



Volume 10, Issue 2 (2022)
Health Educ Health Promot 2022, 10(2): 395-401 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Moradzadeh R, Nazari J, Orouji A, Zamanian M, Shamsi M, Chezani-Sharahi N. Health Literacy among Mothers with Children under 6 Years Old, a Population-based Cross-Sectional Study in Iran, 2019-20. Health Educ Health Promot 2022; 10 (2) :395-401
URL: http://hehp.modares.ac.ir/article-5-54870-en.html
URL: http://hehp.modares.ac.ir/article-5-54870-en.html
1- Department of Epidemiology, School of Health, Arak University of Medical Sciences, Arak, Iran
2- Department of Pediatrics, School of Medicine, Arak University of Medical Sciences, Arak, Iran
3- Department of Health Education and Promotion, Faculty of Health, Khomein University of Medical Sciences, Khomein, Iran
4- Department of Health Education and Promotion, Faculty of Health, Arak University of Medical Sciences, Arak, Iran
5- Health System Research, Arak University of Medical Sciences, Arak, Iran
2- Department of Pediatrics, School of Medicine, Arak University of Medical Sciences, Arak, Iran
3- Department of Health Education and Promotion, Faculty of Health, Khomein University of Medical Sciences, Khomein, Iran
4- Department of Health Education and Promotion, Faculty of Health, Arak University of Medical Sciences, Arak, Iran
5- Health System Research, Arak University of Medical Sciences, Arak, Iran
Full-Text [PDF 838 kb]
(3683 Downloads)
| Abstract (HTML) (2472 Views)
Table 2) Association between health literacy and independent variables in adjusted models among mothers of children under 6 years old
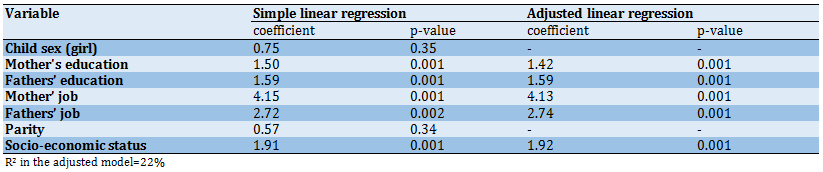
Table 3) Health literacy subscales and percentage among mothers of children under 6 years old (N=1483)

Discussion
The results indicated that the mean score of health literacy was 70.2 in mothers and 36.4% of the participants had adequate health literacy. the study findings were in line with the results of some studies and inconsistent with some studies conducted in this field [21]. In the study of Bashirian in mothers of children under the age of 5 years, the average health literacy score of mothers was 66.98% out of which 32.1% had an inadequate level of health literacy. mothers with occupation and education had different levels of health literacy while mothers who were employees with a university degree had significantly higher levels of health literacy [1]. The effective factors in increasing the level of health literacy in mothers with children under 6 years old, may refer to the education level and their responsibility for their children's health and seeking information about their growth and health. Mothers in this group care more about their children's growth and illness; Therefore, mothers with children under 6 years old are expected to have a good health literacy level [22]. In this regard, the results of some studies have reported low levels of health literacy, which may be attributed to the differences in the target groups of the study; so most of these studies were conducted on ordinary people in the community and not just on mothers with children under 6 years old [23].
The results of this study showed that the education level of the participants was directly associated with their health literacy and the highest mean score of health literacy was related to mothers with university education which was the difference with mothers that have primary education. It may be stated that academic achievement compared to people who have only elementary education causes significant and wide differences in health literacy and the benefits of higher education for health literacy are very obvious. Also, ignoring other differences, the education level of mothers has the most important effect. It has been shown in other studies that parental health literacy is also associated with the low education level of mothers [24-26].
The results of the present study also showed that the education level of the husbands is directly related to the health literacy level of mothers, so the average score of health literacy in mothers whose husbands' education level were elementary school and academic degree were 58.5 and 83.4respectively and There was a significant difference in the mean score of health literacy. It seems to be due to the participatory role of spouses in raising children and the direct relationship between parent's education level and their average scores of health literacy. Also, men with higher education have wives with the same education level and their average scores of health literacy are higher. The direct relationship between education and health literacy has been confirmed in a study by Pirzadeh et al. [27] in Yazd. Also, most Iranian women have a high level of education and university degree today, and as a result, the average score of health literacy is higher for them and also for their husbands. This direct relationship has been shown in most studies conducted in the field of health literacy and education level [21, 28].
In the present study, the mean scores of health literacy and standard deviation in unemployed women and women with temporary and permanent jobs were 71.9±14.7, 81.5±14.7, and 85.3±14.5, respectively. Mothers with full-time jobs had the best health literacy scores. It seems that employed people have the highest education level and also more social interactions and better SES. Also, these people have stronger and larger social and organizational networks and health literacy information can be obtained from these social networks. In previous international studies, health literacy was positively associated with employment, net household income, and perceived social status [26, 29].
The findings from another study showed that the average score of health literacy was 61.2 and 79.3 in mothers with low SES and mothers with the highest level of SES and this difference was statistically significant in mean scores. Also, the findings of a study by Lee et al. in 2016, showed that low-income mothers have infants with relatively low functional health literacy and maternal health literacy is relatively low in this group [30]. The findings emphasized the importance of SES and its impact on health literacy. Poverty and inequality in health are derived from inequality in life and society. Fair access to health services and lack of employment are directly related to SES. According to the National Adult Literacy Survey (NAAL) in the United States, low-income adults have lower health literacy than middle-income adults [31], and 30% of the people receiving health care have "sub-basic" health literacy. Between one-third and one-half of the middle-aged population in the United States have low health literacy, and ethnic minorities and the poverty and injustice in health stem from poverty and injustice in society. Also, information on parental health literacy concerning child health showed that parents with low SES had lower health literacy. Also, low parental health literacy is negatively associated with not being covered by insurance and also living in single-parent families [32-34].
Based on the findings of the present study, there is a negative relationship between the number of children and the mean scores of health literacy, so the mean score of health literacy and standard deviation in mothers with one child is 71.0±17.0 and the same scores for mothers with three and four children were 66.9±16.6 and 60.1±21.2, respectively. These scores were significantly different from each other. It seems that the health literacy scores decrease rapidly following an increase in the number of children, and this decrease was evident even in mothers with two children, 70.3±18.1. Women with four or more children also appear to have lower scores in health literacy due to lower education levels and SES. In the other studies, the results were slightly different, so the health literacy of mothers increased slightly in families with a maximum of four children. Mothers with five or more children have the least knowledge about children's health issues [8]. Unfortunately, it seems that the population policies adopted to reduce the population in the previous decades have had more effects on mothers with higher education and literacy. And according to the results of this study and other findings, these families usually have a better SES. Also, according to the findings of this study, the maternal job was the most predictive factor among the demographic factors affecting health literacy including the mother’s and husband’s education, mother’s and husband’s job, the number of children, and economic and social status. The results of a study on women's health literacy by Agnes in Romania in 2019, showed that full-time mothers have the best health literacy scores [27]. It can be stated that a mother’s job provides better opportunities for social communication and women with higher education also find better jobs.
Besides, according to the Health Literacy Questionnaire for Iranians in the present study, 23.1% of the participating mothers had excellent health literacy, 36.4% had adequate health literacy, 27.9% had partial health literacy, and 12.6% had inadequate health literacy. In a study by Hakkak et al. on health literacy in pregnant women, 61.9% of the participants had excellent health literacy and 36.3% had adequate health literacy [21]. In a study on health literacy in the elderly, the findings were different [35] which could be related to the different SES and measurement tools. Also, based on these findings, most of the participants were skilled enough in the health literacy subgroups such as evaluation (30.0%), decision making (39.5%), comprehension (33.3%), and reading (36.1%), and access to information (34.7%). The decision-making skill of mothers and also the role of other family members in health-related behaviors seem to be so crucial. Shannon emphasized the role of family members in adopting the health literacy subgroups and making the right health decisions in a study on maternal health literacy in Vietnam [36].
There were some limitations in this study. Some variables were self-reported data and may be potentially susceptible to misclassification bias. Moreover, as the study was population-based, the response rate was high, and sufficient sample size, the possibility of selection bias was limited and the results could be representative of the source population.
Conclusion
It was concluded that the health literacy of the mothers was relatively high. The important determinants of health literacy included the mother’s and husband’s education, the mother’s and husband’s job, and SES. It was recommended to the health policy-makers to consider health literacy in strategic planning for the prevention education and self-care approaches.
Acknowledgments: None declared.
Ethical Permissions: Ethic approval was achieved from the Ethics Committee of Arak University of Medical Sciences IR.ARAKMU.REC.98.217.
Conflicts of Interests: The authors declare no conflict of interest.
Authors’ Contributions: Moradzadeh R (First Author), Methodologist/Main Researcher/Statistical Analyst (20%); Nazari J (Second Author), Introduction Writer/
Main Researcher/Discussion Writer (20%); Orouji A (Third Author), Introduction Writer/Assistant Researcher/Discussion Writer (10%); Zamanian M (Forth Author), Introduction Writer /Discussion Writer (5%); Shamsi M (Fifth Author), Statistical Analyst (5%); Chezani-Sharahi N (Sixth Author), Introduction Writer/
Methodologist/Main Researcher/Discussion Writer (40%)
Funding/Support: This work was supported by Arak University of Medical Sciences (grant number: 3112).
Full-Text: (669 Views)
Introduction
Health literacy is “the degree to which individuals can obtain, process, and understand basic health information and services needed to make appropriate health decisions”. In a report, the World Health Organization identified health literacy as a global issue and one of the biggest contributing factors to health. They also recommended the formation of an association to monitor and organize strategies to increase the level of health literacy in different countries [1, 2]. The issue of health literacy with the aim of a healthy and capable society is clearly stated in the vision of the health system map of the Islamic Republic of Iran by 2025 [3]. Health literacy is a crucial predictor of health outcomes [4]. In recent years, the concept of health literacy has received increasing attention in public health research. It is also known in health care reform processes and is currently one of the main factors in the use of personal health services and determining factors in this field [5]. Low health literacy is associated with an increased risk of emergency care and hospitalization, poor adherence to the medication regimen, and a higher mortality rate. Lower health literacy in the population is associated with a higher incidence of chronic illness, poorer self-reported health, lower utilization of preventive health services, higher rates of hospitalization, and higher health care costs [6]. Health literacy is a social determinant of health that can be improved through intervention. Health literacy can be effective by empowering people to overcome health barriers [7]. It is considered an asset for the development of social capital and responding to health inequalities as well as a key component for population health [8]. Recently, health literacy has been recognized as an important skill for patients to make appropriate health decisions in difficult situations ahead. Improving people's health literacy leads to consequences such as increasing patients' potential ability to make informed decisions, reducing health risks, increasing disease prevention, improving safety, increasing the quality of life, and increasing the quality of care for individuals [7-9]. Literacy and numeracy are particularly important for parents of infants because they must use literacy and math in their children’s care: They must measure baby formula, read thermometers, and use over-the-counter (OTC) and prescription medications [9].
The level of health literacy in people is so low that in developed countries such as the United States, nearly 92 million people have a low level of health literacy and it has led to an increase in hospitalization rates and the use of emergency services. It has cost the health system economy $ 19 billion a year. In a meta-analysis study which has summarized the results of 85 different studies, the percentage of insufficient and borderline literacy in the United States was estimated to be 25% and 20%, respectively. A study conducted in Hebei Province, China, has reported that the health literacy level (19%) is significantly higher in urban residents than that in rural residents (7.94%) [10].
The results of the study Tehrani in 2007 showed that 28.1% of the subjects studied adequate health literacy, 15.3 % of borderline health literacy, and 66% were inadequate health literacy. The results of the present study showed that the mean score of total health literacy was for men (67.6) and women (69.02) and this difference was due to the sample size [11].
Mothers who focus on maintaining a healthy family are counted [12]. Because they are the primary caregivers of the babies and will spend more time with their babies. Mothers need to develop and adapt to their babies [13, 14]. Low Maternal Health Literacy Adverse Effects It will affect the health of the child. Including effects Can be directly attributed to medication errors and Indirect effects can increase the incidence of chronic diseases He mentioned the cost of health care, low physical activity, and overweight children [15-17]. In contrast, promoting health literacy Proper physical growth, and Seeking to strengthen the emotional bond between mother and child [18]. Awareness of a population's health knowledge and focus on Health and care planning on the weaknesses of health literacy in Educational planning is required. Therefore due to the high importance of health literacy to understand health messages and decision-making True, it is essential to assess the level of maternal health literacy and current status and adopt additional studies to present Measure effective protocols in promoting community health.
Previous studies in this field are from many years ago, and since the pattern of population health literacy may have changed over the years, we decided to implement this article in Arak; therefore this study aimed to evaluate the level of health literacy of mothers of children referrals to health centers under the auspices of the University of Medical Sciences.
Instrument and Methods
This population-based cross-sectional study was conducted in Arak, Iran from January 2019 to January 2020. Among all of the eligible mothers included in the study (N=37172), 1754 mothers with children under 6 years old were invited through stratified random sampling. Among them, 1483 (response rate=85%) mothers agreed to participate in the study. We divided Arak into 50 categories based on the area under the coverage of 50 health care centers. Among these 50 categories based on the SIB (SAMANEH YEKPARCHE BEHDASHT: Integrated Health System) registry, that list of all eligible mothers is registered, and the required sample size was included by simple random sampling considering the size of the category to be representative of the whole city. Mothers with children under 6 years old, Iranian nationality, and the ability to communicate in Persian were included.
The questionnaires were interviewer-administered and collected on an Android app on the interviewers’ cell phones. To validate data collection, the interviewers of the study participated in the relevant training courses.
Health literacy was assessed by Health Literacy for Iranian Adults (HELIA) questionnaire on a 5-point Likert scale. HELIA consists of 33 items in 5 subscales (access to information (6 items), reading (4 items), understanding (7 items), appraisal (4 items), and decision-making/behavioral intention (12 items)). Tavousi et al. [3] developed and validated the HELIA questionnaire; confirmatory factor analysis indicated a good fit to the data for all subscales and Cronbach's alpha coefficients were from 0.72 to 0.89. Furthermore, the intraclass correlation coefficient was reported at an acceptable level (0.84). Other included variables of the study were children’s age (years) and sex (male/female), Mother’s education (Illiterate and preliminary, Guidance school, High school, Diploma, Higher diploma, undergraduate and postgraduate), husband’s education (Illiterate and preliminary, Guidance school, High school, Diploma, Higher diploma, undergraduate and postgraduate), mother’s job (unemployed, housekeeper, temporary job, permanent job), husband’s job (unemployed, temporary job, permanent job), parity (count), and Socio-economic status (SES; 1st to 5th quintiles based on assets). SES was obtained based on the assets, including the owner of the usual refrigerator, side-by-side refrigerator, color TV, LCD TV, LED TV, cell phone, washing machine, dishwasher, microwave, vacuum cleaner, motorcycle, laptop, access to the internet at home, car, home, number of bedrooms, sanitation facility, bathroom, cooling equipment, heating devices, cooking equipment and place of cooking at home.
This work was approved by the etic committee of Arak University of Medical Sciences. A face-to-face interview was applied to collect data. The interview was conducted on the doorstep of the participants and took 15-20 minutes to complete the study questionnaire.
To calculate each subscale and total score for the HELIA, we used a scoring manual based on the study [3]. The principal component analysis was applied to calculate SES based on asset indices [19, 20]. Descriptive analysis was conducted for the categorical and continuous variables. Chi-square, analysis of variance (ANOVA), independent t-test, and related non-parametric tests were used to compare mean and median values. The dependent variable in this study was health literacy on a continuous scale. Therefore, linear regression was an appropriate test to analyze the association between study variables. Univariate and adjusted linear regression models were applied to assess the determinants of health literacy. P-values<0.05 were considered statistically significant. The analysis was conducted in SPSS 16.0 and STATA 12.0 software.
Findings
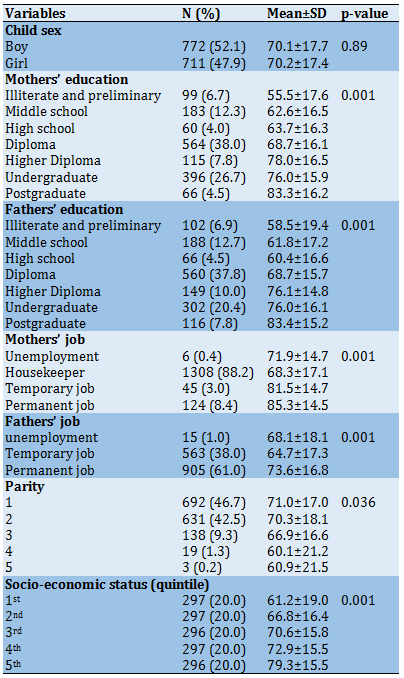
Totally, 1483 mothers with children under 6 years old were included in the study. The mean age of the children was 2.1±1.5. Most of the mothers had a son. Most of the participants were mothers with the diploma, housekeepers, and had just one child (Table 1). In total, the mean score of health literacy in mothers was 70.2±17.5. There was not a significant difference between the health literacy in mothers having sons and mothers having daughters (p>0.05). There was a significant difference in health literacy of the participants due to the mother’s education, husband’s education, mother’s job, husband’s job, parity, and SES (p<0.05).
Table 1) Demographic characteristics of health literacy among mothers with children under 6 years old
In the adjusted model of linear regression, the total health literacy increased following the rise in mothers’ and fathers’ education levels (p=0.001). Moreover, there was a significant difference in the association between mothers’ and their husbands’ permanent jobs and total health literacy (p=0.001). Furthermore, total health literacy was associated with the SES of the participants (Table 2).
Minimum and maximum scores of health literacy were obtained in the appraisal and understanding subscales, respectively. Most of the participants had adequate health literacy in access to information (34.7%), reading (36.1%), understanding (33.3%), appraisal (30%), and decision (39.5%) subscales. In total health literacy, 36.4% of the participants had adequate health literacy (Table 3).
Health literacy is “the degree to which individuals can obtain, process, and understand basic health information and services needed to make appropriate health decisions”. In a report, the World Health Organization identified health literacy as a global issue and one of the biggest contributing factors to health. They also recommended the formation of an association to monitor and organize strategies to increase the level of health literacy in different countries [1, 2]. The issue of health literacy with the aim of a healthy and capable society is clearly stated in the vision of the health system map of the Islamic Republic of Iran by 2025 [3]. Health literacy is a crucial predictor of health outcomes [4]. In recent years, the concept of health literacy has received increasing attention in public health research. It is also known in health care reform processes and is currently one of the main factors in the use of personal health services and determining factors in this field [5]. Low health literacy is associated with an increased risk of emergency care and hospitalization, poor adherence to the medication regimen, and a higher mortality rate. Lower health literacy in the population is associated with a higher incidence of chronic illness, poorer self-reported health, lower utilization of preventive health services, higher rates of hospitalization, and higher health care costs [6]. Health literacy is a social determinant of health that can be improved through intervention. Health literacy can be effective by empowering people to overcome health barriers [7]. It is considered an asset for the development of social capital and responding to health inequalities as well as a key component for population health [8]. Recently, health literacy has been recognized as an important skill for patients to make appropriate health decisions in difficult situations ahead. Improving people's health literacy leads to consequences such as increasing patients' potential ability to make informed decisions, reducing health risks, increasing disease prevention, improving safety, increasing the quality of life, and increasing the quality of care for individuals [7-9]. Literacy and numeracy are particularly important for parents of infants because they must use literacy and math in their children’s care: They must measure baby formula, read thermometers, and use over-the-counter (OTC) and prescription medications [9].
The level of health literacy in people is so low that in developed countries such as the United States, nearly 92 million people have a low level of health literacy and it has led to an increase in hospitalization rates and the use of emergency services. It has cost the health system economy $ 19 billion a year. In a meta-analysis study which has summarized the results of 85 different studies, the percentage of insufficient and borderline literacy in the United States was estimated to be 25% and 20%, respectively. A study conducted in Hebei Province, China, has reported that the health literacy level (19%) is significantly higher in urban residents than that in rural residents (7.94%) [10].
The results of the study Tehrani in 2007 showed that 28.1% of the subjects studied adequate health literacy, 15.3 % of borderline health literacy, and 66% were inadequate health literacy. The results of the present study showed that the mean score of total health literacy was for men (67.6) and women (69.02) and this difference was due to the sample size [11].
Mothers who focus on maintaining a healthy family are counted [12]. Because they are the primary caregivers of the babies and will spend more time with their babies. Mothers need to develop and adapt to their babies [13, 14]. Low Maternal Health Literacy Adverse Effects It will affect the health of the child. Including effects Can be directly attributed to medication errors and Indirect effects can increase the incidence of chronic diseases He mentioned the cost of health care, low physical activity, and overweight children [15-17]. In contrast, promoting health literacy Proper physical growth, and Seeking to strengthen the emotional bond between mother and child [18]. Awareness of a population's health knowledge and focus on Health and care planning on the weaknesses of health literacy in Educational planning is required. Therefore due to the high importance of health literacy to understand health messages and decision-making True, it is essential to assess the level of maternal health literacy and current status and adopt additional studies to present Measure effective protocols in promoting community health.
Previous studies in this field are from many years ago, and since the pattern of population health literacy may have changed over the years, we decided to implement this article in Arak; therefore this study aimed to evaluate the level of health literacy of mothers of children referrals to health centers under the auspices of the University of Medical Sciences.
Instrument and Methods
This population-based cross-sectional study was conducted in Arak, Iran from January 2019 to January 2020. Among all of the eligible mothers included in the study (N=37172), 1754 mothers with children under 6 years old were invited through stratified random sampling. Among them, 1483 (response rate=85%) mothers agreed to participate in the study. We divided Arak into 50 categories based on the area under the coverage of 50 health care centers. Among these 50 categories based on the SIB (SAMANEH YEKPARCHE BEHDASHT: Integrated Health System) registry, that list of all eligible mothers is registered, and the required sample size was included by simple random sampling considering the size of the category to be representative of the whole city. Mothers with children under 6 years old, Iranian nationality, and the ability to communicate in Persian were included.
The questionnaires were interviewer-administered and collected on an Android app on the interviewers’ cell phones. To validate data collection, the interviewers of the study participated in the relevant training courses.
Health literacy was assessed by Health Literacy for Iranian Adults (HELIA) questionnaire on a 5-point Likert scale. HELIA consists of 33 items in 5 subscales (access to information (6 items), reading (4 items), understanding (7 items), appraisal (4 items), and decision-making/behavioral intention (12 items)). Tavousi et al. [3] developed and validated the HELIA questionnaire; confirmatory factor analysis indicated a good fit to the data for all subscales and Cronbach's alpha coefficients were from 0.72 to 0.89. Furthermore, the intraclass correlation coefficient was reported at an acceptable level (0.84). Other included variables of the study were children’s age (years) and sex (male/female), Mother’s education (Illiterate and preliminary, Guidance school, High school, Diploma, Higher diploma, undergraduate and postgraduate), husband’s education (Illiterate and preliminary, Guidance school, High school, Diploma, Higher diploma, undergraduate and postgraduate), mother’s job (unemployed, housekeeper, temporary job, permanent job), husband’s job (unemployed, temporary job, permanent job), parity (count), and Socio-economic status (SES; 1st to 5th quintiles based on assets). SES was obtained based on the assets, including the owner of the usual refrigerator, side-by-side refrigerator, color TV, LCD TV, LED TV, cell phone, washing machine, dishwasher, microwave, vacuum cleaner, motorcycle, laptop, access to the internet at home, car, home, number of bedrooms, sanitation facility, bathroom, cooling equipment, heating devices, cooking equipment and place of cooking at home.
This work was approved by the etic committee of Arak University of Medical Sciences. A face-to-face interview was applied to collect data. The interview was conducted on the doorstep of the participants and took 15-20 minutes to complete the study questionnaire.
To calculate each subscale and total score for the HELIA, we used a scoring manual based on the study [3]. The principal component analysis was applied to calculate SES based on asset indices [19, 20]. Descriptive analysis was conducted for the categorical and continuous variables. Chi-square, analysis of variance (ANOVA), independent t-test, and related non-parametric tests were used to compare mean and median values. The dependent variable in this study was health literacy on a continuous scale. Therefore, linear regression was an appropriate test to analyze the association between study variables. Univariate and adjusted linear regression models were applied to assess the determinants of health literacy. P-values<0.05 were considered statistically significant. The analysis was conducted in SPSS 16.0 and STATA 12.0 software.
Findings
Totally, 1483 mothers with children under 6 years old were included in the study. The mean age of the children was 2.1±1.5. Most of the mothers had a son. Most of the participants were mothers with the diploma, housekeepers, and had just one child (Table 1). In total, the mean score of health literacy in mothers was 70.2±17.5. There was not a significant difference between the health literacy in mothers having sons and mothers having daughters (p>0.05). There was a significant difference in health literacy of the participants due to the mother’s education, husband’s education, mother’s job, husband’s job, parity, and SES (p<0.05).
Table 1) Demographic characteristics of health literacy among mothers with children under 6 years old
In the adjusted model of linear regression, the total health literacy increased following the rise in mothers’ and fathers’ education levels (p=0.001). Moreover, there was a significant difference in the association between mothers’ and their husbands’ permanent jobs and total health literacy (p=0.001). Furthermore, total health literacy was associated with the SES of the participants (Table 2).
Minimum and maximum scores of health literacy were obtained in the appraisal and understanding subscales, respectively. Most of the participants had adequate health literacy in access to information (34.7%), reading (36.1%), understanding (33.3%), appraisal (30%), and decision (39.5%) subscales. In total health literacy, 36.4% of the participants had adequate health literacy (Table 3).
Table 2) Association between health literacy and independent variables in adjusted models among mothers of children under 6 years old
Table 3) Health literacy subscales and percentage among mothers of children under 6 years old (N=1483)
Discussion
The results indicated that the mean score of health literacy was 70.2 in mothers and 36.4% of the participants had adequate health literacy. the study findings were in line with the results of some studies and inconsistent with some studies conducted in this field [21]. In the study of Bashirian in mothers of children under the age of 5 years, the average health literacy score of mothers was 66.98% out of which 32.1% had an inadequate level of health literacy. mothers with occupation and education had different levels of health literacy while mothers who were employees with a university degree had significantly higher levels of health literacy [1]. The effective factors in increasing the level of health literacy in mothers with children under 6 years old, may refer to the education level and their responsibility for their children's health and seeking information about their growth and health. Mothers in this group care more about their children's growth and illness; Therefore, mothers with children under 6 years old are expected to have a good health literacy level [22]. In this regard, the results of some studies have reported low levels of health literacy, which may be attributed to the differences in the target groups of the study; so most of these studies were conducted on ordinary people in the community and not just on mothers with children under 6 years old [23].
The results of this study showed that the education level of the participants was directly associated with their health literacy and the highest mean score of health literacy was related to mothers with university education which was the difference with mothers that have primary education. It may be stated that academic achievement compared to people who have only elementary education causes significant and wide differences in health literacy and the benefits of higher education for health literacy are very obvious. Also, ignoring other differences, the education level of mothers has the most important effect. It has been shown in other studies that parental health literacy is also associated with the low education level of mothers [24-26].
The results of the present study also showed that the education level of the husbands is directly related to the health literacy level of mothers, so the average score of health literacy in mothers whose husbands' education level were elementary school and academic degree were 58.5 and 83.4respectively and There was a significant difference in the mean score of health literacy. It seems to be due to the participatory role of spouses in raising children and the direct relationship between parent's education level and their average scores of health literacy. Also, men with higher education have wives with the same education level and their average scores of health literacy are higher. The direct relationship between education and health literacy has been confirmed in a study by Pirzadeh et al. [27] in Yazd. Also, most Iranian women have a high level of education and university degree today, and as a result, the average score of health literacy is higher for them and also for their husbands. This direct relationship has been shown in most studies conducted in the field of health literacy and education level [21, 28].
In the present study, the mean scores of health literacy and standard deviation in unemployed women and women with temporary and permanent jobs were 71.9±14.7, 81.5±14.7, and 85.3±14.5, respectively. Mothers with full-time jobs had the best health literacy scores. It seems that employed people have the highest education level and also more social interactions and better SES. Also, these people have stronger and larger social and organizational networks and health literacy information can be obtained from these social networks. In previous international studies, health literacy was positively associated with employment, net household income, and perceived social status [26, 29].
The findings from another study showed that the average score of health literacy was 61.2 and 79.3 in mothers with low SES and mothers with the highest level of SES and this difference was statistically significant in mean scores. Also, the findings of a study by Lee et al. in 2016, showed that low-income mothers have infants with relatively low functional health literacy and maternal health literacy is relatively low in this group [30]. The findings emphasized the importance of SES and its impact on health literacy. Poverty and inequality in health are derived from inequality in life and society. Fair access to health services and lack of employment are directly related to SES. According to the National Adult Literacy Survey (NAAL) in the United States, low-income adults have lower health literacy than middle-income adults [31], and 30% of the people receiving health care have "sub-basic" health literacy. Between one-third and one-half of the middle-aged population in the United States have low health literacy, and ethnic minorities and the poverty and injustice in health stem from poverty and injustice in society. Also, information on parental health literacy concerning child health showed that parents with low SES had lower health literacy. Also, low parental health literacy is negatively associated with not being covered by insurance and also living in single-parent families [32-34].
Based on the findings of the present study, there is a negative relationship between the number of children and the mean scores of health literacy, so the mean score of health literacy and standard deviation in mothers with one child is 71.0±17.0 and the same scores for mothers with three and four children were 66.9±16.6 and 60.1±21.2, respectively. These scores were significantly different from each other. It seems that the health literacy scores decrease rapidly following an increase in the number of children, and this decrease was evident even in mothers with two children, 70.3±18.1. Women with four or more children also appear to have lower scores in health literacy due to lower education levels and SES. In the other studies, the results were slightly different, so the health literacy of mothers increased slightly in families with a maximum of four children. Mothers with five or more children have the least knowledge about children's health issues [8]. Unfortunately, it seems that the population policies adopted to reduce the population in the previous decades have had more effects on mothers with higher education and literacy. And according to the results of this study and other findings, these families usually have a better SES. Also, according to the findings of this study, the maternal job was the most predictive factor among the demographic factors affecting health literacy including the mother’s and husband’s education, mother’s and husband’s job, the number of children, and economic and social status. The results of a study on women's health literacy by Agnes in Romania in 2019, showed that full-time mothers have the best health literacy scores [27]. It can be stated that a mother’s job provides better opportunities for social communication and women with higher education also find better jobs.
Besides, according to the Health Literacy Questionnaire for Iranians in the present study, 23.1% of the participating mothers had excellent health literacy, 36.4% had adequate health literacy, 27.9% had partial health literacy, and 12.6% had inadequate health literacy. In a study by Hakkak et al. on health literacy in pregnant women, 61.9% of the participants had excellent health literacy and 36.3% had adequate health literacy [21]. In a study on health literacy in the elderly, the findings were different [35] which could be related to the different SES and measurement tools. Also, based on these findings, most of the participants were skilled enough in the health literacy subgroups such as evaluation (30.0%), decision making (39.5%), comprehension (33.3%), and reading (36.1%), and access to information (34.7%). The decision-making skill of mothers and also the role of other family members in health-related behaviors seem to be so crucial. Shannon emphasized the role of family members in adopting the health literacy subgroups and making the right health decisions in a study on maternal health literacy in Vietnam [36].
There were some limitations in this study. Some variables were self-reported data and may be potentially susceptible to misclassification bias. Moreover, as the study was population-based, the response rate was high, and sufficient sample size, the possibility of selection bias was limited and the results could be representative of the source population.
Conclusion
It was concluded that the health literacy of the mothers was relatively high. The important determinants of health literacy included the mother’s and husband’s education, the mother’s and husband’s job, and SES. It was recommended to the health policy-makers to consider health literacy in strategic planning for the prevention education and self-care approaches.
Acknowledgments: None declared.
Ethical Permissions: Ethic approval was achieved from the Ethics Committee of Arak University of Medical Sciences IR.ARAKMU.REC.98.217.
Conflicts of Interests: The authors declare no conflict of interest.
Authors’ Contributions: Moradzadeh R (First Author), Methodologist/Main Researcher/Statistical Analyst (20%); Nazari J (Second Author), Introduction Writer/
Main Researcher/Discussion Writer (20%); Orouji A (Third Author), Introduction Writer/Assistant Researcher/Discussion Writer (10%); Zamanian M (Forth Author), Introduction Writer /Discussion Writer (5%); Shamsi M (Fifth Author), Statistical Analyst (5%); Chezani-Sharahi N (Sixth Author), Introduction Writer/
Methodologist/Main Researcher/Discussion Writer (40%)
Funding/Support: This work was supported by Arak University of Medical Sciences (grant number: 3112).
Article Type: Descriptive & Survey |
Subject:
Health Literacy
Received: 2021/08/15 | Accepted: 2022/02/6 | Published: 2022/06/14
Received: 2021/08/15 | Accepted: 2022/02/6 | Published: 2022/06/14
References
1. Bashirian S, Esmaeilpour-Zanjani S. Assessing the health literacy level of mothers of under 5-year-old children with malnutrition. J Holist Nurs Midwifery. 2018;28(3):157-62. [Persian] [Link] [DOI:10.29252/hnmj.28.3.157]
2. Fadaiyan Arani E, Amin Shokravi F, Tavakoli Ghouchani H. The relationship between health literacy and nutrition behaviors in patients with type 2 diabetes mellitus. J North Khorasan Univ Med Sci. 2018;9(4):49-55. [Persian] [Link]
3. Tavousi M, Haeri-Mehrizi A, Rakhshani F, Rafiefar S, Soleymanian A, Sarbandi F, et al. Development and validation of a short and easy-to-use instrument for measuring health literacy: the health literacy instrument for adults (HELIA). BMC Public Health. 2020;656:20. [Link] [DOI:10.1186/s12889-020-08787-2]
4. Peyman N, SamieeRoudi K. Investigating the status of health literacy among health providers of rural area. J Health Lit. 2016;1(1):46-52. [Persian] [Link]
5. McCaffery KJ, Holmes-Rovner M, Smith SK, Rovner D, Nutbeam D, Clayman ML, et al. Addressing health literacy in patient decision aids. BMC Med Inf Decis Mak. 2013;13(suppl 2). [Link] [DOI:10.1186/1472-6947-13-S2-S10]
6. Berkman ND SS, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97-107. [Link] [DOI:10.7326/0003-4819-155-2-201107190-00005]
7. Rowlands G, Shaw A, Jaswal S, Smith S, Harpham T. Health literacy and the social determinants of health: a qualitative model from adult learners. Health Promot Int. 2017;32(1):130-8. [Link]
8. Peerson A, Saunders M. Health literacy revisited: what do we mean and why does it matter?. Health Promot Int. 2009;24(3):285-96. [Link] [DOI:10.1093/heapro/dap014]
9. Ferguson B. Health literacy and health disparities: The role they play in maternal and child health. Nurs Women's Health. 2008;12(4):286-98. [Link] [DOI:10.1111/j.1751-486X.2008.00343.x]
10. Tol A, Pourreza A, Foroshani R, Tavassoli E. Assessing the effect of educational program based on small group on promoting knowledge and health literacy among women with type2 diabetes referring to selected hospitals affiliated to Tehran University of Medical Sciences. Razi J Med Sci. 2013;19(104):10-9. [Persian] [Link]
11. Tehrani Banihashemi S, Amir Khani A, Haghdoust A, Alavian M, Asghari Fard H, Baradaran H, et al. Health literacy in five province and relative effective factors. Strides Dev Med Educ. 2007;4(1):1-9. [Link]
12. Saeedi Koupai M, Motaghi M. Comparing health literacy in high school female students and their mothers regarding women's health. J Health Lit. 2017;1(4):220-9. [Persian] [Link]
13. Baker MJ. Nurse perceptions of engaging low-income depressed mothers in a mental health intervention [dissertation]. Carolina: University of North Carolina at Chapel Hill Graduate School; 2017. [Link]
14. Mörelius E, Hemmingsson H. Parents of children with physical disabilities-perceived health in parents related to the child's sleep problems and need for attention at night. Child Care Health Dev. 2014;40(3):412-8. [Link] [DOI:10.1111/cch.12079]
15. İlgün G, Turaç İS, Orak S. Health literacy. Proc Soc Behav Sci. 2015;174:2629-33. [Link] [DOI:10.1016/j.sbspro.2015.01.944]
16. Jayasinghe UW, Harris MF, Parker SM, Litt J, van Driel M, Mazza D, et al. The impact of health literacy and life style risk factors on health-related quality of life of Australian patients. Health Qual Life Outcomes. 2016;14(1):1-13. [Link] [DOI:10.1186/s12955-016-0471-1]
17. Karimi S, Keyvanara M, Hosseini M, Jafarian M, Khorasani E. Health literacy, health status, health services utilization and their relationships in adults in Isfahan. Health Inf Manag. 2014;10(6):862-75. [Persian] [Link]
18. Howard SN. Health literacy program proposal for health care workers [dissertation]. Unknown city: Walden University; 2016. [Link]
19. Morteza-Nejad SH, Yektakooshali M, Moshtaghikojal S, Salmalian Z, Ramezani A, Esmaeilpourbandboni M. Health literacy and its related factors in infant's mothers. J Educ Community Health. 2019;6(4):239-45. [Persian] [Link] [DOI:10.29252/jech.6.4.239]
20. Moradzadeh R, Nadrian H, Golboni F, Kazemi-Galougahi MH, Moghimi N. Economic inequalities amongst women with osteoporosis-related fractures: an application of concentration index decomposition. Health Promot Perspect. 2016;6(4):190. [Link] [DOI:10.15171/hpp.2016.31]
21. Hakkak HM, Joveini HA, Rajabzadeh RE, Robatsarpooshi DA, Tori NA, Haresabadi ME, et al. Health literacy level and related factors among pregnant women referring to bojnord health centers in 2017. Int J Pharmaceut Res. 2019;11(1):152-8. [Link] [DOI:10.31838/ijpr/2019.11.01.015]
22. Charoghchian Khorasani E, Peyman N, Esmaily H. Measuring maternal health literacy in pregnant women referred to the healthcare centers of Mashhad, Iran, in 2015. J Midwifery Reprod Health. 2018;6(1):1157-62. [Persian] [Link]
23. Corrarino JE. Health literacy and women's health: challenges and opportunities. J Midwifery Women's Health. 2013;58(3):257-64. [Link] [DOI:10.1111/jmwh.12018]
24. Lupattelli A, Picinardi M, Einarson A, Nordeng H. Health literacy and its association with perception of teratogenic risks and health behavior during pregnancy. Patient Educn Couns. 2014;96(2):171-8. [Link] [DOI:10.1016/j.pec.2014.04.014]
25. Harrington KF ZB, Magruder T, Bailey WC, Gerald LB. The impact of parent's health literacy on pediatric asthma outcomes. Pediatr Allergy Immunol Pulmonol. 2015;28(1):20-6. [Link] [DOI:10.1089/ped.2014.0379]
26. Santha AR. Maternal health literacy of ethnic Hungarian mothers in Romania. Kontakt. 2019;21:197-205. [Link] [DOI:10.32725/kont.2019.011]
27. Pirzadeh A, Nodooshan T, Nasirian M. Association between maternal health literacy level and prenatal care in Iran. J Health Lit. 2019;4(1):60-7. [Persian] [Link]
28. Masoumy M JZ, Hamedi S, Raisifar A, Zeratpisheh F, Ghaedi F. The relationship between maternal health literacy with Prenatal Cares in pregnant women referring to health centers. J Health Literacy. 2018;3(2):113-23. [Persian] [Link]
29. Tiller D HB, Kluttig A, Haertin J. Health literacy in an urban elderly East-German population - results from the population-based CARLA study. BMC Public Health. 2015;15:883. [Link] [DOI:10.1186/s12889-015-2210-7]
30. Lee JY. Maternal health literacy among low-income mothers with infants [dissertation]. Texas: The University of Texas at Austin; 2016. [Link]
31. Kirsch IS, Jungeblut A, Jenkins L, Kolstad A. Adult literacy in America: a first look at the results of the National Adult Literacy Survey. Washington: National Center for Education Statistics; 1993. [Link]
32. Janisse HC, Naar-King S, Ellis D. Parent's health literacy among high-risk adolescents with insulin dependent diabetes. J Pediatric Psychol. 2010;35(4):436-40. [Link] [DOI:10.1093/jpepsy/jsp077]
33. Yin HS, Johnson M, Mendelsohn AL, Abrams MA, Sanders LM, Dreyer BP. The health literacy of parents in the United States: A nationally representative study. Pediatrics. 2009; 124(suppl 3):S289-98. [Link] [DOI:10.1542/peds.2009-1162E]
34. Bennett IM, Robbins S, Haecker T. Screening for low literacy among adult caregivers of pediatric patients.Fam Med. 2003;35(8):585-90. [Link]
35. Borji M, Tarjoman A, Otaghi M, Salimi E, Naseri A. Health literacy level and its related factors among the elderlies in Ilam in 2015. Iran J Nurs. 2017;30(108):43-33. [Persian] [Link] [DOI:10.29252/ijn.30.108.33]
36. McKinn S, Linh DT, Foster K, McCaffery K. Distributed health literacy in the maternal health context in Vietnam. Health Literacy Res Pract. 2019;3(1):e31-42. [Link] [DOI:10.3928/24748307-20190102-01]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |