



Volume 9, Issue 2 (2021)
Health Educ Health Promot 2021, 9(2): 119-125 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghazanfari Z, Esmaeilikia M, Abedzade M, Gholami-Parizad E. A Randomized Controlled Trial of an Educational Intervention for Reducing the Dental Plaque Index of 3-6 Years Old Children. Health Educ Health Promot 2021; 9 (2) :119-125
URL: http://hehp.modares.ac.ir/article-5-47111-en.html
URL: http://hehp.modares.ac.ir/article-5-47111-en.html
1- Public Health Department, School of Health, Ilam University of Medical Sciences, Ilam, Iran , ghazanfari-z@medilam.ac.ir
2- Public Health Department, School of Health, Ilam University of Medical Sciences, Ilam, Iran
3- Clinical Microbiology Research Center, Ilam University of Medical Sciences, Ilam, Iran
2- Public Health Department, School of Health, Ilam University of Medical Sciences, Ilam, Iran
3- Clinical Microbiology Research Center, Ilam University of Medical Sciences, Ilam, Iran
Keywords: Preschool Children [MeSH], Oral Health [MeSH], Dental Plaque Index [MeSH], Health Belief Model [MeSH], Educational Early Intervention [MeSH]
Full-Text [PDF 497 kb]
(3398 Downloads)
| Abstract (HTML) (2250 Views)
Full-Text: (2082 Views)
Introduction
Dental caries in preschool children continues to be an important health problem in most countries worldwide, particularly in socially vulnerable populations, because of its early onset and high prevalence and the possibility of incurability [1, 2].
In 2010, untreated caries in permanent teeth was the most prevalent condition worldwide, affecting 2.4 billion people, and untreated caries in deciduous teeth was the 10th-most prevalent condition, affecting 621 million children worldwide. The global age-standardized prevalence and incidence of untreated caries remained static between 1990 and 2010. There is evidence that the burden of untreated caries is shifting from children to adults, with three peaks in prevalence at ages 6, 25, and 70 years [3].
According to the American Academy of Dentistry, premature childhood caries is the presence of one or more decayed surfaces in deciduous teeth lost due to caries or restoration in children. A meta-analysis was performed to investigate the prevalence of decay of deciduous and permanent teeth in Iranian children. Twenty-nine thousand two hundred twenty-five people in the age range of 1 to 15 years, including deciduous teeth; 6118 people in the age group of 1 to 7 years, and the permanent teeth; 23107 people in the age range of 8 to 15 years participated in this study. The overall prevalence of caries in Iranian children's deciduous and permanent teeth was 62.8% (62.8% (52.2-72.2) and 78.6% (73.0-83.2) alternatively [4].
Dental plaque has been considered as a direct cause of gingival and periodontal diseases. It is defined as soft deposits that form a biofilm adhering to the tooth surface in the oral cavity, including removable and fixed restorations. Good plaque control causes good gingival and periodontal health, prevents tooth decay, and preserves oral health for a lifetime [5]. In a study conducted in collaboration with Iran's Ministry of Health and the World Health Organization (WHO), the mean score of the DMFT index was found to be 4.5 in Iran, while it should be less than 1 in accordance with the WHO indexes [6, 7].
Plaque control can be achieved by either mechanical or chemical means. However, mechanical plaque control remains the mainstay to prevent dental diseases, with chemical agents acting as adjuncts [5]. The mechanical methods of plaque removal are tooth brushing, flossing, and interdental cleansing devices, while the various chemical methods include the use of antimicrobial mouthwashes, gel, and dentifrices. Tooth brushing is an effective means of removing plaque, thereby preventing gingivitis and, to some extent, controlling dental caries [8]. The high prevalence and severity of dental diseases indicate that tooth brushing, as a basis of prevention, is inadequately performed [5], and this problem is mostly due to cultural and behavioral habits [9]. Therefore, establishing good behaviors and beliefs is warranted to prevent dental caries.
Parents of preschool children have a crucial role in developing a healthy lifestyle and healthy oral habits. Having poor knowledge and attitude towards children's oral health leads to poor oral health practices of their children. Hence, to improve children's oral health, appropriate interventions should be provided among their parents—especially their mothers—as the main caregiver. This determines children's current oral health status and lays the backbone of beliefs and the type of behavior that he/she adopts at this age and continues until adulthood [10-12]. Thus, to plan a health education program to change people's behavior, we should address their underlying beliefs. In these situations, the health belief model (HBM) might be more relevant [9].
The HBM provides a special framework to plan interventions for behavior change [9]. The HBM assumes that people are more likely to engage in oral health behaviors (e.g., brushing and flossing) if they perceive themselves to be susceptible to oral diseases (perceived susceptibility), consider oral diseases to have potentially serious consequences (perceived severity), believe that oral health behaviors will produce positive outcomes (perceived benefits), think that barriers to performing oral health behaviors are less than the benefits (perceived barriers), perceive themselves to be capable of attaining designated types of performance and achieving specific results (self-efficacy), and receive cues to action such as recommendations from health educators, advice from family members and friends, and encouragement from teachers [13, 14].
A few studies have evaluated oral health-related instructional interventions. For example, Chi piloted a bilingual flipchart with Korean-American caregivers of preschoolers and administered pre-/post-intervention surveys. There were significant improvements in knowledge on the bacterial etiology of tooth decay, mother-to-child transmission of tooth decay, fluoride toothpaste safety, and dental visit frequency. Caregivers' self-efficacy to keep their child's teeth healthy also improved [15].
Solhi et al. carried out a quasi-experimental study on twelve-year-old girl students in the central district of Tehran, Iran. Educational planning based on the descriptive results and HBM was applied. Data gathered about quality of brushing, dental flossing, health files, and clinical observation. After education, based on HBM, all the oral health perceptions increased, and correct brushing and flossing were influenced by increased perceptions. Generally, she could show that using HBM in oral health education to increase the likelihood of taking preventive oral health behaviors is applicable [16].
Shahnazi et al. implemented a quasi-experimental study in women in the first trimester of pregnancy who attended private clinics in Delfan city, Iran. After achieving data on demographic characteristics, a DMFT checklist, and some HBM constructs before intervention, an educational intervention consisting of 4 training sessions for the intervention group were scheduled. Methods of lecture, focus-group discussion, video, and role-playing were used as the main educational strategies. Follow-up was done four months after the intervention. Results showed that education on some of the HBM constructs resulted in increased knowledge of oral health, perceived susceptibility, and self-efficacy of pregnant women [17].
Given the lack of studies for children less than six years and the importance of the early years of life in the formation of oral health, this study was designed to evaluate the effect of a health education intervention provided to mothers on decreasing the plaque index (PI) of children less than six years.
Materials and Methods
This experimental study was conducted on 140 mothers and their 3–6-year-old children (NTotal=280) referred to the Health Care Center No. 1 in Ilam (a referral Center to assess children's oral health) in 2015. Participants were randomly selected using a random number and randomly assigned to either intervention or control groups on a 1:1 ratio basis. To detect a 1.5-point increase in the first score of perceived susceptibility at 5% significance, the study would require a sample of 100 participants include 50 mothers and 50 their children per group, anticipating 15% dropout. Participants were considered eligible if they were able to speak in Persian (the formal language in Iran), consented to participate in the study, receiving neither educational nor therapeutic interventions, having no history of disease in the mothers or the children (due to their effect on dental health, such as epilepsy, cancer, diabetes, use of anticholinergic drugs) according to their health care records. The exclusion criteria included the absence of training sessions and their unavailability to complete the questionnaires and dental examinations.
To assess the outcome of the intervention, a three-part questionnaire was used. The first part included items on demographic variables. This part had ten items related to demographic questions about the children's age, sex, birth order, education, and employment of their parents' and families' socioeconomic status. The second part is related to the constructs of the HBM. All Items of the questionnaire were classified using the 5-point Likert scale with the range of strongly disagree to agree strongly (score ranges from 1 to 5). The higher score on all scales indicated a better situation except for perceived barriers which the lower score indicated a better situation on the scale. Sample items on HBM constructs and possible score range for constructs were presented in table 1. The third part addressed 3 questions related to the children's oral health, including visiting a dentist at least once a year, brushing the babies' teeth by mother at least once a day, and rinsing the mouth after eating and drinking sugary drinks/foods. Each behavior received a score of 1 if it was acceptable; otherwise, 0 was considered. The sum of scores for behavior was equal to 3. The time taken to complete the questionnaire in this study was about 10 to 15 minutes. The content validity was evaluated through content validity assessment by panel experts, and essential modifications were made based on the comments of health education specialists and dentists. Also, face validity was evaluated based on the participants' comments, and essential modifications were made to facilitate simplicity, fluency, and understanding of questions and response options. Reliability was also tested via Cronbach's alpha. The results are presented in Table 1.
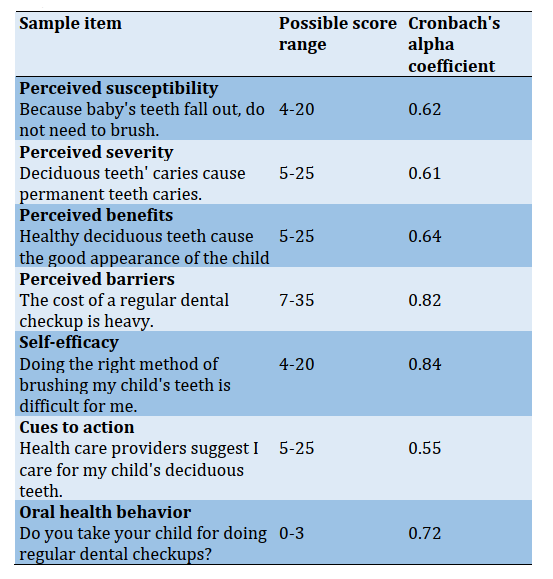
Table 1) Constructs and sample items
Approval for this research was acquired through the Ilam University of Medical Sciences Ethics Committee. The objectives of the study were outlined, and written informed consent was obtained from mothers. Confidentiality of information was ensured, and the participants were given the authority to withdraw from the study if they encountered several difficulties that might have hindered their participation. Randomization was achieved using sealed, opaque numbered envelopes. A research assistant who was not involved in the recruitment of participants prepared the envelopes. Women allocated to the control group (n=50) received a standard "well baby program". Women assigned to the intervention group (n=50) also received a standard "well baby program" plus the educational intervention. All mothers completed a follow-up questionnaire at the one-month follow-up. The control group received standard care "well baby program". This includes the Expanded Program on Immunization (EPI) and child growth and development. Three training sessions were given to the intervention group —each lasted for one hour (once a week)— the content of the educational intervention was derived from materials from the Iran’s Ministry of Health. Also, a panel of experts, including dentists and health education, approved the contents. The importance and necessity of oral health in children and prevention of related diseases was explained in the first session to affect mothers' perceived susceptibility and severity to dental caries in childhood through lecture and discussion methods. The second session concentrated on increasing perceived benefits, self-efficacy, and decreasing perceived barriers held by discussion and an educational video. Using a focus group discussion, participants were invited to share their viewpoints on brushing teeth conducive to preventing dental caries. This session emphasized the perceived benefits of brushing teeth. They were explained how following a regular schedule for brushing teeth could help to reduce PI. Healthy behaviors related to oral health such as regular brushing teeth and visiting a dentist were explained, and ways to engage them were suggested. To address barrier construct, brainstorming was conducted where participants were asked about barriers or difficulties they might face when attempting to engage in preventive behaviors of dental caries. Potential solutions were also discussed as ways of overcoming the barriers. The most practical methods of overcoming barriers were then ranked by participants, and participants were encouraged to use these solutions. In addition, several successful people who had overcome barriers to a regular plan of brushing shared their achievements with others. To enhance self-efficacy, two role models who were excellent in brushing their children and had positive attitudes toward this presented lectures to the group on personal oral health planning for their children and then answered the mother's questions. In addition, there was a discussion of how to break down health behaviors into small activities to be more easily engaged in. At the end of the intervention, a gift including a toothbrush and toothpaste and a booklet and brush chart were given to the participants in the group to record the brushing of their children during a month. Two weeks after the health education program, mothers in the intervention group received a phone call consultation. They were asked for any barriers they encountered and counseled to remove barriers. At one-month follow-up, the post-test questionnaires were administered to both groups. Also, dental examinations were done by the dentist. A trained dentist assessed the oral health status of children using O'Leary PI with a dental mirror and a probe in broad daylight. This index evaluated bacterial plaque on the four dental surfaces (mesial, buccal, distal, and lingual) by adding the total surfaces with the plaque and dividing this by the total number of dental surfaces examined, multiplying it by one-hundred [18]. Plaque-disclosing tablets were dissolved in water and applied to the children's teeth using cotton rolls or chewed by the children that caused the plaque on their teeth to be stained. They rinsed their mouths after 10 minutes, and any plaque on different surfaces of the tooth was reported. This process lasted 15 minutes for each child. To calibrate the dental examinations by a dentist, ten children who were not involved in the study were examined by two independent dentists. Each dentist recorded their examination on a checklist independently. Then the agreement between the examinations was calculated using the Kappa coefficient, which was adequate (κ= 0.8).
SPSS 26 (SPSS Inc., USA) was used for data analysis. The chi-square test was applied to compare the demographic data of the intervention and control groups before intervention. The paired t-test was employed to compare the pre-test and post-test scores of perceived susceptibility, severity, benefits, barriers, self-efficacy, and behavior and PI in both groups after ensuring normalization of data using the Kolmogorov-Smirnov test. The paired t-test was also used to compare the groups before and after the education. Mean score changes between the two groups were compared using an independent t-test.
Findings
Of the 140 women who were approached, 88 people participated (Diagram 1).
Follow-up rates at one month were high, with 45 (90%) women in the intervention group and 43 (86%) women in the control group. The demographic characteristics of participants of both groups were presented in Table 1. The mean±SD ages of mothers and their children were 31.28±5.63 years and 4.5±1.56 years, respectively, and the mean age at recruitment was 35.89±1.75 weeks. No significant differences were found between the intervention and control groups regarding demographic variables (Table 2).
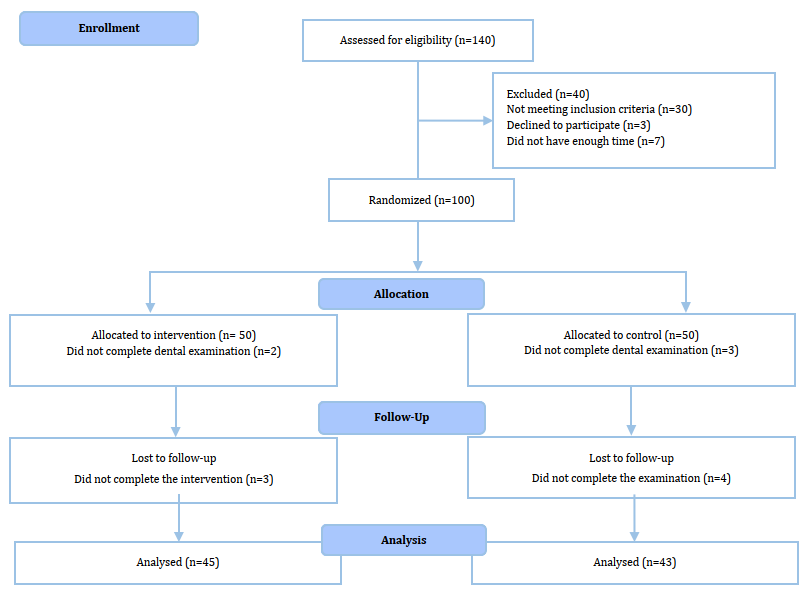
Diagram 1) Flowchart of the study participants
Table 2) Comparison of the frequency (numbers in parentheses are percent) of demographic characteristics of the study participants between two groups (N=176)
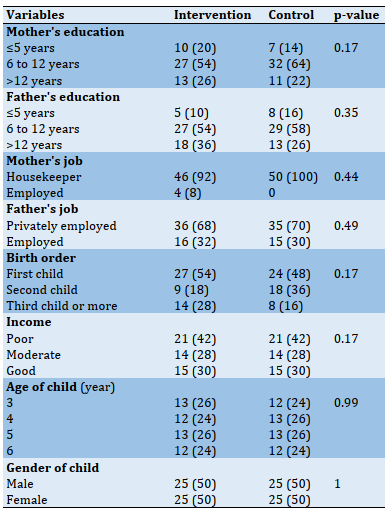
Table 3) Mean±SD of health belief model's variables, oral health practice, and plaque index (N=88)
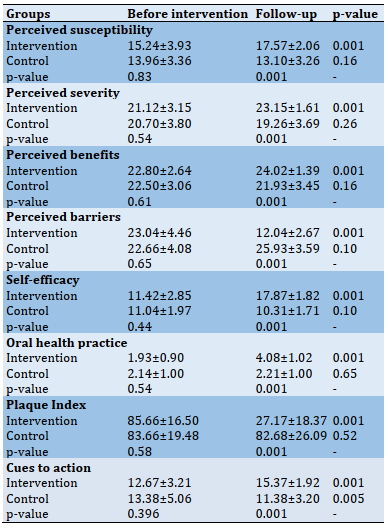
Despite the homogeneity of groups before the intervention in terms of outcome variables (p>0.05), significant differences were found between groups in all HBM variables, oral health practice, and the PI at the end of the study (p≤0.001). Significant differences were found in the intervention group in all HBM variables, oral health practice, and the PI between two times, before and after the intervention (p≤0.001; Table 3).
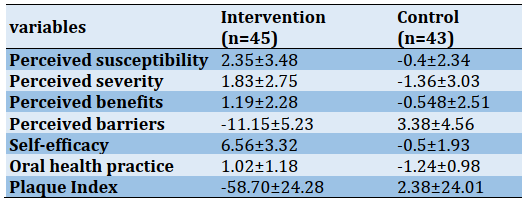
Score changes from before intervention to follow-up were showed in Table 4.
Table 4) Comparison of mean score changes between two groups (p<0.001)
Discussion
This study was carried out to promote oral health behaviors and decrease dental PI in children aged 3–6. The intervention improved maternal behavioral beliefs regarding oral health for children, oral health practice, and PI. Other studies have also demonstrated the effective role of mothers as caregivers of the children's oral health in early childhood [19, 20]. Many studies have shown the effective role of the HBM in behavior change, such as Shamsi et al. [21], Solhi et al. [16], and Tan et al. [22], but there is some ineffective study to create the change that may be a result of short-time-follow up after the intervention [21].
The mean score of barriers of oral health practice decreased in mothers after the intervention compared to the control group. Barriers such as forgetfulness, everyday concerns, and life conditions despite good knowledge of parents towards regular visits similar to previous studies [22-24] might be reduced applying educational interventions. Expensive dental care was also mentioned as a barrier by the participants. It seems that reducing healthcare costs should be placed on the agenda of policymakers.
Dental caries in preschool children continues to be an important health problem in most countries worldwide, particularly in socially vulnerable populations, because of its early onset and high prevalence and the possibility of incurability [1, 2].
In 2010, untreated caries in permanent teeth was the most prevalent condition worldwide, affecting 2.4 billion people, and untreated caries in deciduous teeth was the 10th-most prevalent condition, affecting 621 million children worldwide. The global age-standardized prevalence and incidence of untreated caries remained static between 1990 and 2010. There is evidence that the burden of untreated caries is shifting from children to adults, with three peaks in prevalence at ages 6, 25, and 70 years [3].
According to the American Academy of Dentistry, premature childhood caries is the presence of one or more decayed surfaces in deciduous teeth lost due to caries or restoration in children. A meta-analysis was performed to investigate the prevalence of decay of deciduous and permanent teeth in Iranian children. Twenty-nine thousand two hundred twenty-five people in the age range of 1 to 15 years, including deciduous teeth; 6118 people in the age group of 1 to 7 years, and the permanent teeth; 23107 people in the age range of 8 to 15 years participated in this study. The overall prevalence of caries in Iranian children's deciduous and permanent teeth was 62.8% (62.8% (52.2-72.2) and 78.6% (73.0-83.2) alternatively [4].
Dental plaque has been considered as a direct cause of gingival and periodontal diseases. It is defined as soft deposits that form a biofilm adhering to the tooth surface in the oral cavity, including removable and fixed restorations. Good plaque control causes good gingival and periodontal health, prevents tooth decay, and preserves oral health for a lifetime [5]. In a study conducted in collaboration with Iran's Ministry of Health and the World Health Organization (WHO), the mean score of the DMFT index was found to be 4.5 in Iran, while it should be less than 1 in accordance with the WHO indexes [6, 7].
Plaque control can be achieved by either mechanical or chemical means. However, mechanical plaque control remains the mainstay to prevent dental diseases, with chemical agents acting as adjuncts [5]. The mechanical methods of plaque removal are tooth brushing, flossing, and interdental cleansing devices, while the various chemical methods include the use of antimicrobial mouthwashes, gel, and dentifrices. Tooth brushing is an effective means of removing plaque, thereby preventing gingivitis and, to some extent, controlling dental caries [8]. The high prevalence and severity of dental diseases indicate that tooth brushing, as a basis of prevention, is inadequately performed [5], and this problem is mostly due to cultural and behavioral habits [9]. Therefore, establishing good behaviors and beliefs is warranted to prevent dental caries.
Parents of preschool children have a crucial role in developing a healthy lifestyle and healthy oral habits. Having poor knowledge and attitude towards children's oral health leads to poor oral health practices of their children. Hence, to improve children's oral health, appropriate interventions should be provided among their parents—especially their mothers—as the main caregiver. This determines children's current oral health status and lays the backbone of beliefs and the type of behavior that he/she adopts at this age and continues until adulthood [10-12]. Thus, to plan a health education program to change people's behavior, we should address their underlying beliefs. In these situations, the health belief model (HBM) might be more relevant [9].
The HBM provides a special framework to plan interventions for behavior change [9]. The HBM assumes that people are more likely to engage in oral health behaviors (e.g., brushing and flossing) if they perceive themselves to be susceptible to oral diseases (perceived susceptibility), consider oral diseases to have potentially serious consequences (perceived severity), believe that oral health behaviors will produce positive outcomes (perceived benefits), think that barriers to performing oral health behaviors are less than the benefits (perceived barriers), perceive themselves to be capable of attaining designated types of performance and achieving specific results (self-efficacy), and receive cues to action such as recommendations from health educators, advice from family members and friends, and encouragement from teachers [13, 14].
A few studies have evaluated oral health-related instructional interventions. For example, Chi piloted a bilingual flipchart with Korean-American caregivers of preschoolers and administered pre-/post-intervention surveys. There were significant improvements in knowledge on the bacterial etiology of tooth decay, mother-to-child transmission of tooth decay, fluoride toothpaste safety, and dental visit frequency. Caregivers' self-efficacy to keep their child's teeth healthy also improved [15].
Solhi et al. carried out a quasi-experimental study on twelve-year-old girl students in the central district of Tehran, Iran. Educational planning based on the descriptive results and HBM was applied. Data gathered about quality of brushing, dental flossing, health files, and clinical observation. After education, based on HBM, all the oral health perceptions increased, and correct brushing and flossing were influenced by increased perceptions. Generally, she could show that using HBM in oral health education to increase the likelihood of taking preventive oral health behaviors is applicable [16].
Shahnazi et al. implemented a quasi-experimental study in women in the first trimester of pregnancy who attended private clinics in Delfan city, Iran. After achieving data on demographic characteristics, a DMFT checklist, and some HBM constructs before intervention, an educational intervention consisting of 4 training sessions for the intervention group were scheduled. Methods of lecture, focus-group discussion, video, and role-playing were used as the main educational strategies. Follow-up was done four months after the intervention. Results showed that education on some of the HBM constructs resulted in increased knowledge of oral health, perceived susceptibility, and self-efficacy of pregnant women [17].
Given the lack of studies for children less than six years and the importance of the early years of life in the formation of oral health, this study was designed to evaluate the effect of a health education intervention provided to mothers on decreasing the plaque index (PI) of children less than six years.
Materials and Methods
This experimental study was conducted on 140 mothers and their 3–6-year-old children (NTotal=280) referred to the Health Care Center No. 1 in Ilam (a referral Center to assess children's oral health) in 2015. Participants were randomly selected using a random number and randomly assigned to either intervention or control groups on a 1:1 ratio basis. To detect a 1.5-point increase in the first score of perceived susceptibility at 5% significance, the study would require a sample of 100 participants include 50 mothers and 50 their children per group, anticipating 15% dropout. Participants were considered eligible if they were able to speak in Persian (the formal language in Iran), consented to participate in the study, receiving neither educational nor therapeutic interventions, having no history of disease in the mothers or the children (due to their effect on dental health, such as epilepsy, cancer, diabetes, use of anticholinergic drugs) according to their health care records. The exclusion criteria included the absence of training sessions and their unavailability to complete the questionnaires and dental examinations.
To assess the outcome of the intervention, a three-part questionnaire was used. The first part included items on demographic variables. This part had ten items related to demographic questions about the children's age, sex, birth order, education, and employment of their parents' and families' socioeconomic status. The second part is related to the constructs of the HBM. All Items of the questionnaire were classified using the 5-point Likert scale with the range of strongly disagree to agree strongly (score ranges from 1 to 5). The higher score on all scales indicated a better situation except for perceived barriers which the lower score indicated a better situation on the scale. Sample items on HBM constructs and possible score range for constructs were presented in table 1. The third part addressed 3 questions related to the children's oral health, including visiting a dentist at least once a year, brushing the babies' teeth by mother at least once a day, and rinsing the mouth after eating and drinking sugary drinks/foods. Each behavior received a score of 1 if it was acceptable; otherwise, 0 was considered. The sum of scores for behavior was equal to 3. The time taken to complete the questionnaire in this study was about 10 to 15 minutes. The content validity was evaluated through content validity assessment by panel experts, and essential modifications were made based on the comments of health education specialists and dentists. Also, face validity was evaluated based on the participants' comments, and essential modifications were made to facilitate simplicity, fluency, and understanding of questions and response options. Reliability was also tested via Cronbach's alpha. The results are presented in Table 1.
Table 1) Constructs and sample items
Approval for this research was acquired through the Ilam University of Medical Sciences Ethics Committee. The objectives of the study were outlined, and written informed consent was obtained from mothers. Confidentiality of information was ensured, and the participants were given the authority to withdraw from the study if they encountered several difficulties that might have hindered their participation. Randomization was achieved using sealed, opaque numbered envelopes. A research assistant who was not involved in the recruitment of participants prepared the envelopes. Women allocated to the control group (n=50) received a standard "well baby program". Women assigned to the intervention group (n=50) also received a standard "well baby program" plus the educational intervention. All mothers completed a follow-up questionnaire at the one-month follow-up. The control group received standard care "well baby program". This includes the Expanded Program on Immunization (EPI) and child growth and development. Three training sessions were given to the intervention group —each lasted for one hour (once a week)— the content of the educational intervention was derived from materials from the Iran’s Ministry of Health. Also, a panel of experts, including dentists and health education, approved the contents. The importance and necessity of oral health in children and prevention of related diseases was explained in the first session to affect mothers' perceived susceptibility and severity to dental caries in childhood through lecture and discussion methods. The second session concentrated on increasing perceived benefits, self-efficacy, and decreasing perceived barriers held by discussion and an educational video. Using a focus group discussion, participants were invited to share their viewpoints on brushing teeth conducive to preventing dental caries. This session emphasized the perceived benefits of brushing teeth. They were explained how following a regular schedule for brushing teeth could help to reduce PI. Healthy behaviors related to oral health such as regular brushing teeth and visiting a dentist were explained, and ways to engage them were suggested. To address barrier construct, brainstorming was conducted where participants were asked about barriers or difficulties they might face when attempting to engage in preventive behaviors of dental caries. Potential solutions were also discussed as ways of overcoming the barriers. The most practical methods of overcoming barriers were then ranked by participants, and participants were encouraged to use these solutions. In addition, several successful people who had overcome barriers to a regular plan of brushing shared their achievements with others. To enhance self-efficacy, two role models who were excellent in brushing their children and had positive attitudes toward this presented lectures to the group on personal oral health planning for their children and then answered the mother's questions. In addition, there was a discussion of how to break down health behaviors into small activities to be more easily engaged in. At the end of the intervention, a gift including a toothbrush and toothpaste and a booklet and brush chart were given to the participants in the group to record the brushing of their children during a month. Two weeks after the health education program, mothers in the intervention group received a phone call consultation. They were asked for any barriers they encountered and counseled to remove barriers. At one-month follow-up, the post-test questionnaires were administered to both groups. Also, dental examinations were done by the dentist. A trained dentist assessed the oral health status of children using O'Leary PI with a dental mirror and a probe in broad daylight. This index evaluated bacterial plaque on the four dental surfaces (mesial, buccal, distal, and lingual) by adding the total surfaces with the plaque and dividing this by the total number of dental surfaces examined, multiplying it by one-hundred [18]. Plaque-disclosing tablets were dissolved in water and applied to the children's teeth using cotton rolls or chewed by the children that caused the plaque on their teeth to be stained. They rinsed their mouths after 10 minutes, and any plaque on different surfaces of the tooth was reported. This process lasted 15 minutes for each child. To calibrate the dental examinations by a dentist, ten children who were not involved in the study were examined by two independent dentists. Each dentist recorded their examination on a checklist independently. Then the agreement between the examinations was calculated using the Kappa coefficient, which was adequate (κ= 0.8).
SPSS 26 (SPSS Inc., USA) was used for data analysis. The chi-square test was applied to compare the demographic data of the intervention and control groups before intervention. The paired t-test was employed to compare the pre-test and post-test scores of perceived susceptibility, severity, benefits, barriers, self-efficacy, and behavior and PI in both groups after ensuring normalization of data using the Kolmogorov-Smirnov test. The paired t-test was also used to compare the groups before and after the education. Mean score changes between the two groups were compared using an independent t-test.
Findings
Of the 140 women who were approached, 88 people participated (Diagram 1).
Follow-up rates at one month were high, with 45 (90%) women in the intervention group and 43 (86%) women in the control group. The demographic characteristics of participants of both groups were presented in Table 1. The mean±SD ages of mothers and their children were 31.28±5.63 years and 4.5±1.56 years, respectively, and the mean age at recruitment was 35.89±1.75 weeks. No significant differences were found between the intervention and control groups regarding demographic variables (Table 2).
Diagram 1) Flowchart of the study participants
Table 2) Comparison of the frequency (numbers in parentheses are percent) of demographic characteristics of the study participants between two groups (N=176)
Table 3) Mean±SD of health belief model's variables, oral health practice, and plaque index (N=88)
Despite the homogeneity of groups before the intervention in terms of outcome variables (p>0.05), significant differences were found between groups in all HBM variables, oral health practice, and the PI at the end of the study (p≤0.001). Significant differences were found in the intervention group in all HBM variables, oral health practice, and the PI between two times, before and after the intervention (p≤0.001; Table 3).
Score changes from before intervention to follow-up were showed in Table 4.
Table 4) Comparison of mean score changes between two groups (p<0.001)
Discussion
This study was carried out to promote oral health behaviors and decrease dental PI in children aged 3–6. The intervention improved maternal behavioral beliefs regarding oral health for children, oral health practice, and PI. Other studies have also demonstrated the effective role of mothers as caregivers of the children's oral health in early childhood [19, 20]. Many studies have shown the effective role of the HBM in behavior change, such as Shamsi et al. [21], Solhi et al. [16], and Tan et al. [22], but there is some ineffective study to create the change that may be a result of short-time-follow up after the intervention [21].
The mean score of barriers of oral health practice decreased in mothers after the intervention compared to the control group. Barriers such as forgetfulness, everyday concerns, and life conditions despite good knowledge of parents towards regular visits similar to previous studies [22-24] might be reduced applying educational interventions. Expensive dental care was also mentioned as a barrier by the participants. It seems that reducing healthcare costs should be placed on the agenda of policymakers.
Self-efficacy and perceived benefits were significantly improved in this study, consistent with previous studies on the topic [25]. This study also highlighted the improved behavior of mothers regarding their children's oral health. Given the abovementioned results, the healthcare system should be reorganized so that healthcare providers play an active role in instructing their consumers regarding oral health. It should be noted that this cost-effective measure has a considerable effect and should be considered by planners and policymakers of the health system.
This study gained a 58% decrease in PI O'Leary for the intervention group versus a 1% decrease for the control group. This result is in accordance with Pouradeli et al. [26], but it was a better result than Pouradeli et al. (i.e., 18.7% decrease in the video training group versus 24.7% decrease in the dental model). One possible difference might be that while the study recruited normal children, Pouradeli's study was conducted among hearing impaired children with impaired hearing, which might have more difficulties in education than normal children.
Also, the obtained result for the oral health behavior in this study is consistent with the study by Basir et al., which is done in early childhood in Ahvaz. Similarly, the oral health behaviors in Basir et al. included three items, examination by a dentist, clean the child's teeth after eating sweet things, and daily brushing. They could successfully promote children's oral health behavior following the educational intervention, including lecture and group discussion [27].
This study could significantly enhance young children's oral health and decreased PI. These results are consistent with other studies [28-30]. The PI, as an objective measure of behavior change, confirmed the efficacy of the instructional plan in this study with three educational sessions and a phone call. Hence, developing instructional plans based on the HBM can promote children's oral health behavior and decrease dental caries by providing brief instruction to their mothers. The strength of this study is the use of a clinical indicator called dental PI along with oral health behavior. This index can confirm the effectiveness of education by the framework of HBM and, finally, the change of behavior.
Since the study enrolled only children from a health care center and not involved participants from the private sector, the study results are not generalizable to all children.
Conclusion
Addressing the mothers' cognition and affections could improve their beliefs and behavior regarding children's tooth brushing and finally keep their teeth healthy.
Acknowledgments: We express our gratitude to the Deputy of Research at Ilam University of Medical Sciences and those who helped us conduct this study. We are grateful to the participants who participated in the study.
Ethical Permissions: Approval for this research was acquired through the Ilam University of Medical Sciences Ethics Committee (Code: IR.Medilam.REC.1394.72).
Conflicts of Interests: This article is a part of the result of an MSc thesis approved by the Ilam University of Medical Sciences. The authors declare that they have no competing interests.
Authors' Contribution: Ghazanfari Z. (First author), Methodologist (55%); Esmaeilikia M. (Second author), Original researcher (25%); Abedzade M.S. (Third author), Assistant (10%); Gholami-Parizad E. (Forth author), Assistant (10%).
Funding/Sources: No grant was received for this study.
This study gained a 58% decrease in PI O'Leary for the intervention group versus a 1% decrease for the control group. This result is in accordance with Pouradeli et al. [26], but it was a better result than Pouradeli et al. (i.e., 18.7% decrease in the video training group versus 24.7% decrease in the dental model). One possible difference might be that while the study recruited normal children, Pouradeli's study was conducted among hearing impaired children with impaired hearing, which might have more difficulties in education than normal children.
Also, the obtained result for the oral health behavior in this study is consistent with the study by Basir et al., which is done in early childhood in Ahvaz. Similarly, the oral health behaviors in Basir et al. included three items, examination by a dentist, clean the child's teeth after eating sweet things, and daily brushing. They could successfully promote children's oral health behavior following the educational intervention, including lecture and group discussion [27].
This study could significantly enhance young children's oral health and decreased PI. These results are consistent with other studies [28-30]. The PI, as an objective measure of behavior change, confirmed the efficacy of the instructional plan in this study with three educational sessions and a phone call. Hence, developing instructional plans based on the HBM can promote children's oral health behavior and decrease dental caries by providing brief instruction to their mothers. The strength of this study is the use of a clinical indicator called dental PI along with oral health behavior. This index can confirm the effectiveness of education by the framework of HBM and, finally, the change of behavior.
Since the study enrolled only children from a health care center and not involved participants from the private sector, the study results are not generalizable to all children.
Conclusion
Addressing the mothers' cognition and affections could improve their beliefs and behavior regarding children's tooth brushing and finally keep their teeth healthy.
Acknowledgments: We express our gratitude to the Deputy of Research at Ilam University of Medical Sciences and those who helped us conduct this study. We are grateful to the participants who participated in the study.
Ethical Permissions: Approval for this research was acquired through the Ilam University of Medical Sciences Ethics Committee (Code: IR.Medilam.REC.1394.72).
Conflicts of Interests: This article is a part of the result of an MSc thesis approved by the Ilam University of Medical Sciences. The authors declare that they have no competing interests.
Authors' Contribution: Ghazanfari Z. (First author), Methodologist (55%); Esmaeilikia M. (Second author), Original researcher (25%); Abedzade M.S. (Third author), Assistant (10%); Gholami-Parizad E. (Forth author), Assistant (10%).
Funding/Sources: No grant was received for this study.
Article Type: Original Research |
Subject:
Health Education and Health Behavior
Received: 2020/10/28 | Accepted: 2021/03/7 | Published: 2021/06/20
Received: 2020/10/28 | Accepted: 2021/03/7 | Published: 2021/06/20
References
1. Chi DL, Masterson EE, Carle AC, Mancl LA, Coldwell SE. Socioeconomic status, food security, and dental caries in US children: Mediation analyses of data from the national health and nutrition examination survey, 2007-2008. Am J Public Health. 2014;104(5):860-4. [Link] [DOI:10.2105/AJPH.2013.301699] [PMID] [PMCID]
2. Bulut G, Bulut H. Zero to five years: First dental visit. Eur J Paediatr Dent. 2020;21(4):326-30. [Link]
3. Kassebaum NJ, Bernabe E, Dahiya M, Bhandari B, Murray CJL, Marcenes W. Global burden of untreated caries: A systematic review and metaregression. J Dent Res. 2015;94(5):650-8. [Link] [DOI:10.1177/0022034515573272] [PMID]
4. Vaisi Raygani AA, Jalali R, Ghobadi A, Salari N. The prevalence of dental caries in deciduous and permanent teeth in Iranian children: A systematic review and meta-analysis. J Res Dent Sci. 2018;15(3):180-9. [Persian] [Link] [DOI:10.29252/jrds.15.3.10]
5. Kallar S, Pandit IK, Srivastava N, Gugnani N. Plaque removal efficacy of powered and manual toothbrushes under supervised and unsupervised conditions: A comparative clinical study. J Indian Soc Pedod Prev Dent. 2011;29(3):235-8. [Link] [DOI:10.4103/0970-4388.85832] [PMID]
6. Naderifar M, Peyrovi H, Galgay F. Mothers attitude towards orodental health of their 1-6 years old children referred to medical centers of Zahedan city, 2006. Iran J Nurs. 2007;20(52):75-86. [Persian] [Link]
7. Karami A, Heidarnia A, Zarei F. Comparison of peer led and teacher led oral health educational program among students. Braz J Oral Sci. 2019;18:e191626. [Link] [DOI:10.20396/bjos.v18i0.8657260]
8. Okada M, Kuwahara S, Kaihara Y, Ishidori H, Kawamura M, Miura K, et al. Relationship between gingival health and dental caries in children aged 7-12 years. J Oral Sci. 2000;42(3):151-5. [Link] [DOI:10.2334/josnusd.42.151] [PMID]
9. Kasmaei P, Shokravi FA, Hidarnia A, Hajizadeh E, Atrkar-Roushan Z, Karimzadeh Shirazi K, et al. Brushing behavior among young adolescents: Does perceived severity matter. BMC Public Health. 2014;14:8. [Link] [DOI:10.1186/1471-2458-14-8] [PMID] [PMCID]
10. Sehrawat P, Shivlingesh KK, Gupta B, Anand R, Sharma A, Chaudhry M. Oral health knowledge, awareness and associated practices of preschool children's mothers in Greater Noida, India. Niger Postgrad Med J. 2016;23(3):152-7. [Link] [DOI:10.4103/1117-1936.190344] [PMID]
11. Dye BA, Vargas CM, Lee JJ, Magder L, Tinanoff N. Assessing the relationship between children's oral health status and that of their mothers. J Am Dent Assoc. 2011;142(2):173-83. [Link] [DOI:10.14219/jada.archive.2011.0061] [PMID]
12. Okada M, Kawamura M, Kaihara Y, Matsuzaki Y, Kuwahara S, Ishidori H, et al. Influence of parents' oral health behavior on oral health status of their school children: An exploratory study employing a causal modelling technique. J Paediatr Dent. 2002;12(2):101-8. [Link] [DOI:10.1046/j.1365-263X.2002.00338.x] [PMID]
13. Yekaninejad MS, Eshraghian MR, Nourijelyani K, Mohammad K, Foroushani AR, Zayeri F, et al. effect of a school‐based oral health‐education program on Iranian children: Results from a group randomized trial. Eur J Oral Sci. 2012;120(5):429-37. [Link] [DOI:10.1111/j.1600-0722.2012.00993.x] [PMID]
14. Hollister MC, Anema MG. Health behavior models and oral health: A review. J Dent Hyg. 2004;78(3):6. [Link]
15. Chi DL, Ko A, Kim JY. Bilingual flipcharts help improve oral health‐related knowledge and self‐efficacy of Korean‐American caregivers of preschoolers. J Public Health Dent. 2014;74(4):261-5. [Link] [DOI:10.1111/jphd.12073] [PMID] [PMCID]
16. Solhi M, Shojaei Zadeh D, Seraj B, Faghih Zadeh S. The application of the health belief model in oral health education. Iran J Public Health. 2010;39(4):114-9. [Link]
17. Shahnazi H, Hosseintalaei M, Esteki Ghashghaei F, Charkazi A, Yahyavi Y, Sharifirad G. Effect of educational intervention on perceived susceptibility self-efficacy and DMFT of pregnant women. Iran Red Crescent Med J. 2016;18(5):24960. [Link] [DOI:10.5812/ircmj.24960] [PMID] [PMCID]
18. Newman MG, Takei H, Carranza FA. Carranza's clinical periodontology. Philadelphia: W.B. Saunders Co; 2002. [Link]
19. Makvandi Z, Karimi-Shahanjarini A, Faradmal J, Bashirian S. Evaluation of an oral health intervention among mothers of young children: A clustered randomized trial. J Res Health Sci. 2015;15(2):88-93. [Link]
20. Azevedo MS, Romano AR, Correa MB, Dos Santos IDS, Cenci MS. Evaluation of a feasible educational intervention in preventing early childhood caries. Braz Oral Res. 2015;29(1):1-8. [Link] [DOI:10.1590/1807-3107BOR-2015.vol29.0089] [PMID]
21. Shamsi M, Hidarnia A, Niknami S, Rafiee M, Zareban I, Karimy M. The effect of educational program on increasing oral health behavior among pregnant women: Applying health belief model. Health Educ Health Promot. 2013;1(2):21-36. [Persian] [Link]
22. Tan BS, Ng KH, Esa R. Health beliefs in oral cancer: Malaysian estate Indian scenario. Patient Educ Couns. 2001;42(3):205-11. [Link] [DOI:10.1016/S0738-3991(00)00121-X]
23. Hallberg U, Camling E, Zickert I, Robertson A, Berggren U. Dental appointment no‐shows: Why do some parents fail to take their children to the dentist. Int J Paediatr Dent. 2008;18(1):27-34. [Link]
24. Zhu L, Petersen PE, Wang HY, Bian JY, Zhang BX. Oral health knowledge, attitudes and behavior of children and adolescents in China. Int Dent J. 2003;53(5):289-98. [Link] [DOI:10.1111/j.1875-595X.2003.tb00762.x] [PMID]
25. Buglar ME, White KM, Robinson NG. The role of self-efficacy in dental patients' brushing and flossing: Testing an extended health belief model. Patient Educ Couns. 2010;78(2):269-72. [Link] [DOI:10.1016/j.pec.2009.06.014] [PMID]
26. Pouradeli S, Hashemipour MA, Zolala F, Baneshi MR, Ahmadi-Tabatabaei SV, Habib-Agahi R. Short term effect of two education methods on oral health among hearing impairment children. J Oral Health Oral Epidemiol. 2016;5(4):221-7. [Persian] [Link]
27. Basir L, Rasteh B, Motazeri A, Araban M. Four-level evaluation of health promotion intervention for preventing early childhood caries: A randomized controlled trial. BMC Public Health. 2017;17:767. [Link] [DOI:10.1186/s12889-017-4783-9] [PMID] [PMCID]
28. Rajab LD, Petersen PE, Bakaeen G, Hamdan MA. Oral health behavior of schoolchildren and parents in Jordan. Int J Paediatr Dent. 2002;12(3):168-76. [Link] [DOI:10.1046/j.1365-263X.2002.00359.x] [PMID]
29. Worthington HV, Hill KB, Mooney J, Hamilton FA, Blinkhorn AS. A cluster randomized controlled trial of a dental health education program for 10‐year‐old children. J Public Health Dent. 2001;61(1):22-7. [Link] [DOI:10.1111/j.1752-7325.2001.tb03351.x] [PMID]
30. Biesbrock AR, Walters PA, Bartizek RD. Initial impact of a national dental education program on the oral health and dental knowledge of children. J Contemp Dent Pract. 2003;4(2):1-10. [Link] [DOI:10.5005/jcdp-4-2-1]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |