



Volume 10, Issue 3 (2022)
Health Educ Health Promot 2022, 10(3): 625-631 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Galdames S, González M. Coping Profiles and Health-Related Quality of Life of Public University Students. Health Educ Health Promot 2022; 10 (3) :625-631
URL: http://hehp.modares.ac.ir/article-5-60868-en.html
URL: http://hehp.modares.ac.ir/article-5-60868-en.html

1- Psychology Department, University of La Serena, La Serena, Chile
Keywords: University [MeSH], Students [MeSH], Coping Strategies [MeSH], Health-Related Quality of Life [MeSH]
Full-Text [PDF 586 kb]
(3153 Downloads)
| Abstract (HTML) (1767 Views)
Full-Text: (649 Views)
Introduction
University students go through a critical developmental period and the transition to university they are commonly exposed to several stressors like home changes, new social relationships, academic evaluations, increased academic difficulties, and self-regulation demands, which increases their risk of having mental health problems [1-3]. The prevalence of mental health disorders and emotional symptoms in Chile has been found in more than 45% of university students [4]. There is also a high prevalence of alcohol, cigarette, and other drug use in this population [5] which co-occur and increase depression, eating disorders, and suicide risk [6, 7]. The increased mental health vulnerability of university and college students is recognized worldwide widely and still is a problem to work on [8].
Educational consequences of poor mental health in university students have been associated with lower academic results, longer time of graduation, and dropout [9, 10]. Although this academic impact is important, the principal consequence of these stressful years is a decrease in the mental health and health life quality of students. Scientific evidence review has supported the negative association between stress and lower quality of life in university students [11].
Moreover, the consequences of high academic stress may increase by the presence of multiple risk factors and the lack of protective ones [12]. Therefore, socioeconomically vulnerable students must face a greater amount of stress during their university years, and from a positive psychology perspective, their psychosocial resources are crucial to complete university programs successfully. In this sense, we hope to contribute to the study of coping resources that help students maintain adequate integral health and life quality. This can be a guide for health promotion interventions for university students.
From this perspective, we follow the concept of coping strategies, with a widely accepted theoretical frame [13], and a good amount of empirical studies that allow its application to university students with stress issues.
The coping strategies concept refers to the psychological efforts that a person unfolds to adapt efficaciously to a perceived stressful situation. Due to the dynamic nature of social contexts, it is difficult to define standard favorable coping strategies, but the tendency has been to consider the approach and problem-solving coping more adaptive than avoidant coping, associating the avoidant strategies with adverse outcomes or negative implications for health and/or well-being [14-16].
Regarding academic stress coping strategies, there has been found that the most adaptive strategies, based on the transactional model [17], are classified as a- strategies oriented to problem-solving, including cognitive re-evaluation and planning, and b- emotion-oriented coping strategies that modulate stress impact, and they include social support seeking. Coping strategies can be learned, so they are a modifiable health factor and a promising concept for intervention development.
Even though several studies relate academic stress coping strategies and several health and well-being variables [18], less research has been done from a positive perspective, not focused on stress, but on personal resources that function as a catalyst of health self-regulation processes [19], that lid to maintain well-being adequate levels. for this reason, we include the study of positive affect regulation strategies as a complement to the study of coping stress strategies. positive psychology perspective has proposed the concept of happiness strategies, defined as the activities that students use to increase and maintain positive affect [15]. this concept has been studied in Chile as a positive effect-enhancing strategy [20], and its study has shown the association of happiness with specific strategies such as psychological control, active leisure/exercising, seeking instrumental goals, and partying. Other evidence on positive attitudes and related life quality in university students showed a significant role of forgiveness in the prediction of mental health outcomes [21].
Being coherent with the positive health psychology perspective, our study focuses on students’ life quality in health-related aspects, instead of emphasizing a psychopathological perspective. we follow an integral vision of health, which is well represented by the concept of healthy life quality (HLQ), where the subjective individual perception of health affection is a central factor [22]. Life quality perception is a cognitive evaluation of well-being and satisfaction with specific life contexts, such as health, and it is mediated by cognitive processes that include the identification of relevant indicators of one’s health, the definition of standards, and making a judgment about the personal condition [22].
Considering that academic context increases negative stress for university students, the aim was to analyze the relationship between coping academic profiles including stress, and positive affect-enhancing strategies with high health-related quality of life in university students.
Instrument and Methods
Through a relational transversal design, we obtained a random stratified polietapic sample. We evaluated 351 students at the University of La Serena. This sample was calculated based on the total regular students that enrolled in the second semester at the University of La Serena, which is a public university located in the north of Chile, enrolling an approximated 57% of students from the socioeconomically vulnerable situation. Sample stratification considered the four faculties that compose this university. The number of students of each faculty was obtained through the enrolment records platform. Then, we sorted 3 to 5 academic programs from each Faculty and student’s level to be evaluated.
The questionnaires were as follows:
-Academic Stress Coping Scale (Escala de Afrontamiento al Estrés Académico, ACEA) is the Spanish version of a self-reporting measure of academic stress coping strategies that university students use [17]. It contains 23 items of 5 Likert scale points that are grouped into three subscales: Cognitive Re-evaluation, Planning, and Social Support strategies. Answers go from 1=never use to 5=always use. It previously reported internal consistency with Cronbach Alpha=0.89 and a three-factor structure explaining 54% variance. And in the present application, internal consistency estimator for each sub-scale was cognitive re-evaluation’s Cronbach alpha=0.87 (9 items, n=351, item-total r=0.44-0.71), planning’s Cronbach alpha=0.85 (7 items, n=351, item-total r=0.46-0.67), and social support’s Cronbach alpha=0.91 (7 items, n=351, item-total r=0.63-0.80). Cronbach's alpha for the total scale (23 items) was 0.92.
-Health-related life quality was measured by the EUROQL-5D. The European :union: Health related to the quality of life group developed this instrument, and it has been widely used, including in Chile by health heading institutions [23]. This instrument has three components, the first is a descriptive general measure of self-perception of health in five domains: mobility, self-care, daily life activities, pain/discomfort, and anxiety/depression symptoms. each domain is evaluated by one item that gives three level answers: 1 for “no problems”, 2 for “moderated problems”, and 3 for “severe problems”. Its scores can be analyzed as single health problems or in a profile (health state) or added as a general score that goes from 5 (no symptoms) to 25 (severe symptoms). The EUROQL-5D includes a visual analog scale (VAS) that shows a picture of a thermometer in a vertical position, showing grades of the perceived state of health instead of temperature. The person is asked to mark a point/score from 0 to 100 representing her/his actual state of health. On this scale, “0” represents the worst imaginable state of health and “100” represents the best imaginable state of health. The last component converts the 5 dimension descriptive scores into an aggregated health index, based on a standard of general population preferences that is interpreted as a social evaluation of the different health states. But we did not apply this component for it exceeded our research objectives. Validity studies of EUROQL-5D found that its results correlate with the Stanford health assessment questionnaire (r=0.78 for EQ and r=0.61 for VAS) [24]. Also, it has been adapted and applied to the Chilean population [25, 26] and its diagnostic has been tested for suicidal risk detection in Chilean adolescents [27].
-Positive effects enhancing scale [20]: A Chilean version of the happiness increasing strategies scale (HIS) [28] that measures by self-report the behavioral strategies that a person uses to increase positive affect. Its Likert format of 4 points and 44 items has reported Cronbach Alpha=0.78 and a structural analysis that accounted for 46% variability [20]. Our validity of previous analysis for this scale using factor analysis showed inadequate model fit indices, so we decided of keeping only the items that had the best factorial loading in our analysis. this could be considered a shorter version of the instrument to be applied in this study. the selected items were structured in three factors: happiness disposition (12, 15, 16, 19), goal orientation (22, 26, 30, 37) and partying (20, 27, 32, 36). The final construct validity of this short version was studied by confirmatory factor analysis, ran by JAMOVI software. Model fit indices were X2(51fd)=136, p<0.01, CFI≥0.932, TLI≥0.912, RMSEA<0.068 (CI 0.054-0.083), and SRMR≤0.066. Cronbach’s Alpha internal consistency for happiness disposition was=0.79; for goal orientation=0.70 and for partying was 0.75.
We finally applied a form to register: sex, age, and program. All our research procedures followed the ethical guidelines derived from the Helsinki declaration. Students were asked to answer the instruments after an ordinary class, after accepting to participate by signing an informed participation consent.
Analysis was made with JAMOVI 1.6 software (free use). We applied descriptive statistics (Mean, Standard Dev, Frequency, and Percentages), student t, hierarchical cluster analysis with ward method, and ANOVA (Tukey post hoc).
Findings
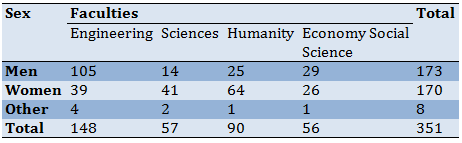
The mean age of participants was 21.83±2.83 and 91% of students ranged in age from 18-25 years old. Also, 49.3% of students were women, 48.4% were men and 2.3% did not feel represented by the two choices (Table 1).
Table 1) The number of students based on faculty and sex
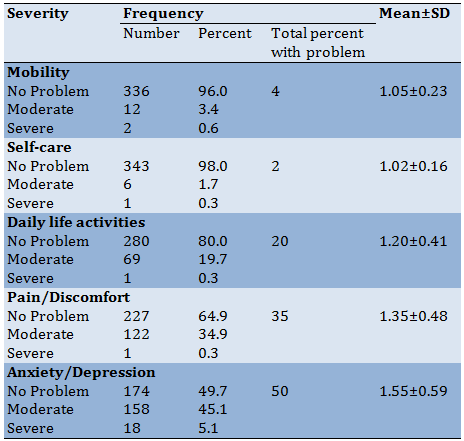
The EUROQOL-5D was first analyzed by calculating the percent of health singular items, which showed that 4% of students declare having mobility problems, 2% have self-care problems, 20% have daily life activities problems, 35% have pain/discomfort, 50% anxiety/depression symptoms (Table 2).
Table 2) Health problems descriptive statistics
The total percentage of students that manifested from 1 to 5 health problems was 65.24%, while 34.76% manifested not having any health problems. If the item’s scores are aggregated, we observed 6.18±1.16 with a range from 5 to 12 points. The students with one or more health problems had 27 different health states, the most frequent; 1-1-1-1-2 (31.6%), where the only problem >1 is the fifth (anxiety/depression) and 1-1-1-2-2 (19.3%) which shows the fourth problem also >1 (pain/discomfort). VAS`s general mean was 76.70±16.87 with a range of scores from 20 to 100. The correlation between the two evaluated components of health problems and health self-evaluation was Spearman r=-0.46.
Exploring differences in sociodemographic variables and faculty precedence, we found that individual health problems by faculty had no significant difference using the Chi-square estimator. Neither, there was no difference comparing problems sum by faculty using one-way ANOVA (F(3,346)=1.77, p<0.151). Nevertheless, analysis of Health Self-evaluation using ANOVA among faculties showed significant differences (F(3,344)=6.45, p<0.001). Tukey estimation showed the difference of lower level of health self-evaluation in humanities faculty (70.853±18.063) compared to engineering (80.164±15.128; p<0.001) and compared to sciences faculty (74.625±18.655; p=0.026).
We also found significant differences by sex in health self-evaluation means (t(347)=3,32, p<0.001), where men had higher mean score (79.780±15.326) than women (73.739±17.761). In the analysis focused on health problems, women declared having more total health problems (6.307±1.214) than men (6.034±1.099; t(340)=-2.18, p<0.030). More women declared to have pain/discomfort (n=69) than men (n=49; χ2(2, n=342)=6.46, p<0.01) and more women (n=95) declared to have anxiety/depression than men (n=76; χ2(2, n=342)=5.159, p=0.023). We found no differences in health self-evaluation or health problems by age of students.
The average mean scores for academic stress coping strategies variable were cognitive re-evaluation (3.218±.757), planning (3.077±.748), and social support seeking (3.054±.938). Testing for differences among faculties with ANOVA, we found significant differences in cognitive re-evaluation (F(3,347)=4.83, p<0.001) and planning (F(3,347)=4.07, p<0.01). Tukey post hoc estimation among groups, for cognitive re-evaluation, showed that differences were between engineering faculty (3.374±0.673) versus sciences (3.025±0.799; p<0.01) and humanities (p<0.01). Also, applying Tukey analysis to the planning subscale we only found a significant difference between engineering (3.237±0.675) and sciences faculty (2.922±0.883; p=0.033), and engineering compared to humanities faculty (2.960±0.771; p=0.027).
Difference by sex of the total sample was calculated with student t for independent samples and we only found a significant difference in cognitive re-evaluation (t(341)=5.20, p<0.001), where men had higher mean scores (3.422±0.693) than women (3.013±0.762). There were no differences by age of students in academic stress coping.
Subscales showed the following means: happiness disposition (2.858±.598), partying (2.299±.725), and goal orientation (2.912±.582). Testing for differences with ANOVA by faculty in positive effects enhancing strategies didn`t show significant results. Using student t for independent samples, we found a significant difference in happiness disposition by sex (t(341)=-2.27, p=0.024), in which women had a higher mean score (2.938±.619) than men (2.793±.568).
Profile analysis was made through hierarchical cluster analysis using the ward method, including the three academic coping stress strategies means and the three positive affect enhancing strategies means, previously standardized to Z scores. This analysis provided four different cluster solutions: 2, 3, 4, and 5 clusters and their theoretical interpretation criteria made the 5-cluster solution the most eligible one. These 5 clusters were interpreted as 5 different profiles based on the copying strategies that had higher scores than the mean. These profiles were named passive (all strategies are below mean), the optimist (happiness disposition and partying are higher than mean), intellectual (cognitive re-evaluation, planning, and goal orientation are higher than mean), support seeking (help to seek is higher than mean), and active (all strategies are higher than mean).
Then, we compared strategies' means by testing significant differences with simple ANOVA. All strategies mean differ significantly among profiles. ANOVA’s results for each coping strategy was cognitive re-evaluation (F(4,346)=82.94, p<0.01), help-seeking (F(4,346)=110.20, p<0.01), planning (F(4,346)=92.922, p<0.01), happiness disposition (F(4,346)=48.903, p<0.01), partying (F(4,346)=39.413, p<0.01), and goal orientation (F(3,346)=74.945, p<0.01). To test specific profile differences, we ran Tukey post hoc analysis (recommended for different group sizes), and to keep adequate extension, we will only detail the differences that were not significant, assuming the rest to be significantly different with p<0.01. Tukey's results showed that the cognitive re-evaluation strategy score was higher than the mean and had no significant difference between intellectual and active profiles (p<0.069); the help-seeking score was lower than the mean and had no difference between the optimist and intellectual profiles (p<1.0); planning score was higher than mean and had no difference between intellectual and active profiles (p<0.98); happiness disposition was close to mean and had no difference between Intellectual and Optimist profiles (p<0.135) and it was slightly lower than mean and had no difference between Intellectual and support seeking profile (p<0.529); partying was lower than mean and had no difference between passive and support seeking profiles (p<0.789) and it was higher than mean and had no difference between the optimist and Active profiles (p<0.380), and finally, goal orientation was lower than mean and had no significant difference between optimist and support seeking profiles (p<1.0).
Once we had analyzed the differences in coping strategies of profiles, we analyzed the differences in the HRLQ of profiles. First, we described health self-evaluation (VAS: 1-100) for each profile: passive profile (65.59±20.06; n=81), optimist profile (79.97±14.89; n=76), intellectual profile (79.63±15.12; n=68), support seeking (78.14±12.23; n=77) and active profile (85.55±16.80; n=38). Then, ANOVA showed a significant difference among health self-evaluation by profiles (F(4,343)=16.095, p<0.01), and post hoc Tukey analysis showed that the passive profile had lower health self-evaluation than the rest of the profiles (p<0.001).
On the second HRQL variable: health problems, we observed the following means for each profile: passive profile (6.70±1.4; n=81), optimist profile (6.00±1.11; n=76), intellectual profile (6.01±1.02; n=68), support seeking (6.15±.96; n=77) and active profile (5.74±.92; n=38). ANOVA results showed a significant difference among means (F(4,345)=7.091, p<0.001). Tukey's post hoc analysis showed that the passive profile’s health problems were significantly higher than the rest of the profiles (p<0.001).
Discussion
The first issue to be discussed from this study’s results is the high percentage of students that reported having health problems: 65.24%. This percentage is over statistics from the general Chilean population (from different age segments) which has been reported as 63.1%. And the high percentage of students who manifested psychological problems, that is, 50% of students compared to 42% in the general Chilean population. Both statistics are measured by the same instrument: EUROQOL-5D. In addition, VAS results show a mean of Self-evaluation of Health of 76.70±16.87, which is similar to VAS results of the Chilean general population, that is 75.65±19,06, but it is lower than the mean of healthy people without health problems: 87±12,89 [23]. This result shows that students from this public university have a lower HRLQ than the normal Chilean population, and it shows the same tendency, in similar study [29].
Our results on faculty differences, showed a significant difference in health self-evaluation, with lower scores of humanities students in comparison to engineering and economy/social sciences students. Our hypothesis on this difference is not related to academic demands but to gender-stereotyped differences, considering that humanities faculty has a greater number of women students and also programs that could be associated with more stereotyped feminine fields, such as psychology, teaching, special education, children education, literature, and language studies. in this sense, previous research shows a lower HRLQ in the women/feminine population [30]. this same tendency is confirmed by our results on Sex differences of the whole sample in Health Problems, where there is a gap effect between men's and women`s health, particularly on Health Self-evaluation and the presence of health problems such as pain/discomfort and anxiety/depression. This difference could be explained by previous gender inequality socialization, particularly in Latin-American has a patriarchal pattern where women have more social pressure, restrictive social expectations, familiar emotional load, different health behaviors, etc. [31]. Students’ mental health and gender should be recognized as important aspects of health promotion for university students with vulnerable conditions.
Another important result to be discussed is related to Academic Stress Coping strategies. Of the three types of strategies, Cognitive Re-evaluation was the most used by students. Exploring differences by sociodemographic variables, we found that men show more use of cognitive re-evaluation strategy compared to women, resulting also in significant differences in students from different faculty, where students from engineering faculty (more men) showed more cognitive re-evaluation and planning strategies compared to sciences and humanities (more women). Sex differences in the use of coping strategies are consistent with previous research [29, 30], and we follow the same hypothesis on gender inequality socialization and its effects on health.
Previous studies had shown that women tended to use more Help Seeking strategies [30], but our study found no such difference, for we have no tentative explicative hypothesis.
Results on positive effects enhancing strategies showed more use of happiness disposition and goal orientation than partying, as a whole sample, which is possibly associated with the low time disposition of university students.
There were no differences by age of students in academic stress coping nor in positive affect-enhancing strategies. This could be due to the sample characteristic where most students had similar ages, for they were in a brief range of age.
Profile results highlight the relevance of using academic stress coping and positive affect Enhancing strategies. In this way, the passive profile is characterized by the small use of all coping strategies, and students with this profile show more health problems and lower health self-evaluation than the rest of the profiles. This is a risk group of students that should have the opportunity to get support from the university system.
The best HRLQ was related to the active profile, which is characterized by using all strategies to cope with academic stress and enhance positive affect, which is the optimal situation, but we observed that it is a profile compound by a small number of students and that it is more common to find students from the three other profiles which use distinctive strategies. This shows that there are alternative patterns to cope with academic stress and maintain positive affect.
Conclusion
In conclusion, our results show a positive relationship between the use of coping strategies with better HRLQ of students. We also found some sex differences that could be showing gender inequities. From a preventive and promoting perspective of HRLQ in university students, we open the question of how we make university years a safer healthy environment for all students. We believe that this challenge needs the participation of all educational communities.
Acknowledgments: None declared.
Ethical Permissions: None declared.
Conflicts of Interests: None declared.
Authors’ Contributions: Galdames S (First Author), Introduction Writer/Main Researcher/Statistical Analyst/Discussion Writer (60%); Gonzalez M (Second Author), Methodologist/Statistical Analyst/Discussion Writer (40%)
Funding/Support: None declared.
University students go through a critical developmental period and the transition to university they are commonly exposed to several stressors like home changes, new social relationships, academic evaluations, increased academic difficulties, and self-regulation demands, which increases their risk of having mental health problems [1-3]. The prevalence of mental health disorders and emotional symptoms in Chile has been found in more than 45% of university students [4]. There is also a high prevalence of alcohol, cigarette, and other drug use in this population [5] which co-occur and increase depression, eating disorders, and suicide risk [6, 7]. The increased mental health vulnerability of university and college students is recognized worldwide widely and still is a problem to work on [8].
Educational consequences of poor mental health in university students have been associated with lower academic results, longer time of graduation, and dropout [9, 10]. Although this academic impact is important, the principal consequence of these stressful years is a decrease in the mental health and health life quality of students. Scientific evidence review has supported the negative association between stress and lower quality of life in university students [11].
Moreover, the consequences of high academic stress may increase by the presence of multiple risk factors and the lack of protective ones [12]. Therefore, socioeconomically vulnerable students must face a greater amount of stress during their university years, and from a positive psychology perspective, their psychosocial resources are crucial to complete university programs successfully. In this sense, we hope to contribute to the study of coping resources that help students maintain adequate integral health and life quality. This can be a guide for health promotion interventions for university students.
From this perspective, we follow the concept of coping strategies, with a widely accepted theoretical frame [13], and a good amount of empirical studies that allow its application to university students with stress issues.
The coping strategies concept refers to the psychological efforts that a person unfolds to adapt efficaciously to a perceived stressful situation. Due to the dynamic nature of social contexts, it is difficult to define standard favorable coping strategies, but the tendency has been to consider the approach and problem-solving coping more adaptive than avoidant coping, associating the avoidant strategies with adverse outcomes or negative implications for health and/or well-being [14-16].
Regarding academic stress coping strategies, there has been found that the most adaptive strategies, based on the transactional model [17], are classified as a- strategies oriented to problem-solving, including cognitive re-evaluation and planning, and b- emotion-oriented coping strategies that modulate stress impact, and they include social support seeking. Coping strategies can be learned, so they are a modifiable health factor and a promising concept for intervention development.
Even though several studies relate academic stress coping strategies and several health and well-being variables [18], less research has been done from a positive perspective, not focused on stress, but on personal resources that function as a catalyst of health self-regulation processes [19], that lid to maintain well-being adequate levels. for this reason, we include the study of positive affect regulation strategies as a complement to the study of coping stress strategies. positive psychology perspective has proposed the concept of happiness strategies, defined as the activities that students use to increase and maintain positive affect [15]. this concept has been studied in Chile as a positive effect-enhancing strategy [20], and its study has shown the association of happiness with specific strategies such as psychological control, active leisure/exercising, seeking instrumental goals, and partying. Other evidence on positive attitudes and related life quality in university students showed a significant role of forgiveness in the prediction of mental health outcomes [21].
Being coherent with the positive health psychology perspective, our study focuses on students’ life quality in health-related aspects, instead of emphasizing a psychopathological perspective. we follow an integral vision of health, which is well represented by the concept of healthy life quality (HLQ), where the subjective individual perception of health affection is a central factor [22]. Life quality perception is a cognitive evaluation of well-being and satisfaction with specific life contexts, such as health, and it is mediated by cognitive processes that include the identification of relevant indicators of one’s health, the definition of standards, and making a judgment about the personal condition [22].
Considering that academic context increases negative stress for university students, the aim was to analyze the relationship between coping academic profiles including stress, and positive affect-enhancing strategies with high health-related quality of life in university students.
Instrument and Methods
Through a relational transversal design, we obtained a random stratified polietapic sample. We evaluated 351 students at the University of La Serena. This sample was calculated based on the total regular students that enrolled in the second semester at the University of La Serena, which is a public university located in the north of Chile, enrolling an approximated 57% of students from the socioeconomically vulnerable situation. Sample stratification considered the four faculties that compose this university. The number of students of each faculty was obtained through the enrolment records platform. Then, we sorted 3 to 5 academic programs from each Faculty and student’s level to be evaluated.
The questionnaires were as follows:
-Academic Stress Coping Scale (Escala de Afrontamiento al Estrés Académico, ACEA) is the Spanish version of a self-reporting measure of academic stress coping strategies that university students use [17]. It contains 23 items of 5 Likert scale points that are grouped into three subscales: Cognitive Re-evaluation, Planning, and Social Support strategies. Answers go from 1=never use to 5=always use. It previously reported internal consistency with Cronbach Alpha=0.89 and a three-factor structure explaining 54% variance. And in the present application, internal consistency estimator for each sub-scale was cognitive re-evaluation’s Cronbach alpha=0.87 (9 items, n=351, item-total r=0.44-0.71), planning’s Cronbach alpha=0.85 (7 items, n=351, item-total r=0.46-0.67), and social support’s Cronbach alpha=0.91 (7 items, n=351, item-total r=0.63-0.80). Cronbach's alpha for the total scale (23 items) was 0.92.
-Health-related life quality was measured by the EUROQL-5D. The European :union: Health related to the quality of life group developed this instrument, and it has been widely used, including in Chile by health heading institutions [23]. This instrument has three components, the first is a descriptive general measure of self-perception of health in five domains: mobility, self-care, daily life activities, pain/discomfort, and anxiety/depression symptoms. each domain is evaluated by one item that gives three level answers: 1 for “no problems”, 2 for “moderated problems”, and 3 for “severe problems”. Its scores can be analyzed as single health problems or in a profile (health state) or added as a general score that goes from 5 (no symptoms) to 25 (severe symptoms). The EUROQL-5D includes a visual analog scale (VAS) that shows a picture of a thermometer in a vertical position, showing grades of the perceived state of health instead of temperature. The person is asked to mark a point/score from 0 to 100 representing her/his actual state of health. On this scale, “0” represents the worst imaginable state of health and “100” represents the best imaginable state of health. The last component converts the 5 dimension descriptive scores into an aggregated health index, based on a standard of general population preferences that is interpreted as a social evaluation of the different health states. But we did not apply this component for it exceeded our research objectives. Validity studies of EUROQL-5D found that its results correlate with the Stanford health assessment questionnaire (r=0.78 for EQ and r=0.61 for VAS) [24]. Also, it has been adapted and applied to the Chilean population [25, 26] and its diagnostic has been tested for suicidal risk detection in Chilean adolescents [27].
-Positive effects enhancing scale [20]: A Chilean version of the happiness increasing strategies scale (HIS) [28] that measures by self-report the behavioral strategies that a person uses to increase positive affect. Its Likert format of 4 points and 44 items has reported Cronbach Alpha=0.78 and a structural analysis that accounted for 46% variability [20]. Our validity of previous analysis for this scale using factor analysis showed inadequate model fit indices, so we decided of keeping only the items that had the best factorial loading in our analysis. this could be considered a shorter version of the instrument to be applied in this study. the selected items were structured in three factors: happiness disposition (12, 15, 16, 19), goal orientation (22, 26, 30, 37) and partying (20, 27, 32, 36). The final construct validity of this short version was studied by confirmatory factor analysis, ran by JAMOVI software. Model fit indices were X2(51fd)=136, p<0.01, CFI≥0.932, TLI≥0.912, RMSEA<0.068 (CI 0.054-0.083), and SRMR≤0.066. Cronbach’s Alpha internal consistency for happiness disposition was=0.79; for goal orientation=0.70 and for partying was 0.75.
We finally applied a form to register: sex, age, and program. All our research procedures followed the ethical guidelines derived from the Helsinki declaration. Students were asked to answer the instruments after an ordinary class, after accepting to participate by signing an informed participation consent.
Analysis was made with JAMOVI 1.6 software (free use). We applied descriptive statistics (Mean, Standard Dev, Frequency, and Percentages), student t, hierarchical cluster analysis with ward method, and ANOVA (Tukey post hoc).
Findings
The mean age of participants was 21.83±2.83 and 91% of students ranged in age from 18-25 years old. Also, 49.3% of students were women, 48.4% were men and 2.3% did not feel represented by the two choices (Table 1).
Table 1) The number of students based on faculty and sex
The EUROQOL-5D was first analyzed by calculating the percent of health singular items, which showed that 4% of students declare having mobility problems, 2% have self-care problems, 20% have daily life activities problems, 35% have pain/discomfort, 50% anxiety/depression symptoms (Table 2).
Table 2) Health problems descriptive statistics
The total percentage of students that manifested from 1 to 5 health problems was 65.24%, while 34.76% manifested not having any health problems. If the item’s scores are aggregated, we observed 6.18±1.16 with a range from 5 to 12 points. The students with one or more health problems had 27 different health states, the most frequent; 1-1-1-1-2 (31.6%), where the only problem >1 is the fifth (anxiety/depression) and 1-1-1-2-2 (19.3%) which shows the fourth problem also >1 (pain/discomfort). VAS`s general mean was 76.70±16.87 with a range of scores from 20 to 100. The correlation between the two evaluated components of health problems and health self-evaluation was Spearman r=-0.46.
Exploring differences in sociodemographic variables and faculty precedence, we found that individual health problems by faculty had no significant difference using the Chi-square estimator. Neither, there was no difference comparing problems sum by faculty using one-way ANOVA (F(3,346)=1.77, p<0.151). Nevertheless, analysis of Health Self-evaluation using ANOVA among faculties showed significant differences (F(3,344)=6.45, p<0.001). Tukey estimation showed the difference of lower level of health self-evaluation in humanities faculty (70.853±18.063) compared to engineering (80.164±15.128; p<0.001) and compared to sciences faculty (74.625±18.655; p=0.026).
We also found significant differences by sex in health self-evaluation means (t(347)=3,32, p<0.001), where men had higher mean score (79.780±15.326) than women (73.739±17.761). In the analysis focused on health problems, women declared having more total health problems (6.307±1.214) than men (6.034±1.099; t(340)=-2.18, p<0.030). More women declared to have pain/discomfort (n=69) than men (n=49; χ2(2, n=342)=6.46, p<0.01) and more women (n=95) declared to have anxiety/depression than men (n=76; χ2(2, n=342)=5.159, p=0.023). We found no differences in health self-evaluation or health problems by age of students.
The average mean scores for academic stress coping strategies variable were cognitive re-evaluation (3.218±.757), planning (3.077±.748), and social support seeking (3.054±.938). Testing for differences among faculties with ANOVA, we found significant differences in cognitive re-evaluation (F(3,347)=4.83, p<0.001) and planning (F(3,347)=4.07, p<0.01). Tukey post hoc estimation among groups, for cognitive re-evaluation, showed that differences were between engineering faculty (3.374±0.673) versus sciences (3.025±0.799; p<0.01) and humanities (p<0.01). Also, applying Tukey analysis to the planning subscale we only found a significant difference between engineering (3.237±0.675) and sciences faculty (2.922±0.883; p=0.033), and engineering compared to humanities faculty (2.960±0.771; p=0.027).
Difference by sex of the total sample was calculated with student t for independent samples and we only found a significant difference in cognitive re-evaluation (t(341)=5.20, p<0.001), where men had higher mean scores (3.422±0.693) than women (3.013±0.762). There were no differences by age of students in academic stress coping.
Subscales showed the following means: happiness disposition (2.858±.598), partying (2.299±.725), and goal orientation (2.912±.582). Testing for differences with ANOVA by faculty in positive effects enhancing strategies didn`t show significant results. Using student t for independent samples, we found a significant difference in happiness disposition by sex (t(341)=-2.27, p=0.024), in which women had a higher mean score (2.938±.619) than men (2.793±.568).
Profile analysis was made through hierarchical cluster analysis using the ward method, including the three academic coping stress strategies means and the three positive affect enhancing strategies means, previously standardized to Z scores. This analysis provided four different cluster solutions: 2, 3, 4, and 5 clusters and their theoretical interpretation criteria made the 5-cluster solution the most eligible one. These 5 clusters were interpreted as 5 different profiles based on the copying strategies that had higher scores than the mean. These profiles were named passive (all strategies are below mean), the optimist (happiness disposition and partying are higher than mean), intellectual (cognitive re-evaluation, planning, and goal orientation are higher than mean), support seeking (help to seek is higher than mean), and active (all strategies are higher than mean).
Then, we compared strategies' means by testing significant differences with simple ANOVA. All strategies mean differ significantly among profiles. ANOVA’s results for each coping strategy was cognitive re-evaluation (F(4,346)=82.94, p<0.01), help-seeking (F(4,346)=110.20, p<0.01), planning (F(4,346)=92.922, p<0.01), happiness disposition (F(4,346)=48.903, p<0.01), partying (F(4,346)=39.413, p<0.01), and goal orientation (F(3,346)=74.945, p<0.01). To test specific profile differences, we ran Tukey post hoc analysis (recommended for different group sizes), and to keep adequate extension, we will only detail the differences that were not significant, assuming the rest to be significantly different with p<0.01. Tukey's results showed that the cognitive re-evaluation strategy score was higher than the mean and had no significant difference between intellectual and active profiles (p<0.069); the help-seeking score was lower than the mean and had no difference between the optimist and intellectual profiles (p<1.0); planning score was higher than mean and had no difference between intellectual and active profiles (p<0.98); happiness disposition was close to mean and had no difference between Intellectual and Optimist profiles (p<0.135) and it was slightly lower than mean and had no difference between Intellectual and support seeking profile (p<0.529); partying was lower than mean and had no difference between passive and support seeking profiles (p<0.789) and it was higher than mean and had no difference between the optimist and Active profiles (p<0.380), and finally, goal orientation was lower than mean and had no significant difference between optimist and support seeking profiles (p<1.0).
Once we had analyzed the differences in coping strategies of profiles, we analyzed the differences in the HRLQ of profiles. First, we described health self-evaluation (VAS: 1-100) for each profile: passive profile (65.59±20.06; n=81), optimist profile (79.97±14.89; n=76), intellectual profile (79.63±15.12; n=68), support seeking (78.14±12.23; n=77) and active profile (85.55±16.80; n=38). Then, ANOVA showed a significant difference among health self-evaluation by profiles (F(4,343)=16.095, p<0.01), and post hoc Tukey analysis showed that the passive profile had lower health self-evaluation than the rest of the profiles (p<0.001).
On the second HRQL variable: health problems, we observed the following means for each profile: passive profile (6.70±1.4; n=81), optimist profile (6.00±1.11; n=76), intellectual profile (6.01±1.02; n=68), support seeking (6.15±.96; n=77) and active profile (5.74±.92; n=38). ANOVA results showed a significant difference among means (F(4,345)=7.091, p<0.001). Tukey's post hoc analysis showed that the passive profile’s health problems were significantly higher than the rest of the profiles (p<0.001).
Discussion
The first issue to be discussed from this study’s results is the high percentage of students that reported having health problems: 65.24%. This percentage is over statistics from the general Chilean population (from different age segments) which has been reported as 63.1%. And the high percentage of students who manifested psychological problems, that is, 50% of students compared to 42% in the general Chilean population. Both statistics are measured by the same instrument: EUROQOL-5D. In addition, VAS results show a mean of Self-evaluation of Health of 76.70±16.87, which is similar to VAS results of the Chilean general population, that is 75.65±19,06, but it is lower than the mean of healthy people without health problems: 87±12,89 [23]. This result shows that students from this public university have a lower HRLQ than the normal Chilean population, and it shows the same tendency, in similar study [29].
Our results on faculty differences, showed a significant difference in health self-evaluation, with lower scores of humanities students in comparison to engineering and economy/social sciences students. Our hypothesis on this difference is not related to academic demands but to gender-stereotyped differences, considering that humanities faculty has a greater number of women students and also programs that could be associated with more stereotyped feminine fields, such as psychology, teaching, special education, children education, literature, and language studies. in this sense, previous research shows a lower HRLQ in the women/feminine population [30]. this same tendency is confirmed by our results on Sex differences of the whole sample in Health Problems, where there is a gap effect between men's and women`s health, particularly on Health Self-evaluation and the presence of health problems such as pain/discomfort and anxiety/depression. This difference could be explained by previous gender inequality socialization, particularly in Latin-American has a patriarchal pattern where women have more social pressure, restrictive social expectations, familiar emotional load, different health behaviors, etc. [31]. Students’ mental health and gender should be recognized as important aspects of health promotion for university students with vulnerable conditions.
Another important result to be discussed is related to Academic Stress Coping strategies. Of the three types of strategies, Cognitive Re-evaluation was the most used by students. Exploring differences by sociodemographic variables, we found that men show more use of cognitive re-evaluation strategy compared to women, resulting also in significant differences in students from different faculty, where students from engineering faculty (more men) showed more cognitive re-evaluation and planning strategies compared to sciences and humanities (more women). Sex differences in the use of coping strategies are consistent with previous research [29, 30], and we follow the same hypothesis on gender inequality socialization and its effects on health.
Previous studies had shown that women tended to use more Help Seeking strategies [30], but our study found no such difference, for we have no tentative explicative hypothesis.
Results on positive effects enhancing strategies showed more use of happiness disposition and goal orientation than partying, as a whole sample, which is possibly associated with the low time disposition of university students.
There were no differences by age of students in academic stress coping nor in positive affect-enhancing strategies. This could be due to the sample characteristic where most students had similar ages, for they were in a brief range of age.
Profile results highlight the relevance of using academic stress coping and positive affect Enhancing strategies. In this way, the passive profile is characterized by the small use of all coping strategies, and students with this profile show more health problems and lower health self-evaluation than the rest of the profiles. This is a risk group of students that should have the opportunity to get support from the university system.
The best HRLQ was related to the active profile, which is characterized by using all strategies to cope with academic stress and enhance positive affect, which is the optimal situation, but we observed that it is a profile compound by a small number of students and that it is more common to find students from the three other profiles which use distinctive strategies. This shows that there are alternative patterns to cope with academic stress and maintain positive affect.
Conclusion
In conclusion, our results show a positive relationship between the use of coping strategies with better HRLQ of students. We also found some sex differences that could be showing gender inequities. From a preventive and promoting perspective of HRLQ in university students, we open the question of how we make university years a safer healthy environment for all students. We believe that this challenge needs the participation of all educational communities.
Acknowledgments: None declared.
Ethical Permissions: None declared.
Conflicts of Interests: None declared.
Authors’ Contributions: Galdames S (First Author), Introduction Writer/Main Researcher/Statistical Analyst/Discussion Writer (60%); Gonzalez M (Second Author), Methodologist/Statistical Analyst/Discussion Writer (40%)
Funding/Support: None declared.
Article Type: Qualitative Research |
Subject:
Quality of Life
Received: 2022/04/14 | Accepted: 2022/07/15 | Published: 2022/08/30
Received: 2022/04/14 | Accepted: 2022/07/15 | Published: 2022/08/30
References
1. Auerbach RP, Alonso J, Axinn WG, Cuijpers P, Ebert DD, Green JG, et al. Mental disorders among college students in the World Health Organization World Mental Health Surveys. Psychol Med. 2016;46(14):2955-70. [Link] [DOI:10.1017/S0033291716001665]
2. Chung W, Hudziak J. The transitional age brain: the best of times and the worst of times. Child Adolesc Psychiatr Clin N Am. 2017;26:157-75. [Link] [DOI:10.1016/j.chc.2016.12.017]
3. Evans T, Bira L, Gastelum J, Weiss T, Vanderford N. Evidence for a mental health crisis in graduate education. Nat Biotechnol. 2018;36:282-4. [Link] [DOI:10.1038/nbt.4089]
4. Barrera A. Study revealed that 44% of university students have been in psychological treatment [Internet]. Chile: Catholic University of Temuco; 2019 [Cited 2021 Feb 12]. Available from: https://prensa.uct.cl/2019/04/estudio-revelo-que-el-44-de-los-universitarios-ha-estado-en-tratamiento-psicologico/ [Spanish] [Link]
5. Becerra S. Description of health behavior of a group of university students in Lima. Revista de Psicología. 2016;34(2):239-60. [Spanish] [Link] [DOI:10.18800/psico.201602.001]
6. Baader T, Rojas C, Molina J, Gotelli M, Alamo C, Fierro C, et al. Diagnostic of the prevalence of mental health disorders in college students and associated emotional risk factors. Rev Chil Neuro Psiquiatr. 2014;52(3):167-76. [Spanish] [Link] [DOI:10.4067/S0717-92272014000300004]
7. Barrera-Herrera A. Prevalence of mental health symptoms and health related habits in a sample of Chilean university students. Psykhe. 2021;30(1). [Spanish] [Link]
8. Duffy A, Saunders KEA, Malhi GS, Patten S, Cipriani A, McNevin S, et al. Mental health care for university students: a way forward?. Lancet Psychiatry. 2019;6(11):885-7. [Link] [DOI:10.1016/S2215-0366(19)30275-5]
9. Bruffaerts R, Mortier P, Kiekens G, Auerbach R, Cuijpersd P, Demyttenaere K, et al. Mental health problems in college freshmen: prevalence and academic functioning. J Affect Disord. 2018;225:97-103. [Link] [DOI:10.1016/j.jad.2017.07.044]
10. Cornaglia F, Crivellaro E, McNally S. Mental health and education decisions. Labour Econ. 2015;33:1-12. [Link] [DOI:10.1016/j.labeco.2015.01.005]
11. Ribeiro IJS, Pereira R, Freire IV, de Oliveira BG, Casotti CA, Boer EN. Stress and quality of life among university students: a systematic literature review. Health Prof Educ. 2018;4(2):70-7. [Link] [DOI:10.1016/j.hpe.2017.03.002]
12. World Health Organization. Social determinants of mental health. Geneva: World Health Organization; 2014. [Link]
13. Lazarus RS, Folkma S. Stress, appraisal and coping. New York: Springer Publishing Company; 1984. [Link]
14. Frydenber E, Care E, Chan E, Freeman E. Interrelationships between coping, school connectedness and wellbeing. Aust J Educ. 2009;53(3):261-76. [Link] [DOI:10.1177/000494410905300305]
15. Lyubomirsky S, Sheldon K, Schkade D. Pursuing happiness: the architecture of sustainable change. Rev Gen Psychol. 2005;9(2):111-31. [Link] [DOI:10.1037/1089-2680.9.2.111]
16. Veenhoven R. Healthy happiness: effects of happiness on physical health and the consequences for preventive health care. J Happiness Stud. 2008;9:449-69. [Link] [DOI:10.1007/s10902-006-9042-1]
17. Cabanach RG, Souto-Gesta A, Franco V. Academic Stressors Scale for the evaluation of academic stressors in university student. Ibero Am J Psychol Health. 2016;7:41-50. [Spanish] [Link]
18. Freire C, Ferradas MDM, Valle A, Nuñez JC, Vallejo G. Profiles of psychological well-being and coping strategies among university students. Fron Psychol. 2016;7:1554. [Link] [DOI:10.3389/fpsyg.2016.01554]
19. Cameron LD, Jago L. Emotion regulation interventions: a common-sense model approach. Br J Health Psychol. 2008;13(Pt 2):215-21. [Link] [DOI:10.1348/135910708X288800]
20. Moyano-Díaz E, Páez D, Torres M. Psychometric properties of the questionnaire to measure strategies to increase happiness (HIS) in the Spanish version (CEA-EAP). Ter Psicol. 2016;34(2):143-54. [Link] [DOI:10.4067/S0718-48082016000200006]
21. Whitley M. Mental health and quality of life of graduate level therapy students :a look at the role of coping [dissertation]. Ottawa: University of Ottawa; 2018. [Link]
22. EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. [Link] [DOI:10.1016/0168-8510(90)90421-9]
23. Health Superintendence of Chile. Health related quality of life (HR-Qol) in Chilean general population [Internet]. Digital Library; 2006 [cited 2021 April 2] [Spanish]. Available from: Available from: https:// www.supersalud.gob.cl/documentacion/666/articles-3818_recurso_1.pdf [Link]
24. Hurst PN, Kind P, Ruta D, Hunter M, Stubbings A. Health-related quality of life in rheumatoid arthritis: validity, responsiveness and reliability of EuroQol (EQ-5D). Br J Rheumatol. 1997;36(5):551-9. [Link] [DOI:10.1093/rheumatology/36.5.551]
25. Herdman M, Badia X, Berra S. EuroQol-5D: a simple alternative for measuring health-related quality of life in primary care. Aten Primaria. 2001;28(6):425-30. [Spanish] [Link] [DOI:10.1016/S0212-6567(01)70406-4]
26. Olivares-Tirado P. Health related quality of life in Medicare beneficiaries: questionnaire validity of EQ-5D. Unknown city: Chilean Ministry of Health; 2005. [Spanish] [Link]
27. Faure M, Urquidi C, Bustamante F, Florenzano R, Ampuero K, Terán L, et al. Association between health life quality and suicidal risk in adolescents: a cross-sectional study. Rev Chil Pediatr. 2018;89(3):318-24. [Spanish] [Link]
28. Takch C, Lyubomirsky S. How do people pursue happiness?: relating personality, happiness-increasing strategies, and well-being. J Happiness Stud. 2006;7:183-225. [Link] [DOI:10.1007/s10902-005-4754-1]
29. Molina R, Sepúlveda R. Health related life quality in first year university students. Rev Chil Salud Pub. 2016;20(2):101-12. [Spanish] [Link] [DOI:10.5354/0719-5281.2016.44928]
30. Freire T, Ferreira G. Health-related quality of life of adolescents: relations with positive and negative psychological dimensions. Int J Adolesc Youth. 2018;23(1):11-24. [Link] [DOI:10.1080/02673843.2016.1262268]
31. Heise L, Greene M, Opper N, Stavropoulou M, Harper C, Nascimento M, et al. Gender inequality and restrictive gender norms: framing the challenges to health. Lancet. 2019;393:2440-54. [Link] [DOI:10.1016/S0140-6736(19)30652-X]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |