function is assessed in six areas, namely desire, arousal, lubrication, orgasm, sexual satisfaction, and sexual pain. The results showed that most participants (70.5%) had sexual dysfunction. Many studies have indicated that the frequency of sexual dysfunction varies significantly across different regions. Numerous studies have reported high rates of sexual dysfunction among women of reproductive age. Ahmadi et al. assessed women of reproductive age in Bushehr city with 48.8% of them experiencing sexual dysfunction [9]. Afshary et al. reported that 56.8% of women in Ahvaz have sexual dysfunction [24]. The high rate of sexual dysfunction in women may be influenced by the complexities of their sexual cycles, multiple births, breastfeeding, the use of hormonal contraceptives, and fatigue resulting from the multiple roles and responsibilities women have in married life and society. Additionally, in rural areas, cultural conditions, fear of stigma, and limited access to counseling centers and specialists in this field lead both women and men to be less likely to seek treatment for their sexual problems, contributing to a very high rate of sexual dysfunction in these areas.
Additionally, this study showed that the lowest average score was related to the dimensions of desire and arousal. The findings of Ahmadi et al. also indicate the highest frequency of disorders in the areas of desire and arousal [9]. However, in many studies, disturbances in the stages of the sexual cycle have been reported differently; for example, sexual pain disorder in Sari, Iran [25], and sexual desire in Kohgiloye and Boyer Ahmad, and Sabzevar [26, 27]. Furthermore, in other countries, such as Australia, disorders in the orgasm phase [28] and in Malaysia, pain disorders during intercourse [29] are the most common issues. These results demonstrate the impact of specific sociocultural conditions, demographic differences, and varying cultural understandings of sexual issues. Additionally, the high number of individuals with sexual dysfunction in rural areas may be attributed to their limited access to health facilities and information, including sexual health resources.
The results of the present study indicated a statistically significant relationship between the level of sexual health literacy and the sexual function score. The average sexual function score of women with an insufficient level of sexual health literacy was lower than that of women with an excellent level of sexual health literacy. The average sexual function score of women with a not quite sufficient level of sexual health literacy was lower than that of women with a high level of sexual health literacy.
There was no statistically significant difference between the average sexual function scores of women with adequate and excellent levels of sexual health literacy. Women with a higher level of sexual health literacy have more information about sex and its relationship with physical and mental health. Additionally, these women may be better equipped to search for, understand, and apply the best methods of sexual health care. Women with a higher level of sexual health literacy may also utilize sexual health services and related counseling more than other women.
Another influential factor in sexual function is the level of education of individuals. The average score of participants without a university education was lower than that of those with a university education. Ahmadi et al. indicated that sexual dysfunction is more common among individuals with a lower level of education [9]. Education may help individuals better understand themselves and their bodies, leading to increased awareness that encourages them to seek care and address their sexual problems. Additionally, individuals with higher education are generally more capable of searching for information and following up on the advice of experts. Considering the effect of education on the level of sexual health literacy, education may also indirectly influence individuals’ sexual function [30].
No statistically significant relationship was found between the method of delivery and the sexual function of women. Consistent with these results, the study by Gutzeit et al. demonstrated that the method of delivery has no effect on short-term and long-term sexual function after delivery. Furthermore, while episiotomy does not negatively impact sexual function, 3rd- and 4th-degree perineal tears were strongly associated with postpartum sexual dysfunction [6].
In the present study, there was no statistically significant relationship between age and sexual function. This lack of correlation may be attributed to the fact that most of the participants were young women of reproductive age, resulting in minimal differences in the levels of sex hormones. Additionally, the impact of other variables, such as psychological, social, and cultural conditions, on their sexual function is likely more significant.
The results of this research indicated that a considerable degree of sexual dysfunction was present among most rural women, with many experiencing disorders in the areas of desire and arousal. One of the factors influencing the sexual function score is the level of sexual health literacy and education of individuals. Those with good and excellent sexual health literacy tend to have better sexual function, and individuals with a university education also demonstrate improved sexual function. According to the findings of this study, one effective way to enhance women’s sexual function is to improve their sexual health literacy. Therefore, it is recommended to conduct studies on the effect of education on enhancing women’s sexual health literacy. One of the limitations of this research is that the study was conducted only on women living in the village.
Conclusion
Increasing awareness and education in the field of sexual health enhances individual sexual function, thereby improving couples’ relationships and increasing quality of life.
Acknowledgments: We are very grateful to the research vice-chancellor of Tarbiat Modares University for approving and funding this research, as well as to all the colleagues working at the Banaroye Health Center and to all the married women of reproductive age who patiently cooperated during the study.
Ethical Permissions: The present study was conducted after obtaining approval from the Ethics Committee of Tarbiat Modares University, Tehran (IR.MODARES.1398.199). After assuring the participants that their information would remain confidential and obtaining written consent from each participant, they were asked to complete the questionnaires.
Authors’ Contribution: Bahrampour B (First Author), Introduction Writer/Main Researcher/Discussion Writer/Statistical Analyst (45%); Lamyian M (Second Author), Methodologist/Assistant Researcher (40%); Shahali Sh (Third Author), Introduction Writer/Assistant Researcher/Discussion Writer (15%)
Funding/Support: The present study was funded by the Tarbiat Modares University.
Sexual activity is one of the most important aspects of human life and can be influenced by individual characteristics, interpersonal relationships, family and socio-cultural conditions, the environment, the context of sexual activity for both the individual and their partner, as well as physical and mental health [1].
Sexual function is a complex process that encompasses both physical and psychological dimensions, which are related to sexual satisfaction, quality of life, and psychological well-being [2]. Human sexual function involves a combination of different components and requires coordination among the nervous, vascular, and endocrine systems; related disabilities are classified as disorders [3]. The sexual response cycle consists of four stages: sexual desire, arousal, orgasm, and resolution [4]. Among these stages, sexual desire disorder is one of the most common sexual disorders and is strongly associated with negative consequences for quality of life [5].
Sexual dysfunction in women is one of the most common problems worldwide [6]. It is caused by various factors, including biological factors such as chronic diseases, psychological factors such as depression and anxiety, and social factors such as socio-cultural anomalies [7, 8]. Additionally, sexual disorders are closely related to social issues, such as crime, mental illnesses, and divorce. Consequences of failing to satisfy sexual instincts include low quality of life, anxiety, low self-esteem, selfishness, nervousness, inability to concentrate, and even difficulty in performing routine tasks [9]. Studies on sexual dysfunction globally have shown a high prevalence of this disorder, affecting 30% to 50% of women [9]. The prevalence of sexual dysfunction in women ranges from 34% to 90%. This variation is attributed to differing definitions, study protocols, cultural differences, and environmental factors [10]. Research on sexual health in Iran has indicated that the level of sexual dysfunction among Iranian men and women is relatively high, with participating women reporting unfavorable sexual function [11]. In Iran, the prevalence of sexual disorders in women across different age groups has been reported to range from 31% to 72%, with the most common types being orgasm disorders, sexual arousal issues, and decreased sexual desire [12].
Changes in sexual function for various reasons can lead to disturbances in emotional and interpersonal communication, which subsequently affects other functions in women [1]. Numerous studies highlight the special importance of healthy and satisfactory sexual function and its relationship with the quality of sexual life [12]. Evidence has shown that diagnosis, treatment, and education for couples can prevent many problems and improve their quality of life together [13]. Women who report low desire or arousal, difficulty with orgasm, or inadequate sexual stimulation may benefit from normalization, sexual health education, and referral to a sex therapist [14]. Although sexual desires are innate and involuntary, sexual attitudes and behaviors can be learned. There is substantial evidence supporting the importance of sexual health education and addressing women’s sexual dysfunction, which is a significant public health issue [15]. Most women do not discuss their sexual health concerns with healthcare providers but hope that these providers will offer them sexual health education [16].
Sexual health literacy programs provide comprehensive, lifelong information about sex, knowledge, risks, and vulnerabilities related to unhealthy sexual activity, all of which promote sexual health [17]. Having sexual health literacy enhances the ability to understand and assess risks associated with sexual health, delays the onset of the first sexual experience, encourages safe sexual practices, creates appropriate opportunities for fulfilling gender roles, improves the sexual interactions of couples, and ultimately enhances individual sexual health. This, in turn, contributes to the overall health of families and society [18].
Sexual health literacy encompasses a set of skills, abilities, and capacities across different dimensions of sexual health, which can influence sexual function in areas such as access to sexual health information, reading, understanding, evaluation, and analysis [19]. Given that the prevalence of sexual disorders in women is higher than in men [20], and that rural women are among the groups lacking access to sexual health programs, this study assessed the relationship between the level of sexual health literacy and sexual function in married women of reproductive age in rural areas.
Instrument and Methods
Study design
This cross-sectional study was conducted on 200 women in 2021. The statistical population included all married women of reproductive age referring to the health center in the Banaroye sector. Banaroye district is located in Fars province, and the number of women of reproductive age under the comprehensive health service center in this district was 4500 women [21].
Inclusion criteria
Inclusion criteria included being aged 15-45 years, having a marriage history of at least one year, being literate in reading and writing, possessing Iranian citizenship, having a husband who is monogamous and has lived with his wife for the past two months, not being pregnant at the time of the research, not breastfeeding during the research period, having no stressful events in the past month, having no chronic illnesses or mental health disorders, having no addiction to drugs or alcohol, not using medications that affect sexual function, and having no uterine prolapse, cystocele, or rectocele of grade 3 or 4, as well as no urinary tract infection. Participants with education in medical or paramedical fields and those employed in health and treatment centers were excluded from the research.
Sampling
In this study, convenience sampling was employed. The sample size was calculated using PASS software and Cohen’s method [22]. The first and second type errors were set at α=0.05 and β=0.20, and the test power was established at 0.80. The sample size was determined to be at least 157 women, and considering a 20% attrition rate, the final sample size was calculated to be 200 women.
Data collection tools
Three questionnaires were used in this research. A researcher-made questionnaire collected demographic and fertility information (age, occupation, number of pregnancies, education, etc.). The second scale was the Adult Sexual Health Literacy Level Questionnaire (SHELA), which consists of 40 items scoring on a five-point Likert scale ranging from completely agree (5) to completely disagree (1). The scoring range is from 0 to 100 with four insufficient levels, including not very sufficient (0-50), adequate (55.1-66), good (66.1-84), and excellent (84.1-100). The Cronbach’s alpha for all dimensions of this tool is above 0.6, indicating favorable face validity, content validity, and structural validity of the questionnaire. Additionally, the overall Cronbach’s alpha was 0.95, indicating a favorable level of overall internal consistency for the tool [19]. Also, the Female Sexual Function Index (FSFI), which includes 19 questions measured women’s sexual function in six areas of desire, arousal, lubrication, orgasm, sexual satisfaction, and sexual pain. It is scored on a Likert scale and the score of each individual in each section is calculated by summing the scores of the questions related to that area and multiplying the sum by the coefficient for each section. The maximum score for each dimension is six, and the maximum score for the entire scale is 36. A total score of less than 26 is considered indicative of sexual dysfunction. The validity and reliability of this questionnaire in Iran were established by Mohammadi et al., with a Cronbach’s alpha internal consistency coefficient of 0.70. Additionally, the validity of the Persian version demonstrated a significant difference between the average scores of the entire scale and the areas in each case and control group [23].
After assuring the participants of the confidentiality of their information and obtaining written consent from each participant, they were asked to complete the questionnaire. The questionnaires were completed in person and under the supervision of the researcher.
Statistical analysis
After data collection, the data were analyzed using SPSS 21 software. The collected data were analyzed using descriptive statistical methods (frequency, mean, and standard deviation) and analysis of covariance, with a p-value of 0.05 considered significant.
Findings
A total of 200 women with an average age of 36.65±5.95 years were included in the study. The average duration of marriage among the women was 12.18±6.65 years, and the average number of children was 1.6±1.1. Eighty percent of the women were housewives, and more than 70% of them did not have a university education (Table 1).
Table 1. Frequency of demographic and fertility characteristics of the participants (n=200)
The level of sexual health literacy was favorable in 82.5% of the women. The average sexual function score of the participants was 25.39±4.24 (Table 2).
Table 2. Descriptive indicators of sexual function and its dimensions based on the Female Sexual Function Index (FSFI) (n=200)
Seventy percent of the participants experienced some degree of sexual dysfunction. The average sexual function score of women with an insufficient level of sexual health literacy was 4.50 points lower than those who had an excellent level of sexual health literacy (p-value=0.014). The average sexual function score of women without a university education was 1.67 points lower than that of those with a university education (p-value=0.023; Table 3).
Table 3. The results of the analysis of covariance between sexual function and the sexual health literacy level and demographic and fertility characteristics of the participants (n=200)
Discussion
This study assessed the relationship between the level of sexual health literacy and sexual function in married women of reproductive age in rural areas. The FSFI was used to measure the sexual function of women. In this questionnaire, women’s sexual function is assessed in six areas, namely desire, arousal, lubrication, orgasm, sexual satisfaction, and sexual pain. The results showed that most participants (70.5%) had sexual dysfunction. Many studies have indicated that the frequency of sexual dysfunction varies significantly across different regions. Numerous studies have reported high rates of sexual dysfunction among women of reproductive age. Ahmadi et al. assessed women of reproductive age in Bushehr city with 48.8% of them experiencing sexual dysfunction [9]. Afshary et al. reported that 56.8% of women in Ahvaz have sexual dysfunction [24]. The high rate of sexual dysfunction in women may be influenced by the complexities of their sexual cycles, multiple births, breastfeeding, the use of hormonal contraceptives, and fatigue resulting from the multiple roles and responsibilities women have in married life and society. Additionally, in rural areas, cultural conditions, fear of stigma, and limited access to counseling centers and specialists in this field lead both women and men to be less likely to seek treatment for their sexual problems, contributing to a very high rate of sexual dysfunction in these areas.
Additionally, this study showed that the lowest average score was related to the dimensions of desire and arousal. The findings of Ahmadi et al. also indicate the highest frequency of disorders in the areas of desire and arousal [9]. However, in many studies, disturbances in the stages of the sexual cycle have been reported differently; for example, sexual pain disorder in Sari, Iran [25], and sexual desire in Kohgiloye and Boyer Ahmad, and Sabzevar [26, 27]. Furthermore, in other countries, such as Australia, disorders in the orgasm phase [28] and in Malaysia, pain disorders during intercourse [29] are the most common issues. These results demonstrate the impact of specific sociocultural conditions, demographic differences, and varying cultural understandings of sexual issues. Additionally, the high number of individuals with sexual dysfunction in rural areas may be attributed to their limited access to health facilities and information, including sexual health resources.
The results of the present study indicated a statistically significant relationship between the level of sexual health literacy and the sexual function score. The average sexual function score of women with an insufficient level of sexual health literacy was lower than that of women with an excellent level of sexual health literacy. The average sexual function score of women with a not quite sufficient level of sexual health literacy was lower than that of women with a high level of sexual health literacy.
There was no statistically significant difference between the average sexual function scores of women with adequate and excellent levels of sexual health literacy. Women with a higher level of sexual health literacy have more information about sex and its relationship with physical and mental health. Additionally, these women may be better equipped to search for, understand, and apply the best methods of sexual health care. Women with a higher level of sexual health literacy may also utilize sexual health services and related counseling more than other women.
Another influential factor in sexual function is the level of education of individuals. The average score of participants without a university education was lower than that of those with a university education. Ahmadi et al. indicated that sexual dysfunction is more common among individuals with a lower level of education [9]. Education may help individuals better understand themselves and their bodies, leading to increased awareness that encourages them to seek care and address their sexual problems. Additionally, individuals with higher education are generally more capable of searching for information and following up on the advice of experts. Considering the effect of education on the level of sexual health literacy, education may also indirectly influence individuals’ sexual function [30].
No statistically significant relationship was found between the method of delivery and the sexual function of women. Consistent with these results, the study by Gutzeit et al. demonstrated that the method of delivery has no effect on short-term and long-term sexual function after delivery. Furthermore, while episiotomy does not negatively impact sexual function, 3rd- and 4th-degree perineal tears were strongly associated with postpartum sexual dysfunction [6].
In the present study, there was no statistically significant relationship between age and sexual function. This lack of correlation may be attributed to the fact that most of the participants were young women of reproductive age, resulting in minimal differences in the levels of sex hormones. Additionally, the impact of other variables, such as psychological, social, and cultural conditions, on their sexual function is likely more significant.
The results of this research indicated that a considerable degree of sexual dysfunction was present among most rural women, with many experiencing disorders in the areas of desire and arousal. One of the factors influencing the sexual function score is the level of sexual health literacy and education of individuals. Those with good and excellent sexual health literacy tend to have better sexual function, and individuals with a university education also demonstrate improved sexual function. According to the findings of this study, one effective way to enhance women’s sexual function is to improve their sexual health literacy. Therefore, it is recommended to conduct studies on the effect of education on enhancing women’s sexual health literacy. One of the limitations of this research is that the study was conducted only on women living in the village.
Conclusion
Increasing awareness and education in the field of sexual health enhances individual sexual function, thereby improving couples’ relationships and increasing quality of life.
Acknowledgments: We are very grateful to the research vice-chancellor of Tarbiat Modares University for approving and funding this research, as well as to all the colleagues working at the Banaroye Health Center and to all the married women of reproductive age who patiently cooperated during the study.
Ethical Permissions: The present study was conducted after obtaining approval from the Ethics Committee of Tarbiat Modares University, Tehran (IR.MODARES.1398.199). After assuring the participants that their information would remain confidential and obtaining written consent from each participant, they were asked to complete the questionnaires.
Authors’ Contribution: Bahrampour B (First Author), Introduction Writer/Main Researcher/Discussion Writer/Statistical Analyst (45%); Lamyian M (Second Author), Methodologist/Assistant Researcher (40%); Shahali Sh (Third Author), Introduction Writer/Assistant Researcher/Discussion Writer (15%)
Funding/Support: The present study was funded by the Tarbiat Modares University.
Article Type: Original Research |
Subject:
Sexual Health Education/Promotion
Received: 2024/01/23 | Accepted: 2024/06/16 | Published: 2024/07/12
Received: 2024/01/23 | Accepted: 2024/06/16 | Published: 2024/07/12
References
1. Nezal AJ, Samii Rad F, Kalhor M, Hasanpour K, Alipour M, Montazeri A. Sexual quality of life in pregnant women: A cross-sectional study. PAYESH. 2018;17(4):421-9. [Persian] [Link]
2. Tavares IM, Laan ETM, Nobre PJ. Cognitive-affective dimensions of female orgasm: The role of automatic thoughts and affect during sexual activity. J Sex Med. 2017;14(6):818-28. [Link] [DOI:10.1016/j.jsxm.2017.04.004]
3. Daud S, Zahid AZM, Mohamad M, Abdullah B, Mohamad NAN. Prevalence of sexual dysfunction in pregnancy. Arch Gynecol Obstet. 2019;300(5):1279-85. [Link] [DOI:10.1007/s00404-019-05273-y]
4. Sommet N, Berent J. Porn use and men's and women's sexual performance: Evidence from a large longitudinal sample. Psychol Med. 2023;53(7):3105-14. [Link] [DOI:10.1017/S003329172100516X]
5. Leiblum SR, Koochaki PE, Rodenberg CA, Barton IP, Rosen RC. Hypoactive sexual desire disorder in postmenopausal women: US results from the Women's International Study of Health and Sexuality (WISHeS). Menopause. 2006;13(1):46-56. [Link] [DOI:10.1097/01.gme.0000172596.76272.06]
6. Gutzeit O, Levy G, Lowenstein L. Postpartum female sexual function: Risk factors for postpartum sexual dysfunction. Sex Med. 2020;8(1):8-13. [Link] [DOI:10.1016/j.esxm.2019.10.005]
7. Karimi-Valoujaei S, Hasani-Moghaddam S, Kashi Z, Yousefi SS, Sharifinia H, Khani S. Effective factors on sexual dysfunction in women with diabetes: A systematic review. Clin Excell. 2020;10(1):71-85. [Persian] [Link]
8. Hajnasiri H, Aslanbeygi N, Moafi F, Mafi M, Bajalan Z. Investigating the relationship between sexual function and mental health in pregnant females. Iran J Psychiatr Nurs. 2018;6(2):33-40. [Persian] [Link]
9. Ahmadi F, Tahmasebi R, Noroozi A, Akbarizade F. Prevalence of and factors affecting sexual dysfunction in women of reproductive age. Iran South Med J. 2022;25(2):114-29. [Persian] [Link] [DOI:10.52547/ismj.25.2.114]
10. Mendes N, Palma F, Serrano F. Sexual and reproductive health of Portuguese adolescents. Int J Adolesc Med Health. 2014;26(1):3-12. [Link] [DOI:10.1515/ijamh-2012-0109]
11. Masoumi SZ, Alavipour N, Parsa P, Kazemi F. Demographic factors affecting sexual dysfunction in postmenopausal women. J Educ Community Health. 2020;7(1):5-12. [Persian] [Link]
12. Ahmadnia E, Haseli A, Karamat A. Therapeutic interventions conducted on improving women's sexual satisfaction and function during reproductive ages in Iran: A systematic review. J Mazandaran Univ Med Sci. 2017;27(153):146-62. [Persian] [Link]
13. Aslan E, Beji NK, Gungor I, Kadioglu A, Dikencik BK. Prevalence and risk factors for low sexual function in women: A study of 1,009 women in an outpatient clinic of a university hospital in Istanbul. J Sex Med. 2008;5(9):2044-52. [Link] [DOI:10.1111/j.1743-6109.2008.00873.x]
14. Faubion SS, Rullo JE. Sexual dysfunction in women: A practical approach. Am Fam Physician. 2015;92(4):281-8. [Link]
15. Brotto L, Atallah S, Johnson-Agbakwu C, Rosenbaum T, Abdo C, Byers ES, et al. Psychological and interpersonal dimensions of sexual function and dysfunction. J Sex Med. 2016;13(4):538-71. [Link] [DOI:10.1016/j.jsxm.2016.01.019]
16. Faubion SS, Parish SJ. Sexual dysfunction in women: Can we talk about it?. Cleve Clin J Med. 2017;84(5):367-76. [Link] [DOI:10.3949/ccjm.84a.16021]
17. Graf AS, Patrick JH. Foundations of life-long sexual health literacy. Health Educ. 2015;115(1):56-70. [Link] [DOI:10.1108/HE-12-2013-0073]
18. Maasoumi R, Tavousi M, Zarei Z. Development and psychometric properties of sexual health literacy for adults (SHELA) questionnaire. J HAYAT. 2019;25(1):56-69. [Persian] [Link]
19. Patras G, Safdari F, Jafari H, Rafiei S, Fathnezhad Kazemi A. Correlation of health literacy and sexual satisfaction in infertile women referred to infertility center of Al-Zahra Hospital in Tabriz. J Health Promot Manag. 2020;9(4):58-67. [Persian] [Link]
20. Maasoumi R, Elsous A, Hussein H, Taghizadeh Z, Baloushah S. Female sexual dysfunction among married women in the Gaza Strip: An internet-based survey. Ann Saudi Med. 2019;39(5):319-27. [Link] [DOI:10.5144/0256-4947.2019.319]
21. Statistical Centre of Iran. General population and housing census, census results, detailed census results 2015-city-population Table 1 [Internet]. Tehran: Statistical Centre of Iran [cited 2023 Jan 5]. Available from: https://old.sci.org.ir/english/Population-and-Housing-Censuses. [Persian] [Link]
22. Cohen J. Statistical power analysis for the behavioral sciences. New Jersey: Lawrence Erlbaum Associates Publishers; 1988. [Link]
23. Mohammadi kh, Heydari M, Faghihzadeh S. The female sexual function index (FSFI): Validation of the Iranian version. PAYESH. 2008;7(3). [Persian] [Link]
24. Afshary P, Nik Bina M, Najjar S. Determination of factors related to sexual function in women; A case study. Health Res J. 2018;3(4):197-203. [Persian] [Link] [DOI:10.29252/hrjbaq.3.4.197]
25. Hoseini Tabaghdehi M, Haji Kazemi E, Hoseini F. The relative frequency of sexual dysfunction and some related factors in the women referred to the health centers of Sari city. J Mazandaran Univ Med Sci. 2012;22(91):102-7. [Persian] [Link]
26. Bakhtiari A, Basirat B, Nasiri-Amiri F. Sexual dysfunction in women undergoing fertility treatment in Iran: Prevalence and associated risk factors. J Reprod Infertil. 2016;17(1):26-33. [Link]
27. Barabadi A, Agah Zh, Akrami R. Prevalence of sexual dysfunction and ralated psychological factors in women of Sabzevar. J Sabzevar Univ Med Sci. 2018;25(1):101-9. [Persian] [Link]
28. Ponholzer A, Roehlich M, Racz U, Temml C, Madersbacher C. Female sexual dysfunction in a healthy Austrian cohort: Prevalence and risk factors. Eur Urol. 2005;47(3):366-75. [Link] [DOI:10.1016/j.eururo.2004.10.005]
29. Sidi H, Puteh S, Abdullah N, Midin M. The prevalence of sexual dysfunction and potential risk factors that may impair sexual function in Malaysian women. J Sex Med. 2007;4(2):311-21. [Link] [DOI:10.1111/j.1743-6109.2006.00319.x]
30. Bahrampour B, Lamyian M, Shahali S. The relationship between sexual health literacy and sexual assertiveness in married women: A quantitative study in southern Iran. PAYESH. 2022;21(1):59-67. [Persian] [Link] [DOI:10.52547/payesh.21.1.59]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |