



Volume 10, Issue 3 (2022)
Health Educ Health Promot 2022, 10(3): 539-545 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Didehvar M, Arzani A, Dadkhah S, Ghanbarzehi V. Is It Necessary to Maintain Social Distancing during the COVID-19 Pandemic? An Assessment of Students’ Knowledge, Attitude, and Practice. Health Educ Health Promot 2022; 10 (3) :539-545
URL: http://hehp.modares.ac.ir/article-5-58890-en.html
URL: http://hehp.modares.ac.ir/article-5-58890-en.html

1- “Department of Public Health, School of Public Health and Allied Medical Sciences,” and “Tropical and Communicable Disease Research Center”, Iranshah University of Medical Sciences, Iranshahr, Iran
2- Tropical and Communicable Diseases Research Center, Iranshahr University of Medical Science, Iranshahr, Iran
3- “Department of Nursing, School of Medicine,” and “Tropical and Communicable Diseases Research Center”, Iranshahr University of Medical Sciences, Iranshahr, Iran
2- Tropical and Communicable Diseases Research Center, Iranshahr University of Medical Science, Iranshahr, Iran
3- “Department of Nursing, School of Medicine,” and “Tropical and Communicable Diseases Research Center”, Iranshahr University of Medical Sciences, Iranshahr, Iran
Keywords: Knowledge [MeSH], Attitude [MeSH], Professional Practice [MeSH], Physical Distancing [MeSH], COVID-19 [MeSH]
Full-Text [PDF 499 kb]
(2923 Downloads)
| Abstract (HTML) (1746 Views)
Table 2) Frequency distribution of answers to questions about awareness of social distance

Table 3) Frequency distribution of answers to questions about the attitude toward social distance
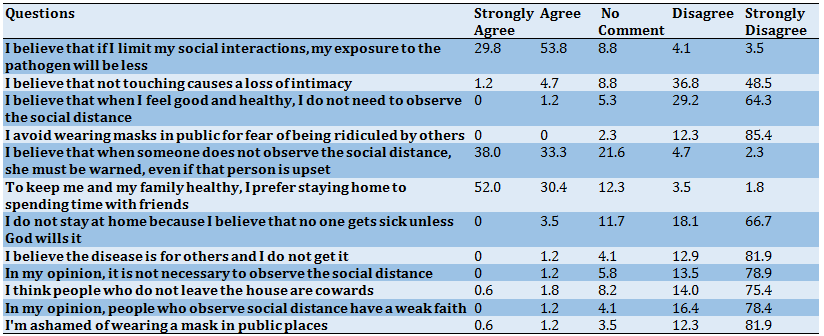
Table 4) Frequency distribution of answers to questions about social distance practice

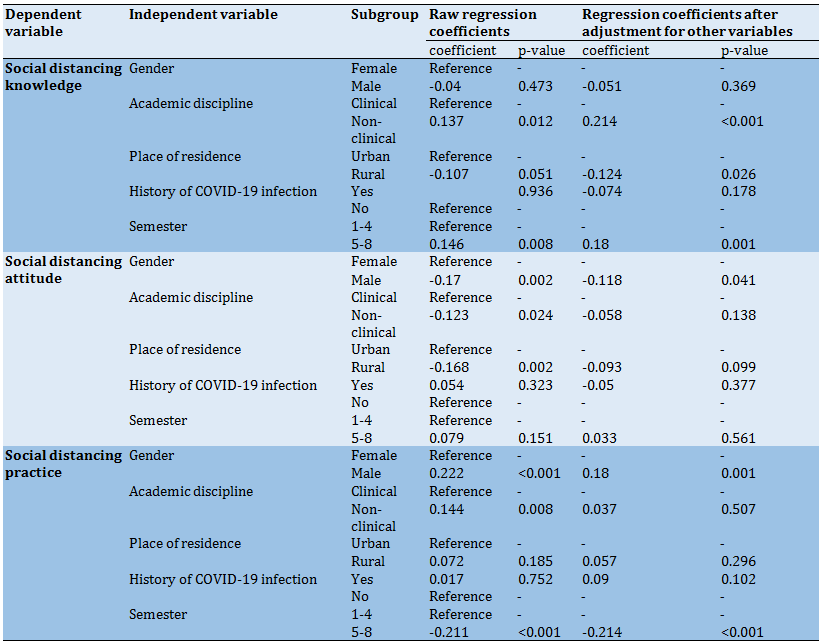
Table 5) Regression coefficients estimated for the relationship between social distancing knowledge, Attitude, and Practice with independent variables in linear regression
Discussion
The goal of this study was to examine the knowledge of social distancing, attitude towards social distancing, and degree of practicing social distancing in the students of Iranshahr University of Medical Sciences. In this study, 96.8% of the surveyed students earned a good score in social distancing knowledge and 76% of them earned a good score in attitude towards social distancing, but only 0.6% of them earned a good score in the area of social distancing practice. Our findings showed that although most students had an acceptable level of social distancing knowledge and an acceptable attitude towards social distancing, this was not well reflected in how they practiced social distancing. Unlike the present study, a 2020 study by Lammers et al. in the United States showed a relationship between people’s knowledge of the nature of the coronavirus and their acceptance of social distancing rules [16]. However, like our study, a study conducted by Reiger on German students showed that while the surveyed students had an average level of knowledge and a relatively good attitude (69%), their commitment to social distancing rules was far lower, a trend that they attributed to conspiracy theories and politicians’ views on the subject [14]. In a 2020 study carried out by Taghrir et al. on Iranian medical students, there was an inverse relationship between the perceived risk of the disease and practice [17]. Gibson et al. reported a decline in people’s commitment to preventive behaviors despite an improvement in their attitudes over time [18].
In the present study, we found a significant relationship between the students’ social distancing practice scores and how advanced they were in their education (semester). More specifically, students who were in their 5th to 8th semesters had lower social distancing practice scores than those in their 1st to 4th semesters. The first reason for the poor practice scores of more senior students could be that they mostly live in dormitories near where they are undergoing internships, and people who live in dormitories tend to be generally less compliant with protocols. The second reason could be the age range of less senior students (19-24 years), because, according to Erikson’s psychosocial development theory, these students are in the fifth and sixth stages of psychosocial development, where peers and friends play a key role in the formation of personality and behavior [19]. This difference may also be related to the poor performance of the government and policymakers in containing the pandemic.
Our findings showed a significant relationship between the social distancing knowledge of the students and whether they were studying in a clinical or non-clinical field, as students in the non-clinical group earned higher knowledge scores. This is inconsistent with the findings of a study by Ikhlaq et al. on the knowledge and attitude of Pakistani students regarding the coronavirus, which showed a higher level of knowledge among nursing students than among public health students [20]. Yang et al. also reported a higher level of knowledge among clinical medical students than among students of fundamental sciences [21]. However, like our study, Modi et al. also observed a higher level of knowledge about quarantine conditions among non-clinical students than among clinical students [22]. This is perhaps because most non-clinical students surveyed in this study have been attending virtual classes from their homes and thus have been more exposed to general information about the disease and its implications on account of having extra leisure time.
We also observed a significant relationship between the social distancing knowledge of the students and their place of residence, as the students living in urban areas had higher knowledge than those residing in rural areas. In a study by Shehata et al., urban students earned a higher score in the knowledge of preventive behaviors, but there was no significant difference between urban and rural students in terms of knowledge of clinical manifestations of COVID-19 infection [23]. White et al. also reported a higher level of knowledge among people living in urban areas than those living in rural areas [24]. This could be due to lower access in rural areas to the Internet and mobile phone networks, which results in lower engagement with social networks and online media and therefore lower access to information about the pandemic.
The findings of the present study also showed a significant relationship between the social distancing knowledge of students and their semester (their advancement in their education), as more senior students had more knowledge of the subject. This is consistent with the findings of Ikhlaq et al. [20]. This difference in knowledge level could be because many of the more senior students have been attending hospitals and medical centers, which has given them more opportunities to gain better information about the virus, and also because they are more adept at gathering reliable information from the Internet and other sources.
Statistical analyses of this study showed a significant relationship between gender and social distancing practice and also between gender and attitude towards social distancing. More specially, female students earned higher attitude scores than male students, which is consistent with the findings of An et al. regarding the more positive attitude of women toward social distancing [25].
Despite having a less desirable attitude toward social distancing, male students in our study earned higher scores in social distancing practice than female students. This is inconsistent with the findings of a by study Li et al., where they used the health belief model to measure the commitment of student pharmacists to preventive behaviors like social distancing and ultimately reported that female students earned better scores than male students [26]. A study by Nasirzadeh et al. on the knowledge of COVID-19 and attitude toward it also reported a higher rate of preventive behaviors in women than men, which was attributed to women acting more responsibly toward their health and that of their family members [27]. The reason for the difference between our findings and previous reports in this regard could be our research method, as students’ self-reports may not reflect their actual behavior.
The present study had several limitations, which need to be acknowledged. First, since the study was web-based, it is likely that poor internet access, which is particularly prevalent in rural areas of Iranshahr, has acted as a limiting factor. Also, since the study was conducted on medical students, the findings cannot be generalized to larger populations. Another limitation of this study was the use of voluntary sampling, which can affect the generalizability of the results. Lastly, since the study was reliant on the students’ self-reports, the results may not reflect the reality of the situation. Future studies are recommended to investigate the factors that influence students’ compliance with social distancing rules using a random sampling method.
Conclusion
While the surveyed students showed a good level of social distancing knowledge and a good attitude towards social distancing, they earned comparatively lower social distancing practice scores, which is indicative of inadequate compliance with social distancing rules. Also, clinical students showed a lower level of social distancing knowledge than non-clinical students. These findings highlight the need to improve the COVID-19-related knowledge of clinical students as an important part of our medical community and also to find why the students’ good knowledge and attitude do not translate into an equally good commitment to practice preventive behaviors.
Acknowledgments: We would like to express our gratitude to the staff of this university for supporting this research and also thank the participating students for their contribution.
Ethical Permissions: This article was approved by Iranshahr University of Medical Sciences with the ethics code IR.IRSHUMS.REC.1399.013.
Conflict of Interests: This article was derived from a research project approved and supported by Iranshahr University of Medical Sciences.
Authors’ Contributions: Didehvar M (First Author), Introduction Writer/Methodologist (30%); Arzani A (Second Author), Introduction Writer/Statistical Analyst (30%); Dadkhah S (Third Author), Methodologist/ Discussion writer (30%); Ghanbarzehi V (Forth Author) Discussion Writer (10%)
Funding/Supports: This study was supported financially by Iranshahr University of Medical Sciences, Iranshahr, Iran
Full-Text: (381 Views)
Introduction
The World Health Organization (WHO) has recognized the COVID-19 pandemic as global public health concern since early 2020 [1]. According to WHO, as of September 10, 2021, the virus has affected 223,022,538 people, of whom 4,602,882 have died. In Iran, the number of positive cases has been 5,237,799 and the death toll has been 112,935 by September 10, 2021 [2].
Human-to-human transmission of COVID-19 takes place through coughing, sneezing, and nasal and oral discharge. The virus can be transmitted through coughs or sneezes at a distance of 1 to 2 meters [3]. Considering the high spread rate of COVID-19 [4] and the lack of a definitive cure for the disease, most countries have chosen to concentrate on preventive tactics such as quarantine, social distancing, and social containment to control the pandemic [5]. The best way to avoid this disease is to observe social distancing, which involves staying at home as much as possible, limiting social contacts, and wearing protective masks in public [6, 7]. Maintaining a physical distance of 1 to 2 meters from other people can be highly effective in preventing COVID-19 transmission [8].
According to a study by Price, the social distancing policy is indeed effective in reducing the spread of the disease [9]. In a study carried out by Rahmanian et al. on the students of Jahrom University of Medical Sciences (Jahrom, Iran), the students had above-average mean scores in knowledge, attitude, and practice regarding COVID-19 [10]. A 2020 study by Kayes et al. on the attitude of Australians towards social distancing found that 80% of subjects had a positive attitude towards the issue, showing that the practice is widely accepted by this population [11]. It has been shown that occupational status and living conditions tend to have an impact on people’s attitudes toward social distancing [12]. People’s knowledge of, attitude towards, and commitment to preventive behaviors are all highly important in the fight against infectious diseases like COVID-19 [13]. Since young people and especially university students are highly active and social, their attitude toward social distancing can play a key role in controlling the pandemic [14, 15].
In areas where vaccination programs progress slowly, social distancing remains the most effective tool for preventing new cases. In Iran, like in many other countries, despite pressure from the government and the adoption of laws in support of social distancing rules, a large number of people refuse to comply with these rules. Since almost all medical students frequently share COVID-19-related reports and information with their families, they can play a significant role in conveying accurate health information to the population. The goal of this study was to measure the social distancing of knowledge, attitude, and practice in medical students.
Instrument and Methods
The study was designed as descriptive cross-sectional research and was conducted From September 2020 to August 2021 after receiving approval from the research and technology department of Iranshahr University of Medical Sciences. Sampling was performed using the availability sampling method. Using Cochran's formula with a 5% error probability, the appropriate sample size was determined to be 342. The only inclusion criterion was being a student at Iranshahr University of Medical Sciences. The questionnaires that were not incompletely filled out were excluded from the study. Ultimately, 342 of the returned questionnaires were found to be eligible for inclusion in the study.
The research tool was a researcher-made online questionnaire prepared using the Porsline survey service consisting of four sections: demographic characteristics, social distancing knowledge, attitude towards social distancing, and social distancing practice. The first section of the questionnaire contained questions about demographic characteristics including age, gender, education level, academic discipline, semester, and place of residence, and also the history of COVID-19 infection (the respondent or their relatives). The second section of the questionnaire consisted of 12 items measuring students’ attitudes towards social distancing on the five-point Likert scale with scores ranging from 1 to 5 (completely disagree, disagree, disagree, agree, completely agree). The total score of this section was between 12 and 60, with scores below 28 taken as the indication of poor attitude, scores between 28 and 46 taken as the indication of moderate attitude, and scores over 46 taken as the indication of a good attitude. In the third section, students’ knowledge of social distancing was measured by seven 3-choice questions (yes, no, and I do not know), with each correct answer given a score of 1. The total score of this section was between 0 and 7, with scores below or equal to 3 interpreted as poor knowledge, and scores above 3 interpreted as adequate knowledge. In the fourth section, social distancing practice was measured by seven questions on the five-point Likert scale with scores ranging from 1 to 5 (always, often, sometimes, rarely, never). In this section, the total score was between 7 and 35, with scores below 16 taken as the indication of a low level of social distancing practice, scores between 16 and 25 taken as the indication of a moderate level of social distancing practice, and scores above 25 taken as the indication of a high level of social distancing practice. The validity of the questionnaire was established through content and face validity assessment. To assess content validity, the questionnaire was reviewed by five of the university’s faculty members, who were asked to comment on its relevance, clarity, and simplicity. Using this method, the content validity index of the entire tool was determined to be 86%. To assess face validity, while assessing content validity, the consulted experts were also asked to comment on the items of the questionnaire and some of the items were modified according to their inputs. To evaluate the reliability of the questionnaire, it was administered to 20 medical students. Using this method, the reliability of the knowledge, attitude, and practice sections of the questionnaire was established with Cronbach’s alphas of 87%, 85%, and 86%, respectively.
After receiving approval from the university’s ethics committee, the online link of the questionnaire was provided to eligible subjects both individually and publicly through social networking groups with the help of the secretary of the student :union: council. The response rate was 95% (5% of the participants were excluded because of not fill out the questionnaire completely). The data collection period was from April 20 to May 20, 2021.
Data analysis was performed in SPSS version 16 using descriptive measures (mean and standard deviation) and linear regression. In all statistical tests, the significance level was 0.05.
Findings
Out of 342 subjects, 222 (64.9%) were female and 120 (35.1%) were male. The mean age of the students was 21.56±2.112. Out of 342 students, 228 (84.2%) were single and 290 (84.8%) were living in urban areas. Other demographic information about the students was provided in Table 1.
Table 1) Frequency distribution of the students in terms of demographic variables (N=342)
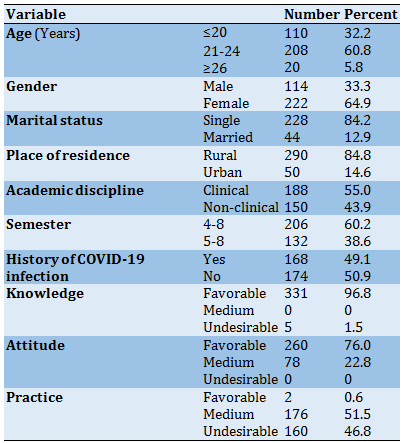
For better analysis, the students were divided into two subgroups in terms of their academic discipline: clinical (medicine, operating room, anesthesia, emergency, midwifery, and nursing) and non-clinical (public health, occupational health, environmental health, and laboratory sciences). The students were also divided into two subgroups in terms of how advanced they were in their education: 1-4 (people in their first to fourth semesters) and 5-8 (people in their fifth to eighth semesters).
Since there were less than 5% missing data for gender, marital status, place of residence, academic discipline, and semester, imputation was not performed. The total social distancing knowledge, attitude and practice scores of the students were in the ranges of 3 to 7, 33 to 56, and 9 to 26, respectively. The median social distancing knowledge, attitude, and practice scores were 6±1, 48±4, and 16±3, respectively. The median and IQR of the social distancing knowledge scores of the students was 6±1. About 77.8% of the students defined social distancing as maintaining at least 2 meters distance from other people, 43.9% of them stated that smart distancing is equal to re-activation of jobs with a low risk of coronavirus exposure, 78.4% of them believed that social distancing is the most effective way to reduce the transmission of the disease, 95.6% of them believed that the virus can be transmitted from asymptomatic and seemingly healthy people, 95% of them believed that people of all ages can be infected with the virus, 86% of them believed that hand washing and wearing mask alone do not provide complete protection against the disease, and 92% of them stated that social distancing is to keep distance from everyone (sick and non-sick). The median and IQR of the social distancing attitude scores of the students was 48±4. Approximately 29.8% of the students believed that limiting social contacts and relationships would reduce exposure to the virus, 38% of them believed that people who do not observe social distancing rules should be asked to do so, and 52% of them stated that to protect the health of their family, they prefer to avoid social gatherings and stay at home.
The median and IQR of the social distancing practice scores of the students was 16 ±3. About 27.5% of the students stated they leave home only when necessary, 82.5% of them stated that they always use masks in public and crowded places, 15.8% of them stated that they always confront people who do not observe social distancing rules, 22.2% of them stated that they do not attend social gatherings, 43.9% of them stated that they stay home despite limited entertainment options available, and 49.7% of them stated that they always avoid shaking hands with others.
The social distancing knowledge, attitude, and practice of the students were analyzed using the quantitative part of the data (total score of each section of the questionnaire). Considering the frequency distribution of the data for gender, academic discipline, semester, and place of residence, it was decided to use the following subgroups as the reference: female, clinical, 1-4 semester, and urban (Tables 2-4).
In the linear regression analysis, simple linear regression (bivariate) was used to estimate the raw regression coefficients (for the relationship between independent variables and dependent variables), and multiple linear regression (multivariate) was used to estimate the adjusted regression coefficients. The raw regression coefficients estimated for social distancing knowledge indicated statistical significance for the variables of academic discipline and semester. For social distancing attitude, the estimated raw regression coefficients showed statistical significance for the variables gender, place of residence, and academic discipline. The raw regression coefficients estimated for social distancing practice showed statistical significance for the variables gender, academic discipline, and semester (Table 5).
The World Health Organization (WHO) has recognized the COVID-19 pandemic as global public health concern since early 2020 [1]. According to WHO, as of September 10, 2021, the virus has affected 223,022,538 people, of whom 4,602,882 have died. In Iran, the number of positive cases has been 5,237,799 and the death toll has been 112,935 by September 10, 2021 [2].
Human-to-human transmission of COVID-19 takes place through coughing, sneezing, and nasal and oral discharge. The virus can be transmitted through coughs or sneezes at a distance of 1 to 2 meters [3]. Considering the high spread rate of COVID-19 [4] and the lack of a definitive cure for the disease, most countries have chosen to concentrate on preventive tactics such as quarantine, social distancing, and social containment to control the pandemic [5]. The best way to avoid this disease is to observe social distancing, which involves staying at home as much as possible, limiting social contacts, and wearing protective masks in public [6, 7]. Maintaining a physical distance of 1 to 2 meters from other people can be highly effective in preventing COVID-19 transmission [8].
According to a study by Price, the social distancing policy is indeed effective in reducing the spread of the disease [9]. In a study carried out by Rahmanian et al. on the students of Jahrom University of Medical Sciences (Jahrom, Iran), the students had above-average mean scores in knowledge, attitude, and practice regarding COVID-19 [10]. A 2020 study by Kayes et al. on the attitude of Australians towards social distancing found that 80% of subjects had a positive attitude towards the issue, showing that the practice is widely accepted by this population [11]. It has been shown that occupational status and living conditions tend to have an impact on people’s attitudes toward social distancing [12]. People’s knowledge of, attitude towards, and commitment to preventive behaviors are all highly important in the fight against infectious diseases like COVID-19 [13]. Since young people and especially university students are highly active and social, their attitude toward social distancing can play a key role in controlling the pandemic [14, 15].
In areas where vaccination programs progress slowly, social distancing remains the most effective tool for preventing new cases. In Iran, like in many other countries, despite pressure from the government and the adoption of laws in support of social distancing rules, a large number of people refuse to comply with these rules. Since almost all medical students frequently share COVID-19-related reports and information with their families, they can play a significant role in conveying accurate health information to the population. The goal of this study was to measure the social distancing of knowledge, attitude, and practice in medical students.
Instrument and Methods
The study was designed as descriptive cross-sectional research and was conducted From September 2020 to August 2021 after receiving approval from the research and technology department of Iranshahr University of Medical Sciences. Sampling was performed using the availability sampling method. Using Cochran's formula with a 5% error probability, the appropriate sample size was determined to be 342. The only inclusion criterion was being a student at Iranshahr University of Medical Sciences. The questionnaires that were not incompletely filled out were excluded from the study. Ultimately, 342 of the returned questionnaires were found to be eligible for inclusion in the study.
The research tool was a researcher-made online questionnaire prepared using the Porsline survey service consisting of four sections: demographic characteristics, social distancing knowledge, attitude towards social distancing, and social distancing practice. The first section of the questionnaire contained questions about demographic characteristics including age, gender, education level, academic discipline, semester, and place of residence, and also the history of COVID-19 infection (the respondent or their relatives). The second section of the questionnaire consisted of 12 items measuring students’ attitudes towards social distancing on the five-point Likert scale with scores ranging from 1 to 5 (completely disagree, disagree, disagree, agree, completely agree). The total score of this section was between 12 and 60, with scores below 28 taken as the indication of poor attitude, scores between 28 and 46 taken as the indication of moderate attitude, and scores over 46 taken as the indication of a good attitude. In the third section, students’ knowledge of social distancing was measured by seven 3-choice questions (yes, no, and I do not know), with each correct answer given a score of 1. The total score of this section was between 0 and 7, with scores below or equal to 3 interpreted as poor knowledge, and scores above 3 interpreted as adequate knowledge. In the fourth section, social distancing practice was measured by seven questions on the five-point Likert scale with scores ranging from 1 to 5 (always, often, sometimes, rarely, never). In this section, the total score was between 7 and 35, with scores below 16 taken as the indication of a low level of social distancing practice, scores between 16 and 25 taken as the indication of a moderate level of social distancing practice, and scores above 25 taken as the indication of a high level of social distancing practice. The validity of the questionnaire was established through content and face validity assessment. To assess content validity, the questionnaire was reviewed by five of the university’s faculty members, who were asked to comment on its relevance, clarity, and simplicity. Using this method, the content validity index of the entire tool was determined to be 86%. To assess face validity, while assessing content validity, the consulted experts were also asked to comment on the items of the questionnaire and some of the items were modified according to their inputs. To evaluate the reliability of the questionnaire, it was administered to 20 medical students. Using this method, the reliability of the knowledge, attitude, and practice sections of the questionnaire was established with Cronbach’s alphas of 87%, 85%, and 86%, respectively.
After receiving approval from the university’s ethics committee, the online link of the questionnaire was provided to eligible subjects both individually and publicly through social networking groups with the help of the secretary of the student :union: council. The response rate was 95% (5% of the participants were excluded because of not fill out the questionnaire completely). The data collection period was from April 20 to May 20, 2021.
Data analysis was performed in SPSS version 16 using descriptive measures (mean and standard deviation) and linear regression. In all statistical tests, the significance level was 0.05.
Findings
Out of 342 subjects, 222 (64.9%) were female and 120 (35.1%) were male. The mean age of the students was 21.56±2.112. Out of 342 students, 228 (84.2%) were single and 290 (84.8%) were living in urban areas. Other demographic information about the students was provided in Table 1.
Table 1) Frequency distribution of the students in terms of demographic variables (N=342)
For better analysis, the students were divided into two subgroups in terms of their academic discipline: clinical (medicine, operating room, anesthesia, emergency, midwifery, and nursing) and non-clinical (public health, occupational health, environmental health, and laboratory sciences). The students were also divided into two subgroups in terms of how advanced they were in their education: 1-4 (people in their first to fourth semesters) and 5-8 (people in their fifth to eighth semesters).
Since there were less than 5% missing data for gender, marital status, place of residence, academic discipline, and semester, imputation was not performed. The total social distancing knowledge, attitude and practice scores of the students were in the ranges of 3 to 7, 33 to 56, and 9 to 26, respectively. The median social distancing knowledge, attitude, and practice scores were 6±1, 48±4, and 16±3, respectively. The median and IQR of the social distancing knowledge scores of the students was 6±1. About 77.8% of the students defined social distancing as maintaining at least 2 meters distance from other people, 43.9% of them stated that smart distancing is equal to re-activation of jobs with a low risk of coronavirus exposure, 78.4% of them believed that social distancing is the most effective way to reduce the transmission of the disease, 95.6% of them believed that the virus can be transmitted from asymptomatic and seemingly healthy people, 95% of them believed that people of all ages can be infected with the virus, 86% of them believed that hand washing and wearing mask alone do not provide complete protection against the disease, and 92% of them stated that social distancing is to keep distance from everyone (sick and non-sick). The median and IQR of the social distancing attitude scores of the students was 48±4. Approximately 29.8% of the students believed that limiting social contacts and relationships would reduce exposure to the virus, 38% of them believed that people who do not observe social distancing rules should be asked to do so, and 52% of them stated that to protect the health of their family, they prefer to avoid social gatherings and stay at home.
The median and IQR of the social distancing practice scores of the students was 16 ±3. About 27.5% of the students stated they leave home only when necessary, 82.5% of them stated that they always use masks in public and crowded places, 15.8% of them stated that they always confront people who do not observe social distancing rules, 22.2% of them stated that they do not attend social gatherings, 43.9% of them stated that they stay home despite limited entertainment options available, and 49.7% of them stated that they always avoid shaking hands with others.
The social distancing knowledge, attitude, and practice of the students were analyzed using the quantitative part of the data (total score of each section of the questionnaire). Considering the frequency distribution of the data for gender, academic discipline, semester, and place of residence, it was decided to use the following subgroups as the reference: female, clinical, 1-4 semester, and urban (Tables 2-4).
In the linear regression analysis, simple linear regression (bivariate) was used to estimate the raw regression coefficients (for the relationship between independent variables and dependent variables), and multiple linear regression (multivariate) was used to estimate the adjusted regression coefficients. The raw regression coefficients estimated for social distancing knowledge indicated statistical significance for the variables of academic discipline and semester. For social distancing attitude, the estimated raw regression coefficients showed statistical significance for the variables gender, place of residence, and academic discipline. The raw regression coefficients estimated for social distancing practice showed statistical significance for the variables gender, academic discipline, and semester (Table 5).
Table 2) Frequency distribution of answers to questions about awareness of social distance
Table 3) Frequency distribution of answers to questions about the attitude toward social distance
Table 4) Frequency distribution of answers to questions about social distance practice
Table 5) Regression coefficients estimated for the relationship between social distancing knowledge, Attitude, and Practice with independent variables in linear regression
Discussion
The goal of this study was to examine the knowledge of social distancing, attitude towards social distancing, and degree of practicing social distancing in the students of Iranshahr University of Medical Sciences. In this study, 96.8% of the surveyed students earned a good score in social distancing knowledge and 76% of them earned a good score in attitude towards social distancing, but only 0.6% of them earned a good score in the area of social distancing practice. Our findings showed that although most students had an acceptable level of social distancing knowledge and an acceptable attitude towards social distancing, this was not well reflected in how they practiced social distancing. Unlike the present study, a 2020 study by Lammers et al. in the United States showed a relationship between people’s knowledge of the nature of the coronavirus and their acceptance of social distancing rules [16]. However, like our study, a study conducted by Reiger on German students showed that while the surveyed students had an average level of knowledge and a relatively good attitude (69%), their commitment to social distancing rules was far lower, a trend that they attributed to conspiracy theories and politicians’ views on the subject [14]. In a 2020 study carried out by Taghrir et al. on Iranian medical students, there was an inverse relationship between the perceived risk of the disease and practice [17]. Gibson et al. reported a decline in people’s commitment to preventive behaviors despite an improvement in their attitudes over time [18].
In the present study, we found a significant relationship between the students’ social distancing practice scores and how advanced they were in their education (semester). More specifically, students who were in their 5th to 8th semesters had lower social distancing practice scores than those in their 1st to 4th semesters. The first reason for the poor practice scores of more senior students could be that they mostly live in dormitories near where they are undergoing internships, and people who live in dormitories tend to be generally less compliant with protocols. The second reason could be the age range of less senior students (19-24 years), because, according to Erikson’s psychosocial development theory, these students are in the fifth and sixth stages of psychosocial development, where peers and friends play a key role in the formation of personality and behavior [19]. This difference may also be related to the poor performance of the government and policymakers in containing the pandemic.
Our findings showed a significant relationship between the social distancing knowledge of the students and whether they were studying in a clinical or non-clinical field, as students in the non-clinical group earned higher knowledge scores. This is inconsistent with the findings of a study by Ikhlaq et al. on the knowledge and attitude of Pakistani students regarding the coronavirus, which showed a higher level of knowledge among nursing students than among public health students [20]. Yang et al. also reported a higher level of knowledge among clinical medical students than among students of fundamental sciences [21]. However, like our study, Modi et al. also observed a higher level of knowledge about quarantine conditions among non-clinical students than among clinical students [22]. This is perhaps because most non-clinical students surveyed in this study have been attending virtual classes from their homes and thus have been more exposed to general information about the disease and its implications on account of having extra leisure time.
We also observed a significant relationship between the social distancing knowledge of the students and their place of residence, as the students living in urban areas had higher knowledge than those residing in rural areas. In a study by Shehata et al., urban students earned a higher score in the knowledge of preventive behaviors, but there was no significant difference between urban and rural students in terms of knowledge of clinical manifestations of COVID-19 infection [23]. White et al. also reported a higher level of knowledge among people living in urban areas than those living in rural areas [24]. This could be due to lower access in rural areas to the Internet and mobile phone networks, which results in lower engagement with social networks and online media and therefore lower access to information about the pandemic.
The findings of the present study also showed a significant relationship between the social distancing knowledge of students and their semester (their advancement in their education), as more senior students had more knowledge of the subject. This is consistent with the findings of Ikhlaq et al. [20]. This difference in knowledge level could be because many of the more senior students have been attending hospitals and medical centers, which has given them more opportunities to gain better information about the virus, and also because they are more adept at gathering reliable information from the Internet and other sources.
Statistical analyses of this study showed a significant relationship between gender and social distancing practice and also between gender and attitude towards social distancing. More specially, female students earned higher attitude scores than male students, which is consistent with the findings of An et al. regarding the more positive attitude of women toward social distancing [25].
Despite having a less desirable attitude toward social distancing, male students in our study earned higher scores in social distancing practice than female students. This is inconsistent with the findings of a by study Li et al., where they used the health belief model to measure the commitment of student pharmacists to preventive behaviors like social distancing and ultimately reported that female students earned better scores than male students [26]. A study by Nasirzadeh et al. on the knowledge of COVID-19 and attitude toward it also reported a higher rate of preventive behaviors in women than men, which was attributed to women acting more responsibly toward their health and that of their family members [27]. The reason for the difference between our findings and previous reports in this regard could be our research method, as students’ self-reports may not reflect their actual behavior.
The present study had several limitations, which need to be acknowledged. First, since the study was web-based, it is likely that poor internet access, which is particularly prevalent in rural areas of Iranshahr, has acted as a limiting factor. Also, since the study was conducted on medical students, the findings cannot be generalized to larger populations. Another limitation of this study was the use of voluntary sampling, which can affect the generalizability of the results. Lastly, since the study was reliant on the students’ self-reports, the results may not reflect the reality of the situation. Future studies are recommended to investigate the factors that influence students’ compliance with social distancing rules using a random sampling method.
Conclusion
While the surveyed students showed a good level of social distancing knowledge and a good attitude towards social distancing, they earned comparatively lower social distancing practice scores, which is indicative of inadequate compliance with social distancing rules. Also, clinical students showed a lower level of social distancing knowledge than non-clinical students. These findings highlight the need to improve the COVID-19-related knowledge of clinical students as an important part of our medical community and also to find why the students’ good knowledge and attitude do not translate into an equally good commitment to practice preventive behaviors.
Acknowledgments: We would like to express our gratitude to the staff of this university for supporting this research and also thank the participating students for their contribution.
Ethical Permissions: This article was approved by Iranshahr University of Medical Sciences with the ethics code IR.IRSHUMS.REC.1399.013.
Conflict of Interests: This article was derived from a research project approved and supported by Iranshahr University of Medical Sciences.
Authors’ Contributions: Didehvar M (First Author), Introduction Writer/Methodologist (30%); Arzani A (Second Author), Introduction Writer/Statistical Analyst (30%); Dadkhah S (Third Author), Methodologist/ Discussion writer (30%); Ghanbarzehi V (Forth Author) Discussion Writer (10%)
Funding/Supports: This study was supported financially by Iranshahr University of Medical Sciences, Iranshahr, Iran
Article Type: Descriptive & Survey |
Subject:
Social Health
Received: 2022/01/22 | Accepted: 2022/04/9 | Published: 2022/07/17
Received: 2022/01/22 | Accepted: 2022/04/9 | Published: 2022/07/17
References
1. Adhikari SP, Meng S, Wu YJ, Mao YP, Ye RX, Wang QZ, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. 2020;9(29):1-12. [Link] [DOI:10.1186/s40249-020-00646-x]
2. WHO. WHO Coronavirus (COVID-19) dashboard [Internet]. Geneva: WHO; 2020 [Cited 2021 Jan 1]. Available from: https://covid19.who.int/ [Link]
3. Ben Abdel Ouahab I, Elaachak L, Elouaai F, Bouhorma M, editors. A smart surveillance prototype ensures the respect of social distance during COVID-19. Cham: Springer International Publishing; 2021 [Link] [DOI:10.1007/978-3-030-66840-2_91]
4. Bakhshi Mofrad Kashani A, Asalani Mehr M, Abedi Elkhichi P. Challenges of laboratory sampling and diagnosis of SARS-Cov-2 virus of disease (COVID-19). Stud Med Sci. 2021;32(3):156-74. [Persian] [Link]
5. Ebrahimi M, Khodabakhshian Z, Reihani HR, Habibzadeh SR, Rezaiyan MK, Kalani N, et al. Evaluation of awareness, attitude, and practice of residents in Mashhad towards new Coronavirus disease 2019 in 2020. NAVIDNO. 2021;24(77):69-83. [Persian] [Link]
6. Chen S, Yang J, Yang W, Wang C, Bärnighausen T. COVID-19 control in China during mass population movements at new year. Lancet. 2020;395(10226):764-6. [Link] [DOI:10.1016/S0140-6736(20)30421-9]
7. Rosmana T, Chasiotisa A, Kerwera M, Steinmetza H, Oliver, Wedderhoffa, et al. Will COVID-19-related economic worries superimpose the health worries, reducing acceptance of social distancing measures? A prospective pre-registered study. Int J Psychol. 2021;56(4):607-22. [Link] [DOI:10.1002/ijop.12753]
8. Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973-87. [Link] [DOI:10.1016/S0140-6736(20)31142-9]
9. Price G, van Holm E. The effect of social distancing on the early spread of the novel coronavirus. Soc Sci Q. 2021;102(5):2331-40. [Link] [DOI:10.1111/ssqu.12988]
10. Rahmanian M, Dorodchi A, Zarenezhad M, Hatami N, Javdani F, Kalani N. Knowledge, attitude and practice of students of Jahrom University of Medical Sciences to the new coronavirus (COVID-19). Med J Mashhad Univ Med Sci. 2021;63(3):2359-69. [Persian] [Link]
11. Kayes ASM, Islam MS, Watters PA, Ng A, Kayesh H. Automated measurement of attitudes towards social distancing using social media: a COVID-19 case study. First Monday. 25(11). [Link]
12. Matthews VS, Stough-Hunter A, Marazita JM. Attitudes towards social distancing in response to COVID-19. Public health nursing (Boston, Mass). Public Health Nurs. 2021;38(6):1019-29. [Link] [DOI:10.1111/phn.12954]
13. Yakar B, Kaygusuz TÖ, Pirinçci E, Önalan E, Ertekin YH. Knowledge, attitude and anxiety of medical students about the current COVID-19 outbreak in Turkey. Fam Pract Palliat Care. 2020;5(2):36-44. [Link] [DOI:10.22391/fppc.737469]
14. Rieger MO. What makes young people think positively about social distancing during the corona crisis in Germany?. Front Sociol. 2020;5:61. [Link] [DOI:10.3389/fsoc.2020.00061]
15. Karimi R. Easy statistical analysis guide with SPSS. Tehran: Hengam; 2017. [Persian] [Link]
16. Lammers J, Crusius J, Gast A. Correcting misperceptions of exponential coronavirus growth increases support for social distancing. Proc Natl Acad Sci. 2020;117(28):16264-6. [Link] [DOI:10.1073/pnas.2006048117]
17. Taghrir MH, Borazjani R, Shiraly R. COVID-19 and Iranian medical students; a survey on their related-knowledge, preventive behaviors and risk perception. Arch Iranian Med. 2020;23(4):249-54. [Persian] [Link] [DOI:10.34172/aim.2020.06]
18. Gibson LP, Magnan RE, Kramer EB, Bryan AD. Theory of planned behavior analysis of social distancing during the COVID-19 pandemic: focusing on the intention-behavior gap. Ann Behav Med. 2021;55(8):805-12. [Link] [DOI:10.1093/abm/kaab041]
19. Saffari M, Shogaeizadeh D, Ghofranipoor F, Heidarnia A, Pakpour Haji Agha A. Health education & promotion theories, models & methods. Tehran: Asar Sobhan; 2010. [Persian] [Link]
20. Ikhlaq A, Bint-E-Riaz H, Bashir I, Ijaz F. Awareness and attitude of undergraduate medical students towards 2019-novel Corona virus. Pak J Med Sci. 2020;36(COVID19-S4):S32-6. [Link] [DOI:10.12669/pjms.36.COVID19-S4.2636]
21. Yang H, Zheng Y, Yu F, Cheng B, Zhu Z, Liao S, et al. Knowledge, attitudes, and social responsiveness toward Corona virus disease 2019 (COVID-19) among Chinese medical students-thoughts on medical education. Front Med. 2021;8:647679. [Link] [DOI:10.3389/fmed.2021.647679]
22. Modi PD, Nair G, Uppe A, Janhavi Modi, Tuppekar B, Gharpure AS, et al. COVID-19 awareness among healthcare students and professionals in Mumbai metropolitan region: a questionnaire-based survey. Cureus. 2020;12(4):e7514. [Link] [DOI:10.7759/cureus.7514]
23. Shehata MA, Adel A, Armaneous AF, EL-Sonbaty MM, Atti MA, El‑Hariri HM, et al. Egyptian school children awareness and precautions in COVID-19 pandemic: a cross sectional survey study. Bull Natl Res Cent. 2021;45(1):39. [Link] [DOI:10.1186/s42269-021-00495-0]
24. White S, Omer M, Mohamma GN. Knowledge, attitude and practice on prevention of airborne and droplet infections during the outbreak of corona virus among the college students in University of Bisha, Saudi Arabia. Int J Contemporary Res Rev. 2020;11:20773-6. [Link]
25. An L, Hawley S, van Horn ML, Bacon E, Yang P, Resnicow K. Development of a coronavirus social distance attitudes scale. Patient Educ Couns. 2021;104(6):1451-9. [Link] [DOI:10.1016/j.pec.2020.11.027]
26. Li M, Lv G, Hsieh S, Shao R, Yuan J. Pandemic worry and preventive health behaviors during the COVID-19 outbreak. Front Med. 2021;8:879. [Link] [DOI:10.3389/fmed.2021.700072]
27. Nasirzadeh M, Aligol M. Assessmentof knowledge, attitude, and factors associated with the preventive behaviors of COVID-19 in Qom, Iran, in 2020. Qom Univ Med Sci J. 2020;14(7):50-7. [Persian] [Link] [DOI:10.29252/qums.14.7.50]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |