



Volume 12, Issue 2 (2024)
Health Educ Health Promot 2024, 12(2): 357-364 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tahmasebi Ghorabi S, Karimi Rouzbahani A, Abedzadeh Zavareh M, Sadeghifar J, Jalilian M. Effect of a Mapping Model Education on Health-Promoting Behaviors in Medical University Staff. Health Educ Health Promot 2024; 12 (2) :357-364
URL: http://hehp.modares.ac.ir/article-5-72970-en.html
URL: http://hehp.modares.ac.ir/article-5-72970-en.html
S. Tahmasebi Ghorabi1, A. Karimi Rouzbahani2, M.S. Abedzadeh Zavareh3, J. Sadeghifar4, M. Jalilian *3
1- Clinical Research Development Unit, Emam Khomeini Hospital, Ilam University of Medical Sciences, Ilam, Iran
2- Student Research Committee, Lorestan University of Medical Sciences, Khorramabad, Iran
3- Department of Public Health and Health Education, School of Health, Ilam University of Medical Sciences, Ilam, Iran
4- “School of Health” and “Health and Environment Research Center”, Ilam University of Medical Sciences, Ilam, Iran
2- Student Research Committee, Lorestan University of Medical Sciences, Khorramabad, Iran
3- Department of Public Health and Health Education, School of Health, Ilam University of Medical Sciences, Ilam, Iran
4- “School of Health” and “Health and Environment Research Center”, Ilam University of Medical Sciences, Ilam, Iran
Full-Text [PDF 615 kb]
(2334 Downloads)
| Abstract (HTML) (1024 Views)
Full-Text: (144 Views)
Introduction
A person's lifestyle is their regular, everyday activity, which impacts their health [1, 2]. The total of these lifestyle measures, which include eating healthy food, getting enough sleep, exercising, managing body weight, and quitting smoking, is what humans do to maintain and improve their health and prevent diseases [1-3]. One of the primary criteria for determining health is engaging in behaviors that promote health. These behaviors are directly linked to health and contribute to a high quality of life. They are also considered a background factor in avoiding many diseases [4]. One of the most excellent ways for people to preserve their health is to engage in health-promoting behaviors [5]. It is also one of the most crucial issues because of its effects on quality of life and illness prevention [6]. Numerous research studies have examined the prevalence of activities promoting health in various communities. In Saqez City, Mahmoodi et al. conducted a study to compare the health-promoting behaviors of nurses, health professionals, and administrative staff. Diet and spiritual development dimensions received the highest ratings for health-promoting behaviors, while physical activity received the lowest ratings [7]. Harooni et al. and McElligott et al. studies had the lowest score in the physical activity dimension [8, 9]. Healthy food, physical activity, taking responsibility for one's health, stress management, interpersonal relationships, and spiritual growth are some of the most crucial components of a lifestyle that promotes health [10]. Designing targeted health promotion programs can significantly reduce and eliminate health problems, improve health, and improve people's lifestyles [11].
Researchers use role models to alter behavior. The intervention mapping technique is one of the models and strategies that the scientists in this field have developed for the execution and assessment of education and health promotion initiatives. The primary and readily available tools for health educators are the scientific literature and relevant ideas, and this method can effectively address their demands. However, how and where to employ these resources in program planning is only sometimes apparent. Kok et. al. introduced the intervention mapping technique [12]. This method applies an ecological and problem-solving framework to evaluating and intervening in health and social participation issues. The goal of intervention mapping is to give planners of education and health promotion programs a framework for efficient decision-making at every level of intervention design, implementation, and assessment [13-14]. The intervention mapping approach focuses on changing the behavior of the person at risk and the people influencing their behavior under environmental factors to address the health problem at various ecological levels (individual, interpersonal, organizational, social, community, and global). While altering an individual's behavior, consideration should also be given to altering the behavior of the powerful environmental elements, as this will ultimately improve the quality of life of health and health-related issues [15].
According to the descriptive study that identified the physical activity dimension as the most critical predictor of health-promoting behaviors, this study aims to investigate the effect of training based on the intervention mapping model on promoting physical activity among employees of Ilam University of Medical Sciences.
Materials and Methods
This semi-experimental study was conducted in all Ilam University of Medical Sciences employees. The study was conducted in two phases; descriptive and interventional. The sample size for the descriptive phase was calculated using Cochran's formula, which was 221 individuals. For the interventional phase, 52 individuals, based on Bayat et al. [16], considering a 15% sample drop, 60 individuals were selected. Employees of the administrative field with at least one year of work experience, having an unfavorable situation in the priority dimension identified from Walker's health-promoting lifestyle questionnaire, and lack physical limitations were selected for the study. Failure to participate in two training sessions, permanent departure of the person from the field under the researcher's investigation, and unwillingness to continue cooperation caused exclusion.
The data collection tools were participants' demographic information (age, gender, marital status, education level, employment status, work experience, and income), Walker's Health Promotion Lifestyle Questionnaire [17], and the long form of International Physical Activity Questionnaire, whose validity and reliability have been examined and confirmed in several studies [18-20].
The health promotion lifestyle questionnaire contains 52 questions and is scored on a 4-point Likert scale (never 1, sometimes 2, usually 3, always 4). The questions are classified into six areas; responsibility for health, physical activity, spiritual growth, healthy nutrition, interpersonal relations, and stress management. The range of the total score of the health-promoting behaviors questionnaire is between 52-208, where a higher score means a better health status. The validity and reliability of the Persian version have been evaluated, and Mohammadi Zeidi et al. confirmed content validity in Iran [21]. To determine the reliability, the internal consistency method of the items by calculating Cronbach's alpha was used. For this purpose, the questionnaire was completed by 30 employees who were outside the study, and its reliability has been reported as 0.89 for responsibility for health, 0.84 for physical activity, 0.88 for spiritual growth, 0.76 for healthy nutrition, 0.83 for interpersonal relations, 0.75 for stress management, and 0.87 for the whole questionnaire.
The International Physical Activity Questionnaire includes 27 items in 4 fields; physical activity related to work (7 questions), physical activity for transportation (6 questions), housework, home maintenance, and family care (6 questions), and physical activities related to leisure, sports, and entertainment (8 questions) during the last seven days. This questionnaire reports activities in the form of moderate and intense activity. Metabolic equivalents were considered for the mentioned physical activities. The metabolic equivalent of a person's oxygen intake coefficients at rest is that all physical activities can be classified as multiples of energy consumption at rest. The metabolic equivalents were considered 3.3 for leisure walking, 8 for intense leisure activity, 4 for moderate leisure activity, 5.5 for intense household activities, 4 for moderate indoor activities and yard, 3.3 for walking to go from place to place, 8 for intense workplace activities, and 3.3 for moderate workplace activities and walking related to the workplace. These numbers are multiplied by the duration of physical activity in minutes and the number of days of that activity per week. In the end, the sum of the obtained values was calculated. According to the scoring protocol of the IPAQ questionnaire, the amount of physical activity of a person can be extracted and reported as follows: The total amount of physical activity of a person in the last week according to the number of calories consumed in the last week (MET-minutes/week). The term MET, or metabolic unit, estimates the metabolic cost of physical activity, and its value is approximately equal to a person's resting energy consumption. The whole amount must be calculated to calculate the total weekly quantity of physical activity. The amount of walking (MET×minute×day) should be added together with the amount of moderate physical activity (MET×minute×day) and the amount of intense physical activity of the person (MET×MET; Minute×day) in the last week. According to the IPAQ questionnaire, the amount of weekly calories people consume determines the intensity of their physical activity [22, 23].
The intervention mapping approach was implemented based on the steps described below:
1- Needs assessment: After creating the collaborative planning group, the needs assessment of the health problem was done in the first step. The research team conducted a descriptive study to assess the needs and determine the problematic dimension of lifestyle. Walker's health-promoting lifestyle questionnaire was provided to 221 participants for completion. According to the analysis of the questionnaire, the dimension of physical activity was identified as the problematic dimension of lifestyle for educational intervention.
2- Preparation of matrices of change objectives: Increasing physical activity was the aim of the study change, based on the descriptive study and the planning group's remarks. Dividing the outcomes into functional goals is the second task in the intervention mapping process second step. The current program's functional goals include dispelling myths about obstacles to physical activity, adopting a positive outlook on it, choosing to exercise regardless of the weather, considering the various effects of it, and having a strategy in place for performing the right sports movements to avoid injuries.
3- Selection of theory-based intervention methods and practical applications: After the goals of program change are determined, the third stage of intervention mapping begins: Selecting theory-based intervention methods and practical applications. The theoretical method is a general technique or process of influencing changes in determining factors. For example, a goal of change in an intervention can be to increase the self-efficacy of employees to perform physical activity in all conditions. Theoretical methods related to increasing self-efficacy include skill training. In this study, promoting physical activity was considered the goal of change. A combination of educational and practical methods was used to promote physical activity. Attitude: Encouragement to combine affective and cognitive evaluations of one's self-image with and without unhealthy behavior. For example, one can compare one's self-image as a healthy, cheerful, and active person with a possible self-image as a dull, tired person in society. Social support is defined as the amount of love, companionship, and attention given to family members, friends, and other people. For example, managers and colleagues should support employees' physical activity, and time should be allocated to this activity in the university environment.
4- Production of program components and materials: The educational program was designed according to the following goals and variables and provided to the participants.
a) Holding training classes about physical activity, the importance of physical activity in everyday life, types of physical activity with examples, complications caused by lack of physical activity, workplace ergonomics, and workplace sports, and also providing educational materials (photos, posters, educational clips related to physical activity) in the field of familiarizing with the complications caused by physical inactivity (sensitizing the target group)
b) Designing and making an educational clip for doing sports at work (to promote physical activity at work)
c) Designing an educational poster of sports at work and installing it at the workplace
d) Providing educational content through Telegram for the target group
e) Holding sports competitions to keep employees fresh and energetic
f) Implementing a morning exercise program in the work environment to promote physical activity
5- Planning for the program's approval, implementation, and sustainability: The fifth step of intervention mapping focuses on intervention planning to ensure that the program developed in the previous stages can be used and maintained for the required time. After the full description of the intervention mapping steps and the preparation of the implementation plan, considering that the study was designed to be a control group and intervention in the central campus and headquarters staff, after conducting a descriptive study and examining the status of health-promoting behaviors and identifying the dimension of physical activity as a problematic dimension for educational intervention, the staff of the central headquarters had higher scores than the staff of the central campus. Also, the number of samples did not reach the quorum. On the other hand, the physical activity of the staff of the central campus was different from the situation did not have a favorable outcome, the study was carried out as a before-and-after intervention in the employees of the central campus. Sixty people with the lowest score who were in an unfavorable condition regarding physical activity were included in the study. After selecting the samples, the participants completed the international physical activity questionnaire. After the needs assessment from the initial evaluation results, the required educational content was designed and implemented. The educational intervention program consisted of three theoretical training sessions and one practical session. The morning exercise program was organized for the employees for two weeks in coordination with the director of the physical education group. Sports competitions were held in Neshat Sports Hall for the refreshment and well-being of employees. Employees competed in darts, ping pong, and hand football. Designing and making an educational clip: First, some sports movements that can be done behind the desk to exercise behind the desk were designed with the approval of a physical education expert, and then filming and editing of the desired clip was done. The approval of the film was given to the employees in the Bargazari Telegram groups and persons. The poster of sports activities was designed in the workplace and installed in the employees' workplace. After the end of the intervention program, weekly follow-up was done in person. Subsequent reminders were done through the Telegram group every two weeks. To determine the effectiveness of the intervention, a questionnaire was provided to the employees three months after the implementation of the educational intervention, and 55 people managed to finish the study.
6- Evaluation planning: In the intervention mapping process, planners decide on change goals, methods, applications, and implementations. At this stage, the student was assured by the advice from the supervisors and advisors regarding the correct selection of the determining factors, methods, target group selection, the matrix of the program's objectives, and how to implement the program. Also, all the tools used to evaluate the program participants were determined at this stage.
Data analysis was done using SPSS 22 software by independent t-test, paired t-test, Pearson correlation coefficient, one-way analysis of variance, and generalized linear regression at a significance level of 0.05.
Findings
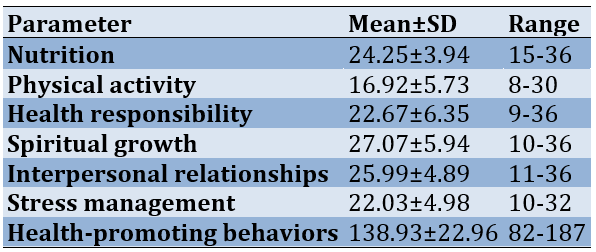
The mean score of the participants' health-promoting behaviors was 138.22±93.96 (141.29±23.18 for men and 136.53±22.59 for women). The highest score was spiritual growth (27.07±5.94), and the lowest was physical activity (16.92±5.73; Table 1).
Table 1. Possible range, observed range, mean, and standard deviation of health-promoting behaviors in each subgroup and total score
The mean score obtained in men was higher than in women, but the difference was not statistically significant (p=0.136). An independent t-test was used to investigate the relationship between gender, marital status, and the total score of health-promoting behaviors and their dimensions. The mean score of physical activity, spiritual growth, stress management, and total health-promoting score was higher in males, but the difference was significant only in the physical activity dimension (p=0.0001).
The highest correlation of overall health-promoting behaviors with spiritual growth (r=0.782) followed by stress management (r=0.777), interpersonal relationships (r=0.767), responsibility for health (r=0.73), nutrition (r=0.641), and physical activity (r=0.611; p<0.001). Among the subscales, the highest correlation between spiritual growth and stress management (r=0.676) and the lowest correlation between physical activity and interpersonal relationships (r=0.253) were observed (p=0.001).
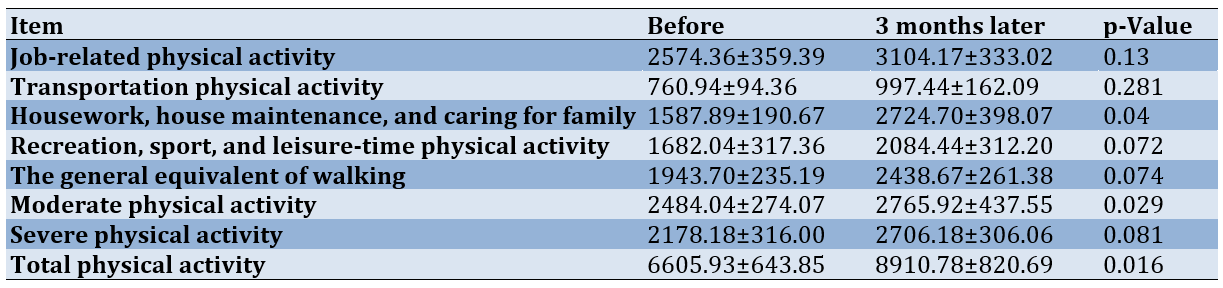
In an intervention study, 60 people were included in the intervention group at the beginning of training. In the three-month follow-up, 55 people completed the study. The mean and standard deviation of the participant's age was 40.42±6.89. On the other hand, the study's results showed that out of 55 people participating, 24 people (43.6%) were men, 31 (56.4%) were women, 76.4% were married, and the rest were single. The participants had between 1 and 30 years of work experience, and their average work experience was 15.76±9.17. 54.5% had a master's degree. 74.5% of employees reported an average income level. A paired t-test was used to compare the average physical activity and its items before and after the educational intervention. The results showed that the average for all the physical activity items increased after the educational intervention. The statistical test showed a significant difference before and after the educational intervention in the housework and family care item and the average physical activity item (p=0.04; p=0.029). The average total physical activity after the educational intervention in people (8910.78±820.69) increased compared to before the intervention (6605.93±643.85), and the statistical test showed a significant difference (p<0.016; Table 2).
Table 2. Comparison of average physical activity and items before and 3 months after the educational intervention
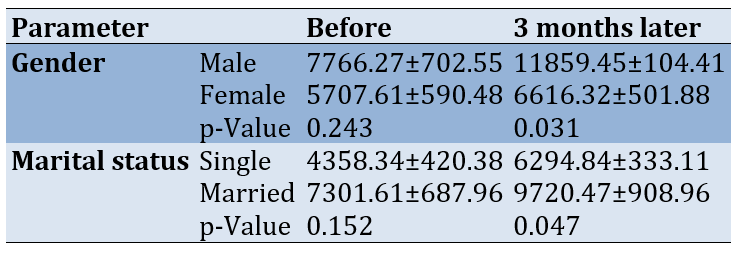
The average score for the total physical activity of the participants after the intervention was higher in men than in women. Also, the average score of total physical activity of married people after the intervention was higher than that of single people. Independent t-test was used to investigate the relationship between gender, marital status, and total physical activity score. Before the educational intervention, there was no significant relationship between gender, marital status, and average physical activity (p<0.05). Still, the independent t-test showed a significant relationship between gender, marital status, and average physical activity after the educational intervention (p<0.05; Table 3).
Table 3. Comparison of average physical activity in participants according to gender and marital status before and three months after the educational intervention
Discussion
A healthy lifestyle is essential in reducing the spread of diseases, promoting health, and improving quality of life. Considering the critical role of employees as valuable resources and service providers to the people and their essential role in their family and surrounding environment, this study was conducted to investigate the status of health-promoting behaviors of the employees of Ilam University of Medical Sciences. The study's findings indicate that the employees' practices that promote health are in good shape. The results of a study by Moradi & Shojaizade on the lifestyle of workers in Andimeshk health centers revealed that the amount of health-improving behavior described was average [24]. The average status of health-promoting habits has been the subject of several research, one of which was conducted by Chenary et al. [25]. Mostafay Najafabadi & Rezaei's [26] research on nurses supports this study's findings. Furthermore, most nurses had an average overall score for health-promoting activities in a Taiwanese study, which aligns with the findings of the current investigation [25-27].
Men than women reported living better lives in this survey. This outcome agrees with the findings of Moradi & Shojaizade [24]. Mahmoodi et al.'s study on promoting a healthy lifestyle revealed that women had better lives than men, a finding that is at odds with our own. The disparity in health-promoting behaviors across genders may stem from factors such as awareness, education, availability of suitable environments for physical exercise, and community culture that influences these behaviors [7]. The findings showed that the participants had appropriate conditions in the spiritual growth dimension compared to other dimensions of health-promoting behaviors. Participants physical activity level was low and was not enough to impact on health status and quality of life. A review of studies showed that results from similar studies are consistent with the results of the present study. In the studies of Chenary et al. [25], Motlagh et al. [28], and Ghorabi et al. [29], the highest score was in the dimension of spiritual growth; these results are consistent with the result of the present study. In the present study, the lowest score on behavior was in the dimension of physical activity. In line with this finding, the lowest score of behavior in the studies of Chenary et al. [25], Edrisi et al. [5], and Ghorabi et al. [29], were in the dimension of physical activity. Regarding the intervention study, the results show that the individuals' physical activity increased when the instructional program was implemented. Numerous research studies have shown that an educational intervention enhanced participants' performance regarding weekly physical activity totals [30-33]. Furthermore, Teymoori et al. demonstrated that the Pender model intervention program had the highest impact on activity levels [34]. In the study of Parhoodeh et al., the educational intervention program increased people's level of physical activity, which is generally consistent with the present study. This issue shows the importance and effect of holding educational and cultural meetings and recommending and persuading people [35].
Vafaee Najar et al.'s employee-based study demonstrated a statistically significant rise in the training group's average physical activity scores following the educational intervention. According to the results of this study, 75% of the test group members were engaging in moderate physical activity following the execution of the training program, and none of them were in the light or sedentary stage. Only 11.2% of participants in the control group had moderate physical activity after the intervention, compared to 88.2% of light and sedentary individuals [22]. In the investigation of the efficacy of the electronic training program that raised the BMI and physical activity levels of female employees, Amini et al. demonstrated that, before the training, there was no discernible difference in the levels of physical activity between the intervention group and the control group; However, following the training, the average the favorable impact of educational programs in the intervention group is demonstrated by the score in the intervention group, which grew up to three times and was considerably higher than the control group. As a result, web-based, brief message, multimedia training treatments have the potential to both prevent and exacerbate diseases associated with inactivity in female employees [19]. Exercise has a positive effect on lowering depression levels in women, according to research by Jalalinia et al. on the relationship between depression and obesity [36]. After investigating how the University of Medical Sciences female students' regular activities were affected by the second physical education curriculum based on the Bezenf model, Hazavehei et al. concluded that there was a significant difference in the average scores of the Bezenf model components between the intervention group and the control group following the educational intervention. After the training session ended, the intervention group significantly improved in engaging in regular physical activity in the following two and four months [37]. Men scored higher on the average for physical activity than women, and the statistical test revealed a significant correlation between gender and physical activity level. This finding is consistent with Sane et al.'s study, which found that working women engaged in less physical activity than men [38]. Male employees engaged in more significant physical activity than female employees, according to a study by Vafaee Najar et al. on workers in Aqqola City. This suggests a significant correlation between gender and physical activity level. Other contextual factors mentioned in this issue as intrapersonal and environmental barriers to women leading active lives in Iran include the unique characteristics of society and family norms, attention to cultural considerations regarding women's sports, and limited access to gyms and physical exercise spaces [22].
The average physical activity of married individuals was higher than that of single individuals in the current study, with a statistically significant difference. According to Vafaee Najar et al.'s study, married individuals had higher average physical activity levels than single individuals. However, the Mann-Whitney statistical test revealed no significant correlation between marital status and physical activity level, contradicting the current investigation's findings [22]. An increase in the average was noted before and after the educational intervention in the following fields on the standard physical activity questionnaire: Sports and leisure time physical activity, housework and family care, physical activity for transportation, and physical activity related to daily work. The statistical test revealed significant physical activity in the domain of housework, which includes walking during leisure time, intense and moderate physical activity, and moderate physical activity. This finding contradicts the findings of Mazloumi Mahmoodabad et al., which focused on homemakers. Mazloumi Mahmoodabad et al. found no significant differences when comparing the intervention and control groups in the areas of housework and family care. Consistent with the findings of Mazloumi Mahmoodabad et al. [18], there was no statistically significant variation in physical activity for transportation in the current study. In Mazloumi Mahmoodabad et al., significant differences were observed between the two groups (control and intervention) when comparing physical activity during leisure time and sports. These findings are incongruent with the current investigation. Intense and moderate physical exercise, as well as recreational walking, fall under this category. Mazloumi Mahmoodabad et al. focused exclusively on homemakers, who have more free time for physical activity than working women, which could be one of the possible causes of this problem [18].
The program's design was based on identifying the priority dimension of the lifestyle questionnaire. This allowed the educational program to be designed based on the real needs of the studied population, and as a result, it had a favorable effect on the employees' physical activity.
Conclusion
The training program's design, based on the intervention mapping model, improves the employees' physical activity.
Acknowledgements: This research was the thesis for the master's degree in health education, and we are grateful to all the study participants.
Ethical Permissions: The research ethics committee confirmed the study (code: IR. MEDILAM. REC.1398.098).
Conflicts of Interests: No conflict of interest is reported in this study.
Authors' Contribution: Tahmasebi Ghorabi S (First Author), Introduction Writer/Main Researcher (35%); Karimi Rouzbahani A (Second Author), Introduction Writer/Assistant Researcher (15%); Abedzadeh Zavareh MS (Third Author), Methodologist (15%); Sadeghifar J (Fourth Author), Methodologist (10%); Jalilian M (Fifth Author), Discussion Writer/Statistical Analyst (25%)
Funding/Support: This study was financially supported by the Deputy of Research of Ilam University of Medical Sciences.
A person's lifestyle is their regular, everyday activity, which impacts their health [1, 2]. The total of these lifestyle measures, which include eating healthy food, getting enough sleep, exercising, managing body weight, and quitting smoking, is what humans do to maintain and improve their health and prevent diseases [1-3]. One of the primary criteria for determining health is engaging in behaviors that promote health. These behaviors are directly linked to health and contribute to a high quality of life. They are also considered a background factor in avoiding many diseases [4]. One of the most excellent ways for people to preserve their health is to engage in health-promoting behaviors [5]. It is also one of the most crucial issues because of its effects on quality of life and illness prevention [6]. Numerous research studies have examined the prevalence of activities promoting health in various communities. In Saqez City, Mahmoodi et al. conducted a study to compare the health-promoting behaviors of nurses, health professionals, and administrative staff. Diet and spiritual development dimensions received the highest ratings for health-promoting behaviors, while physical activity received the lowest ratings [7]. Harooni et al. and McElligott et al. studies had the lowest score in the physical activity dimension [8, 9]. Healthy food, physical activity, taking responsibility for one's health, stress management, interpersonal relationships, and spiritual growth are some of the most crucial components of a lifestyle that promotes health [10]. Designing targeted health promotion programs can significantly reduce and eliminate health problems, improve health, and improve people's lifestyles [11].
Researchers use role models to alter behavior. The intervention mapping technique is one of the models and strategies that the scientists in this field have developed for the execution and assessment of education and health promotion initiatives. The primary and readily available tools for health educators are the scientific literature and relevant ideas, and this method can effectively address their demands. However, how and where to employ these resources in program planning is only sometimes apparent. Kok et. al. introduced the intervention mapping technique [12]. This method applies an ecological and problem-solving framework to evaluating and intervening in health and social participation issues. The goal of intervention mapping is to give planners of education and health promotion programs a framework for efficient decision-making at every level of intervention design, implementation, and assessment [13-14]. The intervention mapping approach focuses on changing the behavior of the person at risk and the people influencing their behavior under environmental factors to address the health problem at various ecological levels (individual, interpersonal, organizational, social, community, and global). While altering an individual's behavior, consideration should also be given to altering the behavior of the powerful environmental elements, as this will ultimately improve the quality of life of health and health-related issues [15].
According to the descriptive study that identified the physical activity dimension as the most critical predictor of health-promoting behaviors, this study aims to investigate the effect of training based on the intervention mapping model on promoting physical activity among employees of Ilam University of Medical Sciences.
Materials and Methods
This semi-experimental study was conducted in all Ilam University of Medical Sciences employees. The study was conducted in two phases; descriptive and interventional. The sample size for the descriptive phase was calculated using Cochran's formula, which was 221 individuals. For the interventional phase, 52 individuals, based on Bayat et al. [16], considering a 15% sample drop, 60 individuals were selected. Employees of the administrative field with at least one year of work experience, having an unfavorable situation in the priority dimension identified from Walker's health-promoting lifestyle questionnaire, and lack physical limitations were selected for the study. Failure to participate in two training sessions, permanent departure of the person from the field under the researcher's investigation, and unwillingness to continue cooperation caused exclusion.
The data collection tools were participants' demographic information (age, gender, marital status, education level, employment status, work experience, and income), Walker's Health Promotion Lifestyle Questionnaire [17], and the long form of International Physical Activity Questionnaire, whose validity and reliability have been examined and confirmed in several studies [18-20].
The health promotion lifestyle questionnaire contains 52 questions and is scored on a 4-point Likert scale (never 1, sometimes 2, usually 3, always 4). The questions are classified into six areas; responsibility for health, physical activity, spiritual growth, healthy nutrition, interpersonal relations, and stress management. The range of the total score of the health-promoting behaviors questionnaire is between 52-208, where a higher score means a better health status. The validity and reliability of the Persian version have been evaluated, and Mohammadi Zeidi et al. confirmed content validity in Iran [21]. To determine the reliability, the internal consistency method of the items by calculating Cronbach's alpha was used. For this purpose, the questionnaire was completed by 30 employees who were outside the study, and its reliability has been reported as 0.89 for responsibility for health, 0.84 for physical activity, 0.88 for spiritual growth, 0.76 for healthy nutrition, 0.83 for interpersonal relations, 0.75 for stress management, and 0.87 for the whole questionnaire.
The International Physical Activity Questionnaire includes 27 items in 4 fields; physical activity related to work (7 questions), physical activity for transportation (6 questions), housework, home maintenance, and family care (6 questions), and physical activities related to leisure, sports, and entertainment (8 questions) during the last seven days. This questionnaire reports activities in the form of moderate and intense activity. Metabolic equivalents were considered for the mentioned physical activities. The metabolic equivalent of a person's oxygen intake coefficients at rest is that all physical activities can be classified as multiples of energy consumption at rest. The metabolic equivalents were considered 3.3 for leisure walking, 8 for intense leisure activity, 4 for moderate leisure activity, 5.5 for intense household activities, 4 for moderate indoor activities and yard, 3.3 for walking to go from place to place, 8 for intense workplace activities, and 3.3 for moderate workplace activities and walking related to the workplace. These numbers are multiplied by the duration of physical activity in minutes and the number of days of that activity per week. In the end, the sum of the obtained values was calculated. According to the scoring protocol of the IPAQ questionnaire, the amount of physical activity of a person can be extracted and reported as follows: The total amount of physical activity of a person in the last week according to the number of calories consumed in the last week (MET-minutes/week). The term MET, or metabolic unit, estimates the metabolic cost of physical activity, and its value is approximately equal to a person's resting energy consumption. The whole amount must be calculated to calculate the total weekly quantity of physical activity. The amount of walking (MET×minute×day) should be added together with the amount of moderate physical activity (MET×minute×day) and the amount of intense physical activity of the person (MET×MET; Minute×day) in the last week. According to the IPAQ questionnaire, the amount of weekly calories people consume determines the intensity of their physical activity [22, 23].
The intervention mapping approach was implemented based on the steps described below:
1- Needs assessment: After creating the collaborative planning group, the needs assessment of the health problem was done in the first step. The research team conducted a descriptive study to assess the needs and determine the problematic dimension of lifestyle. Walker's health-promoting lifestyle questionnaire was provided to 221 participants for completion. According to the analysis of the questionnaire, the dimension of physical activity was identified as the problematic dimension of lifestyle for educational intervention.
2- Preparation of matrices of change objectives: Increasing physical activity was the aim of the study change, based on the descriptive study and the planning group's remarks. Dividing the outcomes into functional goals is the second task in the intervention mapping process second step. The current program's functional goals include dispelling myths about obstacles to physical activity, adopting a positive outlook on it, choosing to exercise regardless of the weather, considering the various effects of it, and having a strategy in place for performing the right sports movements to avoid injuries.
3- Selection of theory-based intervention methods and practical applications: After the goals of program change are determined, the third stage of intervention mapping begins: Selecting theory-based intervention methods and practical applications. The theoretical method is a general technique or process of influencing changes in determining factors. For example, a goal of change in an intervention can be to increase the self-efficacy of employees to perform physical activity in all conditions. Theoretical methods related to increasing self-efficacy include skill training. In this study, promoting physical activity was considered the goal of change. A combination of educational and practical methods was used to promote physical activity. Attitude: Encouragement to combine affective and cognitive evaluations of one's self-image with and without unhealthy behavior. For example, one can compare one's self-image as a healthy, cheerful, and active person with a possible self-image as a dull, tired person in society. Social support is defined as the amount of love, companionship, and attention given to family members, friends, and other people. For example, managers and colleagues should support employees' physical activity, and time should be allocated to this activity in the university environment.
4- Production of program components and materials: The educational program was designed according to the following goals and variables and provided to the participants.
a) Holding training classes about physical activity, the importance of physical activity in everyday life, types of physical activity with examples, complications caused by lack of physical activity, workplace ergonomics, and workplace sports, and also providing educational materials (photos, posters, educational clips related to physical activity) in the field of familiarizing with the complications caused by physical inactivity (sensitizing the target group)
b) Designing and making an educational clip for doing sports at work (to promote physical activity at work)
c) Designing an educational poster of sports at work and installing it at the workplace
d) Providing educational content through Telegram for the target group
e) Holding sports competitions to keep employees fresh and energetic
f) Implementing a morning exercise program in the work environment to promote physical activity
5- Planning for the program's approval, implementation, and sustainability: The fifth step of intervention mapping focuses on intervention planning to ensure that the program developed in the previous stages can be used and maintained for the required time. After the full description of the intervention mapping steps and the preparation of the implementation plan, considering that the study was designed to be a control group and intervention in the central campus and headquarters staff, after conducting a descriptive study and examining the status of health-promoting behaviors and identifying the dimension of physical activity as a problematic dimension for educational intervention, the staff of the central headquarters had higher scores than the staff of the central campus. Also, the number of samples did not reach the quorum. On the other hand, the physical activity of the staff of the central campus was different from the situation did not have a favorable outcome, the study was carried out as a before-and-after intervention in the employees of the central campus. Sixty people with the lowest score who were in an unfavorable condition regarding physical activity were included in the study. After selecting the samples, the participants completed the international physical activity questionnaire. After the needs assessment from the initial evaluation results, the required educational content was designed and implemented. The educational intervention program consisted of three theoretical training sessions and one practical session. The morning exercise program was organized for the employees for two weeks in coordination with the director of the physical education group. Sports competitions were held in Neshat Sports Hall for the refreshment and well-being of employees. Employees competed in darts, ping pong, and hand football. Designing and making an educational clip: First, some sports movements that can be done behind the desk to exercise behind the desk were designed with the approval of a physical education expert, and then filming and editing of the desired clip was done. The approval of the film was given to the employees in the Bargazari Telegram groups and persons. The poster of sports activities was designed in the workplace and installed in the employees' workplace. After the end of the intervention program, weekly follow-up was done in person. Subsequent reminders were done through the Telegram group every two weeks. To determine the effectiveness of the intervention, a questionnaire was provided to the employees three months after the implementation of the educational intervention, and 55 people managed to finish the study.
6- Evaluation planning: In the intervention mapping process, planners decide on change goals, methods, applications, and implementations. At this stage, the student was assured by the advice from the supervisors and advisors regarding the correct selection of the determining factors, methods, target group selection, the matrix of the program's objectives, and how to implement the program. Also, all the tools used to evaluate the program participants were determined at this stage.
Data analysis was done using SPSS 22 software by independent t-test, paired t-test, Pearson correlation coefficient, one-way analysis of variance, and generalized linear regression at a significance level of 0.05.
Findings
The mean score of the participants' health-promoting behaviors was 138.22±93.96 (141.29±23.18 for men and 136.53±22.59 for women). The highest score was spiritual growth (27.07±5.94), and the lowest was physical activity (16.92±5.73; Table 1).
Table 1. Possible range, observed range, mean, and standard deviation of health-promoting behaviors in each subgroup and total score
The mean score obtained in men was higher than in women, but the difference was not statistically significant (p=0.136). An independent t-test was used to investigate the relationship between gender, marital status, and the total score of health-promoting behaviors and their dimensions. The mean score of physical activity, spiritual growth, stress management, and total health-promoting score was higher in males, but the difference was significant only in the physical activity dimension (p=0.0001).
The highest correlation of overall health-promoting behaviors with spiritual growth (r=0.782) followed by stress management (r=0.777), interpersonal relationships (r=0.767), responsibility for health (r=0.73), nutrition (r=0.641), and physical activity (r=0.611; p<0.001). Among the subscales, the highest correlation between spiritual growth and stress management (r=0.676) and the lowest correlation between physical activity and interpersonal relationships (r=0.253) were observed (p=0.001).
In an intervention study, 60 people were included in the intervention group at the beginning of training. In the three-month follow-up, 55 people completed the study. The mean and standard deviation of the participant's age was 40.42±6.89. On the other hand, the study's results showed that out of 55 people participating, 24 people (43.6%) were men, 31 (56.4%) were women, 76.4% were married, and the rest were single. The participants had between 1 and 30 years of work experience, and their average work experience was 15.76±9.17. 54.5% had a master's degree. 74.5% of employees reported an average income level. A paired t-test was used to compare the average physical activity and its items before and after the educational intervention. The results showed that the average for all the physical activity items increased after the educational intervention. The statistical test showed a significant difference before and after the educational intervention in the housework and family care item and the average physical activity item (p=0.04; p=0.029). The average total physical activity after the educational intervention in people (8910.78±820.69) increased compared to before the intervention (6605.93±643.85), and the statistical test showed a significant difference (p<0.016; Table 2).
Table 2. Comparison of average physical activity and items before and 3 months after the educational intervention
The average score for the total physical activity of the participants after the intervention was higher in men than in women. Also, the average score of total physical activity of married people after the intervention was higher than that of single people. Independent t-test was used to investigate the relationship between gender, marital status, and total physical activity score. Before the educational intervention, there was no significant relationship between gender, marital status, and average physical activity (p<0.05). Still, the independent t-test showed a significant relationship between gender, marital status, and average physical activity after the educational intervention (p<0.05; Table 3).
Table 3. Comparison of average physical activity in participants according to gender and marital status before and three months after the educational intervention
Discussion
A healthy lifestyle is essential in reducing the spread of diseases, promoting health, and improving quality of life. Considering the critical role of employees as valuable resources and service providers to the people and their essential role in their family and surrounding environment, this study was conducted to investigate the status of health-promoting behaviors of the employees of Ilam University of Medical Sciences. The study's findings indicate that the employees' practices that promote health are in good shape. The results of a study by Moradi & Shojaizade on the lifestyle of workers in Andimeshk health centers revealed that the amount of health-improving behavior described was average [24]. The average status of health-promoting habits has been the subject of several research, one of which was conducted by Chenary et al. [25]. Mostafay Najafabadi & Rezaei's [26] research on nurses supports this study's findings. Furthermore, most nurses had an average overall score for health-promoting activities in a Taiwanese study, which aligns with the findings of the current investigation [25-27].
Men than women reported living better lives in this survey. This outcome agrees with the findings of Moradi & Shojaizade [24]. Mahmoodi et al.'s study on promoting a healthy lifestyle revealed that women had better lives than men, a finding that is at odds with our own. The disparity in health-promoting behaviors across genders may stem from factors such as awareness, education, availability of suitable environments for physical exercise, and community culture that influences these behaviors [7]. The findings showed that the participants had appropriate conditions in the spiritual growth dimension compared to other dimensions of health-promoting behaviors. Participants physical activity level was low and was not enough to impact on health status and quality of life. A review of studies showed that results from similar studies are consistent with the results of the present study. In the studies of Chenary et al. [25], Motlagh et al. [28], and Ghorabi et al. [29], the highest score was in the dimension of spiritual growth; these results are consistent with the result of the present study. In the present study, the lowest score on behavior was in the dimension of physical activity. In line with this finding, the lowest score of behavior in the studies of Chenary et al. [25], Edrisi et al. [5], and Ghorabi et al. [29], were in the dimension of physical activity. Regarding the intervention study, the results show that the individuals' physical activity increased when the instructional program was implemented. Numerous research studies have shown that an educational intervention enhanced participants' performance regarding weekly physical activity totals [30-33]. Furthermore, Teymoori et al. demonstrated that the Pender model intervention program had the highest impact on activity levels [34]. In the study of Parhoodeh et al., the educational intervention program increased people's level of physical activity, which is generally consistent with the present study. This issue shows the importance and effect of holding educational and cultural meetings and recommending and persuading people [35].
Vafaee Najar et al.'s employee-based study demonstrated a statistically significant rise in the training group's average physical activity scores following the educational intervention. According to the results of this study, 75% of the test group members were engaging in moderate physical activity following the execution of the training program, and none of them were in the light or sedentary stage. Only 11.2% of participants in the control group had moderate physical activity after the intervention, compared to 88.2% of light and sedentary individuals [22]. In the investigation of the efficacy of the electronic training program that raised the BMI and physical activity levels of female employees, Amini et al. demonstrated that, before the training, there was no discernible difference in the levels of physical activity between the intervention group and the control group; However, following the training, the average the favorable impact of educational programs in the intervention group is demonstrated by the score in the intervention group, which grew up to three times and was considerably higher than the control group. As a result, web-based, brief message, multimedia training treatments have the potential to both prevent and exacerbate diseases associated with inactivity in female employees [19]. Exercise has a positive effect on lowering depression levels in women, according to research by Jalalinia et al. on the relationship between depression and obesity [36]. After investigating how the University of Medical Sciences female students' regular activities were affected by the second physical education curriculum based on the Bezenf model, Hazavehei et al. concluded that there was a significant difference in the average scores of the Bezenf model components between the intervention group and the control group following the educational intervention. After the training session ended, the intervention group significantly improved in engaging in regular physical activity in the following two and four months [37]. Men scored higher on the average for physical activity than women, and the statistical test revealed a significant correlation between gender and physical activity level. This finding is consistent with Sane et al.'s study, which found that working women engaged in less physical activity than men [38]. Male employees engaged in more significant physical activity than female employees, according to a study by Vafaee Najar et al. on workers in Aqqola City. This suggests a significant correlation between gender and physical activity level. Other contextual factors mentioned in this issue as intrapersonal and environmental barriers to women leading active lives in Iran include the unique characteristics of society and family norms, attention to cultural considerations regarding women's sports, and limited access to gyms and physical exercise spaces [22].
The average physical activity of married individuals was higher than that of single individuals in the current study, with a statistically significant difference. According to Vafaee Najar et al.'s study, married individuals had higher average physical activity levels than single individuals. However, the Mann-Whitney statistical test revealed no significant correlation between marital status and physical activity level, contradicting the current investigation's findings [22]. An increase in the average was noted before and after the educational intervention in the following fields on the standard physical activity questionnaire: Sports and leisure time physical activity, housework and family care, physical activity for transportation, and physical activity related to daily work. The statistical test revealed significant physical activity in the domain of housework, which includes walking during leisure time, intense and moderate physical activity, and moderate physical activity. This finding contradicts the findings of Mazloumi Mahmoodabad et al., which focused on homemakers. Mazloumi Mahmoodabad et al. found no significant differences when comparing the intervention and control groups in the areas of housework and family care. Consistent with the findings of Mazloumi Mahmoodabad et al. [18], there was no statistically significant variation in physical activity for transportation in the current study. In Mazloumi Mahmoodabad et al., significant differences were observed between the two groups (control and intervention) when comparing physical activity during leisure time and sports. These findings are incongruent with the current investigation. Intense and moderate physical exercise, as well as recreational walking, fall under this category. Mazloumi Mahmoodabad et al. focused exclusively on homemakers, who have more free time for physical activity than working women, which could be one of the possible causes of this problem [18].
The program's design was based on identifying the priority dimension of the lifestyle questionnaire. This allowed the educational program to be designed based on the real needs of the studied population, and as a result, it had a favorable effect on the employees' physical activity.
Conclusion
The training program's design, based on the intervention mapping model, improves the employees' physical activity.
Acknowledgements: This research was the thesis for the master's degree in health education, and we are grateful to all the study participants.
Ethical Permissions: The research ethics committee confirmed the study (code: IR. MEDILAM. REC.1398.098).
Conflicts of Interests: No conflict of interest is reported in this study.
Authors' Contribution: Tahmasebi Ghorabi S (First Author), Introduction Writer/Main Researcher (35%); Karimi Rouzbahani A (Second Author), Introduction Writer/Assistant Researcher (15%); Abedzadeh Zavareh MS (Third Author), Methodologist (15%); Sadeghifar J (Fourth Author), Methodologist (10%); Jalilian M (Fifth Author), Discussion Writer/Statistical Analyst (25%)
Funding/Support: This study was financially supported by the Deputy of Research of Ilam University of Medical Sciences.
Article Type: Original Research |
Subject:
Health Education and Health Behavior
Received: 2024/02/16 | Accepted: 2024/08/17 | Published: 2024/08/24
Received: 2024/02/16 | Accepted: 2024/08/17 | Published: 2024/08/24
References
1. Tol A, Tavassoli E, Shariferad GR, Shojaeezadeh D. Health-promoting lifestyle and quality of life among undergraduate students at school of health, Isfahan university of medical sciences. J Educ Health Promot. 2013;2:11. [Link] [DOI:10.4103/2277-9531.108006]
2. Nilsaz M, Tavasoli E, Mazaheri M, Sohrabi F, Khezeli M, Ghazanfari Z, et al. Study of health-promotion behaviors and life style among students of Dezful universities. J Ilam Univ Med Sci. 2013;20(5):168-75. [Persian] [Link]
3. Phipps WJ, Sands JK, Marek JF. Medical-surgical nursing: Concepts and clinical practice. Maryland Heights: Mosby; 1999. [Link]
4. Habibi A, Neekpoor S, Seyedolshohda M, Haghani H. Health promotion behaviours and Quality of life among elderly people: A crosssectional survey 2006. J Ardabil Univ Med Sci. 2008;8(1):29-36. [Persian] [Link]
5. Edrisi M, Khademloo M, Ghorban AA, Gooran F, Khalili-Azandehi H, Bahrami B, et al. Self report of health promoting behaviors of nurses working in the teaching hospitals. J Mazandaran Univ Med Sci. 2013;23(105):52-9. [Persian] [Link]
6. Potter PA, Perry AG. Fundamentals of nursing. Maryland Heights: Mosby Elsevier; 2009. [Link]
7. Mahmoodi H, Zareipour MA, Hasanpoor E, Housaenpour H, Babazadeh T, Sharifi-Saqqezi P. Compare the health promoting behaviors among nurses, health and administrative staff. Iran J Nurs. 2016;29(99-100):56-65. [Persian] [Link] [DOI:10.29252/ijn.29.99.100.56]
8. Harooni J, Hassanzadeh A, Mostafavi F. Influencing factors on health promoting behavior among the elderly living in the community. J Educ Health Promot. 2014;3:40. [Link] [DOI:10.4103/2277-9531.131921]
9. Mcelligott D, Siemers S, Thomas L, Kohn N. Health promotion in nurses: Is there a healthy nurse in the house?. Appl Nurs Res. 2009;22(3):211-5. [Link] [DOI:10.1016/j.apnr.2007.07.005]
10. Hassani L, Alighias M, Ghanbarnejad A, Shahab-Jahanlu A, Gholamnia-Shirvani Z. Effect of educational intervention on health-promoting behaviors of high school students in Karaj city. J Prev Med. 2015;2(1):62-9. [Persian] [Link]
11. Nezhaddadgar N, Nokhostin B, Zakipoor Gh. Intervention mapping to design adolescent puberty health promotion programs. Ardabil: Mohaghegh Ardabili; 2018. [Persian] [Link]
12. Kok G, Gottlieb NH, Peters GJ, Mullen PD, Parcel GS, Ruiter RA, et al. A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychol Rev. 2015;10(3):297-312. [Link] [DOI:10.1080/17437199.2015.1077155]
13. Mirzaei-Alavijeh M, Kok G, Hidarnia A, Niknami S, Motlagh MI. My family-study, early-onset substance use prevention program: An application of intervention mapping approach. J Educ Community Health. 2017;3(4):1-15. [Persian] [Link] [DOI:10.22631/ajhms.2016.43197]
14. Kok G. A practical guide to effective behavior change: How to apply theory- and evidence-based behavior change methods in an intervention. Eur Health Psychol. 2014;16(5):156-70. [Link]
15. Mirzaei-Alavijeh M, Hidarnia A, Kok G, Niknami S, Motlagh MI. The 'my family-study' onset substance use prevention programme in early childhood: An introduction. Arvand J Health Med Sci. 2016;1(3):188-90. [Link] [DOI:10.22631/ajhms.2016.43197]
16. Bayat B, Mohebbi B, Tol A, Sadeghi R, Yekaninejad MS. Effectiveness of an educational intervention on improving health-promoting behaviors and quality of life among health volunteers: Application the BASNEF model. Payesh. 2018;17(1):53-65. [Persian] [Link]
17. Walker SN, Sechrist KR, Pender N. The health-promoting lifestyle profile: Development and psychometric characteristics. Nurs Res. 1987;36(2):76-81. [Link] [DOI:10.1097/00006199-198703000-00002]
18. Mazloumi Mahmoodabad SS, Rahavi Ezabadi R, Baghiani Moghadam MH, Niknejad N, DehghaniTafti A. Effects of exercise training on housewives married 20-45 years Noor city. J Toloo-E-Behdasht. 2017;16(3):21-33. [Persian] [Link]
19. Amini N, Shojaeezadeh D, Saffari M. The study of the effect of e-education on physical activity and body mass index of female employees. J Sch Public Health Inst Public Health Res. 2014;11(3):95-106. [Persian] [Link]
20. Baghiani M, Bakhtari Aghdam F, Asghari Jafarabadi M, Allahverdipour H, Dabagh Nikookheslat S, Safarpour S. The Iranian version of international physical activity questionnaire (IPAQ) in Iran: Content and construct validity, factor structure, internal consistency and stability. World Appl Sci J. 2012;18(8):1073-80. [Link]
21. Mohammadi Zeidi I, Pakpour Hajiagha A, Mohammadi Zeidi B. Reliability and validity of Persian version of the health-promoting lifestyle profile. J Mazandaran Univ Med Sci. 2011;20(1):102-13. [Persian] [Link]
22. Vafaee Najar A, Vahedian Shahroody M, Dogonchi M, Dogonchi AM. The effectiveness of physical activity training on emotional exhaustion of employees in city of Agh Ghala-2013. Pajouhan Sci J. 2017;15(2):20-6. [Persian] [Link]
23. Vafaee Najar A, Vahedian-Shahroodi M, Tehrani H, Dogonchi M, Lael-monfared E. The effectiveness of physical activity training on depersonalization and lack of accomplishment of employees. Iran J Health Educ Health Promot. 2015;3(2):116-24. [Persian] [Link]
24. Moradi A, Shojaizade D. A survey on healthy lifestyle of health care workers in Andimeshk. J Toloo-E-Behdasht. 2016;14(5):38-49. [Persian] [Link]
25. Chenary R, Noroozi A, Tahmasebi R, SaeedFiroozabadi M. Association between health locus of control and health promotion behaviors among employees' Bushehr university of medical sciences in 2013-14. Iran South Med J. 2016;19(5):877-87. [Persian] [Link] [DOI:10.18869/acadpub.ismj.19.5.877]
26. Mostafay Najafabadi H, Rezaei B. The health promotion behaviors and its correlation with selected professional factors in nurses. J Health Promot Manag. 2017;6(3):28-35. [Persian] [Link] [DOI:10.21859/jhpm-07014]
27. Tsai YC, Liu CH. Factors and symptoms associated with work stress and health-promoting lifestyle among hospital staff: A pilot study in Taiwan. BMC Health Serv Res. 2012;12:199. [Link] [DOI:10.1186/1472-6963-12-199]
28. Motlagh Z, Mazloomy-Mahmoodabad S, Momayyezi M. Study of health promotion behaviors among university of medical sciences students. Zahedan J Res Med Sci. 2011;13(4):e93999. [Persian] [Link]
29. Ghorabi ST, Jalilian M, Sadeghifar J, Zavareh MSA. Investigation of health-promoting behaviors of employees of medical university: A perspective from West of Iran. J Edu Health Promot. 2021;10:139. [Link] [DOI:10.4103/jehp.jehp_835_20]
30. Solhi M, Zinat Motlagh F, Karimzade Shirazi K, Taghdisi MH, Jalilian F. Designing and implementing educational programs to promote physical activity among students: An application of the theory of planned behavior. J Intern Med Today. 2012;18(1):45-52. [Persian] [Link]
31. Hasanvandi S, Valizade M, Honarmand MM, Mohammadesmaeel F. Effectiveness of stress management on mental health of divorced women. Procedia Soc Behav Sci. 2013;84:1559-64. [Link] [DOI:10.1016/j.sbspro.2013.06.788]
32. Khorvash M, Alam Sh, Botshkan M. The relationship between physical activity and job burnout in faculty Islamic Azad University in four countries. J Sport Manag Mot Behav. 2009;5(10):49-60. [Persian] [Link]
33. Norozi A, Tahmasbi R, Ghofranipour F, Heidarnia A. Effect of health promotion model (HPM) based education on physical activity in diabetic women. Iran J Endocrinol Metab. 2011;13(4):361-7. [Persian] [Link]
34. Teymoori P, Niknami Sh, Ghofranipour F. Effects of a school-based intervention on the basis of Pender's health promotion model to improve physical activity among high school girls. Armaghan-E-Danesh. 2007;12(2):47-59. [Persian] [Link]
35. Parhoodeh Y, Khezeli M, Bakhtiyari M, Delpisheh A, Latifi A. Effects of education based on transtheoretical model on physical activity of college students. J Health Syst Res. 2012;8(2):320-9. [Persian] [Link]
36. Jalalinia SF, Varaei Sh, Rasoulzadeh N, Kazemnejad A. Effect of physical activity on depression in obese women. Iran J Nurs Res. 2010;5(18):33-41. [Persian] [Link]
37. Hazavehei SMM, Asadi ZS, Hasanzade A, Shekarchizadeh P. A study on the effect of physical education (Π) curriculum based on BASNEF model on female students' regular physical activity in Isfahan university of medical sciences. J Adv Med Biomed Res. 2009;17(69):70-83. [Persian] [Link]
38. Sane MA, Fahim Devin H, Jafari R, Zohoorian Z. Relationship between physical activity and it's components with burnout in academic members of Daregaz Universities. Procedia Soc Behav Sci. 2012;46:4291-4. [Link] [DOI:10.1016/j.sbspro.2012.06.242]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |