



Volume 11, Issue 1 (2023)
Health Educ Health Promot 2023, 11(1): 117-124 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yekefallah L, Namdar P, Mohammadi S, Dost Mohammadi S, Minaei Moghaddam S, Mafi M. Effect of Multimedia Sexual Index Promotion Package on Sexual Function, Desire, and Satisfaction of Married People: A Randomized Clinical Trial. Health Educ Health Promot 2023; 11 (1) :117-124
URL: http://hehp.modares.ac.ir/article-5-67106-en.html
URL: http://hehp.modares.ac.ir/article-5-67106-en.html
L. Yekefallah1  , P. Namdar2 , S. Mohammadi3 , S. Dost Mohammadi4, S. Minaei Moghaddam5 , M.H. Mafi * 6
, P. Namdar2 , S. Mohammadi3 , S. Dost Mohammadi4, S. Minaei Moghaddam5 , M.H. Mafi * 6
, P. Namdar2 , S. Mohammadi3 , S. Dost Mohammadi4, S. Minaei Moghaddam5 , M.H. Mafi * 6
1- “Social Determinants of Health Research Center” and “Department of Critical Care Nursing, Faculty of Nursing and Midwifery”, Qazvin University of Medical Sciences, Qazvin, Iran
2- “Department of Emergency Medicine” and “Metabolic Disease Research Center”, Qazvin University of Medical Science, Qazvin, Iran
3- Department of Intensive Care Nursing, Alborz University of Medical Sciences, Karaj, Iran
4- Department of Critical Care Nursing, School of Nursing & Midwifery, Qazvin University of Medical Sciences, Qazvin, Iran
5- Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
6- “Social Determinants of Health Research Center” and “Clinical Research Development Unit, Rajae Hospital”, Qazvin University of Medical Sciences, Qazvin, Iran
2- “Department of Emergency Medicine” and “Metabolic Disease Research Center”, Qazvin University of Medical Science, Qazvin, Iran
3- Department of Intensive Care Nursing, Alborz University of Medical Sciences, Karaj, Iran
4- Department of Critical Care Nursing, School of Nursing & Midwifery, Qazvin University of Medical Sciences, Qazvin, Iran
5- Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
6- “Social Determinants of Health Research Center” and “Clinical Research Development Unit, Rajae Hospital”, Qazvin University of Medical Sciences, Qazvin, Iran
Keywords: Multimedia [MeSH], Sexual Activity [MeSH], Sexual Arousal [MeSH], Sexual Satisfaction [MeSH], Covid-19 [MeSH]
Full-Text [PDF 1741 kb]
(2582 Downloads)
| Abstract (HTML) (1606 Views)
There was no significant difference in the number of sexual intercourses in the last week before the intervention between the two groups (Table 1), but after the intervention, there was a significant difference between the intervention group (2.36±1.36) and the control group (0.80±0.80) (t=4.148; p<0.001). Moreover, the intragroup test showed that there was a significant difference in the intervention group (z=-3.382; p=0.001), while this difference was not significant in the control group before and after the intervention (z= -1.000; p=0.317).
There was no significant difference between the sexual function scores before intervention in the control and intervention groups (p=0.661), while this difference was significant after the intervention (p<0.001). A significant difference was observed in the sexual function scores between before and after the intervention in the intervention group (p<0.001), but this difference was not significant in the control group in the mentioned time periods (p=0.126; Table 2).
Before the intervention, the sexual function scores of men did not differ significantly between the two groups (p=0.736), but after the intervention, a significant difference was observed (p=0.025). The results of the intragroup test showed that the difference between mean scores of the sexual function of men in the stages before and after the intervention in the control group was not significant (p=0.105), but in the intervention group it was significant (p=0.009; Table 2).
Table 1) Demographic information of the participants in two groups
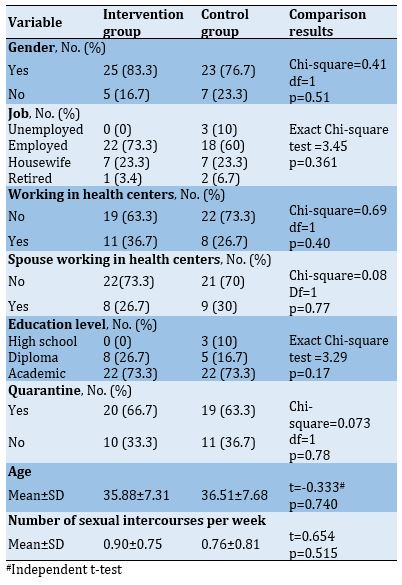
Table 2) Female and male sexual function scores before and after the intervention in two groupsIn sexual desire, there was no significant difference between the control and intervention groups
 .
.
in the pre-intervention stage (p=0.754). However, after the intervention, the score of the intervention group was significantly higher than the control group (p<0.001). The intragroup results did not show a significant difference between the score of sexual desire in the control group in the pre-test and post-test stages (p=0.145), while in the intervention group, the post-test score had a significant increase compared to the pre-test (p<0.001; Table 3).
Table 3) Total sexual desire score before and after the intervention in two groups
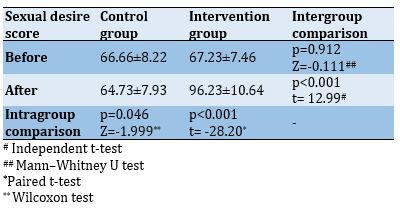
In the pre-intervention stage, there was no significant difference in the score of sexual satisfaction between the control and intervention groups (p=0.912), but in the post-intervention stage, this difference was significant (p<0.001). The results of the intragroup test showed that there was a significant difference between the scores of sexual satisfaction before and after the intervention in the control (p=0.046) and the intervention (p<0.001) groups, so that the scores in the post-test were significantly lower than the pre-test. However, in the intervention group, there was a significant increase in the post-test compared to the pre-test (Table 4). In this study, no harm was predicted for the studied groups.
Table 4) Total sexual satisfaction score before and after the intervention in two groups
Discussion
The results of other studies have shown a decrease in the quality of sexual life of men and women during the outbreak of Covid-19. This decrease in the quality of sexual life and marital relationships has been due to various reasons, including psychological stress caused by Covid-19 epidemic, fear of disease, work in medical centers, and observance of health protocols and so on. According to studies, there is a consensus that the prevalence of Covid-19 has also affected couples' sexual life by changing their lifestyle [29, 30]. Therefore, it is important to perform interventions to improve sexual life status. Now that face-to-face interventions are impossible due to the spread of the Covid-19 disease and that the safety of individuals is endangered, other appropriate educational methods should be used [31].
This study aimed to determine the effect of multimedia sexual indexes promotion packages on the sexual function, desire, and satisfaction of couples during the outbreak of Covid-19. The results showed that the multimedia sexual index promotion package improved the sexual function of men and women. The sexual function scores of both genders in the intervention group increased significantly after the intervention compared to the control group. The results of the present study were consistent with the study of Aliei et al. so that training for post-menopausal women with sexual dysfunction could improve their sexual function [32]. In other studies, training sexual intercourse to healthy or sick people with sexual dysfunction was able to improve their sexual function [33, 34]. Since sexual dysfunction has devastating effects on aspects of personal and social life, leading to psychological distress, incompatibility, marital failure, and divorce [35]. As a result, it is important to use appropriate interventions to promote sexual function during the pandemic. Proper sexual function is associated with greater enjoyment of life, improved quality of life, and improved cognitive function [7].
In the present study, the results indicated a positive and significant effect of sexual education on improving sexual desire in both genders. Sexual education in the present study, like the study of Kaviani et al. was able to modify sexual desire in individuals. By promoting knowledge and self-awareness, this education can identify people's sexual interests and decrease some of the barriers, which will lead couples to balanced sexual desires [19]. During the pandemic, the psychological burden of the outbreak of the disease changes behaviors and tendencies, even in people who are not infected. Because of the nature of the virus and the way it is transmitted, physical distance, and fear of getting the disease, obvious changes can be seen in sexual behavior [36]. Decreasing sexual desire itself takes sexual behavior out of balance because sexual desire depends on psychological factors, which can be affected by the psychological burden of the pandemic [37]. Many factors reducing sexual desire are due to the transition phase during the Covid-19 pandemic, and with proper sexual training, couples can provide a safe and disease-free condition to have healthy sexual relationships according to appropriate protocols. In this way, it reduces the stress and fear of getting infected during sexual intercourse and brings about a good experience and sexual satisfaction, which in itself is effective in improving sexual desire.
Regarding sexual satisfaction, like other sexual indexes, sexual education can improve sexual satisfaction in married people. The results of the present study were consistent with the study of Salehi Moghaddam et al., in which the results also showed the positive effect of sexual education on women's sexual satisfaction [38]. In the study of Zamani et al., sexual health counseling was effective in women's sexual satisfaction in the postpartum period [39]. Sexual training during the Covid-19 pandemic can provide safe sexual intercourse for married couples. According to studies, sexual satisfaction decreased during the outbreak of Covid-19 due to the pandemic and its consequences among men and women. This is due to the couple's ignorance about how to have a proper sexual relationship with their partner, which is mainly caused by the improper relationship [40]. Teaching proper sexual behavior and improving emotional relationships during this period will lead married couples to have sexual intercourse without any psychological pressure and improve the quality of their sexual intercourse by following the protocols related to having relaxed and stress-free sexual intercourse.
The outbreak of Covid-19, social distancing, and preventive protocols have negatively affected couples' sexual status, which in addition to reducing mental and physical health has also affected individuals' sexual health. Accordingly, such targeted interventions during this pandemic seem to be necessary to improve the quality of the sexual life of married people. Because society focuses more on patients and measures to reduce the burden of disease, and less attention is paid to healthy people. Therefore, planning should pay more attention to sexual and reproductive health services to avoid their negative consequences during the pandemic.
Conclusion
Multimedia sexual indexes promotion packages improve sexual function, desire, and satisfaction of couples during the outbreak of Covid-19.
Acknowledgments: The research team would like to express their gratitude for the cooperation of the esteemed participants and the Vice-Chancellor for Research of Qazvin University of Medical Sciences.
Ethical permission: The present study was registered with the ethics committee of Qazvin University of Medical Sciences with the ethics code IR.QUMS.REC.1399.341 (privacy protection was guaranteed). Also, this study was registered in the Iranian registry of clinical trials system (IRCT20191026045251N2). An informed consent form was obtained from all participants. This form was sent to them electronically in one of the virtual networks. Before sending the form, oral consent was obtained from them by phone call. Participation in this study was voluntary. Participants were assured that they could withdraw from the study at any time. Ensuring the samples keep personal information confidential and observing ethical principles in publishing research findings and all stages of the study are other cases in this field.
Conflict of Interests: The researchers stated that there is no conflict of interest in the present study.
Authors’ Contribution: Yekeh Fallah L (First Author), Introduction Writer/Methodologist/Main Researcher
/Discussion Writer (25%); Namdar P (Second Author), Methodologist/Discussion Writer (20%); Mohammadi S (Third Author), Introduction Writer/Discussion Writer (15%); Dost Mohammadi S (Fourth Author), Statistical Analyst/Discussion Writer (15%); Minaei Moghaddam S (Fifth Author), Statistical Analyst/Discussion Writer (15%); Mafi MH (Sixth Author), Methodologist (10%)
Funding: This research was financially supported by the Qazvin University of Medical Sciences.
Full-Text: (223 Views)
Introduction
On March 11, 2020, the World Health Organization announced that the respiratory disease caused by the new coronavirus, called Covid-19, was a pandemic [1], which is transmitted directly by contact [2]. The results of the studies showed no evidence of the presence of the virus in sexual secretions and its transmission through it [3, 4]. However, due to close contact during sexual intercourse, the couple may be more likely to transmit the virus, and the relationship can be more stressful. The stress of the possibility of transmitting the virus can lead to anxiety, fear, and lack of interest and frustration in sexual intercourse, and accordingly affect individuals' sexual function, desire, and satisfaction [5].
Sexual function is affected by many biological, psychological, and social factors. Sexual function has a significant impact on personal and social life, so it is the cause of some psychological problems and incompatibilities [6]. According to studies, there is a direct relationship between proper sexual function with physical and mental health and life quality [7]. Protocols now recommend the avoidance of social interactions and close personal contact, which have negative consequences for sexual behavior and function [8]. In addition to sexual function, sexual desire can also be affected by pandemic conditions. The starting point of sexual function and the necessity of sexual arousal is sexual desire, which is a set of forces and desires that lead a person to or away from sexual behaviors [9]. One of the factors affecting sexual desire is psychological factors [10]. The psychological burden of Covid-19 has exposed the general public to stress. Fear, stress, anxiety, and other disturbing mental symptoms can adversely affect sexual desire and function [11]. On the other hand, in addition to the two mentioned components, the quality of sexual intercourse is determined by an index called sexual satisfaction. Sexual satisfaction is defined as each person's judgment and analysis of the pleasurableness of sexual behavior [12]. Sexual satisfaction can lead to mental health and balance, and human happiness. If sexual satisfaction is not provided, sexual conflicts can endanger the couple's married life [13]. Sexual pleasure and satisfaction are mostly the product of the human mind, and psychological factors play an important role in sexual satisfaction [14]. Due to the consequences of the pandemic, the couple's relationship and sex life are at risk, which in itself has a negative effect on their sexual satisfaction. Hence, interventions to improve sexual intercourse is essential [15].
Sexual education studies have been able to improve sexual function in women with sexual dysfunction, and it is recommended that proper sexual behavior be provided as an effective and cost-effective solution to improve women's sexual function [16, 17]. Interventions such as medication, psychotherapy, and sexual education are also recommended to improve sexual desire. In studies, gaining skills and knowledge compared to drug therapy to improve sexual desire has been reported to be more effective. On the other hand, drug therapy has short-term effects, but the acquisition of knowledge, skills, and self-awareness have long-term and ongoing effects on sexual desire [18]. In the study of Kaviani et al., an educational intervention in the field of sexual health was reported to be effective for women with decreased sexual desire. Educational interventions can help people to treat sexual disorders by promoting sexual knowledge [19]. In the field of improving sexual satisfaction, many interventions such as life skills education [20] and sexual health education [21] have been done, the results of which have indicated the positive effect of educational interventions. In the study of Zargar Shoushtari et al., on-phone sexual education significantly increased sexual satisfaction [22].
As mentioned, the Covid-19 pandemic can have a significant effect on the components of sexual function, desire, and satisfaction, which according to studies sexual knowledge plays a significant role in predicting these components. Many inappropriate sexual activities of couples result from a lack of sexual skills and knowledge [23]. Therefore, in the current situation, interventions should be made to promote sexual knowledge, awareness, and skills. On the other hand, due to prevention protocols and contact restrictions, remote intervention is the best option. Therefore, the present study aimed to determine the effect of multimedia sexual indexes promotion packages on the sexual function, desire, and satisfaction of couples during the outbreak of coronavirus.
Materials and Methods
Study design and participants
This study was a two-group randomized clinical trial performed on 60 married people in Qazvin in 2022. This trial was conducted in parallel. Based on the inclusion criteria, 60 people were selected from the registrants as samples. Inclusion criteria included: being literate in reading and writing, having a smartphone and membership in a social network, consenting to participate in the study, living in Qazvin, having no pregnancy and lactation, and not having mental and physical chronic diseases. Exclusion criteria included: using drugs that affect sexual potency, being infected with coronavirus before the study, Participating in similar intervention, and having a sexually transmitted disease. All participants were present until the end of the study.
Sample size
To determine the sample size, a pilot sample was used so that the first 10 people in each group were considered as a pilot, and then by the formula of comparison of means, the sample size of 60 people was estimated (with a 10% sample drop). In the estimation of the sample size, the confidence level of 95% and the power of 80% were considered.
Randomization
In this study, the selection of the research sample was such that in another study, researchers placed a link at the end of their questionnaire for willing people to participate in the present intervention study. People who were willing to participate in the study expressed their initial desire. Explanations and how to implement the intervention were provided to them. Finally, the participants voluntarily registered to participate in the study. Sampling was performed by the simple random allocation method. The assignment sequence was determined by SPSS software, and participants were randomly divided into control and intervention groups.
In addition, this study was double-blind. In this study, the researcher and data analyzer were blinded in the study. The researcher determined the sequence of allocations and placed them in sealed envelopes to conceal the sequence. Then, the researcher's assistant opened the envelopes during the registration of people and randomly allocated people into two groups. The researcher’s assistant sent multimedia content and questionnaires. Only the researcher had access to the answers to the questionnaires. This method had maximum confidentiality to preserve the identity of people. Even during registration, codes were used instead of people's names. Also, numerical codes were defined for the study groups. The data analyst did not know about the control and intervention groups.
Study groups
Intervention group: In the intervention group, a multimedia package promoting sexual indicators was sent to people through the virtual network. This package was given to people for one month. To prevent the dissemination of information, the content was coded for people. It was also emphasized not to share the content with others during this intervention. People were contacted by phone once a week to answer their questions.
Control group: No action was taken on the control group during this period. At the end of the intervention, the content was given to the control group.
Interventions
• Stage 1) Preparing and validating the multimedia content
Before implementing the intervention, the content was produced based on the recommendations of reputable global health organizations (such as WHO, CDC, etc.) and the opinion of specialists and experts. To determine validity and adaptation to culture, the produced content was provided to specialists and experts in this field. Then the produced content was produced in a multimedia format. Mental issues caused by Covid-19 in sexual relations, how to have healthy sex during Covid-19, education before and during sexual relations when suspected of having a contagious disease, etc. were included in this package.
• Stage 2) Conducting the clinical trial
First, the objectives of the study and how to implement it were explained to the people of both groups. Then the questionnaires were taken as a pre-test. One month after the intervention, a post-test was taken from the intervention group. In the control group, a post-test was taken one month after the pre-test.
Tools
Demographic Questionnaire, Larson Sexual Satisfaction Questionnaire, Hurlbert Index of Sexual Desire, International Index of Erectile Function, and Female Sexual Function Index were used to collect data.
The demographic information questionnaire included questions related to age, number of sexual intercourses per week, quarantine at the time of the outbreak of Covid-19, quarantine at home, gender, employment status, education level, employment in medical centers, and spouse's employment in medical centers.
Larson's 25-item questionnaire (1988) was used to measure sexual satisfaction. Out of these 25 questions, 13 were negative questions (4, 5, 6, 7, 8, 9, 11, 14, 15, 18, 20, 24, 25), and 12 were the positive question (1, 2, 3, 10, 12, 13, 14, 16, 17, 19, 21, 22, 23). In the answer to each question, five options were included based on the Likert scale (never, rarely, sometimes, most of the time, and always), and each question was given a score of 1 to 5. Higher scores indicate more sexual satisfaction. The face and content validity of this tool were reported desirable, and Cronbach's alpha was calculated for the reliability of the tool (α=0.7) [24]. In this study, content validity was determined and confirmed. For reliability, Cronbach's alpha coefficient was estimated to be 0.72.
To assess sexual desire, the 25-item Hurlbert sexual desire questionnaire was used, which measured the subject's sexual desire. Each item was scored on a 5-point Likert scale (from always = 0 to never = 4). Questions 1, 3, 5, 7, 8, 9, 12, 13, 17, 18, 19, and 20 were scored in reverse. The minimum possible score was 0, and the maximum was 100, and a higher score indicated higher sensory cohesion (sexual desire). The validity of this questionnaire was appropriate, and the internal consistency coefficient was calculated at 0.86 using Cronbach's alpha [25]. In this study, content validity was determined and confirmed. For reliability, Cronbach's alpha coefficient was estimated to be 0.80.
Two separate questionnaires were used to assess sexual function in men and women. The Persian and modified versions of the International Index of Erectile Function (IIEF) of men questionnaire by Rosen et al. (1997) were used to assess male sexual function. The questionnaire consisted of 15 questions on a 5-point Likert scale so that for each question, scoring ranged from 1 (very poor function) to 5 (very good function). In the questionnaire, higher scores indicated desirable sexual function [26]. The validity of this tool was reported desirable in the study of Pakpour et al., and Cronbach's alpha rate was 0.73 [27]. The Female Sexual Function Index (FSFI) questionnaire was used to measure sexual performance in women. The questionnaire included areas of desire, arousal, lubrication, pain, orgasm, and satisfaction. Each question received a score from 0 to 5. A score of zero indicated that the person has not a sexual activity for the last 4 weeks. By summing the scores of the six areas together, the total score of the scale was obtained, with a minimum score of 2 and a maximum of 36. The cut-off point of the questionnaire was 26 [28]. This questionnaire had the necessary reliability and validity. To evaluate the reliability, Cronbach's alpha coefficient was calculated to be 0.85 [6]. In the present study, content validity was determined and confirmed for both questionnaires. For reliability, Cronbach's alpha coefficient was estimated to be 0.79 and 0.83, respectively.
Statistical analysis
The obtained data were statistically analyzed using SPSS 25 software. Descriptive statistics were used to describe and categorize the data. Chi-square and independent t-tests were used to evaluate the homogeneity of variables in the two groups. Wilcoxon and paired t-tests were used to evaluate the intragroup mean difference in the pre-test and post-test stages.
Mann-Whitney and independent t-tests were used to evaluate the mean differences between the groups. In all tests, a significance level of 0.05 was considered.
Findings
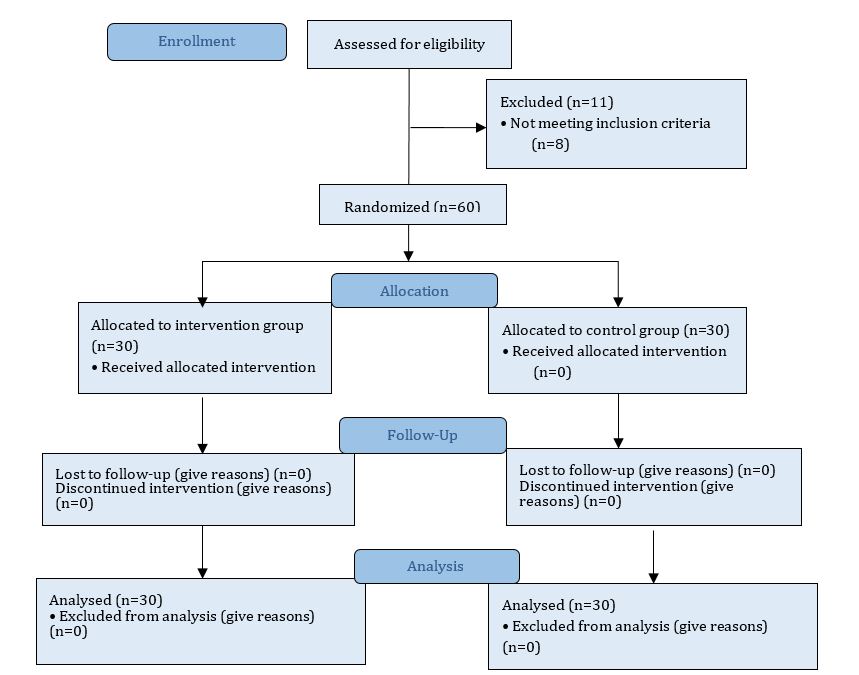
Sixty married people (30 in each group) participated in this study. All participants were present from the beginning to the end of the study, and no dropouts occurred (Figure 1). The mean age of the subjects was 36.18±7.44 years. There was no significant difference between the two groups in demographic characteristics, including gender, employment status, working in health centers, spouse working in health centers, education level, and quarantine (Table 1).
On March 11, 2020, the World Health Organization announced that the respiratory disease caused by the new coronavirus, called Covid-19, was a pandemic [1], which is transmitted directly by contact [2]. The results of the studies showed no evidence of the presence of the virus in sexual secretions and its transmission through it [3, 4]. However, due to close contact during sexual intercourse, the couple may be more likely to transmit the virus, and the relationship can be more stressful. The stress of the possibility of transmitting the virus can lead to anxiety, fear, and lack of interest and frustration in sexual intercourse, and accordingly affect individuals' sexual function, desire, and satisfaction [5].
Sexual function is affected by many biological, psychological, and social factors. Sexual function has a significant impact on personal and social life, so it is the cause of some psychological problems and incompatibilities [6]. According to studies, there is a direct relationship between proper sexual function with physical and mental health and life quality [7]. Protocols now recommend the avoidance of social interactions and close personal contact, which have negative consequences for sexual behavior and function [8]. In addition to sexual function, sexual desire can also be affected by pandemic conditions. The starting point of sexual function and the necessity of sexual arousal is sexual desire, which is a set of forces and desires that lead a person to or away from sexual behaviors [9]. One of the factors affecting sexual desire is psychological factors [10]. The psychological burden of Covid-19 has exposed the general public to stress. Fear, stress, anxiety, and other disturbing mental symptoms can adversely affect sexual desire and function [11]. On the other hand, in addition to the two mentioned components, the quality of sexual intercourse is determined by an index called sexual satisfaction. Sexual satisfaction is defined as each person's judgment and analysis of the pleasurableness of sexual behavior [12]. Sexual satisfaction can lead to mental health and balance, and human happiness. If sexual satisfaction is not provided, sexual conflicts can endanger the couple's married life [13]. Sexual pleasure and satisfaction are mostly the product of the human mind, and psychological factors play an important role in sexual satisfaction [14]. Due to the consequences of the pandemic, the couple's relationship and sex life are at risk, which in itself has a negative effect on their sexual satisfaction. Hence, interventions to improve sexual intercourse is essential [15].
Sexual education studies have been able to improve sexual function in women with sexual dysfunction, and it is recommended that proper sexual behavior be provided as an effective and cost-effective solution to improve women's sexual function [16, 17]. Interventions such as medication, psychotherapy, and sexual education are also recommended to improve sexual desire. In studies, gaining skills and knowledge compared to drug therapy to improve sexual desire has been reported to be more effective. On the other hand, drug therapy has short-term effects, but the acquisition of knowledge, skills, and self-awareness have long-term and ongoing effects on sexual desire [18]. In the study of Kaviani et al., an educational intervention in the field of sexual health was reported to be effective for women with decreased sexual desire. Educational interventions can help people to treat sexual disorders by promoting sexual knowledge [19]. In the field of improving sexual satisfaction, many interventions such as life skills education [20] and sexual health education [21] have been done, the results of which have indicated the positive effect of educational interventions. In the study of Zargar Shoushtari et al., on-phone sexual education significantly increased sexual satisfaction [22].
As mentioned, the Covid-19 pandemic can have a significant effect on the components of sexual function, desire, and satisfaction, which according to studies sexual knowledge plays a significant role in predicting these components. Many inappropriate sexual activities of couples result from a lack of sexual skills and knowledge [23]. Therefore, in the current situation, interventions should be made to promote sexual knowledge, awareness, and skills. On the other hand, due to prevention protocols and contact restrictions, remote intervention is the best option. Therefore, the present study aimed to determine the effect of multimedia sexual indexes promotion packages on the sexual function, desire, and satisfaction of couples during the outbreak of coronavirus.
Materials and Methods
Study design and participants
This study was a two-group randomized clinical trial performed on 60 married people in Qazvin in 2022. This trial was conducted in parallel. Based on the inclusion criteria, 60 people were selected from the registrants as samples. Inclusion criteria included: being literate in reading and writing, having a smartphone and membership in a social network, consenting to participate in the study, living in Qazvin, having no pregnancy and lactation, and not having mental and physical chronic diseases. Exclusion criteria included: using drugs that affect sexual potency, being infected with coronavirus before the study, Participating in similar intervention, and having a sexually transmitted disease. All participants were present until the end of the study.
Sample size
To determine the sample size, a pilot sample was used so that the first 10 people in each group were considered as a pilot, and then by the formula of comparison of means, the sample size of 60 people was estimated (with a 10% sample drop). In the estimation of the sample size, the confidence level of 95% and the power of 80% were considered.
Randomization
In this study, the selection of the research sample was such that in another study, researchers placed a link at the end of their questionnaire for willing people to participate in the present intervention study. People who were willing to participate in the study expressed their initial desire. Explanations and how to implement the intervention were provided to them. Finally, the participants voluntarily registered to participate in the study. Sampling was performed by the simple random allocation method. The assignment sequence was determined by SPSS software, and participants were randomly divided into control and intervention groups.
In addition, this study was double-blind. In this study, the researcher and data analyzer were blinded in the study. The researcher determined the sequence of allocations and placed them in sealed envelopes to conceal the sequence. Then, the researcher's assistant opened the envelopes during the registration of people and randomly allocated people into two groups. The researcher’s assistant sent multimedia content and questionnaires. Only the researcher had access to the answers to the questionnaires. This method had maximum confidentiality to preserve the identity of people. Even during registration, codes were used instead of people's names. Also, numerical codes were defined for the study groups. The data analyst did not know about the control and intervention groups.
Study groups
Intervention group: In the intervention group, a multimedia package promoting sexual indicators was sent to people through the virtual network. This package was given to people for one month. To prevent the dissemination of information, the content was coded for people. It was also emphasized not to share the content with others during this intervention. People were contacted by phone once a week to answer their questions.
Control group: No action was taken on the control group during this period. At the end of the intervention, the content was given to the control group.
Interventions
• Stage 1) Preparing and validating the multimedia content
Before implementing the intervention, the content was produced based on the recommendations of reputable global health organizations (such as WHO, CDC, etc.) and the opinion of specialists and experts. To determine validity and adaptation to culture, the produced content was provided to specialists and experts in this field. Then the produced content was produced in a multimedia format. Mental issues caused by Covid-19 in sexual relations, how to have healthy sex during Covid-19, education before and during sexual relations when suspected of having a contagious disease, etc. were included in this package.
• Stage 2) Conducting the clinical trial
First, the objectives of the study and how to implement it were explained to the people of both groups. Then the questionnaires were taken as a pre-test. One month after the intervention, a post-test was taken from the intervention group. In the control group, a post-test was taken one month after the pre-test.
Tools
Demographic Questionnaire, Larson Sexual Satisfaction Questionnaire, Hurlbert Index of Sexual Desire, International Index of Erectile Function, and Female Sexual Function Index were used to collect data.
The demographic information questionnaire included questions related to age, number of sexual intercourses per week, quarantine at the time of the outbreak of Covid-19, quarantine at home, gender, employment status, education level, employment in medical centers, and spouse's employment in medical centers.
Larson's 25-item questionnaire (1988) was used to measure sexual satisfaction. Out of these 25 questions, 13 were negative questions (4, 5, 6, 7, 8, 9, 11, 14, 15, 18, 20, 24, 25), and 12 were the positive question (1, 2, 3, 10, 12, 13, 14, 16, 17, 19, 21, 22, 23). In the answer to each question, five options were included based on the Likert scale (never, rarely, sometimes, most of the time, and always), and each question was given a score of 1 to 5. Higher scores indicate more sexual satisfaction. The face and content validity of this tool were reported desirable, and Cronbach's alpha was calculated for the reliability of the tool (α=0.7) [24]. In this study, content validity was determined and confirmed. For reliability, Cronbach's alpha coefficient was estimated to be 0.72.
To assess sexual desire, the 25-item Hurlbert sexual desire questionnaire was used, which measured the subject's sexual desire. Each item was scored on a 5-point Likert scale (from always = 0 to never = 4). Questions 1, 3, 5, 7, 8, 9, 12, 13, 17, 18, 19, and 20 were scored in reverse. The minimum possible score was 0, and the maximum was 100, and a higher score indicated higher sensory cohesion (sexual desire). The validity of this questionnaire was appropriate, and the internal consistency coefficient was calculated at 0.86 using Cronbach's alpha [25]. In this study, content validity was determined and confirmed. For reliability, Cronbach's alpha coefficient was estimated to be 0.80.
Two separate questionnaires were used to assess sexual function in men and women. The Persian and modified versions of the International Index of Erectile Function (IIEF) of men questionnaire by Rosen et al. (1997) were used to assess male sexual function. The questionnaire consisted of 15 questions on a 5-point Likert scale so that for each question, scoring ranged from 1 (very poor function) to 5 (very good function). In the questionnaire, higher scores indicated desirable sexual function [26]. The validity of this tool was reported desirable in the study of Pakpour et al., and Cronbach's alpha rate was 0.73 [27]. The Female Sexual Function Index (FSFI) questionnaire was used to measure sexual performance in women. The questionnaire included areas of desire, arousal, lubrication, pain, orgasm, and satisfaction. Each question received a score from 0 to 5. A score of zero indicated that the person has not a sexual activity for the last 4 weeks. By summing the scores of the six areas together, the total score of the scale was obtained, with a minimum score of 2 and a maximum of 36. The cut-off point of the questionnaire was 26 [28]. This questionnaire had the necessary reliability and validity. To evaluate the reliability, Cronbach's alpha coefficient was calculated to be 0.85 [6]. In the present study, content validity was determined and confirmed for both questionnaires. For reliability, Cronbach's alpha coefficient was estimated to be 0.79 and 0.83, respectively.
Statistical analysis
The obtained data were statistically analyzed using SPSS 25 software. Descriptive statistics were used to describe and categorize the data. Chi-square and independent t-tests were used to evaluate the homogeneity of variables in the two groups. Wilcoxon and paired t-tests were used to evaluate the intragroup mean difference in the pre-test and post-test stages.
Mann-Whitney and independent t-tests were used to evaluate the mean differences between the groups. In all tests, a significance level of 0.05 was considered.
Findings
Sixty married people (30 in each group) participated in this study. All participants were present from the beginning to the end of the study, and no dropouts occurred (Figure 1). The mean age of the subjects was 36.18±7.44 years. There was no significant difference between the two groups in demographic characteristics, including gender, employment status, working in health centers, spouse working in health centers, education level, and quarantine (Table 1).
Figure 1) Flowchart of distributions of participants in the intervention and control group
There was no significant difference in the number of sexual intercourses in the last week before the intervention between the two groups (Table 1), but after the intervention, there was a significant difference between the intervention group (2.36±1.36) and the control group (0.80±0.80) (t=4.148; p<0.001). Moreover, the intragroup test showed that there was a significant difference in the intervention group (z=-3.382; p=0.001), while this difference was not significant in the control group before and after the intervention (z= -1.000; p=0.317).
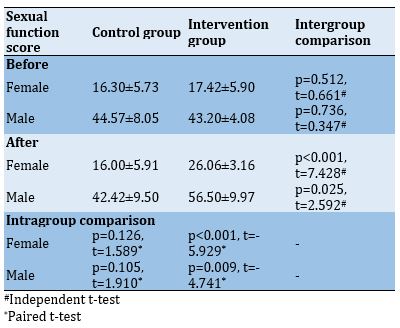
There was no significant difference between the sexual function scores before intervention in the control and intervention groups (p=0.661), while this difference was significant after the intervention (p<0.001). A significant difference was observed in the sexual function scores between before and after the intervention in the intervention group (p<0.001), but this difference was not significant in the control group in the mentioned time periods (p=0.126; Table 2).
Before the intervention, the sexual function scores of men did not differ significantly between the two groups (p=0.736), but after the intervention, a significant difference was observed (p=0.025). The results of the intragroup test showed that the difference between mean scores of the sexual function of men in the stages before and after the intervention in the control group was not significant (p=0.105), but in the intervention group it was significant (p=0.009; Table 2).
Table 1) Demographic information of the participants in two groups
Table 2) Female and male sexual function scores before and after the intervention in two groupsIn sexual desire, there was no significant difference between the control and intervention groups
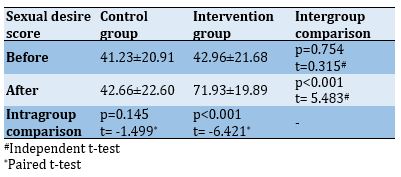
.in the pre-intervention stage (p=0.754). However, after the intervention, the score of the intervention group was significantly higher than the control group (p<0.001). The intragroup results did not show a significant difference between the score of sexual desire in the control group in the pre-test and post-test stages (p=0.145), while in the intervention group, the post-test score had a significant increase compared to the pre-test (p<0.001; Table 3).
Table 3) Total sexual desire score before and after the intervention in two groups
In the pre-intervention stage, there was no significant difference in the score of sexual satisfaction between the control and intervention groups (p=0.912), but in the post-intervention stage, this difference was significant (p<0.001). The results of the intragroup test showed that there was a significant difference between the scores of sexual satisfaction before and after the intervention in the control (p=0.046) and the intervention (p<0.001) groups, so that the scores in the post-test were significantly lower than the pre-test. However, in the intervention group, there was a significant increase in the post-test compared to the pre-test (Table 4). In this study, no harm was predicted for the studied groups.
Table 4) Total sexual satisfaction score before and after the intervention in two groups
Discussion
The results of other studies have shown a decrease in the quality of sexual life of men and women during the outbreak of Covid-19. This decrease in the quality of sexual life and marital relationships has been due to various reasons, including psychological stress caused by Covid-19 epidemic, fear of disease, work in medical centers, and observance of health protocols and so on. According to studies, there is a consensus that the prevalence of Covid-19 has also affected couples' sexual life by changing their lifestyle [29, 30]. Therefore, it is important to perform interventions to improve sexual life status. Now that face-to-face interventions are impossible due to the spread of the Covid-19 disease and that the safety of individuals is endangered, other appropriate educational methods should be used [31].
This study aimed to determine the effect of multimedia sexual indexes promotion packages on the sexual function, desire, and satisfaction of couples during the outbreak of Covid-19. The results showed that the multimedia sexual index promotion package improved the sexual function of men and women. The sexual function scores of both genders in the intervention group increased significantly after the intervention compared to the control group. The results of the present study were consistent with the study of Aliei et al. so that training for post-menopausal women with sexual dysfunction could improve their sexual function [32]. In other studies, training sexual intercourse to healthy or sick people with sexual dysfunction was able to improve their sexual function [33, 34]. Since sexual dysfunction has devastating effects on aspects of personal and social life, leading to psychological distress, incompatibility, marital failure, and divorce [35]. As a result, it is important to use appropriate interventions to promote sexual function during the pandemic. Proper sexual function is associated with greater enjoyment of life, improved quality of life, and improved cognitive function [7].
In the present study, the results indicated a positive and significant effect of sexual education on improving sexual desire in both genders. Sexual education in the present study, like the study of Kaviani et al. was able to modify sexual desire in individuals. By promoting knowledge and self-awareness, this education can identify people's sexual interests and decrease some of the barriers, which will lead couples to balanced sexual desires [19]. During the pandemic, the psychological burden of the outbreak of the disease changes behaviors and tendencies, even in people who are not infected. Because of the nature of the virus and the way it is transmitted, physical distance, and fear of getting the disease, obvious changes can be seen in sexual behavior [36]. Decreasing sexual desire itself takes sexual behavior out of balance because sexual desire depends on psychological factors, which can be affected by the psychological burden of the pandemic [37]. Many factors reducing sexual desire are due to the transition phase during the Covid-19 pandemic, and with proper sexual training, couples can provide a safe and disease-free condition to have healthy sexual relationships according to appropriate protocols. In this way, it reduces the stress and fear of getting infected during sexual intercourse and brings about a good experience and sexual satisfaction, which in itself is effective in improving sexual desire.
Regarding sexual satisfaction, like other sexual indexes, sexual education can improve sexual satisfaction in married people. The results of the present study were consistent with the study of Salehi Moghaddam et al., in which the results also showed the positive effect of sexual education on women's sexual satisfaction [38]. In the study of Zamani et al., sexual health counseling was effective in women's sexual satisfaction in the postpartum period [39]. Sexual training during the Covid-19 pandemic can provide safe sexual intercourse for married couples. According to studies, sexual satisfaction decreased during the outbreak of Covid-19 due to the pandemic and its consequences among men and women. This is due to the couple's ignorance about how to have a proper sexual relationship with their partner, which is mainly caused by the improper relationship [40]. Teaching proper sexual behavior and improving emotional relationships during this period will lead married couples to have sexual intercourse without any psychological pressure and improve the quality of their sexual intercourse by following the protocols related to having relaxed and stress-free sexual intercourse.
The outbreak of Covid-19, social distancing, and preventive protocols have negatively affected couples' sexual status, which in addition to reducing mental and physical health has also affected individuals' sexual health. Accordingly, such targeted interventions during this pandemic seem to be necessary to improve the quality of the sexual life of married people. Because society focuses more on patients and measures to reduce the burden of disease, and less attention is paid to healthy people. Therefore, planning should pay more attention to sexual and reproductive health services to avoid their negative consequences during the pandemic.
Conclusion
Multimedia sexual indexes promotion packages improve sexual function, desire, and satisfaction of couples during the outbreak of Covid-19.
Acknowledgments: The research team would like to express their gratitude for the cooperation of the esteemed participants and the Vice-Chancellor for Research of Qazvin University of Medical Sciences.
Ethical permission: The present study was registered with the ethics committee of Qazvin University of Medical Sciences with the ethics code IR.QUMS.REC.1399.341 (privacy protection was guaranteed). Also, this study was registered in the Iranian registry of clinical trials system (IRCT20191026045251N2). An informed consent form was obtained from all participants. This form was sent to them electronically in one of the virtual networks. Before sending the form, oral consent was obtained from them by phone call. Participation in this study was voluntary. Participants were assured that they could withdraw from the study at any time. Ensuring the samples keep personal information confidential and observing ethical principles in publishing research findings and all stages of the study are other cases in this field.
Conflict of Interests: The researchers stated that there is no conflict of interest in the present study.
Authors’ Contribution: Yekeh Fallah L (First Author), Introduction Writer/Methodologist/Main Researcher
/Discussion Writer (25%); Namdar P (Second Author), Methodologist/Discussion Writer (20%); Mohammadi S (Third Author), Introduction Writer/Discussion Writer (15%); Dost Mohammadi S (Fourth Author), Statistical Analyst/Discussion Writer (15%); Minaei Moghaddam S (Fifth Author), Statistical Analyst/Discussion Writer (15%); Mafi MH (Sixth Author), Methodologist (10%)
Funding: This research was financially supported by the Qazvin University of Medical Sciences.
Article Type: Original Research |
Subject:
Health Education and Health Behavior
Received: 2022/12/28 | Accepted: 2023/03/5 | Published: 2023/03/17
Received: 2022/12/28 | Accepted: 2023/03/5 | Published: 2023/03/17
References
1. World Health Organization. WHO Director-General's remarks at the media brieng on 2019-nCoV on 11 February 2020 [Internet]. Geneva: World Health Organization; 2020. [cited 2022 May 23]. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 [Link]
2. Cipriano M, Giacalone A, Ruberti E. Sexual behaviors during COVID-19: the potential risk of transmission. Arch Sex Behav. 2020;49(5):1431-2. [Link] [DOI:10.1007/s10508-020-01757-0]
3. Cui P, Chen Z, Wang T, Dai J, Zhang J, Ding T, et al. Clinical features and sexual transmission potential of SARS-CoV-2 infected female patients: a descriptive study in Wuhan, China. MedRxiv. 2020. [Link] [DOI:10.1101/2020.02.26.20028225]
4. Pan F, Xiao X, Guo J, Song Y, Li H, Patel DP, et al. No evidence of severe acute respiratory syndrome-coronavirus 2 in semen of males recovering from coronavirus disease 2019. Fertil Steril. 2020;113(6):1135-9. [Link] [DOI:10.1016/j.fertnstert.2020.04.024]
5. Gaspari V, Orioni G, Viviani F, Raone B, Lanzoni A, Bardazzi F. Does COVID‐19 influence sexual behaviors? Dermatol Ther. 2020;33(6):e14004. [Link] [DOI:10.1111/dth.14004]
6. Mousazadeh T, Motavalli R. Sexual function and behavior in pregnant women of Ardabil in 2016. J Health Care. 2018;20(1):40-7. [Persian] [Link] [DOI:10.29252/jhc.20.1.40]
7. Jacob L, Smith L, Butler L, Barnett Y, Grabovac I, McDermott D, et al. Challenges in the practice of sexual medicine in the time of COVID-19 in the United Kingdom. J Sex Med. 2020;17(7):1229-36. [Link] [DOI:10.1016/j.jsxm.2020.05.001]
8. Nenova M, DuHamel K, Zemon V, Rini C, Redd WH. Posttraumatic growth, social support, and social constraint in hematopoietic stem cell transplant survivors. Psychooncology. 2013;22(1):195-202. [Link] [DOI:10.1002/pon.2073]
9. Mitchell KR, Wellings KA, Graham C. How do men and women define sexual desire and sexual arousal? J Sex Marital Ther. 2014;40(1):17-32. [Link] [DOI:10.1080/0092623X.2012.697536]
10. Dosch A, Rochat L, Ghisletta P, Favez N, Van der Linden M. Psychological factors involved in sexual desire, sexual activity, and sexual satisfaction: A multi-factorial perspective. Arch Sex Behav. 2016;45(8):2029-45. [Link] [DOI:10.1007/s10508-014-0467-z]
11. Mertens G, Gerritsen L, Duijndam S, Salemink E, Engelhard IM. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J Anxiety Disord. 2020;74:102258. [Link] [DOI:10.1016/j.janxdis.2020.102258]
12. Pourakbaran E, Amin Yazdi SA. A study of sexual functioning and marital satisfaction in women with and without history of labor. J Fundament Ment Health. 2015;17(4):202-8. [Persian] [Link]
13. Mam Salehi H, Moradi O, Arefi M, Yar Ahmadi Y. The relationship between sex schemas and sexual satisfaction of couples: the mediating role of communication patterns. J Health Care. 2019;21(3):242-51. [Persian] [Link] [DOI:10.29252/jhc.21.3.242]
14. Lee TY, Sun GH, Chao SC. The effect of an infertility diagnosis on the distress, marital and sexual satisfaction between husbands and wives in Taiwan. Hum Reprod. 2001;16(8):1762-7. [Link] [DOI:10.1093/humrep/16.8.1762]
15. Li W, Li G, Xin C, Wang Y, Yang S. Challenges in the practice of sexual medicine in the time of COVID-19 in China. J Sex Med. 2020;17(7):1225-8. [Link] [DOI:10.1016/j.jsxm.2020.04.380]
16. Heidari M, Aminshokravi F, Zayeri F, Azin SA. Effect of sexual education on sexual function of Iranian couples during pregnancy: a quasi-experimental study. J Reprod Infertil. 2018;19(1):39-48. [Link]
17. Sheikhi ZP, Navidian A, Rigi M. Effect of sexual health education on sexual function and resumption of sexual intercourse after childbirth in primiparous women. J Educ Health Promot. 2020;9:87. [Link] [DOI:10.4103/jehp.jehp_591_19]
18. Palaniappan M, Heatherly R, Mintz LB, Connelly K, Wimberley T, Balzer AM, et al. Skills vs. pills: comparative effectiveness for low sexual desire in women. J Sex Marital Ther. 2018;44(1):1-15. [Link] [DOI:10.1080/0092623X.2017.1305029]
19. Kaviani M, Rahnavard T, Azima S, Emamghoreishi M, Asadi N, Sayadi M. The effect of education on the sexual health of women with hypoactive sexual desire disorder: A randomized controlled trial. Int J Community Based Nurs Midwifery. 2014;2(2):94-102. [Link]
20. Azizi A, Esmaeli R, Dehghan Manshadi S, Esmaeli S. The effectiveness of life skills training on marital satisfaction in divorce applicant couples. Iran J Nurs. 2016;29(99-100):22-33. [Persian] [Link] [DOI:10.29252/ijn.29.99.100.22]
21. Karimi A, Dadgar S, Afiat M, Rahimi N. The effect of sexual health education on couples' sexual satisfaction. Iran J Obstet Gynecol Infertil. 2013;15(42):23-30. [Persian] [Link]
22. Zargar Shoushtari S, Afshari P, Abedi P, Tabesh H. The effect of face-to-face with telephone-based counseling on sexual satisfaction among reproductive aged women in Iran. J Sex Marital Ther. 2015;41(4):361-7. [Link] [DOI:10.1080/0092623X.2014.915903]
23. Torabi F, Bakhahayesh A, Zareei H. Prediction of marital satisfaction based on the sensation-seeking and sexual knowledge. J Clin Psychol Person. 2020;18(1):67-77. [Persian] [Link]
24. Bahrami N, Yaghoobzadeh A, Sharif Nia H, Soliemani M, Haghdoost A. Psychometric properties of the Persian version of Larsons sexual satisfaction questionnaire in a sample of Iranian infertile couples. Iran J Epidemiol. 2016;12(2):18-31. [Persian] [Link]
25. Yousefi N, Farsani K, Shakiba A, Hemmati S, Nabavi Hesar J. Halbert Index of Sexual Desire (HISD) Questionnaire validation. J Clin Psychol Personal. 2014;11(2):107-18. [Persian] [Link]
26. Barghi Irani Z. Effectiveness of Cognitive Behavior Therapy in Aging (CBTO) on the improvement of pathological symptoms, cognitive correlations and some health-related behaviors in patients with Parkinson's disease [Dissertation]. Tehran: Payame Noor University Center; 2012. [Persian] [Link]
27. Pakpour AH, Zeidi IM, Yekaninejad MS, Burri A. Validation of a translated and culturally adapted Iranian version of the International Index of Erectile Function. J Sex Marital Ther. 2014;40(6):541-51. [Link] [DOI:10.1080/0092623X.2013.788110]
28. Fuchs A, Matonóg A, Pilarska J, Sieradzka P, Szul M, Czuba B, et al. The impact of COVID−19 on female sexual health. Int J Environ Res Public Health. 2020;17(19):7152. [Link] [DOI:10.3390/ijerph17197152]
29. Fang D, Peng J, Liao S, Tang Y, Cui W, Yuan Y, et al. An online questionnaire survey on the sexual life and sexual function of chinese adult men during the coronavirus disease 2019 epidemic. Sexual Medicine. 2021;9(1):100293. [Link] [DOI:10.1016/j.esxm.2020.100293]
30. Karagöz MA, Gül A, Borg C, Erihan İB, Uslu M, Ezer M, et al. Influence of COVID-19 pandemic on sexuality: a cross-sectional study among couples in Turkey. Int J Impotence Res. 2021;33:815-23. [Link] [DOI:10.1038/s41443-020-00378-4]
31. Ghafourifard M. The promotion of virtual education in Iran: The Potential which turned into reality by coronavirus. Iran J Med Educ. 2020;20:33-4. [Persian] [Link]
32. Aliei MM, Ghelichkhani F, Pakghohar M, Abadi MMM. Effectiveness of a sex education program on sexual function in postmenopausal women with sexual dysfunction: A randomized trial. Payesh (Health Monitor). 2016;15(2):181-92. [Persian] [Link]
33. Afshar M, Mohammad-Alizadeh-Charandabi S, Merghti-Khoei E-S, Yavarikia P. The effect of sex education on the sexual function of women in the first half of pregnancy: a randomized controlled trial. J Caring Sci. 2012;1(4):173-81. [Link]
34. Mansouri A, Shahramian I, Salehi H, Kord N, Khosravi F, Heidari MA. Effect of sexual health education based on health belief and pender health promotion models on the sexual function of females with type II diabetes. J Diabetes Nurs. 2020;8(1):992-1001. [Persian] [Link]
35. Heidari M, Ghodusi M, Rezaei P, Abyaneh SK, Sureshjani EH, Sheikhi RA. Sexual function and factors affecting menopause: a systematic review. J Menopausal Med. 2019;25(1):15-27. [Link] [DOI:10.6118/jmm.2019.25.1.15]
36. Ibarra FP, Mehrad M, Mauro MD, Godoy MFP, Cruz EG, Nilforoushzadeh MA, et al. Impact of the COVID-19 pandemic on the sexual behavior of the population. The vision of the east and the west. Int Braz J Urol. 2020;46(suppl.1):104-12. [Link] [DOI:10.1590/s1677-5538.ibju.2020.s116]
37. Carvalho J, Nobre P. Predictors of women's sexual desire: The role of psychopathology, cognitive-emotional determinants, relationship dimensions, and medical factors. J Sex Med. 2010;7(2):928-37. [Link] [DOI:10.1111/j.1743-6109.2009.01568.x]
38. Salehi Moghaddam F, TurkZahrani S, Moslemi A, Azin SA, Ozgoli G, Joulaee Rad N. Effectiveness of sexual skills training program on promoting sexual intimacy and satisfaction in women in Tehran (Iran): a randomized clinical trial study. Urol J. 2020;17(3):281-8. [Link]
39. Zamani M, Latifnejad Roudsari R, Moradi M, Esmaily H. The effect of sexual health counseling on women's sexual satisfaction in postpartum period: A randomized clinical trial. Int J Reprod Biomed. 2019;17(1):41-50. [Link] [DOI:10.18502/ijrm.v17i1.3819]
40. Omar SS, Dawood W, Eid N, Eldeeb D, Munir A, Arafat W. Psychological and sexual health during the Covid-19 pandemic in Egypt: are women suffering more? Sex Med. 2021;9(1):100295. [Link] [DOI:10.1016/j.esxm.2020.100295]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |