



Volume 12, Issue 1 (2024)
Health Educ Health Promot 2024, 12(1): 111-117 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Naghavi S, Dortaj F, Ghaemi F, Salari-Far M. Impact of Recovery-Oriented Cognitive Therapy on Quality of Life, and Life Expectancy in Cardiovascular Patients. Health Educ Health Promot 2024; 12 (1) :111-117
URL: http://hehp.modares.ac.ir/article-5-72421-en.html
URL: http://hehp.modares.ac.ir/article-5-72421-en.html

1- Department of Psychology, Science and Research Branch, Islamic Azad University, Tehran, Iran
2- Department of Educational Psychology, Faculty of Psychology and Education, University of Allameh Tabataba’i, Tehran, Iran
3- Ministry of Health, Treatment and Medical Education, Tehran, Iran
4- Cardiovascular Diseases Research Institute, Tehran University of Medical Sciences, Tehran, Iran
2- Department of Educational Psychology, Faculty of Psychology and Education, University of Allameh Tabataba’i, Tehran, Iran
3- Ministry of Health, Treatment and Medical Education, Tehran, Iran
4- Cardiovascular Diseases Research Institute, Tehran University of Medical Sciences, Tehran, Iran
Keywords: Cardiovascular Disease [Mesh], Life Expectancy [MeSH], Quality of Life [MeSH], Recovery-Oriented Cognitive Therapy [MeSH]
Full-Text [PDF 654 kb]
(2922 Downloads)
| Abstract (HTML) (1717 Views)
Full-Text: (173 Views)
Introduction
Cardiovascular disease is a widespread condition that impacts many individuals globally, significantly altering their lifestyles [1, 2]. Apart from the physical implications, heart disease frequently has a profound influence on the psychological and emotional well-being of patients, ultimately diminishing their overall life quality [3, 4]. In addressing these concerns and promoting emotional well-being, counseling or cognitive-behavioral therapy (CBT) can be deemed advantageous [5]. In conjunction with professional assistance, individuals with heart ailments also necessitate a robust support system and open communication with their friends and family. Social isolation and strained relationships can potentially affect cardiovascular patients’ life quality detrimentally, but support groups and educational initiatives can aid individuals in coping emotionally and enriching their social interactions.
The role of life expectancy is significantly influenced by the severity and type of heart disease [6-8]. Conditions like congestive heart failure and severe coronary artery disease can significantly impact how long a person lives. It's crucial to identify these conditions early and provide medical treatment promptly. Delaying treatment can lead to complications and a shorter lifespan [9-11]. Moreover, the life expectancy of individuals with cardiovascular diseases is greatly affected by psychological factors. The strong connection between psychological well-being and cardiovascular health underscores the importance of addressing these factors to improve a patient's overall prognosis [6, 12-14]. Chronic stress and anxiety may lead to unhealthy behaviors such as smoking, making poor dietary choices, and lacking physical activity [14-16]. Psychological factors, such as self-efficacy and motivation, play a substantial role in determining a patient's capacity to adhere to recommended health behaviors. Patients who possess confidence in their ability to manage their condition and are motivated to do so are more inclined to embrace positive lifestyle alterations that can enhance their life expectancy [17]. In the case of cardiac patients, resilience, which refers to the ability to rebound from adversity, can be advantageous. Resilient individuals typically maintain a more optimistic perspective and are better equipped to tackle life's obstacles, benefiting their overall health and durability [18, 19]. In addition, the involvement of patients with healthcare practitioners is impacted by psychological elements. Patients pursuing treatment, inquiring about their condition, and actively participating in joint decision-making processes are more likely to experience positive outcomes and extend their lifespan due to enhanced disease management [20, 21]. Hence, it is imperative to integrate multidisciplinary methodologies for cardiac care that encompass provisions for mental health support, stress management, and interventions targeting behavioral modifications [22].
Recovery-Oriented Cognitive Therapy (CT-R) is a therapeutic modality in mental health that amalgamates components of cognitive therapy with a recovery-oriented principle. The fundamental objective of this approach is to help individuals who confront mental health obstacles gain dominion over their lives and endeavor toward their ambitions and aspirations. Within the framework of CT-R, recovery is endowed with significant importance and is perceived as an intensely personal and individualized expedition toward wellness and a purposeful existence [23-27]. Unlike exclusively focusing on alleviating symptoms, recovery is regarded as a process of self-exploration, empowerment, and the attainment of goals [28-30]. CT-R endeavors to ascertain and foster an individual's aptitudes, assets, and resilience, promoting a positive perspective and a feeling of optimism. Additionally, the therapy advocates for individuals to establish connections within their communities and establish a support system. Participating in peer support groups, vocational rehabilitation programs, and other community resources that assist in recovery exemplifies this concept. A core component of CT-R involves empowering individuals to actively engage in their recovery journey, which can augment their self-esteem, self-assurance, and overall quality of life. CT-R motivates individuals to establish and pursue recovery objectives in various domains, such as employment, education, interpersonal relationships, or personal passions. Accomplishing these aims can profoundly enhance one's sense of purpose and contentment. Accomplishing these aims can significantly ameliorate one's sense of purpose and satisfaction with life. The daily functioning of individuals frequently experiences enhancement as they acquire skills to cope with their symptoms and strive towards their aspirations effectively. This augmentation encompasses better performance in occupational or educational settings, enhanced interpersonal connections, and increased capacity to engage in significant activities [23-26, 31].
Including CT-R in managing patients with cardiovascular diseases recognizes the significance of attending to the psychological dimensions of cardiovascular well-being. Its objective was to enhance the well-being and longevity of individuals with heart ailments by advocating for a more comprehensive and patient-focused approach to their treatment.
Materials and Methods
This semi-experimental study employed a pre-test/post-test design in cardiovascular patients who visited the Tehran Heart Center hospital for cardiac rehabilitation in 2022-2023. According to experimental research principles, the needed number of samples was 15-30 [32]. 60 patients from the cardiac rehabilitation unit were chosen as convenience sampling and were eligible to participate in the study. Patients who underwent coronary artery bypass surgery and percutaneous coronary intervention were selected based on specific entry criteria; age under 70 years, their initial visit to the rehabilitation department, and a lack of concurrent psychotherapy outside the rehabilitation setting. Random allocation was implemented by a nurse utilizing a similar ball method. In this approach, 60 identical balls were prepared, each containing the labels of the two groups. Subsequently, participants were asked to select one ball each, randomly determining their group assignment. Of the 30 patients initially allocated to the experimental group, 6 declined participation in the intervention sessions, resulting in a starting count of 24 patients in the experimental group and 30 patients in the control group.
Data were gathered using the short form 36 (SF-36) and adult hope scale-12 (AHS-12) questionnaires.
Short Form 36 (SF-36): was used to assess the patients’ quality of life under examination. Comprising 36 items, this questionnaire evaluates 8 distinct facets of quality of life, including general health, physical functioning, role limitations arising from physical health issues, role limitations due to emotional challenges, vitality, physical pain, social functioning, and mental health. The internal consistency of the SF-36 sub-scales, as reported by Rafaati et al., exhibited a range between 0.68 and 0.90, as determined through Cronbach's alpha analysis [33]. Furthermore, the validation study by Saleh Pour et al. [34] indicated favorable internal consistency for most SF-36 sub-scales, except for social functioning and emotional difficulties, which yielded coefficients ranging from 0.93 to 0.42 [35].
Adult Hope Scale-12 (AHS-12): The life expectancy questionnaire developed by Snyder et al. (commonly known as the Adult Hope Scale, AHS) is a widely utilized assessment tool. This questionnaire, originating in 1991 and composed of 12 items, employs a five-point Likert scale ranging from "entirely disagree" to "completely agree" to gauge individuals' perspectives on various aspects of life expectancy. The AHS questionnaire delves into two fundamental dimensions of life expectancy: "route thinking" and "agency thinking". Notably, four lie detector questions are integrated into this questionnaire, suitable for individuals aged 15 and above. Scores on the AHS questionnaire can span a range from 8 to 64. Regarding psychometric properties, Snyder and Lopez reported that the full test demonstrated favorable internal consistency, with coefficients ranging from 0.74 to 0.84, and exhibited a test-retest reliability of 0.80 [36]. Additionally, Kermani et al. [37] established the validity coefficient of this scale by applying Cronbach's coefficient of 0.86 and a test-retest coefficient of 0.81. Furthermore, Gholamalishahi et al. [38] and other researchers have affirmed the high overall internal consistency of the 12-item life expectancy questionnaire, reporting a coefficient of 0.93, along with significant evidence of validity.
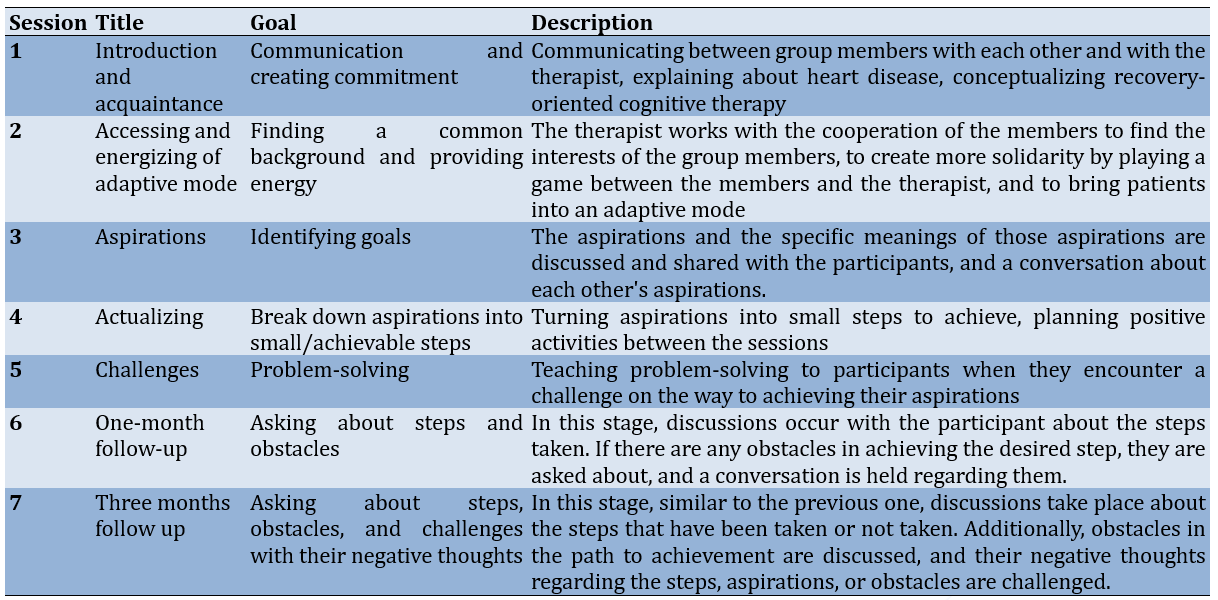
After discussing the start time and how cardiovascular patients participated in the treatment sessions with the staff, the hospital sent a list of the community that was the subject of the study. Getting agreement to participate in therapy, planned interventions, and therapeutic processes marked the start of the following stage. Patients in both groups received the questionnaires to fill out before the start of the therapy session. The experimental group had an intervention for two weekly sessions (each lasting one hour and thirty minutes). Patients had a second evaluation using the questionnaires once the intervention was implemented. After the intervention concluded, patients were assessed again during follow-up evaluations conducted at three- and six-months using questionnaires as part of the assessment process. The outcomes of the post-intervention evaluation were compared to those of the pre-intervention (Table 1).
Table 1. The content of the recovery-oriented cognitive therapy sessions
The data was analyzed using the Bonferroni t-test, covariance-based statistics, and one-way multivariate analysis of variance (MANOVA) using the SPSS 21 software.
Findings
The mean age of the experimental group was 58.20±6.93 years, and that of the control group was 58.56±7.09 years (p>0.05). In the experimental group, 15 were male and 9 were female; in the control group, 18 were male and 12 were female. In the experimental group, 14 patients had CABG surgery, and 10 had PCI surgery, while in the control group, 16 patients had CABG surgery, and 14 had PCI surgery.
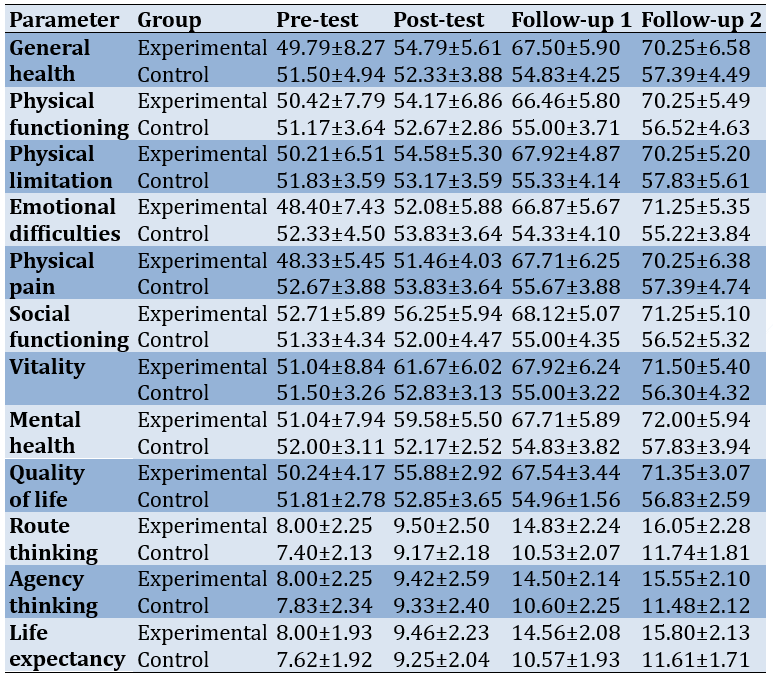
There were no significant differences in the quality of life and life expectancy parameters between the experimental and control groups (Table 2).
Table 2. The mean of the descriptive parameters of pre-test, post-test, follow-up 1, and follow-up 2 in experimental and control groups
The Kolmogorov-Smirnov test showed the normality of the parameters’ distribution. The homogeneity of variance-covariance matrices was shown by the box test. Also, Levene's test demonstrated the equality of variance of the groups (df1=1; df2=41; p>0.05). Mauchly's sphericity test was used to check the equality of covariance assumption. The chi-square value obtained was not significant, and therefore, the assumption of equality of covariance was confirmed.
The time (p<0.001 and F1, 41=533.66) group (p<0.001 and F1, 41=102.54) and time*group (p<0.001 and F1, 41=222.91) significantly affected the quality of life. Also, the time (p<0.001 and F1, 41=3553.94) group (p<0.001 and F1, 41=58.54) and time*group (p<0.001 and F1, 41=519.48) significantly affected life expectancy.
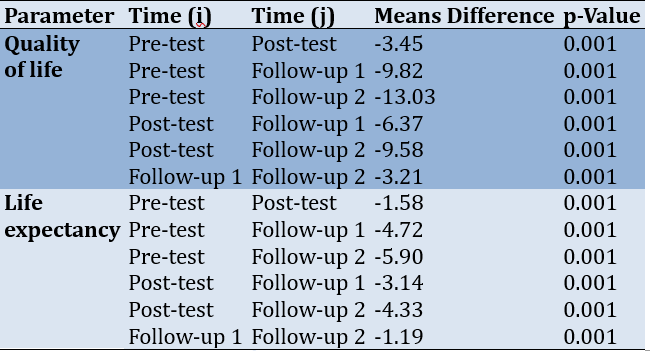
The quality of life and life expectancy showed consistent and significant improvement across all four measured time points (Table 3).
Table 3. Comparing the periods' difference in quality of life and life expectancy by the Bonferroni t-test
Discussion
In the present investigation, the utilization of CT-R exhibits considerable potential in ameliorating the standard of existence in individuals afflicted with cardiac conditions. In accordance with our discoveries, CT-R exerts a remarkable influence on two dimensions of life expectancy. Our discoveries lend support to antecedent scholarly inquiries into the psychological interventions employed in the realm of cardiac treatment. These findings substantiate earlier analyses that have established a correlation between psychological well-being, modifications in lifestyle, and cardiovascular outcomes [39, 40]. They highlight the significance of addressing the physiological and psychological dimensions of managing cardiovascular disease. Cardiovascular disease often carries a notable psychological burden, encompassing anxiety, depression, and fear [41, 42]. The emphasis on cognitive restructuring in CT-R equips patients with strategies to challenge and modify negative thought patterns. CT-R can potentially alleviate psychological distress by promoting positive thinking, affording heart patients increased emotional stability and overall well-being. CT-R equips individuals to tackle stress and setbacks effectively by attending to cognitive distortions and enhancing problem-solving abilities. Patients who acquire confidence in their capacity to cope efficiently experience a heightened sense of control over their condition, thus fostering a more optimistic perspective on life. CT-R empowers individuals to assume responsibility for their well-being by actively engaging patients in their recovery journey and furnishing them with the necessary tools to make informed decisions. This phenomenon of empowerment not only enhances compliance with medical advice but augments overall lifespan and self-regard [23-26, 29].
Due to the limitations imposed by physical constraints and the psychological anguish experienced, cardiovascular illness has the potential to precipitate social seclusion [43-45]. CT-R, an abbreviation for Recovery-oriented cognitive therapy, addresses the predicament of social anxiety and communication proficiencies, thereby encouraging patients to partake in societal engagements and reestablish their support networks actively. Culturing superior social interactions alleviates feelings of isolation and fortifies interpersonal connections, fostering a more gratifying social existence [46, 47]. The recovery-oriented paradigm of CT-R inspires patients to perceive their encounters as occasions for personal maturation and progress. By promoting resilience and adaptability, CT-R enables individuals to discover significance and purpose in their lives despite the tribulations associated with cardiac maladies. This shift in perspective can be transformative, ultimately leading to a more sanguine and rewarding existence.
Recovery-Oriented Cognitive Therapy significantly enhances the quality of life among individuals diagnosed with cardiovascular diseases. CT-R embodies a comprehensive strategy to support heart patients by addressing their psychological distress, cultivating adaptive coping mechanisms and empowerment, facilitating improved social interactions, and fostering resilience. Though the direct impact of CT-R on heart patients is still in development, the fundamental principles and techniques that underlie this therapeutic approach are well-aligned with the diverse needs of individuals with cardiovascular diseases. Long-term follow-up studies and additional research will contribute to a more comprehensive comprehension of how CT-R can be effectively incorporated into cardiac care to optimize patients' overall well-being.
Finally, CT-R offers a promising pathway for enhancing the quality of life for individuals with heart ailments by equipping them with the necessary resources and assistance to navigate their condition's physical and emotional obstacles. As our comprehension of this therapeutic approach deepens, it can transform the field of cardiac care by implementing a more comprehensive and patient-focused framework that duly considers the physiological and psychological dimensions of heart disease.
Cardiovascular patients require physical and psychological interventions to enhance their quality of life post-surgery. Psychological interventions such as cognitive-behavioral therapy and motivational interviewing are administered to improve patients' lives, including medication adherence, dietary compliance, and lifestyle modifications. However, there remains a gap in interventions addressing patients' aspirations and goals, which are crucial for enhancing their overall well-being. Recovery-oriented cognitive therapy aims to address patients' achievable aspirations and rectify cognitive distortions hindering progress towards them. This therapy aims to alleviate stress and anxiety, instill a sense of purpose, and potentially augment patients' life expectancy and overall health by facilitating steps toward these aspirations. This study holds potential significance for healthcare practitioners seeking to optimize patient care strategies.
This study did not include all subgroups of heart patients. Extending the intervention to encompass a broader range of patient demographics, including varying age groups and genders, would yield more comprehensive insights. Questionnaires were administered online and in person, potentially introducing variability. Standardizing the delivery method would enhance data consistency. The long-term efficacy of recovery-oriented cognitive therapy in sustaining improvements among these patients remains unexplored. This study marks the inaugural implementation of recovery-oriented cognitive therapy among heart patients in Iran, offering valuable insigts for healthcare practitioners. This study distinguishes itself by exploring novel variables affecting heart patients' quality of life and overall health, rendering it instrumental in elucidating various factors influencing health outcomes.
Conclusion
Recovery-oriented cognitive therapy positively affects the quality of life and life expectancy in cardiac patients.
Acknowledgments: We would like to express our sincere gratitude to the Tehran Heart Center for their invaluable support and collaboration.
Ethical Permissions: The Tehran Science and Research Branch, the Department of Psychology, the Institutional Ethical Review Board of Azad University all approved this study under the designation IR.IAU.SRB.REC.1402.089.
Conflicts of Interests: Authors declare that they have no conflict of interest.
Authors’ Contribution: Naghavi S (First Author), Main Researcher/Discussion Writer/Statistical Analyst (30%); Dortaj F (Second Author), Main Researcher/Discussion Writer (30%); Ghaemi F (Third Author), Introduction Writer (20%); Salari Far M (Fourth Author), Main Researcher/Methodologist (20%)
Funding/Support: Nothing declared by the authors.
Cardiovascular disease is a widespread condition that impacts many individuals globally, significantly altering their lifestyles [1, 2]. Apart from the physical implications, heart disease frequently has a profound influence on the psychological and emotional well-being of patients, ultimately diminishing their overall life quality [3, 4]. In addressing these concerns and promoting emotional well-being, counseling or cognitive-behavioral therapy (CBT) can be deemed advantageous [5]. In conjunction with professional assistance, individuals with heart ailments also necessitate a robust support system and open communication with their friends and family. Social isolation and strained relationships can potentially affect cardiovascular patients’ life quality detrimentally, but support groups and educational initiatives can aid individuals in coping emotionally and enriching their social interactions.
The role of life expectancy is significantly influenced by the severity and type of heart disease [6-8]. Conditions like congestive heart failure and severe coronary artery disease can significantly impact how long a person lives. It's crucial to identify these conditions early and provide medical treatment promptly. Delaying treatment can lead to complications and a shorter lifespan [9-11]. Moreover, the life expectancy of individuals with cardiovascular diseases is greatly affected by psychological factors. The strong connection between psychological well-being and cardiovascular health underscores the importance of addressing these factors to improve a patient's overall prognosis [6, 12-14]. Chronic stress and anxiety may lead to unhealthy behaviors such as smoking, making poor dietary choices, and lacking physical activity [14-16]. Psychological factors, such as self-efficacy and motivation, play a substantial role in determining a patient's capacity to adhere to recommended health behaviors. Patients who possess confidence in their ability to manage their condition and are motivated to do so are more inclined to embrace positive lifestyle alterations that can enhance their life expectancy [17]. In the case of cardiac patients, resilience, which refers to the ability to rebound from adversity, can be advantageous. Resilient individuals typically maintain a more optimistic perspective and are better equipped to tackle life's obstacles, benefiting their overall health and durability [18, 19]. In addition, the involvement of patients with healthcare practitioners is impacted by psychological elements. Patients pursuing treatment, inquiring about their condition, and actively participating in joint decision-making processes are more likely to experience positive outcomes and extend their lifespan due to enhanced disease management [20, 21]. Hence, it is imperative to integrate multidisciplinary methodologies for cardiac care that encompass provisions for mental health support, stress management, and interventions targeting behavioral modifications [22].
Recovery-Oriented Cognitive Therapy (CT-R) is a therapeutic modality in mental health that amalgamates components of cognitive therapy with a recovery-oriented principle. The fundamental objective of this approach is to help individuals who confront mental health obstacles gain dominion over their lives and endeavor toward their ambitions and aspirations. Within the framework of CT-R, recovery is endowed with significant importance and is perceived as an intensely personal and individualized expedition toward wellness and a purposeful existence [23-27]. Unlike exclusively focusing on alleviating symptoms, recovery is regarded as a process of self-exploration, empowerment, and the attainment of goals [28-30]. CT-R endeavors to ascertain and foster an individual's aptitudes, assets, and resilience, promoting a positive perspective and a feeling of optimism. Additionally, the therapy advocates for individuals to establish connections within their communities and establish a support system. Participating in peer support groups, vocational rehabilitation programs, and other community resources that assist in recovery exemplifies this concept. A core component of CT-R involves empowering individuals to actively engage in their recovery journey, which can augment their self-esteem, self-assurance, and overall quality of life. CT-R motivates individuals to establish and pursue recovery objectives in various domains, such as employment, education, interpersonal relationships, or personal passions. Accomplishing these aims can profoundly enhance one's sense of purpose and contentment. Accomplishing these aims can significantly ameliorate one's sense of purpose and satisfaction with life. The daily functioning of individuals frequently experiences enhancement as they acquire skills to cope with their symptoms and strive towards their aspirations effectively. This augmentation encompasses better performance in occupational or educational settings, enhanced interpersonal connections, and increased capacity to engage in significant activities [23-26, 31].
Including CT-R in managing patients with cardiovascular diseases recognizes the significance of attending to the psychological dimensions of cardiovascular well-being. Its objective was to enhance the well-being and longevity of individuals with heart ailments by advocating for a more comprehensive and patient-focused approach to their treatment.
Materials and Methods
This semi-experimental study employed a pre-test/post-test design in cardiovascular patients who visited the Tehran Heart Center hospital for cardiac rehabilitation in 2022-2023. According to experimental research principles, the needed number of samples was 15-30 [32]. 60 patients from the cardiac rehabilitation unit were chosen as convenience sampling and were eligible to participate in the study. Patients who underwent coronary artery bypass surgery and percutaneous coronary intervention were selected based on specific entry criteria; age under 70 years, their initial visit to the rehabilitation department, and a lack of concurrent psychotherapy outside the rehabilitation setting. Random allocation was implemented by a nurse utilizing a similar ball method. In this approach, 60 identical balls were prepared, each containing the labels of the two groups. Subsequently, participants were asked to select one ball each, randomly determining their group assignment. Of the 30 patients initially allocated to the experimental group, 6 declined participation in the intervention sessions, resulting in a starting count of 24 patients in the experimental group and 30 patients in the control group.
Data were gathered using the short form 36 (SF-36) and adult hope scale-12 (AHS-12) questionnaires.
Short Form 36 (SF-36): was used to assess the patients’ quality of life under examination. Comprising 36 items, this questionnaire evaluates 8 distinct facets of quality of life, including general health, physical functioning, role limitations arising from physical health issues, role limitations due to emotional challenges, vitality, physical pain, social functioning, and mental health. The internal consistency of the SF-36 sub-scales, as reported by Rafaati et al., exhibited a range between 0.68 and 0.90, as determined through Cronbach's alpha analysis [33]. Furthermore, the validation study by Saleh Pour et al. [34] indicated favorable internal consistency for most SF-36 sub-scales, except for social functioning and emotional difficulties, which yielded coefficients ranging from 0.93 to 0.42 [35].
Adult Hope Scale-12 (AHS-12): The life expectancy questionnaire developed by Snyder et al. (commonly known as the Adult Hope Scale, AHS) is a widely utilized assessment tool. This questionnaire, originating in 1991 and composed of 12 items, employs a five-point Likert scale ranging from "entirely disagree" to "completely agree" to gauge individuals' perspectives on various aspects of life expectancy. The AHS questionnaire delves into two fundamental dimensions of life expectancy: "route thinking" and "agency thinking". Notably, four lie detector questions are integrated into this questionnaire, suitable for individuals aged 15 and above. Scores on the AHS questionnaire can span a range from 8 to 64. Regarding psychometric properties, Snyder and Lopez reported that the full test demonstrated favorable internal consistency, with coefficients ranging from 0.74 to 0.84, and exhibited a test-retest reliability of 0.80 [36]. Additionally, Kermani et al. [37] established the validity coefficient of this scale by applying Cronbach's coefficient of 0.86 and a test-retest coefficient of 0.81. Furthermore, Gholamalishahi et al. [38] and other researchers have affirmed the high overall internal consistency of the 12-item life expectancy questionnaire, reporting a coefficient of 0.93, along with significant evidence of validity.
After discussing the start time and how cardiovascular patients participated in the treatment sessions with the staff, the hospital sent a list of the community that was the subject of the study. Getting agreement to participate in therapy, planned interventions, and therapeutic processes marked the start of the following stage. Patients in both groups received the questionnaires to fill out before the start of the therapy session. The experimental group had an intervention for two weekly sessions (each lasting one hour and thirty minutes). Patients had a second evaluation using the questionnaires once the intervention was implemented. After the intervention concluded, patients were assessed again during follow-up evaluations conducted at three- and six-months using questionnaires as part of the assessment process. The outcomes of the post-intervention evaluation were compared to those of the pre-intervention (Table 1).
Table 1. The content of the recovery-oriented cognitive therapy sessions
The data was analyzed using the Bonferroni t-test, covariance-based statistics, and one-way multivariate analysis of variance (MANOVA) using the SPSS 21 software.
Findings
The mean age of the experimental group was 58.20±6.93 years, and that of the control group was 58.56±7.09 years (p>0.05). In the experimental group, 15 were male and 9 were female; in the control group, 18 were male and 12 were female. In the experimental group, 14 patients had CABG surgery, and 10 had PCI surgery, while in the control group, 16 patients had CABG surgery, and 14 had PCI surgery.
There were no significant differences in the quality of life and life expectancy parameters between the experimental and control groups (Table 2).
Table 2. The mean of the descriptive parameters of pre-test, post-test, follow-up 1, and follow-up 2 in experimental and control groups
The Kolmogorov-Smirnov test showed the normality of the parameters’ distribution. The homogeneity of variance-covariance matrices was shown by the box test. Also, Levene's test demonstrated the equality of variance of the groups (df1=1; df2=41; p>0.05). Mauchly's sphericity test was used to check the equality of covariance assumption. The chi-square value obtained was not significant, and therefore, the assumption of equality of covariance was confirmed.
The time (p<0.001 and F1, 41=533.66) group (p<0.001 and F1, 41=102.54) and time*group (p<0.001 and F1, 41=222.91) significantly affected the quality of life. Also, the time (p<0.001 and F1, 41=3553.94) group (p<0.001 and F1, 41=58.54) and time*group (p<0.001 and F1, 41=519.48) significantly affected life expectancy.
The quality of life and life expectancy showed consistent and significant improvement across all four measured time points (Table 3).
Table 3. Comparing the periods' difference in quality of life and life expectancy by the Bonferroni t-test
Discussion
In the present investigation, the utilization of CT-R exhibits considerable potential in ameliorating the standard of existence in individuals afflicted with cardiac conditions. In accordance with our discoveries, CT-R exerts a remarkable influence on two dimensions of life expectancy. Our discoveries lend support to antecedent scholarly inquiries into the psychological interventions employed in the realm of cardiac treatment. These findings substantiate earlier analyses that have established a correlation between psychological well-being, modifications in lifestyle, and cardiovascular outcomes [39, 40]. They highlight the significance of addressing the physiological and psychological dimensions of managing cardiovascular disease. Cardiovascular disease often carries a notable psychological burden, encompassing anxiety, depression, and fear [41, 42]. The emphasis on cognitive restructuring in CT-R equips patients with strategies to challenge and modify negative thought patterns. CT-R can potentially alleviate psychological distress by promoting positive thinking, affording heart patients increased emotional stability and overall well-being. CT-R equips individuals to tackle stress and setbacks effectively by attending to cognitive distortions and enhancing problem-solving abilities. Patients who acquire confidence in their capacity to cope efficiently experience a heightened sense of control over their condition, thus fostering a more optimistic perspective on life. CT-R empowers individuals to assume responsibility for their well-being by actively engaging patients in their recovery journey and furnishing them with the necessary tools to make informed decisions. This phenomenon of empowerment not only enhances compliance with medical advice but augments overall lifespan and self-regard [23-26, 29].
Due to the limitations imposed by physical constraints and the psychological anguish experienced, cardiovascular illness has the potential to precipitate social seclusion [43-45]. CT-R, an abbreviation for Recovery-oriented cognitive therapy, addresses the predicament of social anxiety and communication proficiencies, thereby encouraging patients to partake in societal engagements and reestablish their support networks actively. Culturing superior social interactions alleviates feelings of isolation and fortifies interpersonal connections, fostering a more gratifying social existence [46, 47]. The recovery-oriented paradigm of CT-R inspires patients to perceive their encounters as occasions for personal maturation and progress. By promoting resilience and adaptability, CT-R enables individuals to discover significance and purpose in their lives despite the tribulations associated with cardiac maladies. This shift in perspective can be transformative, ultimately leading to a more sanguine and rewarding existence.
Recovery-Oriented Cognitive Therapy significantly enhances the quality of life among individuals diagnosed with cardiovascular diseases. CT-R embodies a comprehensive strategy to support heart patients by addressing their psychological distress, cultivating adaptive coping mechanisms and empowerment, facilitating improved social interactions, and fostering resilience. Though the direct impact of CT-R on heart patients is still in development, the fundamental principles and techniques that underlie this therapeutic approach are well-aligned with the diverse needs of individuals with cardiovascular diseases. Long-term follow-up studies and additional research will contribute to a more comprehensive comprehension of how CT-R can be effectively incorporated into cardiac care to optimize patients' overall well-being.
Finally, CT-R offers a promising pathway for enhancing the quality of life for individuals with heart ailments by equipping them with the necessary resources and assistance to navigate their condition's physical and emotional obstacles. As our comprehension of this therapeutic approach deepens, it can transform the field of cardiac care by implementing a more comprehensive and patient-focused framework that duly considers the physiological and psychological dimensions of heart disease.
Cardiovascular patients require physical and psychological interventions to enhance their quality of life post-surgery. Psychological interventions such as cognitive-behavioral therapy and motivational interviewing are administered to improve patients' lives, including medication adherence, dietary compliance, and lifestyle modifications. However, there remains a gap in interventions addressing patients' aspirations and goals, which are crucial for enhancing their overall well-being. Recovery-oriented cognitive therapy aims to address patients' achievable aspirations and rectify cognitive distortions hindering progress towards them. This therapy aims to alleviate stress and anxiety, instill a sense of purpose, and potentially augment patients' life expectancy and overall health by facilitating steps toward these aspirations. This study holds potential significance for healthcare practitioners seeking to optimize patient care strategies.
This study did not include all subgroups of heart patients. Extending the intervention to encompass a broader range of patient demographics, including varying age groups and genders, would yield more comprehensive insights. Questionnaires were administered online and in person, potentially introducing variability. Standardizing the delivery method would enhance data consistency. The long-term efficacy of recovery-oriented cognitive therapy in sustaining improvements among these patients remains unexplored. This study marks the inaugural implementation of recovery-oriented cognitive therapy among heart patients in Iran, offering valuable insigts for healthcare practitioners. This study distinguishes itself by exploring novel variables affecting heart patients' quality of life and overall health, rendering it instrumental in elucidating various factors influencing health outcomes.
Conclusion
Recovery-oriented cognitive therapy positively affects the quality of life and life expectancy in cardiac patients.
Acknowledgments: We would like to express our sincere gratitude to the Tehran Heart Center for their invaluable support and collaboration.
Ethical Permissions: The Tehran Science and Research Branch, the Department of Psychology, the Institutional Ethical Review Board of Azad University all approved this study under the designation IR.IAU.SRB.REC.1402.089.
Conflicts of Interests: Authors declare that they have no conflict of interest.
Authors’ Contribution: Naghavi S (First Author), Main Researcher/Discussion Writer/Statistical Analyst (30%); Dortaj F (Second Author), Main Researcher/Discussion Writer (30%); Ghaemi F (Third Author), Introduction Writer (20%); Salari Far M (Fourth Author), Main Researcher/Methodologist (20%)
Funding/Support: Nothing declared by the authors.
Article Type: Original Research |
Subject:
Health Care
Received: 2023/11/13 | Accepted: 2024/04/8 | Published: 2024/04/30
Received: 2023/11/13 | Accepted: 2024/04/8 | Published: 2024/04/30
References
1. Aleksova A, Sinagra G, Beltrami AP, Pierri A, Ferro F, Janjusevic M, et al. Biomarkers in the management of acute heart failure: State of the art and role in COVID‐19 era. ESC Heart Fail. 2021;8(6):4465-83. [Link] [DOI:10.1002/ehf2.13595]
2. WHO. The top 10 causes of death. Geneva: World Health Organization; 2020. [Link]
3. López Barreda R, Guerrero A, De La Cuadra JC, Scotoni M, Salas W, Baraona F, et al. Poverty, quality of life and psychological wellbeing in adults with congenital heart disease in Chile. Plos one. 2020;15(10):e0240383. [Link] [DOI:10.1371/journal.pone.0240383]
4. Proskynitopoulos PJ, Heitland I, Glahn A, Bauersachs J, Westhoff-Bleck M, Kahl KG. Prevalence of child maltreatment in adults with congenital heart disease and its relationship with psychological well-being, health behavior, and current cardiac function. Front Psychiatry. 2021;12:686169. [Link] [DOI:10.3389/fpsyt.2021.686169]
5. Sadlonova M, Kermani MB, Huffman JC, Nikrahan GR, Sadeghi M, Celano CM. Feasibility, acceptability, and preliminary efficacy of a positive psychology intervention in patients with coronary heart disease: A randomized controlled trial. J Acad Consult Liaison Psychiatry. 2022;63(6):557-66. [Link] [DOI:10.1016/j.jaclp.2022.03.004]
6. Abdi A, Doulatyari PK, Mahmodi M, Torabi Y. Relationship of spiritual wellbeing with life expectancy and quality of life for patients living with heart failure. Int J Palliat Nurs. 2022;28(6):262-9. [Link] [DOI:10.12968/ijpn.2022.28.6.262]
7. Buxbaum JD, Chernew ME, Fendrick AM, Cutler DM. Contributions of public health, pharmaceuticals, and other medical care to US life expectancy changes, 1990-2015. Health Aff. 2020;39(9):1546-56. [Link] [DOI:10.1377/hlthaff.2020.00284]
8. Wamil M, Goncalves M, Rutherford A, Borlotti A, Pellikka PA. Multi-modality cardiac imaging in the management of diabetic heart disease. Front Cardiovasc Med. 2022;9:1043711. [Link] [DOI:10.3389/fcvm.2022.1043711]
9. Hung MJ, Yeh CT, Kounis NG, Koniari I, Hu P, Hung MY. Coronary artery spasm-related heart failure syndrome: Literature review. Int J Mol Sci. 2023;24(8):7530. [Link] [DOI:10.3390/ijms24087530]
10. Rezkalla SH, Kloner RA. Invasive versus conservative management in coronary artery disease. Clin Med Res. 2023;21(2):95-104. [Link] [DOI:10.3121/cmr.2023.1806]
11. Wan EYF, Yu EYT, Chin WY, Fong DYT, Choi EPH, Tang EHM, et al. Burden of CKD and cardiovascular disease on life expectancy and health service utilization: A cohort study of Hong Kong Chinese hypertensive patients. J Am Soc Nephrol. 2019;30(10):1991-9. [Link] [DOI:10.1681/ASN.2018101037]
12. Angermann CE, Ertl G. Depression, anxiety, and cognitive impairment: Comorbid mental health disorders in heart failure. Curr Heart Fail Rep. 2018;15(6):398-410. [Link] [DOI:10.1007/s11897-018-0414-8]
13. Levine GN, Cohen BE, Commodore-Mensah Y, Fleury J, Huffman JC, Khalid U, et al. Psychological health, well-being, and the mind-heart-body connection: A scientific statement from the American Heart Association. Circulation. 2021;143(10):e763-83. [Link] [DOI:10.1161/CIR.0000000000000947]
14. Murakami K, Kuriyama S, Hashimoto H. Economic, cognitive, and social paths of education to health-related behaviors: Evidence from a population-based study in Japan. Environ Health Prev Med. 2023;28:9. [Link] [DOI:10.1265/ehpm.22-00178]
15. Lim S, Tellez M, Ismail AI. Chronic stress and unhealthy dietary behaviors among low-income African-American female caregivers. Curr Dev Nutr. 2020;4(3):nzaa029. [Link] [DOI:10.1093/cdn/nzaa029]
16. Sarvandani MN, Asadi M, Khosravi F, Gearhardt AN, Razmhosseini M, Soleimani M, et al. Validation and psychological properties of the Persian version of DSM 5 yale food addiction scale 2.0 (PYFAS 2.0) in non-clinical population. Addict Health. 2022;14(3):175-84. [Link] [DOI:10.34172/ahj.2022.1283]
17. Brust M, Gebhardt WA, Numans ME, Kiefte-de Jong JC. Teachable moments: The right moment to make patients change their lifestyle. Nederlands Tijdschrift Voor Geneeskunde. 2020;164:D4835. [Dutch] [Link]
18. Kalisch R, Köber G, Binder H, Ahrens KF, Basten U, Chmitorz A, et al. The frequent stressor and mental health monitoring-paradigm: A proposal for the operationalization and measurement of resilience and the identification of resilience processes in longitudinal observational studies. Front Psychol. 2021;12:710493. [Link] [DOI:10.3389/fpsyg.2021.710493]
19. Phillips SP, Auais M, Belanger E, Alvarado B, Zunzunegui MV. Life-course social and economic circumstances, gender, and resilience in older adults: The longitudinal International Mobility in Aging Study (IMIAS). SSM Popul Health. 2016;2:708-17. [Link] [DOI:10.1016/j.ssmph.2016.09.007]
20. Faiman B, Tariman JD. Shared decision making: Improving patient outcomes by understanding the benefits of and barriers to effective communication. Clin J Oncol Nurs. 2019;23(5):540-2. [Link] [DOI:10.1188/19.CJON.540-542]
21. Jamal N, Young VN, Shapiro J, Brenner MJ, Schmalbach CE. Patient safety/quality improvement primer, part IV: Psychological safety-drivers to outcomes and well‐being. Otolaryngol Head Neck Surg. 2023;168(4):881-8. [Link] [DOI:10.1177/01945998221126966]
22. Davidson PM, Newton PJ, Tankumpuan T, Paull G, Dennison-Himmelfarb C. Multidisciplinary management of chronic heart failure: Principles and future trends. Clin Ther. 2015;37(10):2225-33. [Link] [DOI:10.1016/j.clinthera.2015.08.021]
23. Chang NA, Grant PM, Luther L, Beck AT. Effects of a recovery-oriented cognitive therapy training program on inpatient staff attitudes and incidents of seclusion and restraint. Community Ment Health J. 2014;50(4):415-21. [Link] [DOI:10.1007/s10597-013-9675-6]
24. Grant PM, Perivoliotis D, Luther L, Bredemeier K, Beck A. Rapid improvement in beliefs, mood, and performance following an experimental success experience in an analogue test of recovery-oriented cognitive therapy. Psychol Med. 2018;48(2):261-8. [Link] [DOI:10.1017/S003329171700160X]
25. Grant PM, Bredemeier K, Beck AT. Six-month follow-up of recovery-oriented cognitive therapy for low-functioning individuals with schizophrenia. Psychiatr Serv. 2017;68(10):997-1002. [Link] [DOI:10.1176/appi.ps.201600413]
26. Grant PM, Reisweber J, Luther L, Brinen AP, Beck AT. Successfully breaking a 20-year cycle of hospitalizations with recovery-oriented cognitive therapy for schizophrenia. Psychol Serv. 2014;11(2):125-33. [Link] [DOI:10.1037/a0033912]
27. Niroumand Sarvandani M, Sheikhi Koohsar J, Rafaiee R, Saeedi M, Seyedhosseini Tamijani SM, Ghazvini H, et al. COVID-19 and the brain: A psychological and resting-state functional Magnetic Resonance Imagin (fMRI) study of the whole-brain functional connectivity. Basic Clin Neurosci. 2023;14(6):753-72. [Link] [DOI:10.32598/bcn.2021.1425.4]
28. Baur A, Trösken A, Renneberg B. Content and attainment of individual treatment goals in CBT. Psychother Res. 2024;34(1):111-23. [Link] [DOI:10.1080/10503307.2023.2173681]
29. Beck AT, Grant P, Inverso E, Brinen AP, Perivoliotis D. Recovery-oriented cognitive therapy for serious mental health conditions. New York: Guilford Publications; 2020. [Link]
30. Kapeller A, Loosman I. Empowerment through health self-testing apps? Revisiting empowerment as a process. Med Health Care Philos. 2023;26(1):143-52. [Link] [DOI:10.1007/s11019-022-10132-w]
31. Kheirabadi G, Asadi M, Niroumand Sarvandani M, Jamshidi A, Mahdavi F. Risk and protective factors affecting drug craving among patients with substance use disorders undergoing opioid agonists maintenance therapy. Subst Use Misuse. 2023;58(13):1742-50. [Link] [DOI:10.1080/10826084.2023.2247068]
32. Delavar A. Psychological and educational research. Tehran: Virayesh Press; 2020. [Persian] [Link]
33. Rafaati S, Bagheri Z, Jafari P, Soltani N. Using confirmatory factor analysis (CFA) to assess structure of SF-36 (Persian version) questions for normal people and patients with chronic diseases. Hormozgan Med J. 2015;19(2):111-8. [Link]
34. Saleh Pour G, Kafi SM, Salehi I, Rezaei S. Psychometric characteristics of the health survey questionnaire (SF-36) for evaluation of multiple sclerosis: Psychometric evaluation in Iranian patients. Jundishapur Sci Med J. 2015;14(4):368-84. [Persian] [Link]
35. Lyons RA, Perry IM, Littlepage BN. Evidence for the validity of the short-form 36 questionnaire (SF-36) in an elderly population. Age Ageing. 1994;23(3):182-4. [Link] [DOI:10.1093/ageing/23.3.182]
36. Snyder CR, Lopez SJ. Positive psychology: The scientific and practical explorations of human strengths. New York: Sage Publications; 2007. [Link]
37. Kermani Z, Khodapanahi M, Heidari M. Psychometrics features of the Snyder Hope Scale. J Appl Psychol. 2011;5(3):7-23. [Link]
38. Gholamalishahi S, Mannocci A, Ettorre E, La Torre G, Okechukwu CE. Lifestyle and life expectancy questionnaire: Validation and assessment in an Italian sample. La Clinica Terapeutica. 2022;173(2):128-34. [Link]
39. Kubzansky LD, Huffman JC, Boehm JK, Hernandez R, Kim ES, Koga HK, et al. Positive psychological well-being and cardiovascular disease: JACC health promotion series. J Am Coll Cardiol. 2018;72(12):1382-96. [Link] [DOI:10.1016/j.jacc.2018.07.042]
40. Luque B, Farhane-Medina NZ, Villalba M, Castillo-Mayén R, Cuadrado E, Tabernero C. Positivity and health locus of control: Key variables to intervene on well-being of cardiovascular disease patients. J Pers Med. 2023;13(5):873. [Link] [DOI:10.3390/jpm13050873]
41. Caponnetto P. Psychological and psychopathological sequelae in cardiovascular acute disease. Ment Illn. 2018;10(2):7887. [Link] [DOI:10.4081/mi.2018.7887]
42. Niroumand Sarvandani M, Khezri Moghadam N, Kalalian Moghadam H, Asadi M, Rafaiee R, Soleimani M. The effectiveness of mindfulness-based stress reduction (MBSR) treatment on anxiety, depression and prevention of substance use relapse. Int J Health Stud. 2021;7(2):12-6. [Link]
43. Gronewold J, Engels M, Van De Velde S, Cudjoe TKM, Duman EE, Jokisch M, et al. Effects of life events and social isolation on stroke and coronary heart disease. Stroke. 2021;52(2):735-47. [Link] [DOI:10.1161/STROKEAHA.120.032070]
44. Li H, Xia N. The role of oxidative stress in cardiovascular disease caused by social isolation and loneliness. Redox Biol. 2020;37:101585. [Link] [DOI:10.1016/j.redox.2020.101585]
45. Prado JP, Galdino G. Effect of a cardiac telerehabilitation program during COVID-19 associated social isolation. Sports Med Health Sci. 2023. [Link] [DOI:10.1016/j.smhs.2023.03.002]
46. Palmer AD, Newsom JT, Rook KS. How does difficulty communicating affect the social relationships of older adults? An exploration using data from a national survey. J Commun Disord. 2016;62:131-46. [Link] [DOI:10.1016/j.jcomdis.2016.06.002]
47. Takashima R, Onishi R, Saeki K, Hirano M. The values and meanings of social activities for older urban men after retirement. PLoS One. 2020;15(11):e0242859. [Link] [DOI:10.1371/journal.pone.0242859]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |