



Volume 10, Issue 4 (2022)
Health Educ Health Promot 2022, 10(4): 763-769 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Purabdollah M, Mokhtari M, Moghadam Tabrizi F, Khorami Markani A, Emami S. Correlation of Nurses' Social Responsibility with the Missed Nursing Care. Health Educ Health Promot 2022; 10 (4) :763-769
URL: http://hehp.modares.ac.ir/article-5-58461-en.html
URL: http://hehp.modares.ac.ir/article-5-58461-en.html
1- Department of Nursing, Faculty of Nursing, Khoy University of Medical Sciences, Khoy, Iran
2- Department of Midwifery, Faculty of Nursing and Midwifery, Urmia University of Medical Sciences, Urmia, Iran
2- Department of Midwifery, Faculty of Nursing and Midwifery, Urmia University of Medical Sciences, Urmia, Iran
Keywords: Nurses [MeSH], Nursing Care [MeSH], Patient Safety [MeSH], Social Responsibility [MeSH], Iran [MeSH]
Full-Text [PDF 797 kb]
(1398 Downloads)
| Abstract (HTML) (1064 Views)
Full-Text: (436 Views)
Introduction
Patient safety is one of the most important issues in nursing care and is a professional concern of all those involved in patient care to ensure the quality of patient's safety care before incidents [1]. Nursing care is a main component of health care services as a priority in the health care system. In many countries, the quality of nursing care is considered as an important indicator in the validation and ranking of health centers, which should be considered to maximize profits with minimal harm to patients [2]. Therefore, improving the quality of health care is one of the main concerns of health service providers. In this regard, one of the goals of the health care organization is to prevent injury and harm to the patient, to ensure the safety of the patient's health, and as a result, to provide high-quality health services [3].
Missed nursing care is a new concept in nursing, and any delay in caring is defined as the removal of all or part of nursing care, which is also referred to as a nursing mistake or error [4]. Nurses' faults are heavy and in most cases irreparable. Nowadays, nurses independently examine and diagnose patient problems, plan, execute and evaluate nursing measures in the nursing process, and assume the responsibility and legal responsibility for these actions [5]. Misdiagnosis, nursing practices in the wrong place, using the false techniques, delayed diagnosis, inadequate diagnosis, hospital infections, falling in the patient, subcutaneous wounds, and misconceptions are nursing errors [6]. Unfortunately, many of these errors are not reported. Missed nursing care is a global phenomenon, and some aspects of nursing care are missed, and its prevalence varies from country to country [7]. Based on the available evidence, it is estimated that in developing countries, one in 10 people will be injured while receiving hospital services [8]. The results of some studies in this area indicate a high prevalence of neglected nursing care among nurses with a prevalence between 15-98% [9, 10], and more than 70% in the Kalisch et al.’s study, which these estimates are alarming for healthcare systems, health policy-makers, and service providers [4].
The misse of nursing care has undesirable effects, including increasing patient dissatisfaction, reducing patient safety [11], increasing nurses' workload, increasing nurses' job turnover, reducing job satisfaction, increasing quit service [12], increasing the length of admission and care costs, reducing the quality of care, increasing the wound healing time, nursing infections [13], and even increasing the mortality rate of patients [14]. So that its 10% increase raises the probability of death by 7%, all of which can be prevented by nurses [15]. Environmental factors, stress, equipment shortage, nursing shortage, high workload, inappropriate expectations, management factors, and severity of illness are the causes of missing some nursing cares [16]. In this regard, the results of the study by Srulovici and Zahavy showed that by increasing the accountability of nurses, the missed care decreases [16]. On the other hand, professional values are the basis of nursing performance, which, while guiding the interactions of nurses with patients and colleagues, provide a framework for ethical behavior [17, 18]. The American Nursing Association has also emphasized the ethics of nurses' accountability to the patient and the quality of nursing care [19]. In other words, the nurse is responsible for the values of the patient, and nursing ethics focuses on the proper functioning and risk avoidance [20]. The use of these ethical and professional values in nursing is an important issue that has been missed for many reasons [21]. Nursing standards should be considered to provide quality nursing services, including professional and humane accountability. Accountability as an essential element in providing nursing care means having a responsible personality towards oneself and responsible behavior toward others [22]. The responsible nurse considers himself bound to be honest, and in some ways, he has a great responsibility toward patients regarding ethical and professional issues and providing the best services to patients [23]. So today, one of the indicators of the hospital's superiority over each other is the level of accountability and responsiveness of its staff to patients [24]. On the other hand, as science progresses, nursing development, changing the role of nurses from passive to active and decision-making roles, their managerial role in care planning, and increasing people's awareness of the Patients' Rights Charter increases the responsibility of nurses [25]. Also, the healthcare system has entered the accountable era, and with rapid changes in the health system, professional accountability, including the nurses' accountability, plays a very important role in fulfilling the mission of the health system, and this requires research in the field of responsibility [26].
Therefore, after reviewing previous studies in this field, it can be concluded that the role of professional nurses' values in the quality of nursing care has been neglected, and despite the importance of professional values and accountability as an example of professional values in nursing, research in this regard is still rare, and the study that can show the role of responsibility in missed nursing care is much less [27]. Hence, considering the importance of accountability and the quality of nursing care and nursing care without care, the present study aimed to investigate missed nursing care and its relationship with the social responsibility of nurses.
Instrument and Methods
In this descriptive-correlational study that was carried out from 15 December 2018 to 30 July 2019, all nurses working in hospitals affiliated with Khoy Faculty of Medical Sciences entered the study by simple random sampling. The sample size was estimated with a confidence level of 0.95, a test power of 90.90, and the minimum correlation coefficient between the missed care with social accountability (r=0.15) for statistical significance, and using the below formula:
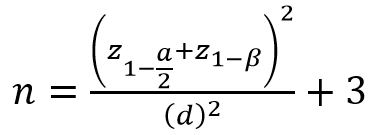
The minimum sample size was calculated to be 300 people. To increase the generalizability of the results and to consider the 14% drop in attrition in the samples, a study was conducted with 342 nurses. The inclusion criteria included at least one year of work experience, a bachelor's degree or higher, and the willingness to participate in the study.
The data collection tool included three parts:
a) Demographic information questionnaire including age, gender, marital status, education degree, years of service, employment status, job shift, job satisfaction, supra satisfaction, workload, communication with colleagues, and job expectations.
b) The Social Responsibility Questionnaire based on the Carol model [28], which included 35 items based on the 5-degree Likert scale from the "totally opposite spectrum" (1) to the "totally agreeable" [5], and had 4 sub-scales including the legal responsibility (7 items), the economic responsibility (7 items), the ethical responsibility (9 items), and discretionary responsibility (12 items). Questionnaire scores were between 175-35. Validity and reliability of the questionnaire were confirmed in previous studies, and its reliability was estimated at 0.95 [29]. In this study, Cronbach's alpha coefficient was estimated at 92% for internal consistency, and 10 nursing experts measured face and content validity.
c) The Misses Nursing Care Questionnaire, designed by Kalisch and Williams, evaluates the occurrence of missed nursing care with 24 items in four subscales, identifies interventions for individual needs, basic care interventions and planning, and answers. It is a self-report with a 5-point Likert scale ranging from "never" (0) to "always". The translation of the questionnaire by the method of Weld et al. in eight stages of the scale was interpreted and adapted. Then it was used to determine the validity of their content and form by the professors of Khoy Medical School. The Content Validity Index (CVI) and the Content Validity Ratio (CVR) were 90.33% and 79.9%, respectively, and the reliability was calculated using the internal consistency (Cronbach’s alpha coefficient) at 0.94. In previous studies, the structural validity of the questionnaire was confirmed by factor analysis, and its reliability was estimated to be 0.87 by a re-test [4, 30].
The study was submitted to the Ethics Committee of the Khoy Medical Sciences Faculty and was approved by the College's Research Council with the ethics code ir.Choy.rec.1397.004. Then the researchers entered the research environment for sampling with the ethical and executive permission of the project and explained the objectives of the project and the sampling method to the officials and the samples and obtained written informed consent.
Questionnaires were distributed in the morning, evening, and night shifts, and nurses were given time to answer their questions. The samples were emphasized to review questions in the presence of the researcher to answer possible uncertainties.
The data were coded and entered into the computer and analyzed by SPSS 20 software using descriptive statistics (frequency distribution and percentage) and analytical statistics tests (Pearson correlation test, Spearman correlation test, Inverse Chi-square test).
Findings
The mean age of participants was 30.04±6.20 years, and the mean work experience was 6.2±2.8 years. 71.3% of nurses were female, and 57.9% were married. 91.2% of them had a bachelor's degree. 35.7%were contractual and 91.2% of them were shift workers. 47.4% of nurses described their nursing duties clearly, and 33% stated that unusual nursing expectations were high. According to 32.7%, nurses had lower decision-making powers, and 40.9% complained about the ratio of nurses to patients. 58.77% of respondents described the workload of nurses, 43% were unsatisfied with nursing jobs, and 47.4% were unsatisfied with their department, and 45.9% gave their nursing work to other colleagues with trust in others.
Based on the nurses' viewpoints, blood glucose control and intravenous line care were the least missed nursing care by the mean of 1.74±0.96 and 1.09±0.88, respectively, and emotional support of patients and companions and hand washing were the most missed nursing care by the mean of 3.12±1.28 and 3.80±1.27, respectively. The frequency of missed nursing care items is provided in Figure 1.
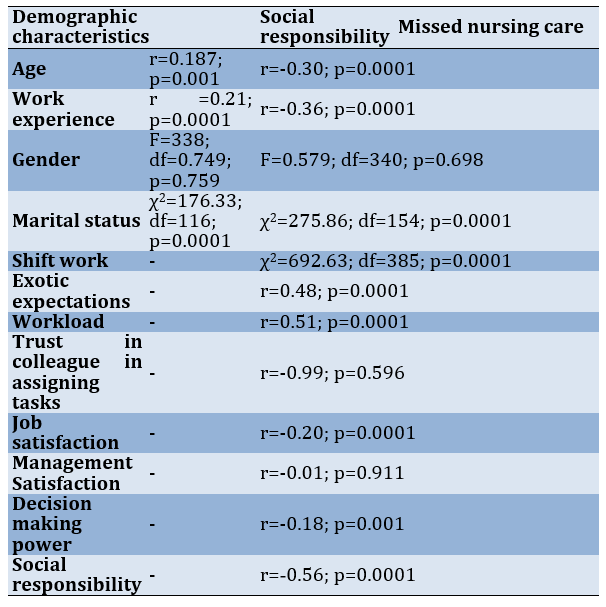
There was a significant and inverse correlation between missed nursing care with social responsibility (p=0.0001; r=-0.56), age (r=-0.30; p=0.0001), work experience (r=-0.33; p=0.0001), job satisfaction (r=-0.20; p=0.0001), and decision making power (r=-0.18; p=0.001), so that with the increase of social responsibility, age, work experience, job satisfaction and decision-making power, the missed nursing care decreases. Also, there was a direct and significant correlation between missed nursing care with workload (r=0.51; p=0.0001), exotic expectations (r=0.48; p=0.0001), so that the increase in workload and exotic expectations of nurses increases missed nursing care. In addition, a direct and significant correlation was observed between social responsibility with age (r=0.187; p=0.001) and work experience (r=0.21; p=0.0001; Table 1).
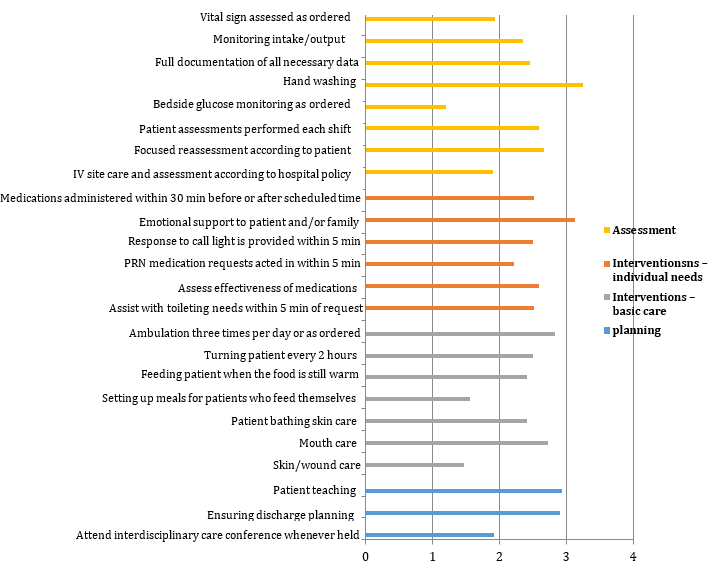
Figure 1) Frequency of missed nursing care items
Table 1) Relationship between missed care and social responsibility of nurses with demographic characteristics
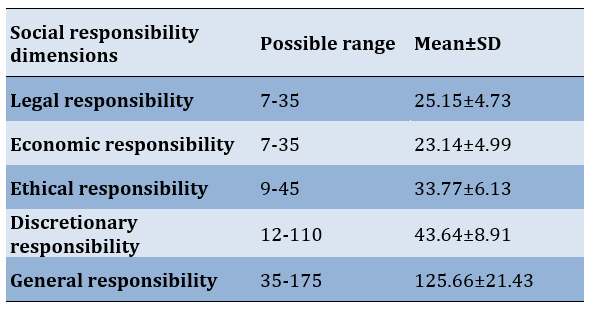
The mean scores of nurses' social responsibility dimensions are presented in Table 2.
Table 2) Mean scores of social responsibility dimensions of nurses
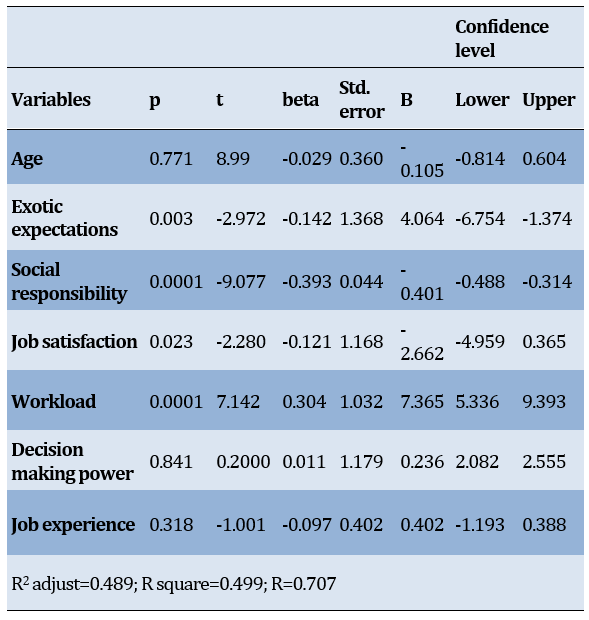
Social responsibility (β=-0.401; p=0.0001), workload (β=7.365; p=0.0001), and exotic expectations (β=4.064; p=0.003) as independent variables were good predictors for missed nursing care as a dependent variable (Table 3).
Table 3) Linear regression model of factors predicting missed nursing care
Discussion
The results of this study showed that based on the nurses' viewpoints, blood glucose control, and intravenous line care were the lowest missed nursing care, and emotional support of patients and companions and hand washing were the highest missed nursing care. This finding is consistent with the results of other studies, including patient education, patient clearance planning, psychological support of the patient and the family of the patient in the study of Needleman [31], patient travel, helping patients with nutrition, oral maturation and participation in Saqer and AbuAlRub's study [32], patient education and discharge program in the study of Kalisch and Lee [33], bathing the patient, giving mouth-watering, and changing the position every 2 hours in the study of Vryonides et al. [34]. Psychological support of the patient and his family, timely drug orders, and evaluation of care programs were the most commonly reported neglected nursing care in Moreno et al. study [35].
Also, according to the results, neglected nursing care decreases with increasing age and work experience [36]. The results of this study were consistent with the results of John et al. [19]. Probably few nurses have enough experience in accepting and assuming tasks such as patient education [37]. Also, with the increase in job satisfaction and decision-making power, the amount of missed nursing care reduces. In justifying this finding, it can be said that job satisfaction increases the employees' productivity and compassion towards the organization, their affiliation and dependence in the workplace, and the increase in quantity and quality, and low job satisfaction results in poor and defective services [38].
The findings of the study also showed that there was a direct and significant relationship between missed nursing care and work shift. Clari Harvey and colleagues showed in their study that an increase in the number of hours worked by nurses more than 8 hours increases the amount of missed care, which is the highest rate at night work and the lowest in the morning shift [39]. This difference in the present study can be due to the high frequency of shift rotations. Griffiths et al. estimated the prevalence of neglected nursing care at the end of the shift from 75% in the UK (51%) to 93% in Germany and a total of 88% in the 12 European countries [40, 41].
The result of the study showed that neglected nursing care has a direct and significant relationship with the increase in nurses' workload, which could be due to a lack of nurses. Kalisch et al. considered nursing scarcity as a source of forgetfulness for some nursing care [42]. Also, Aiken et al. showed in their studies that an increase in the proportion of the patient-nurse by more than 6 to 1 increases the number of missed nursing care and side effects on patients [43].
Another finding was the existence of a direct and significant relationship between missed nursing care with workload and exotic expectations. In this regard, Bazi and Sharafi’s study described the unpredictable expectations of nurses, which sometimes diverts some of these tasks from nurses to the main mission of patient care [39].
The results of the study showed that in the social responsibility dimensions of nurses, economic responsibility has the least, and discretionary responsibility has the highest score. Despite marital status, increase in age, and service record, their social responsibility increased, but between sex and social responsibility of nurses, there was not a significant correlation that it was opposite with the study of Hosseinian et al. [44].
This is logically acceptable because as the age of nurses increases, their professional experience increases.
Also, the results of this study showed that variables of social responsibility of nurses and workload and exotic expectations were missed as predictors of the dependent variable of nursing care. In their study, Sorrowov et al. demonstrated that the social responsibility of nurses has a reverse and significant relationship with neglected nursing care [45]. It is obvious that no matter how much nurses adhere to ethical values and have social responsibility at the top of them, they restrain individual interest and personal benefit and give patients confidence in relationships and show more honesty and accuracy to patients [46].
One of the limitations of the design is the lack of a system to record nursing errors and evaluate these errors based on the nurses' language reports, while the gold standard for recording missed nursing care is straightforward [47]. The rest of the study was restrained by remembering the neglected care. First, it is recommended to change the attitude of managers towards nursing errors and to replace punitive systems with corrective systems because self-reported errors are a key element in maintaining safety and improving the quality of patient care. Second, a system of nursing errors should be created in the departments.
Competent nurses are directly and indirectly responsible for quality responsibility and care errors. Therefore, by increasing accountability, the nurse avoids any neglect and negligence in the direction of treatment and care [48]. On the other hand, some studies also consider the cause of many neglected nursing cares to be related to personal and moral habits and a syndrome called "it's my non-job syndrome" and use the mechanisms of denial of care [48]. In the same way, the American Nurses Association requires nurses to take responsibility for online education and to uphold standards of care and patient rights [29].
The supervisors 'supervisory system has increased the nurses' function (unrecognizable), and especially nursing managers have a special interest in selecting the forces for ethical standards. More studies are needed in this field with a higher sample size and in different hospitals with different cultures and other factors affecting neglected nursing care, such as other aspects of ethical values, competence and cultural sensitivity. Also, practical solutions should be considered to reduce these errors.
Conclusion
Nursing care is neglected among nurses; these errors have an inverse relationship with the social responsibility of nurses. First, the supervision system of supervisors is more effective than that of nurses. Secondly, nursing managers have special ethical standards in the selection of staff.
Acknowledgements: Not reported.
Ethical Permission: The study was submitted to the Ethics Committee of the Khoy Medical Sciences Faculty and was approved by the College's Research Council with the ethics code ir.Choy.rec.1397.004. Then the researchers entered the research environment for sampling with the ethical and executive permission of the project and explained the objectives of the project and the sampling method to the officials and the samples and obtained written informed consent.
Conflict of Interests: There is no conflict of interest.
Authors’ Contribution: Purabdollah M (First Author), Introduction Writer/Methodologist (30%); Mokhtari M (Second Author), Methodologist/Statistical Analyst (20%); Moghadam Tabrizi F (Third Author), Assistant Researcher/Discussion Writer (10%); Khorami Markani A (Fourth Author), Methodologist/Main Researcher (30%); Emami S (Fifth Author), Assistant Researcher/Discussion Writer (10%)
Funding: Not reported.
Patient safety is one of the most important issues in nursing care and is a professional concern of all those involved in patient care to ensure the quality of patient's safety care before incidents [1]. Nursing care is a main component of health care services as a priority in the health care system. In many countries, the quality of nursing care is considered as an important indicator in the validation and ranking of health centers, which should be considered to maximize profits with minimal harm to patients [2]. Therefore, improving the quality of health care is one of the main concerns of health service providers. In this regard, one of the goals of the health care organization is to prevent injury and harm to the patient, to ensure the safety of the patient's health, and as a result, to provide high-quality health services [3].
Missed nursing care is a new concept in nursing, and any delay in caring is defined as the removal of all or part of nursing care, which is also referred to as a nursing mistake or error [4]. Nurses' faults are heavy and in most cases irreparable. Nowadays, nurses independently examine and diagnose patient problems, plan, execute and evaluate nursing measures in the nursing process, and assume the responsibility and legal responsibility for these actions [5]. Misdiagnosis, nursing practices in the wrong place, using the false techniques, delayed diagnosis, inadequate diagnosis, hospital infections, falling in the patient, subcutaneous wounds, and misconceptions are nursing errors [6]. Unfortunately, many of these errors are not reported. Missed nursing care is a global phenomenon, and some aspects of nursing care are missed, and its prevalence varies from country to country [7]. Based on the available evidence, it is estimated that in developing countries, one in 10 people will be injured while receiving hospital services [8]. The results of some studies in this area indicate a high prevalence of neglected nursing care among nurses with a prevalence between 15-98% [9, 10], and more than 70% in the Kalisch et al.’s study, which these estimates are alarming for healthcare systems, health policy-makers, and service providers [4].
The misse of nursing care has undesirable effects, including increasing patient dissatisfaction, reducing patient safety [11], increasing nurses' workload, increasing nurses' job turnover, reducing job satisfaction, increasing quit service [12], increasing the length of admission and care costs, reducing the quality of care, increasing the wound healing time, nursing infections [13], and even increasing the mortality rate of patients [14]. So that its 10% increase raises the probability of death by 7%, all of which can be prevented by nurses [15]. Environmental factors, stress, equipment shortage, nursing shortage, high workload, inappropriate expectations, management factors, and severity of illness are the causes of missing some nursing cares [16]. In this regard, the results of the study by Srulovici and Zahavy showed that by increasing the accountability of nurses, the missed care decreases [16]. On the other hand, professional values are the basis of nursing performance, which, while guiding the interactions of nurses with patients and colleagues, provide a framework for ethical behavior [17, 18]. The American Nursing Association has also emphasized the ethics of nurses' accountability to the patient and the quality of nursing care [19]. In other words, the nurse is responsible for the values of the patient, and nursing ethics focuses on the proper functioning and risk avoidance [20]. The use of these ethical and professional values in nursing is an important issue that has been missed for many reasons [21]. Nursing standards should be considered to provide quality nursing services, including professional and humane accountability. Accountability as an essential element in providing nursing care means having a responsible personality towards oneself and responsible behavior toward others [22]. The responsible nurse considers himself bound to be honest, and in some ways, he has a great responsibility toward patients regarding ethical and professional issues and providing the best services to patients [23]. So today, one of the indicators of the hospital's superiority over each other is the level of accountability and responsiveness of its staff to patients [24]. On the other hand, as science progresses, nursing development, changing the role of nurses from passive to active and decision-making roles, their managerial role in care planning, and increasing people's awareness of the Patients' Rights Charter increases the responsibility of nurses [25]. Also, the healthcare system has entered the accountable era, and with rapid changes in the health system, professional accountability, including the nurses' accountability, plays a very important role in fulfilling the mission of the health system, and this requires research in the field of responsibility [26].
Therefore, after reviewing previous studies in this field, it can be concluded that the role of professional nurses' values in the quality of nursing care has been neglected, and despite the importance of professional values and accountability as an example of professional values in nursing, research in this regard is still rare, and the study that can show the role of responsibility in missed nursing care is much less [27]. Hence, considering the importance of accountability and the quality of nursing care and nursing care without care, the present study aimed to investigate missed nursing care and its relationship with the social responsibility of nurses.
Instrument and Methods
In this descriptive-correlational study that was carried out from 15 December 2018 to 30 July 2019, all nurses working in hospitals affiliated with Khoy Faculty of Medical Sciences entered the study by simple random sampling. The sample size was estimated with a confidence level of 0.95, a test power of 90.90, and the minimum correlation coefficient between the missed care with social accountability (r=0.15) for statistical significance, and using the below formula:
The minimum sample size was calculated to be 300 people. To increase the generalizability of the results and to consider the 14% drop in attrition in the samples, a study was conducted with 342 nurses. The inclusion criteria included at least one year of work experience, a bachelor's degree or higher, and the willingness to participate in the study.
The data collection tool included three parts:
a) Demographic information questionnaire including age, gender, marital status, education degree, years of service, employment status, job shift, job satisfaction, supra satisfaction, workload, communication with colleagues, and job expectations.
b) The Social Responsibility Questionnaire based on the Carol model [28], which included 35 items based on the 5-degree Likert scale from the "totally opposite spectrum" (1) to the "totally agreeable" [5], and had 4 sub-scales including the legal responsibility (7 items), the economic responsibility (7 items), the ethical responsibility (9 items), and discretionary responsibility (12 items). Questionnaire scores were between 175-35. Validity and reliability of the questionnaire were confirmed in previous studies, and its reliability was estimated at 0.95 [29]. In this study, Cronbach's alpha coefficient was estimated at 92% for internal consistency, and 10 nursing experts measured face and content validity.
c) The Misses Nursing Care Questionnaire, designed by Kalisch and Williams, evaluates the occurrence of missed nursing care with 24 items in four subscales, identifies interventions for individual needs, basic care interventions and planning, and answers. It is a self-report with a 5-point Likert scale ranging from "never" (0) to "always". The translation of the questionnaire by the method of Weld et al. in eight stages of the scale was interpreted and adapted. Then it was used to determine the validity of their content and form by the professors of Khoy Medical School. The Content Validity Index (CVI) and the Content Validity Ratio (CVR) were 90.33% and 79.9%, respectively, and the reliability was calculated using the internal consistency (Cronbach’s alpha coefficient) at 0.94. In previous studies, the structural validity of the questionnaire was confirmed by factor analysis, and its reliability was estimated to be 0.87 by a re-test [4, 30].
The study was submitted to the Ethics Committee of the Khoy Medical Sciences Faculty and was approved by the College's Research Council with the ethics code ir.Choy.rec.1397.004. Then the researchers entered the research environment for sampling with the ethical and executive permission of the project and explained the objectives of the project and the sampling method to the officials and the samples and obtained written informed consent.
Questionnaires were distributed in the morning, evening, and night shifts, and nurses were given time to answer their questions. The samples were emphasized to review questions in the presence of the researcher to answer possible uncertainties.
The data were coded and entered into the computer and analyzed by SPSS 20 software using descriptive statistics (frequency distribution and percentage) and analytical statistics tests (Pearson correlation test, Spearman correlation test, Inverse Chi-square test).
Findings
The mean age of participants was 30.04±6.20 years, and the mean work experience was 6.2±2.8 years. 71.3% of nurses were female, and 57.9% were married. 91.2% of them had a bachelor's degree. 35.7%were contractual and 91.2% of them were shift workers. 47.4% of nurses described their nursing duties clearly, and 33% stated that unusual nursing expectations were high. According to 32.7%, nurses had lower decision-making powers, and 40.9% complained about the ratio of nurses to patients. 58.77% of respondents described the workload of nurses, 43% were unsatisfied with nursing jobs, and 47.4% were unsatisfied with their department, and 45.9% gave their nursing work to other colleagues with trust in others.
Based on the nurses' viewpoints, blood glucose control and intravenous line care were the least missed nursing care by the mean of 1.74±0.96 and 1.09±0.88, respectively, and emotional support of patients and companions and hand washing were the most missed nursing care by the mean of 3.12±1.28 and 3.80±1.27, respectively. The frequency of missed nursing care items is provided in Figure 1.
There was a significant and inverse correlation between missed nursing care with social responsibility (p=0.0001; r=-0.56), age (r=-0.30; p=0.0001), work experience (r=-0.33; p=0.0001), job satisfaction (r=-0.20; p=0.0001), and decision making power (r=-0.18; p=0.001), so that with the increase of social responsibility, age, work experience, job satisfaction and decision-making power, the missed nursing care decreases. Also, there was a direct and significant correlation between missed nursing care with workload (r=0.51; p=0.0001), exotic expectations (r=0.48; p=0.0001), so that the increase in workload and exotic expectations of nurses increases missed nursing care. In addition, a direct and significant correlation was observed between social responsibility with age (r=0.187; p=0.001) and work experience (r=0.21; p=0.0001; Table 1).
Figure 1) Frequency of missed nursing care items
Table 1) Relationship between missed care and social responsibility of nurses with demographic characteristics
The mean scores of nurses' social responsibility dimensions are presented in Table 2.
Table 2) Mean scores of social responsibility dimensions of nurses
Social responsibility (β=-0.401; p=0.0001), workload (β=7.365; p=0.0001), and exotic expectations (β=4.064; p=0.003) as independent variables were good predictors for missed nursing care as a dependent variable (Table 3).
Table 3) Linear regression model of factors predicting missed nursing care
Discussion
The results of this study showed that based on the nurses' viewpoints, blood glucose control, and intravenous line care were the lowest missed nursing care, and emotional support of patients and companions and hand washing were the highest missed nursing care. This finding is consistent with the results of other studies, including patient education, patient clearance planning, psychological support of the patient and the family of the patient in the study of Needleman [31], patient travel, helping patients with nutrition, oral maturation and participation in Saqer and AbuAlRub's study [32], patient education and discharge program in the study of Kalisch and Lee [33], bathing the patient, giving mouth-watering, and changing the position every 2 hours in the study of Vryonides et al. [34]. Psychological support of the patient and his family, timely drug orders, and evaluation of care programs were the most commonly reported neglected nursing care in Moreno et al. study [35].
Also, according to the results, neglected nursing care decreases with increasing age and work experience [36]. The results of this study were consistent with the results of John et al. [19]. Probably few nurses have enough experience in accepting and assuming tasks such as patient education [37]. Also, with the increase in job satisfaction and decision-making power, the amount of missed nursing care reduces. In justifying this finding, it can be said that job satisfaction increases the employees' productivity and compassion towards the organization, their affiliation and dependence in the workplace, and the increase in quantity and quality, and low job satisfaction results in poor and defective services [38].
The findings of the study also showed that there was a direct and significant relationship between missed nursing care and work shift. Clari Harvey and colleagues showed in their study that an increase in the number of hours worked by nurses more than 8 hours increases the amount of missed care, which is the highest rate at night work and the lowest in the morning shift [39]. This difference in the present study can be due to the high frequency of shift rotations. Griffiths et al. estimated the prevalence of neglected nursing care at the end of the shift from 75% in the UK (51%) to 93% in Germany and a total of 88% in the 12 European countries [40, 41].
The result of the study showed that neglected nursing care has a direct and significant relationship with the increase in nurses' workload, which could be due to a lack of nurses. Kalisch et al. considered nursing scarcity as a source of forgetfulness for some nursing care [42]. Also, Aiken et al. showed in their studies that an increase in the proportion of the patient-nurse by more than 6 to 1 increases the number of missed nursing care and side effects on patients [43].
Another finding was the existence of a direct and significant relationship between missed nursing care with workload and exotic expectations. In this regard, Bazi and Sharafi’s study described the unpredictable expectations of nurses, which sometimes diverts some of these tasks from nurses to the main mission of patient care [39].
The results of the study showed that in the social responsibility dimensions of nurses, economic responsibility has the least, and discretionary responsibility has the highest score. Despite marital status, increase in age, and service record, their social responsibility increased, but between sex and social responsibility of nurses, there was not a significant correlation that it was opposite with the study of Hosseinian et al. [44].
This is logically acceptable because as the age of nurses increases, their professional experience increases.
Also, the results of this study showed that variables of social responsibility of nurses and workload and exotic expectations were missed as predictors of the dependent variable of nursing care. In their study, Sorrowov et al. demonstrated that the social responsibility of nurses has a reverse and significant relationship with neglected nursing care [45]. It is obvious that no matter how much nurses adhere to ethical values and have social responsibility at the top of them, they restrain individual interest and personal benefit and give patients confidence in relationships and show more honesty and accuracy to patients [46].
One of the limitations of the design is the lack of a system to record nursing errors and evaluate these errors based on the nurses' language reports, while the gold standard for recording missed nursing care is straightforward [47]. The rest of the study was restrained by remembering the neglected care. First, it is recommended to change the attitude of managers towards nursing errors and to replace punitive systems with corrective systems because self-reported errors are a key element in maintaining safety and improving the quality of patient care. Second, a system of nursing errors should be created in the departments.
Competent nurses are directly and indirectly responsible for quality responsibility and care errors. Therefore, by increasing accountability, the nurse avoids any neglect and negligence in the direction of treatment and care [48]. On the other hand, some studies also consider the cause of many neglected nursing cares to be related to personal and moral habits and a syndrome called "it's my non-job syndrome" and use the mechanisms of denial of care [48]. In the same way, the American Nurses Association requires nurses to take responsibility for online education and to uphold standards of care and patient rights [29].
The supervisors 'supervisory system has increased the nurses' function (unrecognizable), and especially nursing managers have a special interest in selecting the forces for ethical standards. More studies are needed in this field with a higher sample size and in different hospitals with different cultures and other factors affecting neglected nursing care, such as other aspects of ethical values, competence and cultural sensitivity. Also, practical solutions should be considered to reduce these errors.
Conclusion
Nursing care is neglected among nurses; these errors have an inverse relationship with the social responsibility of nurses. First, the supervision system of supervisors is more effective than that of nurses. Secondly, nursing managers have special ethical standards in the selection of staff.
Acknowledgements: Not reported.
Ethical Permission: The study was submitted to the Ethics Committee of the Khoy Medical Sciences Faculty and was approved by the College's Research Council with the ethics code ir.Choy.rec.1397.004. Then the researchers entered the research environment for sampling with the ethical and executive permission of the project and explained the objectives of the project and the sampling method to the officials and the samples and obtained written informed consent.
Conflict of Interests: There is no conflict of interest.
Authors’ Contribution: Purabdollah M (First Author), Introduction Writer/Methodologist (30%); Mokhtari M (Second Author), Methodologist/Statistical Analyst (20%); Moghadam Tabrizi F (Third Author), Assistant Researcher/Discussion Writer (10%); Khorami Markani A (Fourth Author), Methodologist/Main Researcher (30%); Emami S (Fifth Author), Assistant Researcher/Discussion Writer (10%)
Funding: Not reported.
Article Type: Descriptive & Survey |
Subject:
Health Promotion Approaches
Received: 2022/02/9 | Accepted: 2022/05/1 | Published: 2022/09/1
Received: 2022/02/9 | Accepted: 2022/05/1 | Published: 2022/09/1
References
1. Chiozza ML, Ponzetti C. FMEA: a model for reducing medical errors. Clin Chim Acta. 2009;404(1):75-8. [Link] [DOI:10.1016/j.cca.2009.03.015]
2. Zirak M, Moghadasian S, Abdollahzadeh F, Rahmani A. The study of level of ethical development in nurses working in training-treatment hospitals affiliated in Tabriz university of medical sciences, Tabriz, Iran. Qom Univ Med Sci J. 2012;6(3):32-9. [Persian] [Link]
3. World Health Organization & WHO Patient Safety. Conceptual framework for the international classification for patient safety version 1.1: final technical report January 2009 [Internet].Geneva: World Health Organization; [cited 2010 Feb 2]. Available from: https://apps.who.int/iris/handle/10665/70882. [Link]
4. Kalisch BJ, Landstrom GL, Hinshaw AS. Missed nursing care: a concept analysis. J Adv Nurs. 2009;65(7):1509-17. [Link] [DOI:10.1111/j.1365-2648.2009.05027.x]
5. Taylor C, Lynn P, Bartlett J. Fundamentals of nursing: The art and science of person-centered care. 9th Edition. Lippincott Williams & Wilkins; 2018. [Link]
6. AbdiI Z, Maleki MR, Khisravi A. Perceptions of patient safety culture among staff of selected hospitals affiliated to Tehran University of Medical Sciences. Payesh. 2011;10(4):411-9. [Persian] [Link]
7. Blackman IR, Henderson JA, Willis EM, Toffoli LP. After hours nurse staffing, work intensity and quality of care-missed care study: New South Wales public and private sectors. Final report to the New South Wales Nurses and Midwives' Association. Flinders University; 2015. [Link]
8. Jones TL, Hamilton P, Murry N. Unfinished nursing care, missed care, and implicitly rationed care: State of the science review. Int J Nurs Stud. 2015;52(6):1121-37. [Link] [DOI:10.1016/j.ijnurstu.2015.02.012]
9. Halbesleben JR, Rathert C. Linking physician burnout and patient outcomes: exploring the dyadic relationship between physicians and patients. Health Care Manage Rev. 2008;33(1):29-39. [Link] [DOI:10.1097/01.HMR.0000304493.87898.72]
10. Helfrich CD, Simonetti JA, Clinton WL, Wood GB, Taylor L, Schectman G, et al. The association of team-specific workload and staffing with odds of burnout among VA primary care team members. J Gen Intern Med. 2017;32(7):760-6. [Link] [DOI:10.1007/s11606-017-4011-4]
11. Landon BE, Reschovsky JD, Pham HH, Blumenthal D. Leaving medicine: the consequences of physician dissatisfaction. Med Care. 2006;44(3):234-42. [Link] [DOI:10.1097/01.mlr.0000199848.17133.9b]
12. Schubert M, Glass TR, Clarke SP, Aiken LH, Schaffert-Witvliet B, Sloane DM, et al. Rationing of nursing care and its relationship to patient outcomes: the Swiss extension of the International Hospital Outcomes Study. Int J Qual Health Care. 2008;20(4):227-37. [Link] [DOI:10.1093/intqhc/mzn017]
13. Schubert M, Clarke SP, Aiken LH, De Geest S. Associations between rationing of nursing care and inpatient mortality in Swiss hospitals. Int J Qual Health Care. 2012;24(3):230-8. [Link] [DOI:10.1093/intqhc/mzs009]
14. Ball JE, Bruyneel L, Aiken LH, Sermeus W, Sloane DM, Rafferty AM, et al. Post-operative mortality, missed care and nurse staffing in nine countries: a cross-sectional study. Int J Nurs Stud. 2018;78:10-5. [Link] [DOI:10.1016/j.ijnurstu.2017.08.004]
15. Kalisch BJ, Lee KH. Missed nursing care: Magnet versus non-Magnet hospitals. Nurs Outlook. 2012;60(5):e32-9. [Link] [DOI:10.1016/j.outlook.2012.04.006]
16. Srulovici E, Drach-Zahavy A. Nurses' personal and ward accountability and missed nursing care: A cross-sectional study. Int J Nurs Stud. 2017;75:163-71. [Link] [DOI:10.1016/j.ijnurstu.2017.08.003]
17. Valizadeh L, Zamanzadeh V, Ghahramanian A, Aghajari P. The exploration of culturally sensitive nursing care in pediatric setting: A qualitative study. Int J Pediatr. 2017;5(2):4329-41. [Link]
18. Clark DK. Professional values: a study of education and experience in nursing students and nurses [Dissertation]. Minneapolis, Minnesota; Capella University; 2009. [Link]
19. Dehghani A, Mohammad Khan Kermanshah S. Evaluating of compliance with professional ethical standards in nursing practice from nursing staff's viewpoints in Tehran University of Medical Sciences. Mod Care. 2012;9(3):208-16. [Persian] [Link]
20. Shahriari M, Baloochestani E. Applying professional values: the perspective of nurses of Isfahan hospitals. J Med Ethics Hist Med. 2014;7:1. [Link]
21. Zarezadeh Kheibari S, Asgharinekah M, Horoofghanad M, Ebrahimhokmabadi M. Expressive arts group therapy with middleschool aged children in family-like community centers. Int J Psychol Behavior Res. 2014;1(4):32-8. [Link]
22. Gorbani A, Etemadi R, Jafari N. Study the responsibility of nurses (professional ethics and human), the recovery rate of patients. J Milit Caring Sci. 2014;1(1):57-62. [Persian] [Link] [DOI:10.18869/acadpub.mcs.1.1.57]
23. Weld KK, Garmon Bibb SC. Concept analysis: malpractice and modern‐day nursing practice. Nurs Forum. 2009;44(1):2-10. [Link] [DOI:10.1111/j.1744-6198.2009.00121.x]
24. Beikzad J, Hoseinpour A, Hejazi Bavil M. A survey on the relationship between responsibility and job satisfaction of nurses working in teaching hospitals affiliated with Tabriz University of Medical Sciences. J Hosp. 2014;13(1):53-60. [Persian] [Link]
25. Papastavrou E, Efstathiou G, Andreou C. Nursing students' perceptions of patient dignity. Nurs Ethics. 2016;23(1):92-103. [Link] [DOI:10.1177/0969733014557136]
26. Krautscheid LC. Defining professional nursing accountability: a literature review. J Prof Nurs. 2014;30(1):43-7. [Link] [DOI:10.1016/j.profnurs.2013.06.008]
27. Day L. Error, blame, and professional responsibility. Am J Crit Care. 2010;19(3):296-8. [Link] [DOI:10.4037/ajcc2010839]
28. Carroll AB. A three-dimensional conceptual model of corporate performance. Acad Manag Rev. 1979;4(4):497-505. [Link] [DOI:10.2307/257850]
29. Siu NY-M, Zhang TJ-F, Kwan H-Y. Effect of corporate social responsibility, customer attribution and prior expectation on post-recovery satisfaction. Int J Hosp Manag. 2014;43:87-97. [Link] [DOI:10.1016/j.ijhm.2014.08.007]
30. Kalisch BJ, Williams RA. Development and psychometric testing of a tool to measure missed nursing care. J Nurs Adm. 2009;39(5):211-9. [Link] [DOI:10.1097/NNA.0b013e3181a23cf5]
31. Needleman J. Nursing skill mix and patient outcomes. BMJ Qual Saf. 2017;26:525-8. [Link] [DOI:10.1136/bmjqs-2016-006197]
32. Saqer TJ, AbuAlRub RF. Missed nursing care and its relationship with confidence in delegation among hospital nurses. J Clin Nurs. 2018;27(13-14):2887-95. [Link] [DOI:10.1111/jocn.14380]
33. Kalisch BJ, Lee KH. The impact of teamwork on missed nursing care. Nurs outlook. 2010;58(5):233-41. [Link] [DOI:10.1016/j.outlook.2010.06.004]
34. Vryonides S, Papastavrou E, Charalambous A, Andreou P, Eleftheriou C, Merkouris A. Ethical climate and missed nursing care in cancer care units. Nurs Ethics. 2018 ;25(6):707-23. [Link] [DOI:10.1177/0969733016664979]
35. Moreno-Monsiváis MG, Moreno-Rodríguez C, Interial-Guzmán MG. Missed nursing care in hospitalized patients. Aquichan. 2015;15(3):318-28. [Link] [DOI:10.5294/aqui.2015.15.3.2]
36. Steege LM, Drake DA, Olivas M, Mazza G. Evaluation of physically and mentally fatiguing tasks and sources of fatigue as reported by registered nurses. J Nurs Manag. 2015;23(2):179-89. [Link] [DOI:10.1111/jonm.12112]
37. Sinn C-LJ, Tran J, Pauley T, Hirdes J. Predicting adverse outcomes after discharge from complex continuing care hospital settings to the community. Prof Case Manag. 2016;21(3):127-36. [Link] [DOI:10.1097/NCM.0000000000000148]
38. Bond S, Thomas LH. Measuring patients' satisfaction with nursing care. J Adv Nurs. 1992;17(1):52-63. [Link] [DOI:10.1111/j.1365-2648.1992.tb01818.x]
39. Bazi A, Sharafi S. Evaluation time nurses for non-nursing tasks and text services in nursing shifts: A cross-sectional study. Navid No. 2016;19(62):24-32. [Persian] [Link]
40. Zander B, Dobler L, Bäumler M, Busse R. Nursing tasks left undone in German acute care hospitals-results from the international study RN4Cast. Gesundheitswesen. 2014;76(11):727-34. [Germany]. [Link] [DOI:10.1055/s-0033-1364016]
41. Griffiths P, Ball J, Drennan J, James L, Jones J, Recio A, et al. The association between patient safety outcomes and nurse/healthcare assistant skill mix and staffing levels and factors that may influence staffing requirements. Southampton, GB: University of Southampton; 2014. [Link]
42. Kalisch BJ, Tschannen D, Lee H, Friese CR. Hospital variation in missed nursing care. Am J Med Qual. 2011;26(4):291-9. [Link] [DOI:10.1177/1062860610395929]
43. Aiken LH, Sloane D, Griffiths P, Rafferty AM, Bruyneel L, McHugh M, et al. Nursing skill mix in European hospitals: cross-sectional study of the association with mortality, patient ratings, and quality of care. BMJ Qual Saf. 2017;26(7):559-68. [Link] [DOI:10.1136/bmjqs-2016-005567]
44. Hasanian ZM, Bagheri A, Sadeghi A, Moghim BA. Nurses'status social responsibility and its relationship with some demographics profile. 2017;25(2):45-53. [Persian] [Link] [DOI:10.21859/nmj-25026]
45. Mahmoodi A, Khani L, Ghaffari M. The relationship of cultural competence and responsibility with nurses attitude toward patient's right: The mediating Role of Ethical Beliefs. Iran J Med Ethics Hist Medi. 2017;9(5):39-51. [Persian] [Link]
46. Kalfoss M. Student's perception of missed care: Focus group results. Open J Nurs. 2017;7(7):850. [Link] [DOI:10.4236/ojn.2017.77064]
47. Mumford V, Greenfield D, Hogden A, Debono D, Gospodarevskaya E, Forde K, et al. Disentangling quality and safety indicator data: a longitudinal, comparative study of hand hygiene compliance and accreditation outcomes in 96 Australian hospitals. BMJ Open. 2014;4(9):e005284. [Link] [DOI:10.1136/bmjopen-2014-005284]
48. Westbrook JI, Li L, Lehnbom EC, Baysari MT, Braithwaite J, Burke R, et al. What are incident reports telling us? A comparative study at two Australian hospitals of medication errors identified at audit, detected by staff and reported to an incident system. Int J Qual Health Care. 2015;27(1):1-9. [Link] [DOI:10.1093/intqhc/mzu098]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |