



Volume 12, Issue 1 (2024)
Health Educ Health Promot 2024, 12(1): 1-8 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Parsaei-Mohammadi P, Sabaghinejad Z, Ghaed-Amini Harouni S. New HeLIA; Validity and Reliability of the HeLIA Test in Thalassemia Major Patients in Iran. Health Educ Health Promot 2024; 12 (1) :1-8
URL: http://hehp.modares.ac.ir/article-5-72021-en.html
URL: http://hehp.modares.ac.ir/article-5-72021-en.html
1- Thalassemia & Hemoglobinopathy Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
2- Department of Medical Library and Information Science, School of Allied Medical Sciences, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
2- Department of Medical Library and Information Science, School of Allied Medical Sciences, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Keywords: Health Education [MeSH], Health Literacy [MeSH], Holistic Health [MeSH], Thalassemia [MeSH]
Full-Text [PDF 730 kb]
(2016 Downloads)
| Abstract (HTML) (1510 Views)
Full-Text: (129 Views)
Introduction
The term "health literacy" was first used in 1974 to describe the impact of health information on the educational system, the healthcare system, and mass communication [1]. There are various definitions for this concept. One of the most well-known, provided by the World Health Organization, defines it as "Cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand, and use information in ways that promote and maintain good health" [2]. Ratzan and Parker [3] stated, "Health literacy is the capacity of people to obtain, process, and understand basic health information and services needed to make appropriate health care decisions." According to a report by the World Health Organization, health literacy has been identified as one of the main factors affecting health. The organization recommends that countries worldwide form health groups to educate and improve the level of health literacy in communities [4].
In the case of patients, the issue of health literacy becomes even more important. Studies have shown the influential role of health literacy on patient health outcomes. It is effective in increasing patient awareness, enhancing patients' ability to make informed decisions, reducing health-threatening risks, improving disease control and prevention, enhancing patient safety, improving quality of life and patient care, ensuring patients correctly understand education, and improving their health information [5-8].
Health literacy is a set of abilities, skills, and capacities in various dimensions. It includes the dimension of reading and accessing medical and health information, understanding and processing it, and the dimension of decision-making and application of this information. Considering the role of health literacy in improving the level of health of an individual and society, the existence of instruments that can measure health literacy is essential. Therefore, many instruments have been designed and used for measuring health literacy in different parts of the world, such as the Rapid Estimate of Adult Literacy in Medicine (REALM) [9], the Test of Functional Health Literacy in Adults (TOFHLA) [10], and Health Literacy Questionnaire (HLQ) [11]. In some countries, indigenous instruments have been developed to measure health literacy, such as the Korean Health Literacy Instrument (KHLI) [12], the Japanese Functional Health Literacy Test (JFHLT) [13], etc.
The Health Literacy Instrument for Adults (HeLIA) is a native instrument that is appropriate to cultural and social contexts designed to measure the health literacy of the general population aged 18 to 65 living in Iranian cities. The reliability and validity of this questionnaire were reported as appropriate in Iran by Montazeri et al. for the first time [6].
Some researchers used the HeLIA to investigate health literacy, including the study by Tavousi et al. [14], which was conducted on a sample of adults aged 18-65 In Iran. Some researchers used it in patients, including Sheikh Sharafi and Seyed Amini, [15] who evaluated health literacy in heart failure patients using the HeLIA. Chajaee et al. [16] investigated health literacy in patients with hypertension in Isfahan province. Ejadi et al. [17] investigated the level of health literacy in patients with angina pectoris disease referring to selected hospitals in Tehran using the HeLIA. Bahadori et al. [18] investigated the level of health literacy among hemodialysis patients.
Various studies have standardized this instrument in Iran, including the study by Zareban et al. [19], which was conducted on the urban population of the Baluchistan area. Haeri Mehrizi et al. [20] performed a confirmatory factor analysis for the HeLIA to ensure its validity further. This study examined data measuring health literacy among Iranian adults aged 18 to 65 years living in 31 provinces using the confirmatory factor analysis. Alijanzadeh et al. [21] reexamined the HeLIA constructs using a large and nearly representative sample in Qazvin province. They examined the psychometric properties, measurement invariance, and differential item functioning information of the HeLIA. Tavousi et al. [22] conducted a study to develop a short version of the HeLIA (HeLIA-SF). In this study, exploratory and confirmatory factor analysis was performed to assess structural validity. Also, the reliability of the instrument was evaluated by internal correlation (Cronbach's alpha coefficient) and intraclass correlation coefficient (ICC).
The results of a review study conducted by Mohamadloo et al. [23] have indicated that HeLIA is one of the most essential instruments for measuring health literacy in Iran. It has been employed in various communities, including patients, the elderly, students, etc. Additionally, Tavousi et al.'s study [24] revealed that among the 17 health literacy assessment tools developed in Iran, HeLIA has garnered more attention from researchers than others. However, while several studies have utilized the HeLIA instrument to measure health literacy in different patient groups, most investigations focusing on its standardization and structural re-evaluation have been conducted within the general population.
It appears that researchers have paid comparatively less attention to standardizing this tool for use within specific patient populations. Thalassemia major is one such condition that warrants special consideration. Thalassemia is a chronic genetic blood disorder that is inherited following genetic principles [25]. Approximately 1.5% of the world's population (80-90 million individuals) suffer from thalassemia major [26]. Each year, an estimated 60,000 to 70,000 infants are born with beta-thalassemia major worldwide [27]. The prevalence of this disease is higher in regions known as the "Thalassemia Belt," which includes the Mediterranean areas, parts of North and West Africa, the Middle East, the Indian subcontinent, and Southeast Asia. Iran, situated within this belt, also experiences a higher prevalence of thalassemia, particularly in the Northern provinces (Golestan and Mazandaran) and the southern regions of the country (Hormozgan and Khuzestan) [28].
There was no validation and adaptation of this test in major thalassemia patients in Iran. Therefore, the aim of this study was the validation and adaption of the HeLIA for measuring health literacy in thalassemia major patients in Iran. This research tried to take a small step toward improving their health status by standardizing health literacy measurement instruments for this special group.
Instrument and Methods
This is a cross-sectional study, and data collection was done from October to December 2022. The research population included patients with thalassemia major hospitalized at Shahid Baghaei 2 Hospital in Ahvaz. This hospital is the main for major thalassemia patients in Ahvaz. Based on the documents related to inpatients, the estimated number of the community was 300 people. According to Cochran's formula, the sample size was considered to be 170. This study used convenience sampling, and people's participation was voluntary. Considering that the Health Literacy Questionnaire is standardized in the age group of 18 to 65 years, the inclusion criteria were having major thalassemia, being hospitalized, and being in the age group of 18 to 65 years. Kaiser-Meyer-Olkin (KMO) is the measure of sampling adequacy. If the p-value is less than 0.05, the sample for factor analysis is adequate [29].
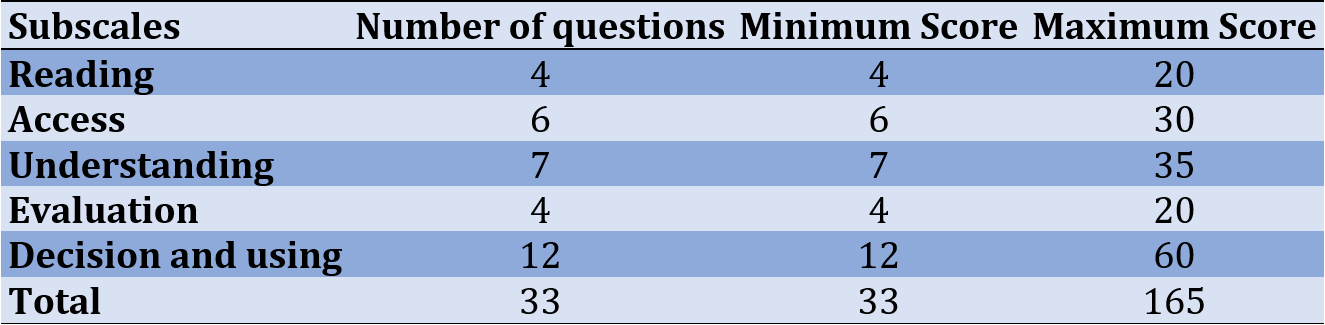
The questionnaire consisted of five subscales and 33 multiple-choice questions. Factor “Reading” consisted of four questions (1 to 4), “Access” consisted of six questions (5 to10), “Understanding” consisted of seven questions (11 to 17), “Evaluation” consisted of four questions (18 to 21) and “Decision and using” consisted of 12 questions (21 to 33). Questions were set as very hard, hard, moderate, easy, and very easy for questions 1 to 4, and never, rarely, sometimes, often, and always, for questions 5 to 33. Scoring was based on a Likert scale from 1 (very hard) to 5 (very easy), and 1 (never) to 5 (always). The raw score of each person in the subscales is obtained from the algebraic sum of the scores. Then, the following formula was used to convert this score to standard scores in the range of zero to 100:
Minimum raw score-raw score obtained/minimum score-maximum score×100
The total score was calculated by dividing the total scores of the subscales by the number of subscales. Table 1 shows minimum and maximum scores for all factors.
Table 1. Scoring of the HeLIA subscales
Content validity was assessed based on the opinions of ten experts by measuring content validity. Three response options were provided: "necessary," "useful but not necessary," and "not necessary." Experts were required to select one option for each question. To establish content validity, when the number of evaluators is at least ten, the minimum acceptable value of content validity ratio (CVR) should be 0.62 [30].
Regarding reliability, various indices, such as construct validity, Cronbach's Alpha, Kuder-Richardson reliability coefficient, and correlation coefficient can be employed [31]. Cronbach's alpha assesses the internal consistency of factors, with an alpha value of ≥0.7 indicating instrument validity [32]. The Kuder-Richardson (KR) test evaluates the consistency between questions, particularly in tests with true-false answers, by considering the ratio of correct to incorrect responses. It involves two formulas: KR 20 and KR 21, with a KR coefficient of ≥0.64 considered acceptable [34]. The correlation coefficient is utilized to assess test stability and can reveal correlations within clusters [35]. In this study, the Pearson correlation coefficient was used.
Explanatory factor analysis, employing principal component analysis (PCA) and varimax rotation, was utilized to establish construct validity. This analysis delved into the internal relationships among variables through principal component analysis, highlighting the classes of variables with the strongest associations with each other [32]. The analysis provided information on the total variance explained, and a model summary was presented. Additionally, an AMOS graph was employed to illustrate the relationships between factors and items. Model fit was assessed using several indices, including incremental fit index (IFI), comparative fit index (CFI), and normed fit index (NFI). Model fitness was deemed satisfactory if the IFI, CFI, and NFI values fell between 0 and 1, with values closer to 1 indicating a better fit [36]. The Root Mean Square Error of Approximation (RMSEA) was used to assess the goodness of fit for the model, with a value of RMSEA less than 0.1 indicating excellent model fitness [37]. Statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS) version 24 and Amos version 24.
Findings
Demographic Information
Most participants were in the age group of 18-28 (F=87, 51.2%) and 29-38 (F=67, 39.4%) years, female (F=108, 63.5%), single (F=134, 78.8%), jobless (F=129, 75.9%), and had a diploma (F=66, 38.8%). Most of them (F=107, 62.9%) acquire health information from doctors and the Internet (F=49, 28.8%).
Content Validity
Content validity was assessed through the input of 10 experts in health literacy from medical universities in Iran, and it was evaluated quantitatively. The CVR was employed to ensure the selection of the most important and appropriate items. The CVR value for the HeLIA test was calculated at 0.83, aligning with Lawshe's criteria, thus confirming content validity.
Key statistical indicators were examined, with a KMO value of 0.894, an approximate Chi-Square value of 3041.445, and a p-value of 0.001, demonstrating the validation of the test. In the exploratory factor analysis conducted with criteria such as Eigenvalue equal to or greater than one, absolute value of loading factor greater than or equal to 0.4, and Varimax rotation, the results revealed the presence of four factors. All items, with the exception of items 13 and 28, were grouped within these factors. The identified factors were as follows: Factor 1 - Understanding, Factor 2 - Reading, Access, and Evaluation, Factor 3 - Care Measures, and Factor 4 - Decision and Utilization.
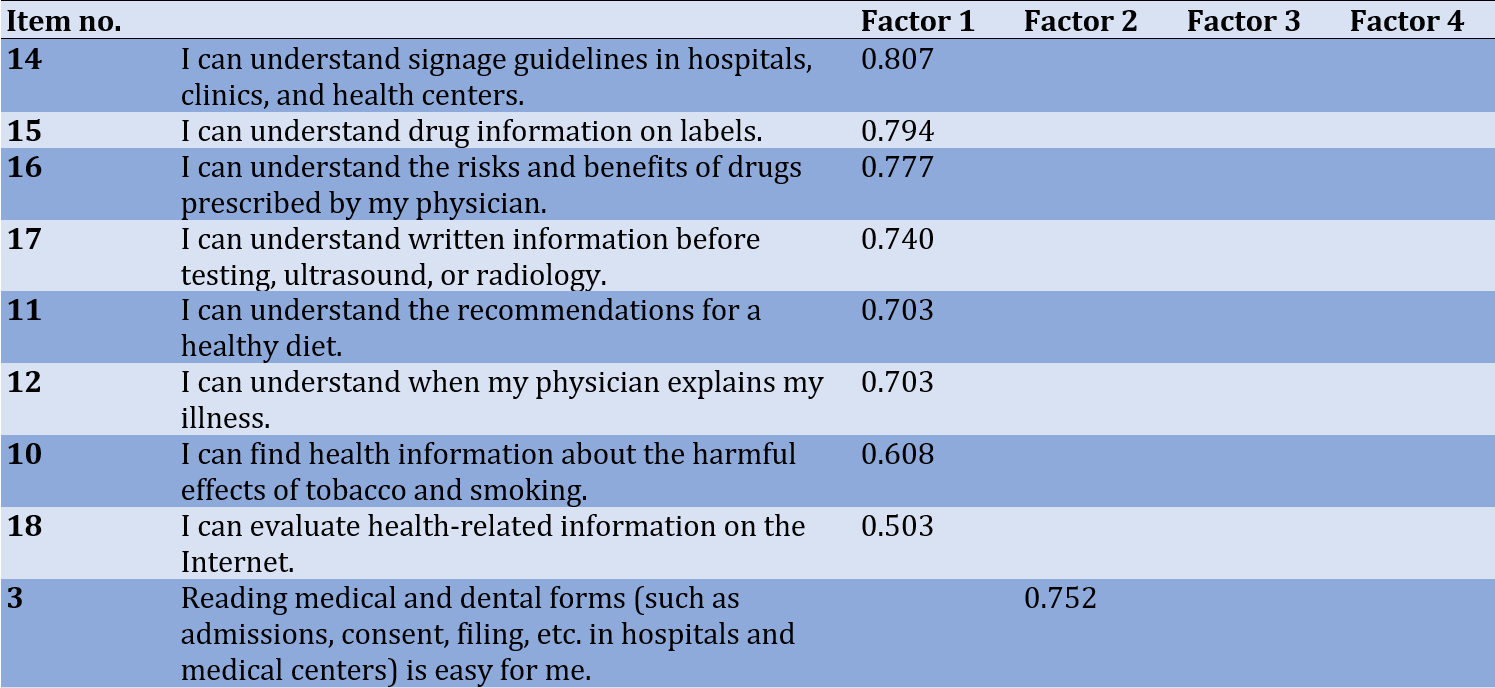
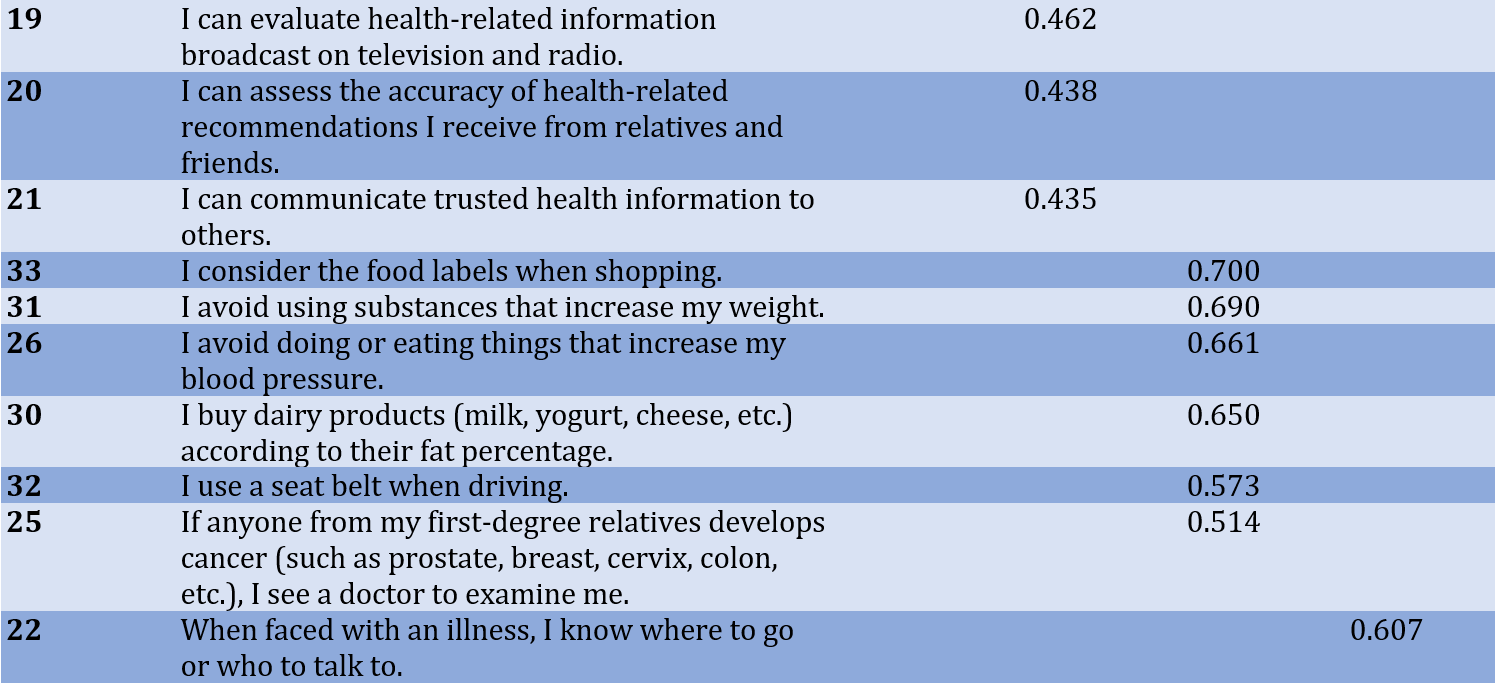
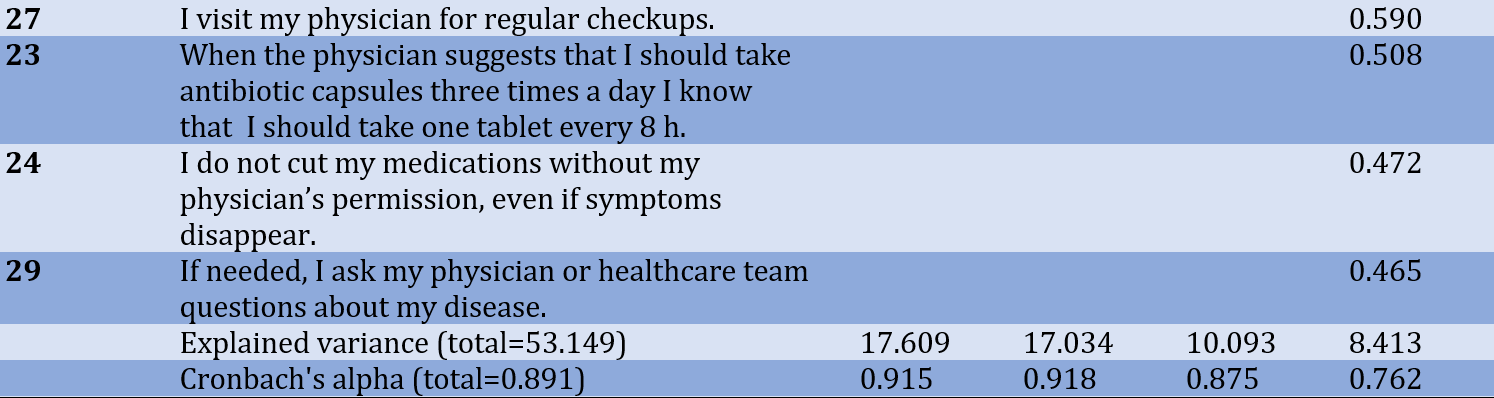
To assess the internal consistency of these factors, Cronbach's alpha was employed, yielding a value of 0.891, which confirms the test's validity. The HeLIA is considered a valid tool for examining health literacy in patients with Major Thalassemia and can account for 53.149 percent of the variance in health literacy. Detailed results of the exploratory factor analysis, Cronbach's alpha, and the explained variance can be found in Table 2.
Table 2. Exploratory factor analysis results, Cronbach`s alpha, and explained variance

The AMOS software was used to fit the conceptual model obtained from the analysis of exploratory factors. Figure 1 shows a graphic export for the model.
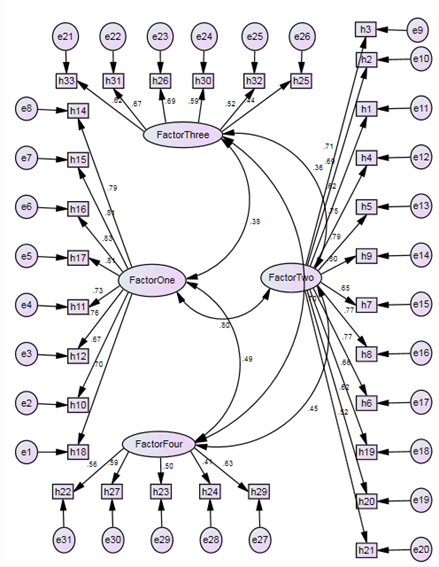
Figure 1. Graphic export for model (AMOS)
The model’s fitness was approved considering the following values: IFI=0.823, CFI=0.816, NFI=0.713 RMSEA=0.08, and the KR21=0.89 indicated the reliability of the test.
Also, the Pearson’s correlation coefficient showed significant correlations between all factors (Table 3).
Table 3. Pearson correlation coefficient results (p=0.000)

Discussion
Health literacy is a concept that is under investigation worldwide to understand and assess it across various segments of society. Consequently, a range of measurement tools, both native and non-native, have been developed and employed globally. In Iran, the HeLIA represents the first native instrument in this domain, created by Montazeri et al. [6] and subjected to psychometric testing among the urban population of Tehran. Given that the fundamental qualities of any scale are its reliability and validity, the primary objective of this study was to establish the validity and reliability of the HeLIA. This validation process aims to enable the use of this tool for assessing the health literacy status of patients with Major Thalassemia receiving care at Shahid Baghaei 2 Hospital in Ahvaz.
Prior to validation, the questionnaire was reviewed by 10 experts. Subsequently, the questionnaire was administered to 50 thalassemia major patients, who were not part of the primary research population, based on expert recommendations. Following this confirmation stage and to conduct post-validation, determining the validity and reliability of the instrument, the questionnaire was distributed among 170 patients. Form validity, content validity, and construct validity were all confirmed. The results of factor analysis revealed a model with four factors: "understanding," "reading, access, and evaluation," "care measures," and "decision and utilization." These factors collectively account for 53.149% of the variance in health literacy among thalassemia major patients.
The concept of understanding encompasses various aspects, including grasping the meaning and principles of signage guidelines within hospitals, clinics, and health centers. It involves paying close attention to drug information provided on labels and understanding both the benefits and potential risks associated with prescribed medications from healthcare professionals. Additionally, it entails comprehending written information before undergoing tests, such as ultrasounds or radiology scans, and heeding recommendations for a healthy diet. Understanding also involves comprehending explanations given by physicians regarding medical conditions and seeking out health information regarding the harmful effects of tobacco and smoking. Furthermore, it involves the ability to assess and evaluate health-related information found on the internet.
The factor of reading, access, and evaluation refers to items related to the ease of reading various documents, including medical and dental forms (such as patient admission forms and consent forms) in hospitals and health centers. It also involves understanding specific written instructions provided by physicians, dentists, and healthcare workers regarding medical conditions. Additionally, it includes the ease of reading educational materials about health, such as booklets, pamphlets, and brochures, as well as leaflets and instructions for laboratory tests, ultrasounds, or radiology procedures. The ability to obtain health information from different sources as needed is another component, covering various health issues such as high blood pressure, high blood sugar, and high lipid levels. Furthermore, it pertains to acquiring health information related to mental health concerns like depression and stress. The category also involves the capability to find health information about specific diseases when necessary, as well as seeking information about healthy eating habits. Lastly, it includes the capacity to evaluate the accuracy of health-related information presented on television and radio, as well as the ability to assess the reliability of health recommendations received from friends and family. Moreover, it involves the skill to communicate trustworthy health information to others.
The factor of "care measures" includes items, such as being mindful of food labels while shopping, avoiding substances that lead to weight gain, refraining from behaviors or foods that can raise blood pressure, and more. It also involves using a seat belt when driving and undergoing medical examinations if a first-degree relative is diagnosed with conditions, like prostate cancer, breast cancer, cervical cancer, colon cancer, and others.
The factor of "decision-making" pertains to knowing where to seek help and whom to consult when facing an illness. It includes regularly visiting the doctor for checkups and adhering to prescribed medication schedules, such as taking antibiotic capsules at eight-hour intervals, even if symptoms have improved. Additionally, it involves not discontinuing medications without the permission of a healthcare provider, even when symptoms have subsided. Lastly, it encourages patients to ask questions to their physicians and healthcare staff about their illnesses when necessary.
Liu et al. [38] conducted a systematic review assessing tools for measuring health literacy among the general population. They observed that most of the instruments employed a multidimensional approach to measure health literacy in the general population. These measurements primarily focused on individuals' abilities to obtain, understand, and process health-related information, along with their decision-making capabilities. These abilities were largely derived from the definition of health literacy, aligning with the findings of this study.
In another study, Haghdoost et al. [39] developed a valid and reliable native instrument for measuring health literacy in Iran. Their research identified several factors, including reading/comprehension skills, individual empowerment, communication/decision-making skills, social empowerment, and health knowledge. Some of these factors show compatibility with the results of this study. Notably, they identified seven factors in factor analysis, with the first factor (reading/comprehension skills) being particularly strong and accounting for 40% of the total variance.
Based on the indicators used, the four-factor model demonstrates a good fit. In the current research, health literacy in thalassemia major patients is examined based on the identified factors, including understanding, reading, access and evaluation, care measures, and decision-making and utilization. Health literacy can significantly contribute to enhancing the well-being of patients and individuals affected by facilitating the promotion of preventive measures, increasing awareness, and strengthening health-related indicators. Nevertheless, this study has its limitations. Given that the research was conducted among thalassemia major patients, caution should be exercised when generalizing the results to the entire population. It is recommended to validate other tools designed to assess health literacy in the thalassemia major patient population and compare their findings with those of the present study.
Conclusion
The HeLIA comprises five subscales and 33 multiple-choice questions. The tool's validity was established by identifying four factors and 31 questions relevant to thalassemia major patients. This tool is well-suited for assessing health literacy in thalassemia major patients, enabling the evaluation of their health literacy status and differentiation between patients with high health literacy scores and those with low scores. Helia was developed based on input from Iranian health researchers and citizens' feedback, making it culturally grounded and effective for measuring various facets of health literacy in Iran.
Acknowledgments: The authors wish to express their gratitude toward the Thalassemia & Hemoglobinopathy Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran, for funding this research.
Ethical Permissions: The ethical code IR.AJUMS.REC.1401.039 was received from the National Ethics Committee in Biological Research. The participants signed an oral consent form.
Conflicts of Interests: The authors declared no conflicts of interests.
Authors’ Contribution: Parsaei-Mohammadi P (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer (40%); Sabaghinejad Z (Second Author), Introduction Writer/Assistant Researcher/Discussion Writer/Statistical Analyst (40%); Ghaed-Amini Harouni Sh (Third Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%)
Funding/Support: the Thalassemia & Hemoglobinopathy Research center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran funded this research (Grant number: Th-0103).
The term "health literacy" was first used in 1974 to describe the impact of health information on the educational system, the healthcare system, and mass communication [1]. There are various definitions for this concept. One of the most well-known, provided by the World Health Organization, defines it as "Cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand, and use information in ways that promote and maintain good health" [2]. Ratzan and Parker [3] stated, "Health literacy is the capacity of people to obtain, process, and understand basic health information and services needed to make appropriate health care decisions." According to a report by the World Health Organization, health literacy has been identified as one of the main factors affecting health. The organization recommends that countries worldwide form health groups to educate and improve the level of health literacy in communities [4].
In the case of patients, the issue of health literacy becomes even more important. Studies have shown the influential role of health literacy on patient health outcomes. It is effective in increasing patient awareness, enhancing patients' ability to make informed decisions, reducing health-threatening risks, improving disease control and prevention, enhancing patient safety, improving quality of life and patient care, ensuring patients correctly understand education, and improving their health information [5-8].
Health literacy is a set of abilities, skills, and capacities in various dimensions. It includes the dimension of reading and accessing medical and health information, understanding and processing it, and the dimension of decision-making and application of this information. Considering the role of health literacy in improving the level of health of an individual and society, the existence of instruments that can measure health literacy is essential. Therefore, many instruments have been designed and used for measuring health literacy in different parts of the world, such as the Rapid Estimate of Adult Literacy in Medicine (REALM) [9], the Test of Functional Health Literacy in Adults (TOFHLA) [10], and Health Literacy Questionnaire (HLQ) [11]. In some countries, indigenous instruments have been developed to measure health literacy, such as the Korean Health Literacy Instrument (KHLI) [12], the Japanese Functional Health Literacy Test (JFHLT) [13], etc.
The Health Literacy Instrument for Adults (HeLIA) is a native instrument that is appropriate to cultural and social contexts designed to measure the health literacy of the general population aged 18 to 65 living in Iranian cities. The reliability and validity of this questionnaire were reported as appropriate in Iran by Montazeri et al. for the first time [6].
Some researchers used the HeLIA to investigate health literacy, including the study by Tavousi et al. [14], which was conducted on a sample of adults aged 18-65 In Iran. Some researchers used it in patients, including Sheikh Sharafi and Seyed Amini, [15] who evaluated health literacy in heart failure patients using the HeLIA. Chajaee et al. [16] investigated health literacy in patients with hypertension in Isfahan province. Ejadi et al. [17] investigated the level of health literacy in patients with angina pectoris disease referring to selected hospitals in Tehran using the HeLIA. Bahadori et al. [18] investigated the level of health literacy among hemodialysis patients.
Various studies have standardized this instrument in Iran, including the study by Zareban et al. [19], which was conducted on the urban population of the Baluchistan area. Haeri Mehrizi et al. [20] performed a confirmatory factor analysis for the HeLIA to ensure its validity further. This study examined data measuring health literacy among Iranian adults aged 18 to 65 years living in 31 provinces using the confirmatory factor analysis. Alijanzadeh et al. [21] reexamined the HeLIA constructs using a large and nearly representative sample in Qazvin province. They examined the psychometric properties, measurement invariance, and differential item functioning information of the HeLIA. Tavousi et al. [22] conducted a study to develop a short version of the HeLIA (HeLIA-SF). In this study, exploratory and confirmatory factor analysis was performed to assess structural validity. Also, the reliability of the instrument was evaluated by internal correlation (Cronbach's alpha coefficient) and intraclass correlation coefficient (ICC).
The results of a review study conducted by Mohamadloo et al. [23] have indicated that HeLIA is one of the most essential instruments for measuring health literacy in Iran. It has been employed in various communities, including patients, the elderly, students, etc. Additionally, Tavousi et al.'s study [24] revealed that among the 17 health literacy assessment tools developed in Iran, HeLIA has garnered more attention from researchers than others. However, while several studies have utilized the HeLIA instrument to measure health literacy in different patient groups, most investigations focusing on its standardization and structural re-evaluation have been conducted within the general population.
It appears that researchers have paid comparatively less attention to standardizing this tool for use within specific patient populations. Thalassemia major is one such condition that warrants special consideration. Thalassemia is a chronic genetic blood disorder that is inherited following genetic principles [25]. Approximately 1.5% of the world's population (80-90 million individuals) suffer from thalassemia major [26]. Each year, an estimated 60,000 to 70,000 infants are born with beta-thalassemia major worldwide [27]. The prevalence of this disease is higher in regions known as the "Thalassemia Belt," which includes the Mediterranean areas, parts of North and West Africa, the Middle East, the Indian subcontinent, and Southeast Asia. Iran, situated within this belt, also experiences a higher prevalence of thalassemia, particularly in the Northern provinces (Golestan and Mazandaran) and the southern regions of the country (Hormozgan and Khuzestan) [28].
There was no validation and adaptation of this test in major thalassemia patients in Iran. Therefore, the aim of this study was the validation and adaption of the HeLIA for measuring health literacy in thalassemia major patients in Iran. This research tried to take a small step toward improving their health status by standardizing health literacy measurement instruments for this special group.
Instrument and Methods
This is a cross-sectional study, and data collection was done from October to December 2022. The research population included patients with thalassemia major hospitalized at Shahid Baghaei 2 Hospital in Ahvaz. This hospital is the main for major thalassemia patients in Ahvaz. Based on the documents related to inpatients, the estimated number of the community was 300 people. According to Cochran's formula, the sample size was considered to be 170. This study used convenience sampling, and people's participation was voluntary. Considering that the Health Literacy Questionnaire is standardized in the age group of 18 to 65 years, the inclusion criteria were having major thalassemia, being hospitalized, and being in the age group of 18 to 65 years. Kaiser-Meyer-Olkin (KMO) is the measure of sampling adequacy. If the p-value is less than 0.05, the sample for factor analysis is adequate [29].
The questionnaire consisted of five subscales and 33 multiple-choice questions. Factor “Reading” consisted of four questions (1 to 4), “Access” consisted of six questions (5 to10), “Understanding” consisted of seven questions (11 to 17), “Evaluation” consisted of four questions (18 to 21) and “Decision and using” consisted of 12 questions (21 to 33). Questions were set as very hard, hard, moderate, easy, and very easy for questions 1 to 4, and never, rarely, sometimes, often, and always, for questions 5 to 33. Scoring was based on a Likert scale from 1 (very hard) to 5 (very easy), and 1 (never) to 5 (always). The raw score of each person in the subscales is obtained from the algebraic sum of the scores. Then, the following formula was used to convert this score to standard scores in the range of zero to 100:
Minimum raw score-raw score obtained/minimum score-maximum score×100
The total score was calculated by dividing the total scores of the subscales by the number of subscales. Table 1 shows minimum and maximum scores for all factors.
Table 1. Scoring of the HeLIA subscales
Content validity was assessed based on the opinions of ten experts by measuring content validity. Three response options were provided: "necessary," "useful but not necessary," and "not necessary." Experts were required to select one option for each question. To establish content validity, when the number of evaluators is at least ten, the minimum acceptable value of content validity ratio (CVR) should be 0.62 [30].
Regarding reliability, various indices, such as construct validity, Cronbach's Alpha, Kuder-Richardson reliability coefficient, and correlation coefficient can be employed [31]. Cronbach's alpha assesses the internal consistency of factors, with an alpha value of ≥0.7 indicating instrument validity [32]. The Kuder-Richardson (KR) test evaluates the consistency between questions, particularly in tests with true-false answers, by considering the ratio of correct to incorrect responses. It involves two formulas: KR 20 and KR 21, with a KR coefficient of ≥0.64 considered acceptable [34]. The correlation coefficient is utilized to assess test stability and can reveal correlations within clusters [35]. In this study, the Pearson correlation coefficient was used.
Explanatory factor analysis, employing principal component analysis (PCA) and varimax rotation, was utilized to establish construct validity. This analysis delved into the internal relationships among variables through principal component analysis, highlighting the classes of variables with the strongest associations with each other [32]. The analysis provided information on the total variance explained, and a model summary was presented. Additionally, an AMOS graph was employed to illustrate the relationships between factors and items. Model fit was assessed using several indices, including incremental fit index (IFI), comparative fit index (CFI), and normed fit index (NFI). Model fitness was deemed satisfactory if the IFI, CFI, and NFI values fell between 0 and 1, with values closer to 1 indicating a better fit [36]. The Root Mean Square Error of Approximation (RMSEA) was used to assess the goodness of fit for the model, with a value of RMSEA less than 0.1 indicating excellent model fitness [37]. Statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS) version 24 and Amos version 24.
Findings
Demographic Information
Most participants were in the age group of 18-28 (F=87, 51.2%) and 29-38 (F=67, 39.4%) years, female (F=108, 63.5%), single (F=134, 78.8%), jobless (F=129, 75.9%), and had a diploma (F=66, 38.8%). Most of them (F=107, 62.9%) acquire health information from doctors and the Internet (F=49, 28.8%).
Content Validity
Content validity was assessed through the input of 10 experts in health literacy from medical universities in Iran, and it was evaluated quantitatively. The CVR was employed to ensure the selection of the most important and appropriate items. The CVR value for the HeLIA test was calculated at 0.83, aligning with Lawshe's criteria, thus confirming content validity.
Key statistical indicators were examined, with a KMO value of 0.894, an approximate Chi-Square value of 3041.445, and a p-value of 0.001, demonstrating the validation of the test. In the exploratory factor analysis conducted with criteria such as Eigenvalue equal to or greater than one, absolute value of loading factor greater than or equal to 0.4, and Varimax rotation, the results revealed the presence of four factors. All items, with the exception of items 13 and 28, were grouped within these factors. The identified factors were as follows: Factor 1 - Understanding, Factor 2 - Reading, Access, and Evaluation, Factor 3 - Care Measures, and Factor 4 - Decision and Utilization.
To assess the internal consistency of these factors, Cronbach's alpha was employed, yielding a value of 0.891, which confirms the test's validity. The HeLIA is considered a valid tool for examining health literacy in patients with Major Thalassemia and can account for 53.149 percent of the variance in health literacy. Detailed results of the exploratory factor analysis, Cronbach's alpha, and the explained variance can be found in Table 2.
Table 2. Exploratory factor analysis results, Cronbach`s alpha, and explained variance
The AMOS software was used to fit the conceptual model obtained from the analysis of exploratory factors. Figure 1 shows a graphic export for the model.
Figure 1. Graphic export for model (AMOS)
The model’s fitness was approved considering the following values: IFI=0.823, CFI=0.816, NFI=0.713 RMSEA=0.08, and the KR21=0.89 indicated the reliability of the test.
Also, the Pearson’s correlation coefficient showed significant correlations between all factors (Table 3).
Table 3. Pearson correlation coefficient results (p=0.000)
Discussion
Health literacy is a concept that is under investigation worldwide to understand and assess it across various segments of society. Consequently, a range of measurement tools, both native and non-native, have been developed and employed globally. In Iran, the HeLIA represents the first native instrument in this domain, created by Montazeri et al. [6] and subjected to psychometric testing among the urban population of Tehran. Given that the fundamental qualities of any scale are its reliability and validity, the primary objective of this study was to establish the validity and reliability of the HeLIA. This validation process aims to enable the use of this tool for assessing the health literacy status of patients with Major Thalassemia receiving care at Shahid Baghaei 2 Hospital in Ahvaz.
Prior to validation, the questionnaire was reviewed by 10 experts. Subsequently, the questionnaire was administered to 50 thalassemia major patients, who were not part of the primary research population, based on expert recommendations. Following this confirmation stage and to conduct post-validation, determining the validity and reliability of the instrument, the questionnaire was distributed among 170 patients. Form validity, content validity, and construct validity were all confirmed. The results of factor analysis revealed a model with four factors: "understanding," "reading, access, and evaluation," "care measures," and "decision and utilization." These factors collectively account for 53.149% of the variance in health literacy among thalassemia major patients.
The concept of understanding encompasses various aspects, including grasping the meaning and principles of signage guidelines within hospitals, clinics, and health centers. It involves paying close attention to drug information provided on labels and understanding both the benefits and potential risks associated with prescribed medications from healthcare professionals. Additionally, it entails comprehending written information before undergoing tests, such as ultrasounds or radiology scans, and heeding recommendations for a healthy diet. Understanding also involves comprehending explanations given by physicians regarding medical conditions and seeking out health information regarding the harmful effects of tobacco and smoking. Furthermore, it involves the ability to assess and evaluate health-related information found on the internet.
The factor of reading, access, and evaluation refers to items related to the ease of reading various documents, including medical and dental forms (such as patient admission forms and consent forms) in hospitals and health centers. It also involves understanding specific written instructions provided by physicians, dentists, and healthcare workers regarding medical conditions. Additionally, it includes the ease of reading educational materials about health, such as booklets, pamphlets, and brochures, as well as leaflets and instructions for laboratory tests, ultrasounds, or radiology procedures. The ability to obtain health information from different sources as needed is another component, covering various health issues such as high blood pressure, high blood sugar, and high lipid levels. Furthermore, it pertains to acquiring health information related to mental health concerns like depression and stress. The category also involves the capability to find health information about specific diseases when necessary, as well as seeking information about healthy eating habits. Lastly, it includes the capacity to evaluate the accuracy of health-related information presented on television and radio, as well as the ability to assess the reliability of health recommendations received from friends and family. Moreover, it involves the skill to communicate trustworthy health information to others.
The factor of "care measures" includes items, such as being mindful of food labels while shopping, avoiding substances that lead to weight gain, refraining from behaviors or foods that can raise blood pressure, and more. It also involves using a seat belt when driving and undergoing medical examinations if a first-degree relative is diagnosed with conditions, like prostate cancer, breast cancer, cervical cancer, colon cancer, and others.
The factor of "decision-making" pertains to knowing where to seek help and whom to consult when facing an illness. It includes regularly visiting the doctor for checkups and adhering to prescribed medication schedules, such as taking antibiotic capsules at eight-hour intervals, even if symptoms have improved. Additionally, it involves not discontinuing medications without the permission of a healthcare provider, even when symptoms have subsided. Lastly, it encourages patients to ask questions to their physicians and healthcare staff about their illnesses when necessary.
Liu et al. [38] conducted a systematic review assessing tools for measuring health literacy among the general population. They observed that most of the instruments employed a multidimensional approach to measure health literacy in the general population. These measurements primarily focused on individuals' abilities to obtain, understand, and process health-related information, along with their decision-making capabilities. These abilities were largely derived from the definition of health literacy, aligning with the findings of this study.
In another study, Haghdoost et al. [39] developed a valid and reliable native instrument for measuring health literacy in Iran. Their research identified several factors, including reading/comprehension skills, individual empowerment, communication/decision-making skills, social empowerment, and health knowledge. Some of these factors show compatibility with the results of this study. Notably, they identified seven factors in factor analysis, with the first factor (reading/comprehension skills) being particularly strong and accounting for 40% of the total variance.
Based on the indicators used, the four-factor model demonstrates a good fit. In the current research, health literacy in thalassemia major patients is examined based on the identified factors, including understanding, reading, access and evaluation, care measures, and decision-making and utilization. Health literacy can significantly contribute to enhancing the well-being of patients and individuals affected by facilitating the promotion of preventive measures, increasing awareness, and strengthening health-related indicators. Nevertheless, this study has its limitations. Given that the research was conducted among thalassemia major patients, caution should be exercised when generalizing the results to the entire population. It is recommended to validate other tools designed to assess health literacy in the thalassemia major patient population and compare their findings with those of the present study.
Conclusion
The HeLIA comprises five subscales and 33 multiple-choice questions. The tool's validity was established by identifying four factors and 31 questions relevant to thalassemia major patients. This tool is well-suited for assessing health literacy in thalassemia major patients, enabling the evaluation of their health literacy status and differentiation between patients with high health literacy scores and those with low scores. Helia was developed based on input from Iranian health researchers and citizens' feedback, making it culturally grounded and effective for measuring various facets of health literacy in Iran.
Acknowledgments: The authors wish to express their gratitude toward the Thalassemia & Hemoglobinopathy Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran, for funding this research.
Ethical Permissions: The ethical code IR.AJUMS.REC.1401.039 was received from the National Ethics Committee in Biological Research. The participants signed an oral consent form.
Conflicts of Interests: The authors declared no conflicts of interests.
Authors’ Contribution: Parsaei-Mohammadi P (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer (40%); Sabaghinejad Z (Second Author), Introduction Writer/Assistant Researcher/Discussion Writer/Statistical Analyst (40%); Ghaed-Amini Harouni Sh (Third Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%)
Funding/Support: the Thalassemia & Hemoglobinopathy Research center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran funded this research (Grant number: Th-0103).
Article Type: Descriptive & Survey |
Subject:
Health Literacy
Received: 2023/10/17 | Accepted: 2023/11/18 | Published: 2023/12/25
Received: 2023/10/17 | Accepted: 2023/11/18 | Published: 2023/12/25
References
1. Parnell TA. Health literacy: History, definitions, and models. Health literacy in nursing: Providing person-centered care. New York: Springer Publishing Company; 2014. pp. 3-2. [Link] [DOI:10.1891/9780826161734]
2. World Health Organization. Division of Health Promotion. Education and Communications Health Education and Health Promotion Unit, Health Promotion Glossary. Geneva: WHO; 1998. [Link]
3. Ratzan SC, Parker RM. Health literacy-identification and response. J Health Commun. 2006;11(8):713-5. [Link] [DOI:10.1080/10810730601031090]
4. World Health Organization. Closing the gap in a generation: health equity through action on the social determinants of health: Commission on Social Determinants of Health final report. Geneva: WHO; 2008. [Link]
5. Paasche‐Orlow MK, Parker RM, Gazmararian JA, Nielsen‐Bohlman LT, Rudd RR. The prevalence of limited health literacy. J Gen Intern Med. 2005;20(2):175-84. [Link] [DOI:10.1111/j.1525-1497.2005.40245.x]
6. Montazeri A, Tavousi M, Rakhshani F,Azin SA, Jahangiri K, Ebadi M, et al. Health literacy for Iranian adults (HeLIA): Development and psychometric properties. Payesh 2014;13(5):589-99. [Persian] [Link]
7. Kountz DS. Strategies for improving low health literacy. Postgrad Med. 2009;121(5):171-7. [Link] [DOI:10.3810/pgm.2009.09.2065]
8. Kaphingst KA, Kreuter MW, Casey C, Leme L, Thompson T, Cheng MR, et al. Health literacy INDEX: Development, reliability, and validity of a new tool for evaluating the health literacy demands of health information materials. J Health Commun. 2012;17(Suppl 3):203-21. [Link] [DOI:10.1080/10810730.2012.712612]
9. Davis TC, Long SW, Jackson RH, Mayeaux EJ, George RB, Murphy PW, et al. Rapid estimate of adult literacy in medicine: A shortened screening instrument. Fam Med. 1993;25(6):391-5. [Link]
10. Parker RM, Baker DW, Williams MV, Nurss JR. The test of functional health literacy in adults: A new instrument for measuring patients' literacy skills. J Gen Intern Med. 1995;10:537-41. [Link] [DOI:10.1007/BF02640361]
11. Osborne RH, Batterham RW, Elsworth GR, Hawkins M, Buchbinder R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health. 2013;13:658. [Link] [DOI:10.1186/1471-2458-13-658]
12. Kang SJ, Lee TW, Paasche-Orlow MK, Kim GS, Won HK. Development and evaluation of the Korean health literacy instrument. J Health Commun. 2014;19(Suppl 2):254-66. [Link] [DOI:10.1080/10810730.2014.946113]
13. Nakagami K, Yamauchi T, Noguchi H, Maeda T, Nakagami T. Development and validation of a new instrument for testing functional health literacy in J apanese adults. Nurs Health Sci. 2014;16(2):201-8. [Link] [DOI:10.1111/nhs.12087]
14. Tavousi M, Haeri Mehrizi AA, Rafiefar S, Solimanian A, Sarbandi F, Ardestani M, et al. Health literacy in Iran: Findings from a national study. Payesh 2016;15(1):95-102. [Persian] [Link]
15. Sheikh Sharafi H, Seyed Amini B. Assessment of health literacy and self-care in heart failure patients. J Health Lit. 2017;1(4):203-19. [Link]
16. Chajaee F, Pirzadeh A, Hasanzadeh A, Mostafavi F. Relationship between health literacy and knowledge among patients with hypertension in Isfahan province, Iran. Electron Physician. 2018;10(3):6470. [Link] [DOI:10.19082/6470]
17. Ejadi A, Javanmardnejad S, Rejeh N, Heravi-Karimooi M, Tadrisi SD. Health Literacy in patients with angina pectoris disease referred to selected hospitals in of Tehran. J Health Lit. 2020;5(2):21-8. [Link]
18. Bahadori M, Najari F, Alimohammadzadeh K. The relationship between health literacy and general health level of hemodialysis patients: A case study in Iran. Nephrourol Mon. 2018;10(3):e66034. [Link] [DOI:10.5812/numonthly.66034]
19. Zareban I, Izadirad H, Araban M. Psychometric evaluation of health literacy for adults (Helia) in Urban area of balochistan. Payesh. 2016;15(6):669-76. [Persian] [Link]
20. Haeri Mehrizi AA, Tavousi M, Rafieifar S, Soleimanian A, Sarbandi F, Ardestani MS, et al. Health literacy for Iranian adults (HeLIA): The confirmatory factor analysis. Payesh 2016;15(3):251-7. [Persian] [Link]
21. Alijanzadeh M, Lin CY, Yahaghi R, Rahmani J, Yazdi N, Jafari E, et al. Measurement invariance and differential item functioning of the health literacy instrument for adults (HeLIA): A large-scale cross-sectional study in Iran. Healthcare. 2022;10(10):2064. [Link] [DOI:10.3390/healthcare10102064]
22. Tavousi M, Haeri-Mehrizi AA, Sedighi J, Montazeri A, Mohammadi S, Ardestani MS. Health Literacy Instrument for Adults-Short Form (HeLIA-SF): Development and psychometric properties. Payesh. 2022;21(3):309-10. [Persian] [Link]
23. Mohamadloo A, Batooli Z, Ramezankhani A. The analysis and review of the literatures in the field of health literacy. Mod Med Inform Sci. 2020;6:58-72. [Persian] [Link] [DOI:10.29252/jmis.6.2.58]
24. Tavousi M, Sedighi J, Montazeri A, Zarei F, Mozafari kermani R, Rostami R, et al. Psychometric properties of health literacy measures in Persian biomedical literature: A systematic review. Payesh. 2021;20(6):773-85. [Link] [DOI:10.52547/payesh.20.6.773]
25. khani H, Majdi MR, Montazeri A, Hoseini SH, Ghorbani A, Ramezani M, et al. Mental health status of beta-thalassemia major in Mazandaran province in 2006. J Fundamentals Ment Health, 2007;9(36):55-65. [Persian] [Link]
26. Ebrahimi Rigi H, Ebrahimi Rigi Z, Abdollahi Mohammad A, Borhanzehi K. Investigate the relationship between therapeutic indicators and quality of life in children aged 8-12 years with thalassemia major in Iranshahr, 2017. J Nurs Educ. 2020;9(3):33-42. [Persian] [Link]
27. Al-Nuaimi MA, AL-Hially YA, AL-Hafidh N. β thalassemia major patients profile in Ninevah governorate-Iraq. Tikrit Med J. 2012;18(2):250-60. [Link]
28. Shiva A, Kalavi M, Pakravan A, Yazdani J, Karami H. Dental treatment needs in thalassemia major patients, Sari, Iran. J Mazandaran Univ Med Sci. 2019;29(179):126-33. [Link]
29. Williams B, Onsman A, Brown T. Exploratory factor analysis: A five-step guide for novices. Australasian J Paramed. 2010;8(3). [Link] [DOI:10.33151/ajp.8.3.93]
30. Lawshe C. A qualitative approach to content validity. Personnel Psychol. 1975;28(4):563-75. [Link] [DOI:10.1111/j.1744-6570.1975.tb01393.x]
31. Mohammadbeigi A, Mohammadsalehi N, Aligol M. Validity and reliability of the instruments and types of measurments in health applied researches. RUMS J. 2015;13(12):1153-70. [Persian] [Link]
32. Helms JE, Henze KT, Sass TL, Mifsud VA. Treating Cronbach's alpha reliability coefficients as data in counseling research. Counsel Psychologist. 2006;34(5):630-60. [Link] [DOI:10.1177/0011000006288308]
33. Cook DA, Beckman TJ. Current concepts in validity and reliability for psychometric instruments: theory and application. Am J Med. 2006;119(2):166.e7-16. [Link] [DOI:10.1016/j.amjmed.2005.10.036]
34. Seif AA. Evaluation and assessment of educational progeression. Tehran: Agah Publication; 1992. [Link]
35. Kristof W. The statistical theory of stepped-up reliability coefficients when a test has been divided into several equivalent parts. Psychometrika. 1963;28(3):221-38. [Link] [DOI:10.1007/BF02289571]
36. Habibi M. Structural equation modeling and scientific analysis. Iran: Jahad-e-Daneshgahi Publication; 2017. [Link]
37. MacCallum RC, Browne MW, Sugawara HM. Power analysis and determination of sample size for covariance structure modeling. Psychological Methods. 1996;1(2):130-49. [Link] [DOI:10.1037/1082-989X.1.2.130]
38. Liu H, Zeng H, Shen Y, Zhang F, Sharma M, Lai W, et al. Assessment tools for health literacy among the general population: A systematic review. Int J Environ Res Public Health. 2018;15(8):1711. [Link] [DOI:10.3390/ijerph15081711]
39. Haghdoost AA, Rakhshani F, Aarabi M, Montazeri A, Tavousi M, Solimanian A, et al. Iranian health literacy questionnaire (IHLQ): An instrument for measuring health literacy in Iran. Iran Red Crescent Med J. 2015;17(6):e25831. [Link] [DOI:10.5812/ircmj.17(6)2015.25831]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |