



Volume 9, Issue 4 (2021)
Health Educ Health Promot 2021, 9(4): 343-349 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Skok N, Fomichev I, Zinenkova A. Adolescents' Health Deviant Behavior in Modern Society. Health Educ Health Promot 2021; 9 (4) :343-349
URL: http://hehp.modares.ac.ir/article-5-56095-en.html
URL: http://hehp.modares.ac.ir/article-5-56095-en.html
1- Department of Marketing and Public Administration, Industrial University of Tyumen, Tyumen, Russian Federation , skok.nata@uohk.com.cn
2- Department of Marketing and Public Administration, Industrial University of Tyumen, Tyumen, Russian Federation
2- Department of Marketing and Public Administration, Industrial University of Tyumen, Tyumen, Russian Federation
Full-Text [PDF 377 kb]
(4669 Downloads)
| Abstract (HTML) (3261 Views)
Full-Text: (3883 Views)
Introduction
Recently, health deviant behaviors, as out of the norm, have become a serious problem of global importance. Every year, the number of students with health deviant behaviors in schools is steadily increasing. Rejected behavior manifests itself in bullying and peer violence and has more serious consequences such as alienation and crime.
Social deviance has been researched for over a century. Emil Durkheim, Lev Semyonovich Vygotsky, and others were the first scientists to address this issue [1]. According to L.S. Vygotsky, social deviations inherently reflect socially acceptable behavior. In this context, social norms can be interpreted as restrictions on behavior permissible in society, which ensure the proper functioning of society and help preserve society [2, 3]. A person's behavior may deviate from socially acceptable norms in both positive and negative ways. Positive deviance occurs when health deviant behavior manifests itself through non-compliance with accepted norms but does not harm anyone. Negative deviations disrupt the stability of the social system and often lead to violence and crime. Positive deviance represents creativity that brings positive change to society, whereas negative deviance is destructive and brings nothing positive to society.
Health deviant behavior is characterized by unconventional character traits that do not conform to accepted social norms. Unlike health deviant behaviors, such as crimes committed by people and generally assessed negatively, health deviant behaviors have a destructive or self-destructive tendency characterized by persistence and repetition. Signs of health deviant behaviors include social isolation and identification of the deviant in terms of age and gender [4]. It is important to distinguish health deviant behavior (illegal and immoral) from character traits such as weirdness and eccentricity, which are not harmful.
The concept of norms and deviations is determined by society because health deviant behaviors are a real threat to the physical and social survival of the individual in specific social or collective contexts. This refers to deviations from social and moral norms and cultural values in the process of assimilation to them and their reproduction [5]. Such deviations are possible due to the individual's actions that do not comply with certain social norms, such as divorce, criminalization of society, corruption of officials, etc. Deviation from accepted social, psychological, and moral norms is harmful to individuals, public welfare, and the environment.
Health deviant behaviors can be considered a choice between socially acceptable and deviant ways to achieve goals [6]. For example, to become rich or successful, a person may choose unacceptable means such as open defiance, protest, rejection of generally accepted social values, including morality and law, participation in various criminal, terrorist, or other extremist groups. Hence there is a tendency to fight against society instead of trying to fit into it. In all these cases, the deviation results from a complete or relative failure of socialization, i.e., the result of the inability or unwillingness of individuals to adapt to society and its requirements.
So far, the causes of health deviant behaviors have not been fully identified [7]. Therefore, this study aimed to identify the causes of health deviant behaviors among young students, to investigate the impact of health deviant behaviors in the learning environment, and to provide recommendations for young people with health deviant behaviors in terms of appropriate adaptation to society, as well as for teachers and parents.
Participants and Methods
This study is mixed research (qualitative and quantitative) conducted on May 21, 2021, to investigate the causes and consequences of health deviant behavior in a group of students aged 16 to 18 years. For this purpose, teachers and parents were asked to identify students with clear health deviant behavior. Therefore, a relatively small group of students (N =142) from the Engels Technological Institute (branch) of Saratov State Technical University named after Yu. A. Gagarin was formed to assess deviant health behavior in higher education and how students adapt to society. So, the purposive sampling method was used to select subjects.
An integral part of the study is a review of the literature on health deviant behavior and its major roots. When the aims and objectives of the research are formulated, it is time to analyze the relevant scientific literature. The study of literature, documents, electronic media, and other sources, as a basis for obtaining facts about the history and current state of the subject under study, serves to provide an initial insight into the primary concept of the subject and identify gaps and uncertainties in the development of the issue. A thorough literature review helps separate the known from the unknown, identify facts, accumulated experience, and clearly outline the issue under investigation. For this aim, the researcher used Google Scholar and Research Gate.
The following criteria were used to select literary sources: publication date, scientific significance, experimental nature of the study, number of citations of other researchers, and relationship with this research. Subsequently, several scientific papers (both theoretical and experimental) were selected to develop the theoretical basis of this study. The materials have been critically evaluated in terms of their suitability for this study.
The research on the problem was conducted in three phases:
1. The first stage involved a theoretical analysis of existing methodological approaches as well as the theory and methodology of research on youth health deviant behavior in modern society. The study's problem, purpose, and methods were highlighted, and an experimental research plan was drawn up.
2. The second stage initially involved interviews with teachers and students' parents, clarifying specific aspects of health deviant behavior. The students were then asked to participate in an anonymous survey specifically designed for this study.
3. In the third stage, we completed the study with statistical analysis.
In our study, a questionnaire survey method was applied to collect data. According to the American Psychological Association, it is very important to clarify questions when conducting a survey [8, 9]. The questions should not presume the desired answers, and some questions should not be asked directly. In our study, a researcher-made questionnaire was used. Students were asked to answer the questionnaire anonymously, enabling more honest responses.
The questionnaire had two parts; The first part consisted of open-ended questions that provided qualitative data to the researcher. This part included information about the social characteristics of the research participants, their past and present behavior, attitudes and standards of behavior, beliefs, and the reasons for their respective actions in line with the topic under investigation.
The second part of the questionnaire consisted of closed-ended questions that evaluated variables of self-esteem, vulnerability to negative peer influence, and health deviant behavior. This part had 10 questions, and the answers were graded based on a Likert scale and students should answer the questions with the options including responsible-influenced by (with a score of 3-1), entertainment-stress coping (with a score of 3-1), not a bad habit-bad habit (with a score of 3-1), had thoughts-had attempted (with a score of 3-1), and watched-don’t watched (with a score of 3-1). The phenomenological approach was used to explore the individual experiences of each participant in our study, as it rejects pre-formulated hypotheses and concepts, which are a necessary auxiliary tool to understanding reality in the natural sciences. The main challenge in the phenomenological research approach is the individual and subjective perception of the meaning of individual experience and mutual understanding between the researcher and the participant of the meaning of individual experience [10]. The basic idea is to examine the participants' subjective experience and see it from their perspective to identify possible solutions. Indeed, qualitative research may lack credibility and reliability due to the subjective bias of the researcher and the unclear justification for the methods involved.
To guarantee the reliability and validity of this study, the following was done methodologically.
Firstly, the questions were formulated so that the subjects could accurately answer the causes and consequences of health deviant behavior, as well as how they managed to cope with situations caused by health deviant behavior. A professional counselor also checked the questionnaire for possible leading questions that could potentially result in biased responses. Finally, a pilot study was conducted to pre-test the potential respondents' understanding of the questionnaire.
The researcher obtained informed consent from the participants before starting the study. Participation in the study was entirely voluntary. Participants were free to answer any questions. However, the questionnaire was designed to limit the possibility of uncomfortable questions. The collected data was kept in private property and was not shared with third parties.
The collected data in the quantitative part of the research were described as frequency, mean and standard deviation. Data analysis was performed using SPSS 22 software. First, the normality of data distribution was checked by the Kolmogorov-Smirnov test. Then, the Pearson correlation test was used to examine the correlation between variables.
Findings
One hundred forty-two students answered the questionnaire, of which 56% were female.
74% of students (18% male and 56% female) were responsible for health deviant behavior, and 26% were influenced by others. 38% consumed alcoholic beverages. The reason for alcohol consumption in 27% was entertainment and in 42% was stress coping. 40% recognized that alcohol consumption by young people is the main cause of deviant health behavior. 16% of male students smoked with their peers. 40% of respondents said smoking is a bad habit, and 2% said smoking is not bad. 76% were familiar with illegal drugs. 38% had suicidal thoughts, and 8% had attempted suicide. 65% of the subjects enjoyed computer games and did not think that it was health deviant behavior. 3% Looked at pornographic content.
Table 1) Mean scores of research variables and matrix of correlation coefficients between them
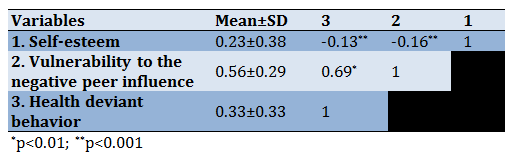
There was a significant positive correlation between health deviant behavior and vulnerability to negative peer influence. The more health deviant behavior respondents engage in, the more aggressive they become and the more vulnerable to negative peer influences. Relatively weak and negative correlations were found between self-esteem and health deviant behavior and vulnerability to the negative peer influence and self-esteem. Thus, the lower the self-esteem of a deviant adolescent, the more susceptible they are too negative peer influences and the more likely they to engage in various types of health deviant behavior (Table 1).
Discussion
This aspect has not been covered in previous studies, even though the concept of deviance is closely linked to the definition of the social norm, which was formulated almost a century ago. Indeed, the behavior of an increasing number of adolescents and young people is characterized by deviance. Normally, adolescents learn patterns of social adjustment. On the contrary, health deviant behavior leads to a conflict with social values. Nevertheless, despite numerous studies, the problem of health deviant behavior is not still fully understood.
Adolescence is characterized by unpredictable behavior, emotional distress, and rebellion. Adolescents in this stage of life strive for independence, develop a self-image, and experiment with the behavioral norms of the adult society and seek to gain trust and acceptance of people around them, especially their peers [11]. School and family are the contexts for adolescent growth, where adolescents develop psychologically and strive to show signs of maturity, shaping their self-image and learning appropriate social behaviors.
Researches show that when adolescents leave their parents to live independently, peer acceptance is of utmost importance to them [12, 13]. Adolescents may face many challenges in establishing their self-identity and integration into society. From this perspective, deviant health behavior can be seen as a sign of growth and independence. However, if confidence and acceptance cannot be gained in traditional groups (e.g., school and family), personal values and self-concepts may be underdeveloped. Consequently, adolescents may feel motivated to pursue life satisfaction and meet their psychological needs through a peer group. In this case, adolescents are likely to underestimate the social appropriateness of social interactions, at the expense of which adolescents gain a sense of acceptance by their peer group. Indeed, the subtle relationships between health deviant behavior and adolescent self-concept need to be considered [14-16].
Adolescents with less good academic performance tend to band together in the name of group support [17], aimed at jointly overcoming the dilemma of choosing between doing well and receiving praise from teachers or doing poorly but being accepted by peers. Cohesive group behavior may be criminal by nature. Nevertheless, involvement in it is necessary to gain acceptance from their peers.
In socio-psychological research on youth health deviant behavior in modern society, it is generally accepted that the possession of developed self-respect is evidence of a developed self-understanding and self-esteem, which allows individuals to treat themselves and others equally, effectively achieve self-integration and develop their potential, and have a higher expectation of self-efficacy [18]. There are several ways in which young people can make positive perceptions of themselves. Sources of respect can be found in the people around them (family, teachers, peers), which on the one hand prevents young people from developing low self-esteem and, on the other hand, also allows them to face challenges and failures with confidence, establishing confident and stable friendships and enabling them to establish and maintain positive relationships with family members and teachers. It makes sense to talk about a positive correlation between high self-esteem and assertive behavior [19].
Sociologists and psychologists have long considered self-esteem an important cause and consequence of deviant health behavior, suggesting that health deviant behavior can function as an adaptive mechanism of the individual and provide psychological self-protection. If self-respect and positive self-esteem cannot be gained through socially acceptable methods, the motivation for such (positive) behavior will gradually decrease. Instead, you can try to achieve self-respect and attention through other means, including health deviant behavior. Thus, low self-esteem is often seen as a motivation for deviant health behavior. It is not the health deviant behavior itself that boosts the adolescent's self-esteem, but the recognition he receives from deviant peers after committing a deviant act [20], which strengthens the psychological connection with other deviant adolescents during similar behavior. Thus, there is no direct link between health deviant behavior and self-esteem, increasing through illicit behavior.
The causes of health deviant behavior are related to upbringing conditions, physical development, and social environment [21]. In assessing his behavior, the adolescent notes the norm, his physical superiority or inferiority, and concludes his social significance and value. The child may have either a passive attitude towards physical weakness, a desire to compensate for weaknesses, or a desire to overcome them through physical exercise. Sometimes the neuromuscular retardation affects the coordination of movements and manifests itself clumsily. Adolescents' health deviant behavior includes anti-social, criminal, illegal, aggressive, self-destructive, and suicidal behavior. These actions can lead to various deviations in personal development. Often such deviations include the reaction of adolescents to difficult life circumstances.
Judgments and minor comments by others about the appearance and awkwardness of teenagers provoke strong feelings and distort the teenagers' behavior. Tallboys are confident in their strength and masculinity and do not have to struggle to earn the respect of their peers. Thus, they behave more naturally and require less attention to themselves. Because of their self-confidence, other children perceive tallboys as very intelligent. Skinny, short, developmentally disabled boys are considered immature by others, so they become rebellious and need constant supervision. To change their self-image, they have to be flexible and courageous and constantly prove their value and competitiveness among their peers [22]. Consequently, emotional tension and communication difficulties inevitably arise, pushing adolescents to break common rules and norms.
Health deviant behavior in adolescents is often caused by social issues, particularly lack of education and upbringing. Crime in most cases originates at home. The first seeds of deviance are planted either out of fear of punishment or out of protest, which then develops into a reflex-like stereotype [23]. The causes of deviant and delinquent behavior in adolescents are the lack of supervision, lack of attention from relatives, fear of punishment, desire to escape from parental care, parental abuse, and unmotivated desire to change the status quo. Separately, it should be noted that early alcohol and drug abuse among adolescents is motivated by a desire to feel like an adult, satisfy curiosity, or change the prevailing mental state [24, 25]. After drinking alcohol, a cheerful mood appears self-confidence and disinhibition increase. Group addiction that occurs when drinking with friends is likely to lead to alcoholism.
As a rule, the starting point and often the only factor contributing to adolescents' social adjustment with health deviant behavior is an external social requirement to behave in a way that conforms to rules and norms. However, this external requirement does not stimulate the experience of positive emotional reactions. We are talking about the fact that a teenager does not have an internal motivation for social adaptation. The educational institution must provide these external requirements to deviant adolescents. It can be said that there is a contradiction here since the government has assigned this responsibility to parents. In practice, however, the main role of educational institutions is to educate children and young people. In our opinion, this is due to the inability of the family to take on such a burden due to material difficulties and a limited understanding of specific characteristics of adolescent development. As people grow up and learn, they either fully, partially accept, or completely reject the life values promoted by educational institutions. Positive social adaptation is achieved when living in an educational institution is fulfilling and attractive, when it creates opportunities to socialize with peers, and a desire for interpersonal communication. Indeed, children with deviant health behavior mostly live in the community in families with no second parent, or this social unit is dysfunctional, so they need special help to coordinate their behavior.
A correlation between negative self-esteem and naughty behavior suggests that adolescents with low self-esteem can increase their self-esteem by engaging in healthy deviant behavior, whereas this effect is not seen among adolescents with high self-esteem. Adolescents may increase their self-esteem through participation in naughty behavior, but a similar effect was not seen in adolescents with high self-esteem. The possible social factors that play a role in creating these problems are, most importantly, the family, the educational community, and the influence of peers. To these should be added some psychological factors such as self-concept and personal values. Correlations show that the more aggressive the respondents' behavior towards their parents and the less motivated they are to study seriously, the lower their self-esteem. However, aggressive behavior towards teachers is noticeably different from aggressive behaviors towards parents and the effect of poor motivation to study seriously, as no significant relationship was found between aggressive behavior towards teachers and respondents' self-esteem. Health deviant behavior can be seen as another manifestation of prosocial behavior, in which the seriousness of recognition by peers is achieved by engaging inappropriate, serious acts of health deviant behavior. Enhancing young people's self-esteem by attracting peer attention through participation in health deviant behavior is a significant factor in the vulnerability of adolescents to peer influence. This socio-psychological mechanism acts as a vicious circle for deviant adolescents. Initially, when health deviant behavior begins, adolescents' self-esteem is relatively low, with a strong desire to be accepted by peers. Once an adolescent's reputation in their peer group for health deviant behavior is established, the adolescent gradually becomes a role model among peers, ceasing to experience the influence of peers on his behavior. Deviant adolescents may have relatively low self-esteem in the initial stages of health deviant behavior, but self-esteem increases significantly when adolescent health deviant behavior is supported by peers.
We can suggest that a key to aggression in health deviant behavior appears to be the creation of a negative mental schema for health deviant behavior. Meanwhile, in adolescents whose needs have been systematically neglected, the lack of a mental schema into which the needs of others are embedded is central. Future research should focus in-depth on these parameters, undoubtedly reflected in the impact of negative experiences on the individual. The age of participants in our study leaves opens the possibility of turning deviant health behavior into chronic. This requires, above all, the active establishment and specialized training of networks involved in identifying deviant health behavior, including educational, health, and justice institutions. They would provide a valuable opportunity to develop social-psychological skills such as empathy and understanding other people's emotions, which is very useful in nurturing altruistic behavior in young people without learning such skills at an earlier age.
The study results enable us to reasonably assert that socio-psychological factors are statistically significant concerning health deviant behavior among young people in the study area. The study rejected the null hypothesis about the absence of a link between socio-psychological factors and health deviant behavior among young people in the study area and adopted an alternative hypothesis. Thus, the study concludes a relationship between socio-psychological factors and health deviant behavior among young people in the study area. In other words, there is a relationship between health deviant behavior and lack of social skills, influence from peers and family.
Despite the valuable results received, it should be noted that this study is not without some limitations. The point is that all variables in this study were measured using self-reports. This method of psychological measurement allows one to have difficulty remembering childhood events. However, the age of the participants in our study is quite young, and therefore, in our opinion, respondents should not experience serious problems in recalling relatively recent events. Moreover, the questionnaire offered to the respondents did not consider the intensity, frequency, duration, or in some cases, the specific culprit of each negative life event.
Conclusion
The causes of health deviant behavior in students lie in the characteristics of the relationship and interaction of the individual with the surrounding world and the social environment. The main reasons for health deviant behavior appear to be biological, psychological, and social. Biological reasons are expressed by the physiological characteristics of adolescence. Psychological reasons lie in temperament and accentuations and the interaction of the teenager with society, family, and school. Thus, the reasons for health deviant behavior can be reduced to the characteristics of the individual, the conditions of the social environment, education, upbringing, and social activity. Students should participate in cooperative or extra-curricular activities to reduce stress and anxiety and channel their health deviant behavior constructively. Active participation in activities organized at the place of study can help develop their potential and increase their self-confidence and self-esteem, thus acting as a protective factor against health deviant behavior. Students seek moral and psychological support from peers, including deviant peers; in times of stress and anxiety, they should be taught how to resist unwanted peer pressure with appropriate social skills. In conclusion, changing the deviant identity of adolescent students is central to social work with young people. Social work in an educational institution should prepare deviant young people for new roles. However, concerns about their previous health deviant behavior create obstacles to positive change, so relapses in health deviant behavior are not excluded, which can be overcome by developing sports talents, providing volunteer services, developing mentoring, and creating role models able to reinforce self-esteem, keeping them on track gradually.
Acknowledgments: -
Ethical Permissions: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the National Ethics Commission of the Ministry of Health of the Russian Federation, September 1, 2021, No 0901-5.
Conflict of Interests: The authors declare no conflict of interest.
Authors’ Contribution: Natalia Skok (First Author), Original Researcher/Methodologist (40%); Igor Fomichev (Second Author), Introduction Writer/Discussion Writer (35%); Arina Zinenkova (Third Author), Introduction Writer/Assistant Researcher (25%).
Funding/Support: -
Recently, health deviant behaviors, as out of the norm, have become a serious problem of global importance. Every year, the number of students with health deviant behaviors in schools is steadily increasing. Rejected behavior manifests itself in bullying and peer violence and has more serious consequences such as alienation and crime.
Social deviance has been researched for over a century. Emil Durkheim, Lev Semyonovich Vygotsky, and others were the first scientists to address this issue [1]. According to L.S. Vygotsky, social deviations inherently reflect socially acceptable behavior. In this context, social norms can be interpreted as restrictions on behavior permissible in society, which ensure the proper functioning of society and help preserve society [2, 3]. A person's behavior may deviate from socially acceptable norms in both positive and negative ways. Positive deviance occurs when health deviant behavior manifests itself through non-compliance with accepted norms but does not harm anyone. Negative deviations disrupt the stability of the social system and often lead to violence and crime. Positive deviance represents creativity that brings positive change to society, whereas negative deviance is destructive and brings nothing positive to society.
Health deviant behavior is characterized by unconventional character traits that do not conform to accepted social norms. Unlike health deviant behaviors, such as crimes committed by people and generally assessed negatively, health deviant behaviors have a destructive or self-destructive tendency characterized by persistence and repetition. Signs of health deviant behaviors include social isolation and identification of the deviant in terms of age and gender [4]. It is important to distinguish health deviant behavior (illegal and immoral) from character traits such as weirdness and eccentricity, which are not harmful.
The concept of norms and deviations is determined by society because health deviant behaviors are a real threat to the physical and social survival of the individual in specific social or collective contexts. This refers to deviations from social and moral norms and cultural values in the process of assimilation to them and their reproduction [5]. Such deviations are possible due to the individual's actions that do not comply with certain social norms, such as divorce, criminalization of society, corruption of officials, etc. Deviation from accepted social, psychological, and moral norms is harmful to individuals, public welfare, and the environment.
Health deviant behaviors can be considered a choice between socially acceptable and deviant ways to achieve goals [6]. For example, to become rich or successful, a person may choose unacceptable means such as open defiance, protest, rejection of generally accepted social values, including morality and law, participation in various criminal, terrorist, or other extremist groups. Hence there is a tendency to fight against society instead of trying to fit into it. In all these cases, the deviation results from a complete or relative failure of socialization, i.e., the result of the inability or unwillingness of individuals to adapt to society and its requirements.
So far, the causes of health deviant behaviors have not been fully identified [7]. Therefore, this study aimed to identify the causes of health deviant behaviors among young students, to investigate the impact of health deviant behaviors in the learning environment, and to provide recommendations for young people with health deviant behaviors in terms of appropriate adaptation to society, as well as for teachers and parents.
Participants and Methods
This study is mixed research (qualitative and quantitative) conducted on May 21, 2021, to investigate the causes and consequences of health deviant behavior in a group of students aged 16 to 18 years. For this purpose, teachers and parents were asked to identify students with clear health deviant behavior. Therefore, a relatively small group of students (N =142) from the Engels Technological Institute (branch) of Saratov State Technical University named after Yu. A. Gagarin was formed to assess deviant health behavior in higher education and how students adapt to society. So, the purposive sampling method was used to select subjects.
An integral part of the study is a review of the literature on health deviant behavior and its major roots. When the aims and objectives of the research are formulated, it is time to analyze the relevant scientific literature. The study of literature, documents, electronic media, and other sources, as a basis for obtaining facts about the history and current state of the subject under study, serves to provide an initial insight into the primary concept of the subject and identify gaps and uncertainties in the development of the issue. A thorough literature review helps separate the known from the unknown, identify facts, accumulated experience, and clearly outline the issue under investigation. For this aim, the researcher used Google Scholar and Research Gate.
The following criteria were used to select literary sources: publication date, scientific significance, experimental nature of the study, number of citations of other researchers, and relationship with this research. Subsequently, several scientific papers (both theoretical and experimental) were selected to develop the theoretical basis of this study. The materials have been critically evaluated in terms of their suitability for this study.
The research on the problem was conducted in three phases:
1. The first stage involved a theoretical analysis of existing methodological approaches as well as the theory and methodology of research on youth health deviant behavior in modern society. The study's problem, purpose, and methods were highlighted, and an experimental research plan was drawn up.
2. The second stage initially involved interviews with teachers and students' parents, clarifying specific aspects of health deviant behavior. The students were then asked to participate in an anonymous survey specifically designed for this study.
3. In the third stage, we completed the study with statistical analysis.
In our study, a questionnaire survey method was applied to collect data. According to the American Psychological Association, it is very important to clarify questions when conducting a survey [8, 9]. The questions should not presume the desired answers, and some questions should not be asked directly. In our study, a researcher-made questionnaire was used. Students were asked to answer the questionnaire anonymously, enabling more honest responses.
The questionnaire had two parts; The first part consisted of open-ended questions that provided qualitative data to the researcher. This part included information about the social characteristics of the research participants, their past and present behavior, attitudes and standards of behavior, beliefs, and the reasons for their respective actions in line with the topic under investigation.
The second part of the questionnaire consisted of closed-ended questions that evaluated variables of self-esteem, vulnerability to negative peer influence, and health deviant behavior. This part had 10 questions, and the answers were graded based on a Likert scale and students should answer the questions with the options including responsible-influenced by (with a score of 3-1), entertainment-stress coping (with a score of 3-1), not a bad habit-bad habit (with a score of 3-1), had thoughts-had attempted (with a score of 3-1), and watched-don’t watched (with a score of 3-1). The phenomenological approach was used to explore the individual experiences of each participant in our study, as it rejects pre-formulated hypotheses and concepts, which are a necessary auxiliary tool to understanding reality in the natural sciences. The main challenge in the phenomenological research approach is the individual and subjective perception of the meaning of individual experience and mutual understanding between the researcher and the participant of the meaning of individual experience [10]. The basic idea is to examine the participants' subjective experience and see it from their perspective to identify possible solutions. Indeed, qualitative research may lack credibility and reliability due to the subjective bias of the researcher and the unclear justification for the methods involved.
To guarantee the reliability and validity of this study, the following was done methodologically.
Firstly, the questions were formulated so that the subjects could accurately answer the causes and consequences of health deviant behavior, as well as how they managed to cope with situations caused by health deviant behavior. A professional counselor also checked the questionnaire for possible leading questions that could potentially result in biased responses. Finally, a pilot study was conducted to pre-test the potential respondents' understanding of the questionnaire.
The researcher obtained informed consent from the participants before starting the study. Participation in the study was entirely voluntary. Participants were free to answer any questions. However, the questionnaire was designed to limit the possibility of uncomfortable questions. The collected data was kept in private property and was not shared with third parties.
The collected data in the quantitative part of the research were described as frequency, mean and standard deviation. Data analysis was performed using SPSS 22 software. First, the normality of data distribution was checked by the Kolmogorov-Smirnov test. Then, the Pearson correlation test was used to examine the correlation between variables.
Findings
One hundred forty-two students answered the questionnaire, of which 56% were female.
74% of students (18% male and 56% female) were responsible for health deviant behavior, and 26% were influenced by others. 38% consumed alcoholic beverages. The reason for alcohol consumption in 27% was entertainment and in 42% was stress coping. 40% recognized that alcohol consumption by young people is the main cause of deviant health behavior. 16% of male students smoked with their peers. 40% of respondents said smoking is a bad habit, and 2% said smoking is not bad. 76% were familiar with illegal drugs. 38% had suicidal thoughts, and 8% had attempted suicide. 65% of the subjects enjoyed computer games and did not think that it was health deviant behavior. 3% Looked at pornographic content.
Table 1) Mean scores of research variables and matrix of correlation coefficients between them
There was a significant positive correlation between health deviant behavior and vulnerability to negative peer influence. The more health deviant behavior respondents engage in, the more aggressive they become and the more vulnerable to negative peer influences. Relatively weak and negative correlations were found between self-esteem and health deviant behavior and vulnerability to the negative peer influence and self-esteem. Thus, the lower the self-esteem of a deviant adolescent, the more susceptible they are too negative peer influences and the more likely they to engage in various types of health deviant behavior (Table 1).
Discussion
This aspect has not been covered in previous studies, even though the concept of deviance is closely linked to the definition of the social norm, which was formulated almost a century ago. Indeed, the behavior of an increasing number of adolescents and young people is characterized by deviance. Normally, adolescents learn patterns of social adjustment. On the contrary, health deviant behavior leads to a conflict with social values. Nevertheless, despite numerous studies, the problem of health deviant behavior is not still fully understood.
Adolescence is characterized by unpredictable behavior, emotional distress, and rebellion. Adolescents in this stage of life strive for independence, develop a self-image, and experiment with the behavioral norms of the adult society and seek to gain trust and acceptance of people around them, especially their peers [11]. School and family are the contexts for adolescent growth, where adolescents develop psychologically and strive to show signs of maturity, shaping their self-image and learning appropriate social behaviors.
Researches show that when adolescents leave their parents to live independently, peer acceptance is of utmost importance to them [12, 13]. Adolescents may face many challenges in establishing their self-identity and integration into society. From this perspective, deviant health behavior can be seen as a sign of growth and independence. However, if confidence and acceptance cannot be gained in traditional groups (e.g., school and family), personal values and self-concepts may be underdeveloped. Consequently, adolescents may feel motivated to pursue life satisfaction and meet their psychological needs through a peer group. In this case, adolescents are likely to underestimate the social appropriateness of social interactions, at the expense of which adolescents gain a sense of acceptance by their peer group. Indeed, the subtle relationships between health deviant behavior and adolescent self-concept need to be considered [14-16].
Adolescents with less good academic performance tend to band together in the name of group support [17], aimed at jointly overcoming the dilemma of choosing between doing well and receiving praise from teachers or doing poorly but being accepted by peers. Cohesive group behavior may be criminal by nature. Nevertheless, involvement in it is necessary to gain acceptance from their peers.
In socio-psychological research on youth health deviant behavior in modern society, it is generally accepted that the possession of developed self-respect is evidence of a developed self-understanding and self-esteem, which allows individuals to treat themselves and others equally, effectively achieve self-integration and develop their potential, and have a higher expectation of self-efficacy [18]. There are several ways in which young people can make positive perceptions of themselves. Sources of respect can be found in the people around them (family, teachers, peers), which on the one hand prevents young people from developing low self-esteem and, on the other hand, also allows them to face challenges and failures with confidence, establishing confident and stable friendships and enabling them to establish and maintain positive relationships with family members and teachers. It makes sense to talk about a positive correlation between high self-esteem and assertive behavior [19].
Sociologists and psychologists have long considered self-esteem an important cause and consequence of deviant health behavior, suggesting that health deviant behavior can function as an adaptive mechanism of the individual and provide psychological self-protection. If self-respect and positive self-esteem cannot be gained through socially acceptable methods, the motivation for such (positive) behavior will gradually decrease. Instead, you can try to achieve self-respect and attention through other means, including health deviant behavior. Thus, low self-esteem is often seen as a motivation for deviant health behavior. It is not the health deviant behavior itself that boosts the adolescent's self-esteem, but the recognition he receives from deviant peers after committing a deviant act [20], which strengthens the psychological connection with other deviant adolescents during similar behavior. Thus, there is no direct link between health deviant behavior and self-esteem, increasing through illicit behavior.
The causes of health deviant behavior are related to upbringing conditions, physical development, and social environment [21]. In assessing his behavior, the adolescent notes the norm, his physical superiority or inferiority, and concludes his social significance and value. The child may have either a passive attitude towards physical weakness, a desire to compensate for weaknesses, or a desire to overcome them through physical exercise. Sometimes the neuromuscular retardation affects the coordination of movements and manifests itself clumsily. Adolescents' health deviant behavior includes anti-social, criminal, illegal, aggressive, self-destructive, and suicidal behavior. These actions can lead to various deviations in personal development. Often such deviations include the reaction of adolescents to difficult life circumstances.
Judgments and minor comments by others about the appearance and awkwardness of teenagers provoke strong feelings and distort the teenagers' behavior. Tallboys are confident in their strength and masculinity and do not have to struggle to earn the respect of their peers. Thus, they behave more naturally and require less attention to themselves. Because of their self-confidence, other children perceive tallboys as very intelligent. Skinny, short, developmentally disabled boys are considered immature by others, so they become rebellious and need constant supervision. To change their self-image, they have to be flexible and courageous and constantly prove their value and competitiveness among their peers [22]. Consequently, emotional tension and communication difficulties inevitably arise, pushing adolescents to break common rules and norms.
Health deviant behavior in adolescents is often caused by social issues, particularly lack of education and upbringing. Crime in most cases originates at home. The first seeds of deviance are planted either out of fear of punishment or out of protest, which then develops into a reflex-like stereotype [23]. The causes of deviant and delinquent behavior in adolescents are the lack of supervision, lack of attention from relatives, fear of punishment, desire to escape from parental care, parental abuse, and unmotivated desire to change the status quo. Separately, it should be noted that early alcohol and drug abuse among adolescents is motivated by a desire to feel like an adult, satisfy curiosity, or change the prevailing mental state [24, 25]. After drinking alcohol, a cheerful mood appears self-confidence and disinhibition increase. Group addiction that occurs when drinking with friends is likely to lead to alcoholism.
As a rule, the starting point and often the only factor contributing to adolescents' social adjustment with health deviant behavior is an external social requirement to behave in a way that conforms to rules and norms. However, this external requirement does not stimulate the experience of positive emotional reactions. We are talking about the fact that a teenager does not have an internal motivation for social adaptation. The educational institution must provide these external requirements to deviant adolescents. It can be said that there is a contradiction here since the government has assigned this responsibility to parents. In practice, however, the main role of educational institutions is to educate children and young people. In our opinion, this is due to the inability of the family to take on such a burden due to material difficulties and a limited understanding of specific characteristics of adolescent development. As people grow up and learn, they either fully, partially accept, or completely reject the life values promoted by educational institutions. Positive social adaptation is achieved when living in an educational institution is fulfilling and attractive, when it creates opportunities to socialize with peers, and a desire for interpersonal communication. Indeed, children with deviant health behavior mostly live in the community in families with no second parent, or this social unit is dysfunctional, so they need special help to coordinate their behavior.
A correlation between negative self-esteem and naughty behavior suggests that adolescents with low self-esteem can increase their self-esteem by engaging in healthy deviant behavior, whereas this effect is not seen among adolescents with high self-esteem. Adolescents may increase their self-esteem through participation in naughty behavior, but a similar effect was not seen in adolescents with high self-esteem. The possible social factors that play a role in creating these problems are, most importantly, the family, the educational community, and the influence of peers. To these should be added some psychological factors such as self-concept and personal values. Correlations show that the more aggressive the respondents' behavior towards their parents and the less motivated they are to study seriously, the lower their self-esteem. However, aggressive behavior towards teachers is noticeably different from aggressive behaviors towards parents and the effect of poor motivation to study seriously, as no significant relationship was found between aggressive behavior towards teachers and respondents' self-esteem. Health deviant behavior can be seen as another manifestation of prosocial behavior, in which the seriousness of recognition by peers is achieved by engaging inappropriate, serious acts of health deviant behavior. Enhancing young people's self-esteem by attracting peer attention through participation in health deviant behavior is a significant factor in the vulnerability of adolescents to peer influence. This socio-psychological mechanism acts as a vicious circle for deviant adolescents. Initially, when health deviant behavior begins, adolescents' self-esteem is relatively low, with a strong desire to be accepted by peers. Once an adolescent's reputation in their peer group for health deviant behavior is established, the adolescent gradually becomes a role model among peers, ceasing to experience the influence of peers on his behavior. Deviant adolescents may have relatively low self-esteem in the initial stages of health deviant behavior, but self-esteem increases significantly when adolescent health deviant behavior is supported by peers.
We can suggest that a key to aggression in health deviant behavior appears to be the creation of a negative mental schema for health deviant behavior. Meanwhile, in adolescents whose needs have been systematically neglected, the lack of a mental schema into which the needs of others are embedded is central. Future research should focus in-depth on these parameters, undoubtedly reflected in the impact of negative experiences on the individual. The age of participants in our study leaves opens the possibility of turning deviant health behavior into chronic. This requires, above all, the active establishment and specialized training of networks involved in identifying deviant health behavior, including educational, health, and justice institutions. They would provide a valuable opportunity to develop social-psychological skills such as empathy and understanding other people's emotions, which is very useful in nurturing altruistic behavior in young people without learning such skills at an earlier age.
The study results enable us to reasonably assert that socio-psychological factors are statistically significant concerning health deviant behavior among young people in the study area. The study rejected the null hypothesis about the absence of a link between socio-psychological factors and health deviant behavior among young people in the study area and adopted an alternative hypothesis. Thus, the study concludes a relationship between socio-psychological factors and health deviant behavior among young people in the study area. In other words, there is a relationship between health deviant behavior and lack of social skills, influence from peers and family.
Despite the valuable results received, it should be noted that this study is not without some limitations. The point is that all variables in this study were measured using self-reports. This method of psychological measurement allows one to have difficulty remembering childhood events. However, the age of the participants in our study is quite young, and therefore, in our opinion, respondents should not experience serious problems in recalling relatively recent events. Moreover, the questionnaire offered to the respondents did not consider the intensity, frequency, duration, or in some cases, the specific culprit of each negative life event.
Conclusion
The causes of health deviant behavior in students lie in the characteristics of the relationship and interaction of the individual with the surrounding world and the social environment. The main reasons for health deviant behavior appear to be biological, psychological, and social. Biological reasons are expressed by the physiological characteristics of adolescence. Psychological reasons lie in temperament and accentuations and the interaction of the teenager with society, family, and school. Thus, the reasons for health deviant behavior can be reduced to the characteristics of the individual, the conditions of the social environment, education, upbringing, and social activity. Students should participate in cooperative or extra-curricular activities to reduce stress and anxiety and channel their health deviant behavior constructively. Active participation in activities organized at the place of study can help develop their potential and increase their self-confidence and self-esteem, thus acting as a protective factor against health deviant behavior. Students seek moral and psychological support from peers, including deviant peers; in times of stress and anxiety, they should be taught how to resist unwanted peer pressure with appropriate social skills. In conclusion, changing the deviant identity of adolescent students is central to social work with young people. Social work in an educational institution should prepare deviant young people for new roles. However, concerns about their previous health deviant behavior create obstacles to positive change, so relapses in health deviant behavior are not excluded, which can be overcome by developing sports talents, providing volunteer services, developing mentoring, and creating role models able to reinforce self-esteem, keeping them on track gradually.
Acknowledgments: -
Ethical Permissions: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the National Ethics Commission of the Ministry of Health of the Russian Federation, September 1, 2021, No 0901-5.
Conflict of Interests: The authors declare no conflict of interest.
Authors’ Contribution: Natalia Skok (First Author), Original Researcher/Methodologist (40%); Igor Fomichev (Second Author), Introduction Writer/Discussion Writer (35%); Arina Zinenkova (Third Author), Introduction Writer/Assistant Researcher (25%).
Funding/Support: -
Article Type: Qualitative Research |
Subject:
Spiritual Health
Received: 2021/09/5 | Accepted: 2021/09/14 | Published: 2021/11/12
Received: 2021/09/5 | Accepted: 2021/09/14 | Published: 2021/11/12
References
1. Conyers A, Calhoun TC. Deviance today. 2nd Edition. New York: Routledge; 2020. [Link] [DOI:10.4324/9781003053286]
2. Newman S. Vygotsky, Wittgenstein, and sociocultural theory. J Theory Soc Behav. 2018;48(3):350-68. [Link] [DOI:10.1111/jtsb.12174]
3. Šmelová E. L.S. Vygotsky and his theory as an inspiration for innovations in education. Int J Innovation Educ Res. 2020;9(2):226-38. [Link] [DOI:10.31686/ijier.vol9.iss2.2944]
4. Adams J, Millie A. Everyday moral judgements of anti-social behavior. Crime Prev Community Saf. 2021;23:56-68. [Link] [DOI:10.1057/s41300-020-00106-6] [PMCID]
5. Loeb EL, Kansky J, Tan JS, Costello MA, Allen JP. Perceived psychological control in early adolescence predicts lower levels of adaptation into mid-adulthood. Child Dev. 2020;92(2):158-72. [Link] [DOI:10.1111/cdev.13377] [PMID] [PMCID]
6. Packer DJ, Ungson ND, Marsh JK. Conformity and reactions to deviance in the time of COVID-19. Group Processes Intergroup Relat. 2021;24(2):311-7. [Link] [DOI:10.1177/1368430220981419]
7. Hilbert RE, Wright CW. On the sociology of deviant behavior. Stillwater: New Forums Press; 2020. [Link]
8. Stewart T. Stammering resources for adults and teenagers. Integrating new evidence into clinical practice. 1st Edition. New York: Routledge; 2021. [Link] [DOI:10.4324/9780429263835-1]
9. Zraick RI, Azios M, Handly MM, Bellon-Harn ML, Manchaiah V. Quality and readability of internet information about stuttering. J Fluency Disord. 2021;67:105824. [Link] [DOI:10.1016/j.jfludis.2020.105824] [PMID]
10. Stanier J, Miglio N. Painful experience and constitution of the intersubjective self: a critical-phenomenological analysis. In: Ferrarello S, editor. Phenomenology of bioethics: Technoethics and lived-experience. 2021;84:101-4. [Link] [DOI:10.1007/978-3-030-65613-3_8] [PMID]
11. Bibi S, Masood S, Mussawar B, Khaliq A. Relationship between self concept and deviant behavior among adolescents. Sci J Neurol Neurosurg. 2021;7(1):7-13. [Link]
12. Busching R, Krahé B. With a little help from their peers: The impact of classmates on adolescents' development of prosocial behavior. J Youth Adolesc. 2020;49:1849-63. [Link] [DOI:10.1007/s10964-020-01260-8] [PMID] [PMCID]
13. Pechmann C, Catlin JR, Zheng Y. Facilitating adolescent well-being: A review of the challenges and opportunities and the beneficial roles of parents, schools, neighborhoods, and policymakers. J Consum Psychol. 2020;30(1):149-77. [Link] [DOI:10.1002/jcpy.1136]
14. Singam V, Rastogi S, Patel KR, Lee HH., Silverberg JI. The mental health burden in acne vulgaris and rosacea: an analysis of the U.S. National Inpatient Sample. Clin Exp Dermatology. 2019;44(7):766-72. [Link] [DOI:10.1111/ced.13919] [PMID]
15. Natsuaki MN, Yates TM. Adolescent acne and disparities in mental health. Child Dev Perspect. 2021;15(1):37-43. [Link] [DOI:10.1111/cdep.12397]
16. Pape H, Rossow I. Less adolescent alcohol and cannabis use: More deviant user groups? Drug Alcohol Rev. 2021;40(1):118-25. [Link] [DOI:10.1111/dar.13146] [PMID]
17. Asiyai RI. Deviant behavior in secondary school and its impact on students' learning. J Educ Soc Res. 2019;9(3):170-7. [Link] [DOI:10.2478/jesr-2019-0034]
18. Hoeben EM, Osgood DW, Siennick SE. Hanging out with the wrong crowd? The role of unstructured socializing in adolescents' specialization in delinquency and substance Use. J Quant Criminol. 2021;37:141-77. [Link] [DOI:10.1007/s10940-019-09447-4]
19. Novita E, Warsono W, Wisnu W. Discourse on adolescent deviant behavior on social media Facebook: Indonesian youth group caption. Int J Educ Vocational Stud. 2020;2(10):828-36. [Link]
20. Adegunju KA. Influence of parental monitoring on adolescents' deviant behaviors as expressed by married adults in Ilorin metropolis. Mimbar Sekolah Dasar. 2020;7(3):269-83. [Link] [DOI:10.17509/mimbar-sd.v7i3.27425]
21. Thompson EL, Mehari KR, Farrell AD. Deviant peer factors during early adolescence: cause or consequence of physical aggression? Child Dev. 2020;91(2):415-31. [Link] [DOI:10.1111/cdev.13242] [PMID] [PMCID]
22. Marandi PK, Salamudin N. Body image appearances in adolescents schoolchildren. Malays J Mov Health Exercise. 2020;9(1):195-206. [Link] [DOI:10.15282/mohe.v9i1.409]
23. Gong X, Wu L, Cong J. Analysis of factors affecting tolerance of deviant behavior based on CGSS2015 data. Adv Soc Sci Educ Humanit Res. 2021;516:142-7. [Link] [DOI:10.2991/assehr.k.210120.028]
24. Li J, Zhan D, Zhou Y, Gao X. Loneliness and problematic mobile phone use among adolescents during the COVID-19 pandemic: The roles of escape motivation and self-control. Addict Behav. 2021;118:106857. [Link] [DOI:10.1016/j.addbeh.2021.106857] [PMID]
25. Oosterhoff B, Palmer CA, Wilson J, Shook N. Adolescents motivations to engage in social distancing during the COVID-19 pandemic: Associations with mental and social health. J Adolesc Health. 2020;67(2):179-85. [Link] [DOI:10.1016/j.jadohealth.2020.05.004] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |