



Volume 11, Issue 2 (2023)
Health Educ Health Promot 2023, 11(2): 311-316 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hatefnia E, Kimiafar M, Moghimbeigi A, Safari-Moradabadi A. Factors Predicting Physical Activity Behaviors related to hypertension in overweight male employees: Application of Health Belief Model. Health Educ Health Promot 2023; 11 (2) :311-316
URL: http://hehp.modares.ac.ir/article-5-68475-en.html
URL: http://hehp.modares.ac.ir/article-5-68475-en.html
1- Social Determinants of Health Research Center, Alborz University of Medical Sciences, Alborz, Iran
2- Department of Health Promotion and Education, School of Health, Alborz University of Medical Sciences, Alborz, Iran
3- “Research Center for Health, Safety and Environment” and “Department of Epidemiology and Biostatistics, School of Health”, Alborz University of Medical Sciences, Alborz, Iran
2- Department of Health Promotion and Education, School of Health, Alborz University of Medical Sciences, Alborz, Iran
3- “Research Center for Health, Safety and Environment” and “Department of Epidemiology and Biostatistics, School of Health”, Alborz University of Medical Sciences, Alborz, Iran
Full-Text [PDF 887 kb]
(3303 Downloads)
| Abstract (HTML) (1883 Views)
Full-Text: (600 Views)
Introduction
Hypertension is one of the most common risk factors for cardiovascular diseases (CVD) and a major global health threat afflicting one billion people worldwide [1]. Hypertension and its complications account for 9.4 million mortalities worldwide every year. It is estimated that the number of hypertension patients will increase to 1.56 billion worldwide by 2025 [2]. The global burden of disease study shows that systolic blood pressure accounts for the largest proportion of life (in years) lost due to premature death, accounting for 212 million years of life lost [3].
Except for some genetic factors that indicate a family history of high blood pressure, factors, such as overweight, high-salt diet, stress and anxiety, consumption of alcoholic beverages, and inactivity cause high blood pressure [4]. Physical inactivity is responsible for a large proportion of coronary heart disease, type II diabetes, and hypertension [5, 6, 7]. Unfortunately, advanced technology and mechanized life have reduced the rate of physical activity among people, and the adverse effects of this are quite evident [8]. The World Health Organization (WHO) reports the prevalence of physical inactivity to be more than 80% in adults and 23% in adolescents [9]. Surveys conducted in Iran show that 70 to 80% of Iranian society has not enough physical activity [10, 11]. On the other hand, employees include the highest proportion of sedentary people in Iranian society [12, 13]. The recently published WHO recommendations on physical activity state that all adults (18-64 years) should engage in 150-300 min of moderate-intensity, or 75-150 min of vigorous-intensity physical activity, or an equivalent combination of moderate- and vigorous-intensity activity throughout the week [14].
Exploring people's perceptions and health beliefs about physical activity may be useful for planning and implementing appropriate interventions thereby reducing the prevalence of hypertension. There are several patterns and models for identifying these effective factors that can be used to predict the foremost influential factors in effective health behaviors, of which the health belief model (HBM) is widely used as a basis for planning health education programs to promote adherence to preventive measures. This model points to the importance of individuals’ opinions about health and the perceived benefits and barriers to preventive and protective behavior. This model can be used to investigate the beliefs, values, and attitudes that underlie behavior because it consists of constructs that account for the important aspects of behavior change (Figure 1) [15].

Figure 1) Conceptual framework of health belief model.
Healthy behaviors are very important to prevent high blood pressure, which is the cause of cardiovascular diseases and diabetes. Considering the importance of men's health in economic performance and the role of family management, and due to the prevalence of overweight or obesity and its relationship with high blood pressure, awareness of men's beliefs and behavior in this field can be used in planning educational interventions to improve men's health. Therefore, the present study aimed to investigate health beliefs, physical activity, and the prevention of hypertension in overweight male employees.
Instrument and Methods
Study Design
The present descriptive-analytical cross-sectional study was done on overweight and obese male employees working in the Urmia offices between November and March 2021.
Sample size and method
The sample size was estimated to be 467 cases based on a formula and consultation with a statistician, considering a confidence level of 95% and a test power of 80%. The sampling procedure was as follows: first, all the offices in Urmia city were identified (19 cases) and then, a sample of 25 offices, which met the inclusion criteria were selected as a cluster for random selection of participants.
Inclusion and exclusion criteria
The inclusion criteria were overweight and obesity (based on body mass index (BMI)) and working in the Urmia offices. The exclusion criterion was incomplete questionnaires (failure to answer more than five questions). To meet the inclusion criteria (overweight and obesity), male employees were weighed, wearing light clothes and no shoes. To this aim, a standard scale (digital scale made in Germany with an accuracy of 0.1 kg) was used. The validity of the scale was checked with a control weight of 5 kg. Body height was also measured in a standing position using a standard caliper with an accuracy of 0.1 cm. The accuracy of the scale was also checked with a standard measurement scale of 100 cm long. Participants with a BMI≥25 were included in the study.
Data collection instrument
The instrument used to collect the required data was a researcher-made questionnaire in four sections. The first part contained demographic information, including age, education level, occupation, family income, and number of children.
The second part included ten questions exploring knowledge about physical activity and blood pressure (e.g., physical activity can prevent hypertension by controlling weight). In this section, a score of one was awarded for a correct answer and a score of zero for an incorrect answer or "I don't know", with a higher score indicating a higher level of knowledge.
The third part included the HBM constructs. Five questions enquired about perceived susceptibility (e.g., my chances of getting hypertension are high), four questions explored perceived severity (e.g., blood pressure can lead to death), five questions explored perceived benefits (e.g., I can get rid of my hypertension if I exercise properly), five questions addressed perceived barriers (e.g., I am too busy and hardly find time for physical activity), and three questions dealt with perceived self-efficacy (e.g., I can exercise every day to gain the right weight).
The fourth part consisted of questions about physical activity collected via the short form of the International Physical Activity Questionnaire (IPAQ) [16]. This questionnaire contained seven questions about intense and moderate physical activity, walking, and sedentary life in the past seven days.
Instrument validation
The content validity index (CVI) and the content validity ratio as well as experts’ commentaries (n=8) were used to validate the instrument. A test-retest method was used at two-week intervals to substantiate the reliability of the instrument. Cronbach's alpha value was higher than 0.7 for all parts.
Data analysis
Data analysis was done by SPSS 18 using descriptive and inferential statistics. Frequency and percentage were used to describe qualitative data and mean and standard deviation were used to describe quantitative data. The normality of data was assessed using the Kolmogorov-Smirnov test. As the normality of data was not confirmed, only standard nonparametric statistical tests were used to test the relationships or differences between quantitative variables. To explore the frequency of data, the Chi-square test was used. To test the between-group mean difference in physical activity and lack of physical activity, the Mann-Whitney U test was used. To assess the difference of three or more mean scores between the two groups, the Kruskal-Wallis test was applied. Pearson’s correlation coefficient was used to test the correlation between quantitative variables.
Findings
The participants’ age range was 28 to 57 years, with an average of 42.54 years. The highest percentage of the participants belonged to the age group of 28 to 38 years. All participants had a university degree, 83% were married, and 46% had an income less than $ 400 (Table 1).
Table 1) Participants’ socio-demographic variables and their correlation with physical activity

Table 2 shows the mean scores of knowledge and HBM constructs in the two groups. There were statistically significant between-group differences in the mean scores of perceived susceptibility, perceived severity, perceived barriers, and self-efficacy in physical activity (p<0.05).
Table2) Comparison of the mean scores of knowledge and health belief model (HBM) constructs in groups with and without physical activity

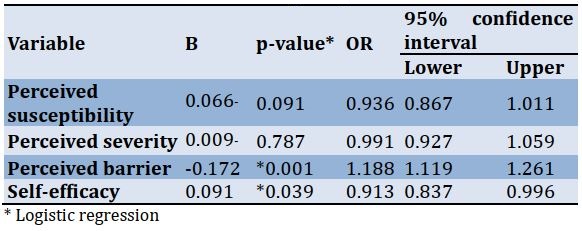
Pearson’s correlation coefficient results showed only a significant correlation between knowledge and perceived severity (r=0.095, p=0.04). No statistically significant correlation was found between knowledge and other HBM constructs. Table 3 indicates the predictors of physical activity measured using a logistic regression analysis. Self-efficacy and perceived barriers were found as predictors of physical activity. Thus, an increase in self-efficacy was followed by an increase in the probability of increasing physical activity to 0.91, and an increase in barriers to physical activity resulted in a 1.18% decrease in physical activity.
Table 3) Predictors of adopting preventive hypertension behavior based on the health belief model (HBM)
Discussion
The present study explored physical activity perceptions and behaviors to reduce the risk of hypertension in overweight male employees. The results showed that 25.1% of male employees had normal physical activity. The present findings are consistent with the findings reported by Bish et al. [17] but not those reported by Yahia et al. [18]. This difference could be related to the younger age of the students compared to the employees or the inherent differences in their profession.
The results of the present research showed no statistically significant difference between the two groups with and without physical activity in terms of the mean score of knowledge about the behavior to prevent hypertension. Both groups had the same level of knowledge about the topic. This result shows that knowledge alone is not sufficient to control health risk factors or adopt health-promoting behaviors. Although knowledge is an important determinant of behavior or lifestyle change, there may be other factors that play an important role in the transfer of knowledge into practice [19]. Al-Deagi et al. reported that participants had poor adherence despite sufficient knowledge about health care services and acquiring knowledge about diabetes was not sufficient to increase adherence to diabetes care [20].
Other researchers found that people's health-related behaviors require a minimum level of knowledge and motivation, and higher levels of knowledge about the disease lead to better self-care and adherence to medication or management. However, there is an inconsistency between knowledge of the disease and adherence to medication and disease management, and there is a mismatch between patient knowledge and behavior and participants were not acting on their knowledge. This noncompliance may be due to emotional, social, biological, and cultural factors that play a role in the adoption or non-adoption of the behavior [21, 22].
Aubert et al. investigated individuals’ knowledge, attitudes, and behaviors regarding hypertension. They found that most people had sufficient knowledge about hypertension, but few were sufficiently motivated and made efforts to change their behavior [23].
The results are also consistent with the findings of Imanipour et al. [24], who found no statistically significant correlation between knowledge and behavior for the prevention of CVDs. However, this was in contrast to the results of Baghianimoghadam et al. [25], who found a statistically significant relationship between knowledge and preventive behavior in CVDs. The present findings about the role of male employees’ health beliefs in the effect of physical activity on preventing hypertension showed a statistically significant difference between the perceived susceptibility of the groups with and without physical activity. The mean perceived susceptibility score was higher in men with physical activity than in men without, indicating that they are susceptible to hypertension and feel more at risk of developing hypertension. This result is consistent with that of Rahmati et al. on AIDS prevention behavior [26] and Morowaty et al. [27] on diabetes self-care behavior. These studies showed a statistically significant relationship between susceptibility and preventive behavior. These were, however, in contrast to the results of Baghianimoghadam et al. and Mahmoodabad and Tanekaboni [25, 28].
As the present study revealed, a statistically significant difference was found between the mean perceived severity scores of the two groups. Overweight male employees who did standard regular physical activities had a higher mean score of perceived severity than overweight male employees who did not. The present findings are consistent with the results of Mahmoodabad and Tanekaboni [28] and in contrast to the findings reported by Aligol et al. [29]. According to the mean perceived severity score and the fact that the symptoms of hypertension develop gradually in the long run, male employees may not have a high perceived severity, which should be considered in educational interventions to raise awareness of the significance of this issue.
There was a statistically significant difference in the mean perceived barriers score of the two groups, pointing to the importance of perceived barriers to physical activity, which is consistent with the findings reported by Baghianimoghadam et al. Mazloomy et al., and Jorvand et al. [25, 30, 31].
A statistically significant difference was found between overweight male employees who exercised regularly and those who did not in terms of the mean perceived self-efficacy of hypertension preventive behaviors. It means that the group with physical activity had a higher mean self-efficacy score. Given that self-efficacy has been cited as a predictor of behavior in most studies, its inclusion in educational interventions may play a critical role in changing or forming behavior. The findings related to self-efficacy are consistent with those reported by Kang et al. [32], Elwesif et al., and McElfish et al. [33, 34], yet contrast with the findings reported by Rahmati-Najarkolaei et al. [35].
The results of the regression analysis showed that self-efficacy was a significant predictor of physical activity in overweight male employees, pointing to the significance of self-efficacy to show healthy behaviors, and interventions to change physical activity should consider education to increase self-efficacy. These findings are consistent with the results of McElfishet al., showing that self-efficacy is a significant predictor of physical activity in obese and overweight adults [34].
Another significant predictor of physical activity was perceived barriers, which points to the importance of this construct (e.g., not having enough time to do physical activity and failure to perceive the real importance of physical activity) in doing physical activity. Lack of time was a barrier found for most employees. Policy making for regular physical activities in the workplace can lead to an increase in physical activity among male employees. The above-mentioned result is consistent with the findings reported by Rahmati-Najarkolaei et al. showing that perceived barriers as a predictor of physical activity among students at Tehran University [35].
According to our findings, an educational intervention to promote a healthy lifestyle, empowerment courses to increase self-efficacy in overweight and obese employees, as well as providing policies based on improving physical activity in the workplace are suggested.
Limitations
One of the limitations of the present study was the respondents' self-assessment of physical activity, which may affect the accuracy of the reported information. Another limitation was the use of the short form of the IPAQ. Although reliable and sufficiently valid in recording physical activity, the short-form fails to distinguish different types of physical activity intensity, such as intense aerobic exercise, resistance training, or weight lifting, and different forms of physical activity that address different hemodynamic pathways.
Conclusion
In light of the present findings, it can be concluded that although the overweight male employees’ knowledge of preventing hypertension was high, their level of physical activity was lower than expected. This study showed that the constructs of the HBM can predict physical activity behavior in hypertension. However, more research is needed to confirm other predictors of related behaviors in employees.
Acknowledgments: The authors would like to thank the Alborz University of Medical Sciences, Karaj, Iran, and also the Social Determinants of Health Research Center.
Ethical Permissions: The research was approved by the Ethics Committee of Alborz University of Medical Sciences (IR.ABZUMS. REC.1398.152). Information about the study was presented to the participants and they gave verbal consent by taking the survey. All study procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki.
Conflicts of Interests: The authors have no conflicts of interests.
Authors’ Contribution: Hatefnia E (First Author), Introduction Writer/Main Researcher/Discussion Writer (30%); Kimiafar M (Second Author), Introduction Writer/Main Researcher/Discussion Writer (20%); Moghimbeigi A (Third Author), Main Researcher/Statistical Analyst (20 %); Safari-Moradabadi A (Forth Author), Methodologist/Assistant Researcher/Discussion Writer (30 %).
Funding/Support: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Hypertension is one of the most common risk factors for cardiovascular diseases (CVD) and a major global health threat afflicting one billion people worldwide [1]. Hypertension and its complications account for 9.4 million mortalities worldwide every year. It is estimated that the number of hypertension patients will increase to 1.56 billion worldwide by 2025 [2]. The global burden of disease study shows that systolic blood pressure accounts for the largest proportion of life (in years) lost due to premature death, accounting for 212 million years of life lost [3].
Except for some genetic factors that indicate a family history of high blood pressure, factors, such as overweight, high-salt diet, stress and anxiety, consumption of alcoholic beverages, and inactivity cause high blood pressure [4]. Physical inactivity is responsible for a large proportion of coronary heart disease, type II diabetes, and hypertension [5, 6, 7]. Unfortunately, advanced technology and mechanized life have reduced the rate of physical activity among people, and the adverse effects of this are quite evident [8]. The World Health Organization (WHO) reports the prevalence of physical inactivity to be more than 80% in adults and 23% in adolescents [9]. Surveys conducted in Iran show that 70 to 80% of Iranian society has not enough physical activity [10, 11]. On the other hand, employees include the highest proportion of sedentary people in Iranian society [12, 13]. The recently published WHO recommendations on physical activity state that all adults (18-64 years) should engage in 150-300 min of moderate-intensity, or 75-150 min of vigorous-intensity physical activity, or an equivalent combination of moderate- and vigorous-intensity activity throughout the week [14].
Exploring people's perceptions and health beliefs about physical activity may be useful for planning and implementing appropriate interventions thereby reducing the prevalence of hypertension. There are several patterns and models for identifying these effective factors that can be used to predict the foremost influential factors in effective health behaviors, of which the health belief model (HBM) is widely used as a basis for planning health education programs to promote adherence to preventive measures. This model points to the importance of individuals’ opinions about health and the perceived benefits and barriers to preventive and protective behavior. This model can be used to investigate the beliefs, values, and attitudes that underlie behavior because it consists of constructs that account for the important aspects of behavior change (Figure 1) [15].
Figure 1) Conceptual framework of health belief model.
Healthy behaviors are very important to prevent high blood pressure, which is the cause of cardiovascular diseases and diabetes. Considering the importance of men's health in economic performance and the role of family management, and due to the prevalence of overweight or obesity and its relationship with high blood pressure, awareness of men's beliefs and behavior in this field can be used in planning educational interventions to improve men's health. Therefore, the present study aimed to investigate health beliefs, physical activity, and the prevention of hypertension in overweight male employees.
Instrument and Methods
Study Design
The present descriptive-analytical cross-sectional study was done on overweight and obese male employees working in the Urmia offices between November and March 2021.
Sample size and method
The sample size was estimated to be 467 cases based on a formula and consultation with a statistician, considering a confidence level of 95% and a test power of 80%. The sampling procedure was as follows: first, all the offices in Urmia city were identified (19 cases) and then, a sample of 25 offices, which met the inclusion criteria were selected as a cluster for random selection of participants.
Inclusion and exclusion criteria
The inclusion criteria were overweight and obesity (based on body mass index (BMI)) and working in the Urmia offices. The exclusion criterion was incomplete questionnaires (failure to answer more than five questions). To meet the inclusion criteria (overweight and obesity), male employees were weighed, wearing light clothes and no shoes. To this aim, a standard scale (digital scale made in Germany with an accuracy of 0.1 kg) was used. The validity of the scale was checked with a control weight of 5 kg. Body height was also measured in a standing position using a standard caliper with an accuracy of 0.1 cm. The accuracy of the scale was also checked with a standard measurement scale of 100 cm long. Participants with a BMI≥25 were included in the study.
Data collection instrument
The instrument used to collect the required data was a researcher-made questionnaire in four sections. The first part contained demographic information, including age, education level, occupation, family income, and number of children.
The second part included ten questions exploring knowledge about physical activity and blood pressure (e.g., physical activity can prevent hypertension by controlling weight). In this section, a score of one was awarded for a correct answer and a score of zero for an incorrect answer or "I don't know", with a higher score indicating a higher level of knowledge.
The third part included the HBM constructs. Five questions enquired about perceived susceptibility (e.g., my chances of getting hypertension are high), four questions explored perceived severity (e.g., blood pressure can lead to death), five questions explored perceived benefits (e.g., I can get rid of my hypertension if I exercise properly), five questions addressed perceived barriers (e.g., I am too busy and hardly find time for physical activity), and three questions dealt with perceived self-efficacy (e.g., I can exercise every day to gain the right weight).
The fourth part consisted of questions about physical activity collected via the short form of the International Physical Activity Questionnaire (IPAQ) [16]. This questionnaire contained seven questions about intense and moderate physical activity, walking, and sedentary life in the past seven days.
Instrument validation
The content validity index (CVI) and the content validity ratio as well as experts’ commentaries (n=8) were used to validate the instrument. A test-retest method was used at two-week intervals to substantiate the reliability of the instrument. Cronbach's alpha value was higher than 0.7 for all parts.
Data analysis
Data analysis was done by SPSS 18 using descriptive and inferential statistics. Frequency and percentage were used to describe qualitative data and mean and standard deviation were used to describe quantitative data. The normality of data was assessed using the Kolmogorov-Smirnov test. As the normality of data was not confirmed, only standard nonparametric statistical tests were used to test the relationships or differences between quantitative variables. To explore the frequency of data, the Chi-square test was used. To test the between-group mean difference in physical activity and lack of physical activity, the Mann-Whitney U test was used. To assess the difference of three or more mean scores between the two groups, the Kruskal-Wallis test was applied. Pearson’s correlation coefficient was used to test the correlation between quantitative variables.
Findings
The participants’ age range was 28 to 57 years, with an average of 42.54 years. The highest percentage of the participants belonged to the age group of 28 to 38 years. All participants had a university degree, 83% were married, and 46% had an income less than $ 400 (Table 1).
Table 1) Participants’ socio-demographic variables and their correlation with physical activity
Table 2 shows the mean scores of knowledge and HBM constructs in the two groups. There were statistically significant between-group differences in the mean scores of perceived susceptibility, perceived severity, perceived barriers, and self-efficacy in physical activity (p<0.05).
Table2) Comparison of the mean scores of knowledge and health belief model (HBM) constructs in groups with and without physical activity
Pearson’s correlation coefficient results showed only a significant correlation between knowledge and perceived severity (r=0.095, p=0.04). No statistically significant correlation was found between knowledge and other HBM constructs. Table 3 indicates the predictors of physical activity measured using a logistic regression analysis. Self-efficacy and perceived barriers were found as predictors of physical activity. Thus, an increase in self-efficacy was followed by an increase in the probability of increasing physical activity to 0.91, and an increase in barriers to physical activity resulted in a 1.18% decrease in physical activity.
Table 3) Predictors of adopting preventive hypertension behavior based on the health belief model (HBM)
Discussion
The present study explored physical activity perceptions and behaviors to reduce the risk of hypertension in overweight male employees. The results showed that 25.1% of male employees had normal physical activity. The present findings are consistent with the findings reported by Bish et al. [17] but not those reported by Yahia et al. [18]. This difference could be related to the younger age of the students compared to the employees or the inherent differences in their profession.
The results of the present research showed no statistically significant difference between the two groups with and without physical activity in terms of the mean score of knowledge about the behavior to prevent hypertension. Both groups had the same level of knowledge about the topic. This result shows that knowledge alone is not sufficient to control health risk factors or adopt health-promoting behaviors. Although knowledge is an important determinant of behavior or lifestyle change, there may be other factors that play an important role in the transfer of knowledge into practice [19]. Al-Deagi et al. reported that participants had poor adherence despite sufficient knowledge about health care services and acquiring knowledge about diabetes was not sufficient to increase adherence to diabetes care [20].
Other researchers found that people's health-related behaviors require a minimum level of knowledge and motivation, and higher levels of knowledge about the disease lead to better self-care and adherence to medication or management. However, there is an inconsistency between knowledge of the disease and adherence to medication and disease management, and there is a mismatch between patient knowledge and behavior and participants were not acting on their knowledge. This noncompliance may be due to emotional, social, biological, and cultural factors that play a role in the adoption or non-adoption of the behavior [21, 22].
Aubert et al. investigated individuals’ knowledge, attitudes, and behaviors regarding hypertension. They found that most people had sufficient knowledge about hypertension, but few were sufficiently motivated and made efforts to change their behavior [23].
The results are also consistent with the findings of Imanipour et al. [24], who found no statistically significant correlation between knowledge and behavior for the prevention of CVDs. However, this was in contrast to the results of Baghianimoghadam et al. [25], who found a statistically significant relationship between knowledge and preventive behavior in CVDs. The present findings about the role of male employees’ health beliefs in the effect of physical activity on preventing hypertension showed a statistically significant difference between the perceived susceptibility of the groups with and without physical activity. The mean perceived susceptibility score was higher in men with physical activity than in men without, indicating that they are susceptible to hypertension and feel more at risk of developing hypertension. This result is consistent with that of Rahmati et al. on AIDS prevention behavior [26] and Morowaty et al. [27] on diabetes self-care behavior. These studies showed a statistically significant relationship between susceptibility and preventive behavior. These were, however, in contrast to the results of Baghianimoghadam et al. and Mahmoodabad and Tanekaboni [25, 28].
As the present study revealed, a statistically significant difference was found between the mean perceived severity scores of the two groups. Overweight male employees who did standard regular physical activities had a higher mean score of perceived severity than overweight male employees who did not. The present findings are consistent with the results of Mahmoodabad and Tanekaboni [28] and in contrast to the findings reported by Aligol et al. [29]. According to the mean perceived severity score and the fact that the symptoms of hypertension develop gradually in the long run, male employees may not have a high perceived severity, which should be considered in educational interventions to raise awareness of the significance of this issue.
There was a statistically significant difference in the mean perceived barriers score of the two groups, pointing to the importance of perceived barriers to physical activity, which is consistent with the findings reported by Baghianimoghadam et al. Mazloomy et al., and Jorvand et al. [25, 30, 31].
A statistically significant difference was found between overweight male employees who exercised regularly and those who did not in terms of the mean perceived self-efficacy of hypertension preventive behaviors. It means that the group with physical activity had a higher mean self-efficacy score. Given that self-efficacy has been cited as a predictor of behavior in most studies, its inclusion in educational interventions may play a critical role in changing or forming behavior. The findings related to self-efficacy are consistent with those reported by Kang et al. [32], Elwesif et al., and McElfish et al. [33, 34], yet contrast with the findings reported by Rahmati-Najarkolaei et al. [35].
The results of the regression analysis showed that self-efficacy was a significant predictor of physical activity in overweight male employees, pointing to the significance of self-efficacy to show healthy behaviors, and interventions to change physical activity should consider education to increase self-efficacy. These findings are consistent with the results of McElfishet al., showing that self-efficacy is a significant predictor of physical activity in obese and overweight adults [34].
Another significant predictor of physical activity was perceived barriers, which points to the importance of this construct (e.g., not having enough time to do physical activity and failure to perceive the real importance of physical activity) in doing physical activity. Lack of time was a barrier found for most employees. Policy making for regular physical activities in the workplace can lead to an increase in physical activity among male employees. The above-mentioned result is consistent with the findings reported by Rahmati-Najarkolaei et al. showing that perceived barriers as a predictor of physical activity among students at Tehran University [35].
According to our findings, an educational intervention to promote a healthy lifestyle, empowerment courses to increase self-efficacy in overweight and obese employees, as well as providing policies based on improving physical activity in the workplace are suggested.
Limitations
One of the limitations of the present study was the respondents' self-assessment of physical activity, which may affect the accuracy of the reported information. Another limitation was the use of the short form of the IPAQ. Although reliable and sufficiently valid in recording physical activity, the short-form fails to distinguish different types of physical activity intensity, such as intense aerobic exercise, resistance training, or weight lifting, and different forms of physical activity that address different hemodynamic pathways.
Conclusion
In light of the present findings, it can be concluded that although the overweight male employees’ knowledge of preventing hypertension was high, their level of physical activity was lower than expected. This study showed that the constructs of the HBM can predict physical activity behavior in hypertension. However, more research is needed to confirm other predictors of related behaviors in employees.
Acknowledgments: The authors would like to thank the Alborz University of Medical Sciences, Karaj, Iran, and also the Social Determinants of Health Research Center.
Ethical Permissions: The research was approved by the Ethics Committee of Alborz University of Medical Sciences (IR.ABZUMS. REC.1398.152). Information about the study was presented to the participants and they gave verbal consent by taking the survey. All study procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki.
Conflicts of Interests: The authors have no conflicts of interests.
Authors’ Contribution: Hatefnia E (First Author), Introduction Writer/Main Researcher/Discussion Writer (30%); Kimiafar M (Second Author), Introduction Writer/Main Researcher/Discussion Writer (20%); Moghimbeigi A (Third Author), Main Researcher/Statistical Analyst (20 %); Safari-Moradabadi A (Forth Author), Methodologist/Assistant Researcher/Discussion Writer (30 %).
Funding/Support: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Article Type: Descriptive & Survey |
Subject:
Health Education and Health Behavior
Received: 2023/03/13 | Accepted: 2023/05/28 | Published: 2023/06/25
Received: 2023/03/13 | Accepted: 2023/05/28 | Published: 2023/06/25
References
1. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224-60. [Link] [DOI:10.1016/S0140-6736(12)61766-8]
2. Rajati F, Hamzeh B, Pasdar Y, Safari R, Moradinazar M, Shakiba E, et al. Prevalence, awareness, treatment, and control of hypertension and their determinants: Results from the first cohort of non-communicable diseases in a Kurdish settlement. Sci Rep. 2019;9(1):1-10. [Link] [DOI:10.1038/s41598-019-48232-y]
3. Mirzaei M, Mirzaei M, Bagheri B, Dehghani A. Awareness, treatment, and control of hypertension and related factors in adult Iranian population. BMC Public Health. 2020;20(1):667. [Link] [DOI:10.1186/s12889-020-08831-1]
4. Gamage AU, Seneviratne RdA. Physical inactivity, and its association with hypertension among employees in the district of Colombo. BMC Public Health. 2021;21(1):1-11. [Link] [DOI:10.1186/s12889-021-12013-y]
5. Hayes P, Ferrara A, Keating A, McKnight K, O'Regan A. Physical activity and hypertension. Rev Cardiovascular Med. 2022;23(9):302. [Link] [DOI:10.31083/j.rcm2309302]
6. Dadipoor S, Shahsavari S, Ghaffari M, Farshidi H, Alavi A, Safari-Moradabadi A. A case-control study on lifestyle-related factors of hypertension in Iran. J Public Health. 2021;29:69-74. [Link] [DOI:10.1007/s10389-019-01109-w]
7. Dadipoor S, Fallahi S, Safari-Moradabadi A, Ghanbarnejad A, Montazerghaem H. Investigation of the epidemiology of hypertension and BMI in the adult population in the province of Hormozgan, during 2011. Life Sci J. 2013;10(10s):161-6. [Link]
8. Taghipour A, Shahroudi MV, Tabesh H, Safari-Moradabadi A, Anbarani MA. The effect of educational intervention based on the theory of planned behavior and stages of change construct on women's physical activity. J Educ Health Promot. 2019;8:195. [Link]
9. Moradi G, Mostafavi F, Piroozi B, Zareie B, Mahboobi M, Rasouli MA. The prevalence of physical inactivity in Iranian adolescents and the impact of economic and social inequalities on it: Results of a National Study in 2018. BMC public health. 2020;20:1-9. [Link] [DOI:10.1186/s12889-020-09618-0]
10. Solhi M, Ahmadi L, Taghdisi MH, Haghani H. The effect of trans theoretical model (TTM) on exercise behavior in pregnant women referred to dehaghan rural health center in. Iran J Med Educ. 2012;11(8):942-50. [Persian] [Link]
11. Hashemi SZ, Rakhshani F, Navidian A, Mosavi SR. Effectiveness of educational program based on Trans-Theoretical model on rate of physical activity among household women in Zahedan, Iran. J Health Syst Res. 2013;9(2):144-52. [Persian] [Link]
12. Shafieinia M, Heidarnia A, Kazemnejad A, Rajabi R. Psychometric factors affecting female employees physical activity status: Applying trans-theoretical model and theory of planned behavior. Avicenna J Clin Med. 2015;21(4):350-9. [Persian] [Link]
13. Baghianimoghadam M, Ehrampoush M, Ardian N, Soltani T. A research about health promoting activities (Lifestyle) at employees. TKJ. 2013;5(3):79-87. [Persian] [Link]
14. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451-62. [Link] [DOI:10.1136/bjsports-2020-102955]
15. Champion VL, Skinner CS. The health belief model. Health behavior and health education: Theory, research, and practice. Am Psychol Association. 2008;4:45-65. [Link]
16. Craig C, Marshall A, Sjostrom M, Bauman A, Lee P, Macfarlane D, et al. International physical activity questionnaire-short form. J Am Coll Health. 2017;65(7):492-501. [Link]
17. Bish CL, Blanck HM, Serdula MK, Marcus M, Kohl III HW, Khan LK. Diet and physical activity behaviors among Americans trying to lose weight: 2000 behavioral risk factor surveillance system. Obes Res. 2005;13(3):596-607. [Link] [DOI:10.1038/oby.2005.64]
18. Yahia N, Wang D, Rapley M, Dey R. Assessment of weight status, dietary habits and beliefs, physical activity, and nutritional knowledge among university students. Perspect Public Health. 2016;136(4):231-44. [Link] [DOI:10.1177/1757913915609945]
19. Bautista-Martinez S, Aguilar-Salinas CA, Lerman I, Velasco ML, Castellanos R, Zenteno E, et al. Diabetes knowledge and its determinants in a Mexican population. Diabetes Educ. 1999;25(3):374-81. [Link] [DOI:10.1177/014572179902500308]
20. Al-Deagi F, McElnay J, Scott M. Factors leading to non-compliance in elderly patients. Pharmaceutical J. 1995;255:8. [Link]
21. Klepac MJ. Theory and practical applications of a wellness perspective in diabetes education. Diabetes Educ. 1996;22(3):225-30. [Link] [DOI:10.1177/014572179602200305]
22. Barreto MdS, Reiners AAO, Marcon SS. Knowledge about hypertension and factors associated with the non-adherence to drug therapy. Rev Lat Am Enfermagem. 2014;22:491-8. [Link] [DOI:10.1590/0104-1169.3447.2442]
23. Aubert L, Bovet P, Gervasoni JP, Rwebogora A, Waeber B, Paccaud F. Knowledge, attitudes, and practices on hypertension in a country in epidemiological transition. Hypertension. 1998;31(5):1136-45. [Link] [DOI:10.1161/01.HYP.31.5.1136]
24. Imanipour M, Bassampour S, Haghani H. Relationship between preventive behaviors and knowledge regarding cardiovascular diseases. Hayat. 2008;14(2). [Persian] [Link]
25. Baghianimoghadam M, Mirzaei M, Rahimdel T. Role of health beliefs in preventive behaviors of individuals at risk of cardiovascular diseases. J Health Syst Res. 2013;8(7):1151-8. [Persian] [Link]
26. Rahmati FN, Shamsedin N, Farkhodeh Amin S, Fazlollah A, Parvin R. The implication of health belief model in planning educational programmes for preventing HIV/AIDS among university students. Payesh. 2009;8(4):349-59. [Persian] [Link]
27. Morowaty SMA, Rouhani TN. Perceived severity and susceptibility of diabetes complications and its relation to self-care behaviors among diabetic patients. Armaghan-e Danesh. 2007;13(3):59-68. [Persian] [Link]
28. Mahmoodabad SM, Tanekaboni NR. Survey of some related factors to oral health in high school female students in Yazd, on the basis of health behavior model (HBM). J Birjand Univ Med Sci. 2008;15(3):40-7. [Persian] [Link]
29. Aligol M, Kazemi S, Salim AY, Nasirzadeh M, Tayyebi Z. A survey on physical activity determinants as osteoporosis preventive behavior among pre-university female students of Rafsanjan in 2017: A descriptive study. JRUMS. 2019;18(5):455-68. [Persian] [Link]
30. Mazloomy S, Mirzaei A, Afkhami Ardakani M, Baghiani Moghadam M, Fallahzadeh H. The role of health beliefs in preventive behaviors of individuals at high-risk of type2 diabetes mellitus. JSSU. 2010;18(1):24-31. [Persian] [Link]
31. Jorvand R, Ghofranipour F, HaeriMehrizi A, Tavousi M. Evaluating the impact of HBM-based education on exercise among health care workers: The usage of mobile applications in Iran. BMC Public Health. 2020;20(1):1-11. [Link] [DOI:10.1186/s12889-020-08668-8]
32. Kang A, Dulin A, Risica PM. Relationship between adherence to diet and physical activity guidelines and self-efficacy among black women with high blood pressure. J Health Psychol. 2022;27(3):663-73. [Link] [DOI:10.1177/1359105320967105]
33. Elwesif SA, Mohammed MA, Elmwafy RI, Mohamed G. Effect of evidence based lifestyle guidelines on self-efficacy among hypertension patients. Port Said Sci J Nurs. 2021;8(1):226-54. [Link] [DOI:10.21608/pssjn.2021.52734.1073]
34. McElfish PA, Rowland B, Scott AJ, Boyers J, Long CR, Felix HC, et al. Examining the relationship between physical activity and self-efficacy for exercise among overweight and obese Marshallese adults. J Immigr Minor Health. 2022;24(2):461-8. [Link] [DOI:10.1007/s10903-021-01194-8]
35. Rahmati-Najarkolaei F, Tavafian SS, Fesharaki MG, Jafari MR. Factors predicting nutrition and physical activity behaviors due to cardiovascular disease in tehran university students: Application of health belief model. Iran Red Crescent Med J. 2015;17(3):e18879. [Link] [DOI:10.5812/ircmj.18879]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |