



Volume 9, Issue 1 (2021)
Health Educ Health Promot 2021, 9(1): 67-71 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Asadi Z, Raiisi F, Amini F, Esmaili Nasab M. The Efficacy of Heart Scan due to Visual-Written Training on Anxiety in Patients with Cardiovascular Diseases. Health Educ Health Promot 2021; 9 (1) :67-71
URL: http://hehp.modares.ac.ir/article-5-46171-en.html
URL: http://hehp.modares.ac.ir/article-5-46171-en.html
1- Shahid Rajaei Cardiovascular Hospital, Tehran, Iran
2- Institute of Cognitive Science Study (IRCSS), Tehran, Iran
3- Health Education and Health Promotion Department, Tarbiat Modares University, Tehran, Iran ,fereshtehamini@modares.ac.ir
4- Psychology Department, Tarbiat Modares University, Tehran, Iran
2- Institute of Cognitive Science Study (IRCSS), Tehran, Iran
3- Health Education and Health Promotion Department, Tarbiat Modares University, Tehran, Iran ,
4- Psychology Department, Tarbiat Modares University, Tehran, Iran
Keywords: Heart Scan [MeSH], Visual-Written Training [MeSH], Anxiety [MeSH], Cardiovascular Diseases [MeSH], Patients [MeSH]
Full-Text [PDF 481 kb]
(3927 Downloads)
| Abstract (HTML) (2379 Views)
Full-Text: (497 Views)
Introduction
Cardiovascular disease is pointed to disease of the heart and blood vessels. This disease and its variants in industrial societies often cause death, and 3.1 People over 35 die from heart disease, especially coronary artery disease [1]. In Iran, cardiovascular disease led to 46% of all deaths [2]. A systematic review showed that smoking, diabetes mellitus, obesity, and psychological factors are related to cardiovascular disease [3]. On the other hand; most mental illnesses are seen as a complication of heart disease. Depression, anxiety, delirium, and cognitive disorders are common problems in these patients [4]. In some studies, anxiety is a core cause for cardiovascular disease, and other psychological problems are in second grade [5]. Moreover, cardiovascular disease is linked to chronic anxiousness in men and new onset of anxiousness in women [6].
About 20% of people in the United States die from cardiovascular diseases, 8% related to heart attack and stroke, each year. About. More than 3/4 of cardiovascular deaths occur in low-and middle-income countries. Of the 16 million deaths from non-communicable diseases under the age of 70, 82% occur in countries with low socioeconomic status, and about 40% of deaths in these communities are due to cardiovascular disease [7].
Cardiac or heart scan is a diagnostic procedure before coronary artery bypass graft surgery to assess the viability of heart tissue and the extent, severity, and location of ischemia [8]. This test is basically non-invasive. It is based on the fact that exercising with a treadmill or drug stress and the injection of radioactive material shows the functional and physiological changes in the blood flow to the heart muscle [9]. This test causes the patient to worry and anxiety and, therefore, reduces the imaging quality [10].
Lack of familiarity with the course of treatment and causing concern in patients leads to frequent questions from medical staff, leading to burnout in the long term. The staff of different treatment and diagnostic departments can take the necessary measures such as familiarizing the patient with the environment, providing the necessary training before each operation, which will play an important role in reducing their anxiety [11].
Today, education and training in the field of health seem to be essential. Because education and training to individuals and society lead them to maintain and promote health and cause a person to adapt to any situation [12]. In education, the patient is taught a combination of different teaching methods and behavior modification techniques, and finally, it promotes healthy behavior in the patient [13]. Education and training give the patient sufficient information and make it easy to tolerate treatment during invasive and non-invasive treatments. In general, education leads to satisfaction and satisfaction with treatment according to the culture and personality of the patient [14]. One of the educational and training methods is using videotapes, which shows real live samples and is a valuable tool in understanding the clinical procedures and how to take care of yourself [15]. Therefore, by giving enough information and creating calm, the patient can be helped to endure the fears caused by unfamiliar situations [16].
In China, a study indicated training influenced on reduction of anxiety of gastroscopy patients [17]. Another research in children showed a reducing anxiety score due to gastroscopy-related stress in the experimental group [18]. Another study reported anxiety reduction due to standardized procedural information on patients' coping style on pre-gastroscopy [19]. In Iran, Momeni (2006), in a study in Tehran Heart Center Hospital, showed that training with two video and training booklet methods at two different times reduces preoperative anxiety in patients undergoing coronary artery bypass grafting [20]. A study indicated an educational video intervention about cardiac scan might effectively decrease anxiety levels before scanning [21].
Despite the importance of this issue, such a package for heart scan has not been prepared in Iran so far. Due to these points, not enough studies have been done in this area regarding psychological variables. There is still room for further research, even with various psychological variables, and evaluate the effectiveness of protocols on psychological aspects to determine the presence or absence of what kind of interventions are on the psychological state and their intensification and continuation. Thus, the purpose of this study was to investigate the efficacy of radiation therapy with written-visual training on the anxiety of heart scan in cardiovascular patients of Shahid Rajaei Heart Hospital. Accordingly, researchers seek to answer the following questions: Is a written-visual training package effective in reducing the anxiety of heart scan patients?
Materials & Methods
The present study was applied research, and its method was quasi-experimental with a pretest-posttest design with a control group. This study was performed on cardiovascular patients in Shahid Rajaei Cardiovascular Center in Tehran in 1398. One hundred patients were selected as at-reach and candidate sampling methods. Inclusion criteria were 25 to 50 years old, understanding Persian language fluency, having a sixth-grade education and above, and exclusion criteria were membership in medical and paramedical staff, history of cardiac scans, and known systemic or mental illness. Based on Cohen's formula and considering the error of the first and second types and the difference between the expected mean in the study groups, the sample size of Twelve people were used as a sample that Due to the size of the work, the drop-in participants, and the nature of the research, the researchers divided the two groups (50 in the control group, 50 in the written-video training). Intervention methods were performed on the experimental group. Before and after the training, all groups completed the Spielberger Anxiety Inventory.
Demographic questionnaire: that includes gender, age, the duration of illness, and so on.
Spielberger Anxiety Inventory: The Spielberger Anxiety Standardized Inventory showed the level of patient anxiety and was developed in 1970 by Berger et al. To determine situational and characteristic anxiety. This questionnaire consists of 40 questions, the first 20 questions assess the state of anxiety (overt anxiety), and the second 20 questions assess the vein of anxiety (covert anxiety). In another word, this questionnaire assesses general and normal anxiety. The answers are on the four-point Likert scale (from 1 to 4). In the end, the sum of the scores obtained for both the first part (overt anxiety) and the second part (covert anxiety) in one of the three groups of mild anxiety (score 20-39), moderate anxiety (score 59-40), severe anxiety (score 80-61) and 80 above is a very strong score. Scoring weights are inverse for expressions that indicate no anxiety. Items that are scored in reverse when scoring are Anxiety Scale: 20-19-16-15-11-10-8-5-2-1, Anxiety Vein Scale: 39-36-34-33-30-27-26-23-21.
There are two subscales: state and vein of anxiety. Some questions are scored in reverse. Therefore, each subscale scores between 20 and 80. Mehram in a study to standardize the Spielberger test and examined the reliability coefficient of the test in two groups of norm and criterion separately. Reliability for the normal group (n=600) in the overt and covert anxiety scale based on Cronbach's alpha was 0.91 and 0.90, respectively, and in the criterion group (n=130) was 0.94. The reliability of the test was calculated via the variance of real scores, and its value was recorded in the normal group of 0.94. The error of the standard of the measurement test is 4.64.
Moreover, the correlation of the observed scores with the true score was equal to 0.97, and the error scores were equal to 0.23. In the study of Khanipour et al., the homogeneity coefficient of this test was 0.66 by Cronbach's alpha method. In test standardization in Iran, the test-retest validity for the Anxiety Trait Scale was 0.65 to 0.86. Cronbach's alpha coefficient for the anxiety state was calculated to be 0.92 [22].
The implementation method was such that after obtaining moral and executive permission from the center officials and approving the subject of the research plan from the research unit and the officials of the hospital and the medical department of the research nucleus, the research began. Receiving a written referral letter from the hospital security unit to prepare an educational video in the nuclear medicine department was the next stage of the research process. This training package includes a figurative CD including all the stages of heart scan from the beginning, including admission, appointment, recovery, exercise test or in case of inability to perform exercise test, drug stress, then the imaging stage with gamma camera devices as SPECT was prepared. In the written training package, the same steps were prepared in the form of a booklet. All steps were explained to the participants in writing, and their satisfaction was expressed in writing, and the researcher undertook to observe ethical principles such as confidentiality of the participants' information. Participants read the video CD and text training between the first visit, the day of the appointment, and the scheduled time of the day, which is usually between 3-5 days. In addition to descriptive statistics, a one-way analysis of covariance was used to analyze the data.
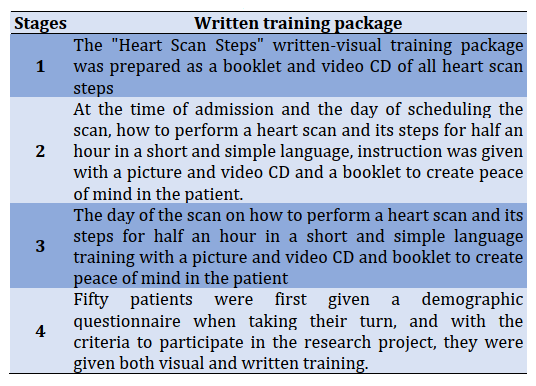
Table 1) Patient training stages before myocardial perfusion scan
Data were analyzed by SPSS 23 software using the Pearson correlation test and linear regression analysis. At first, the normality of the distribution of variables was evaluated by the Kolmogorov-Smirnov test.
Findings
According to the findings on the distribution of demographic scores, out of 100 participants in this study, 46 were men, and 54 were women, of whom 33 were under 50. The mean age of patients in the study was 36.2±8.9 years old.
The mean scores of anxiety a are shown there are differences in pre and post-test (Table 2).
Table 2) Mean±SD of anxiety in pre and post-test

The results of the normality test via Kolmogorov-Smirnov indicated that there is normal distribution in participants' scores. In the end, the written-video training group's anxiety in pre and post-test was 86.28 and 78.04, respectively. This means that the mean of anxiety before admission does not show a difference between the two groups. However, after implementing training measures, the mean of anxiety decreased significantly (p<0.05). While in the control group, no significant change was observed in the mean of anxiety. Therefore, a significant difference was observed between the types of training in the two groups, and anxiety in cardiovascular patients reduced by this training.
Based on the results, the significance level of one-way analysis of variance shows that the repetition of the test, the differences between the means of the three significant groups, is significant (p<0/001).
Discussion
This study aimed to determine the effectiveness of presenting a written-video training package cardiac scan steps on anxiety in cardiovascular patients. The results showed that the mean of anxiety in the experimental group changed. Moreover, the results of one-way analysis of variance showed that there significant reducing anxiety after training. Therefore, the results of this study were based on a study by Callaghan that video and text education in Chinese outpatients reduced their anxiety. In contrast, testing [17] and Momeni that training with two video and training booklet methods at two different times affects preoperative anxiety in patients undergoing vascular transplantation [20] are consistent.
By explaining this finding, it can be stated that although being aware of an unknown situation is associated with a decrease in anxiety. However, if too much or too little is said about a situation and the patient is given too much or too little information about it, it causes anxiety in the patient [22]. However, since the heart scan is associated with specific physical activities, providing video tutorials that show the whole process with regular images allows the person to do all the movement activity they need in advance and when they can see them all beforehand [23]. This helps the patient better understand and follow the instructions provided by the nurse later in the test (heart scan) [24]. In addition, as seen in the effect on anxiety, written-figurative training is effective, but there is no preference between these teaching methods. Therefore, it can be concluded that in cases of planning for education and reducing costs, video training has a better effect than increasing training on increasing the level of anxiety of patients [25].
This study is not without limitations, including that this variable has not been investigated in larger samples with different and the sampling method was purposive. Therefore, it is recommended that future studies provide a more comprehensive study with a higher sample size and probabilistic sampling in order to generalize the findings. Another limitation of this study is the cross-sectional nature study. Therefore, it is suggested that in future studies, the sampling method for cardiac patients is used and if access to the sample, follow-up steps be added to the study.
Conclusion
To conclude, it seems that training patients before performing a myocardial perfusion scan has a significant effect on reducing patients' anxiety and leads to better results and less time wasted. Moreover, there are no significant differences between the groups.
Acknowledgments: The authors announce their gratitude and appreciation to all participants who contribute to this study.
Ethical Permissions: In this study, all ethical principles were respected. The target and procedures of the study were explained for the participants, and the consent form was signed by all participants. This manuscript was taken from a master's thesis and had an ethical code.
Conflict of Interests: The authors declare that there is no interest in confidence.
Authors' Contributions: Asadi Z. (First author), Original researcher (30%); Raiisi F. (Second author), Introduction author/Methodologist/Discussion author (20%); Amini F. (Third author), Assistant (30%); Esmaili Nasab M. (Forth author), Assistant (20%).
Funding/Sources: No declared.
Cardiovascular disease is pointed to disease of the heart and blood vessels. This disease and its variants in industrial societies often cause death, and 3.1 People over 35 die from heart disease, especially coronary artery disease [1]. In Iran, cardiovascular disease led to 46% of all deaths [2]. A systematic review showed that smoking, diabetes mellitus, obesity, and psychological factors are related to cardiovascular disease [3]. On the other hand; most mental illnesses are seen as a complication of heart disease. Depression, anxiety, delirium, and cognitive disorders are common problems in these patients [4]. In some studies, anxiety is a core cause for cardiovascular disease, and other psychological problems are in second grade [5]. Moreover, cardiovascular disease is linked to chronic anxiousness in men and new onset of anxiousness in women [6].
About 20% of people in the United States die from cardiovascular diseases, 8% related to heart attack and stroke, each year. About. More than 3/4 of cardiovascular deaths occur in low-and middle-income countries. Of the 16 million deaths from non-communicable diseases under the age of 70, 82% occur in countries with low socioeconomic status, and about 40% of deaths in these communities are due to cardiovascular disease [7].
Cardiac or heart scan is a diagnostic procedure before coronary artery bypass graft surgery to assess the viability of heart tissue and the extent, severity, and location of ischemia [8]. This test is basically non-invasive. It is based on the fact that exercising with a treadmill or drug stress and the injection of radioactive material shows the functional and physiological changes in the blood flow to the heart muscle [9]. This test causes the patient to worry and anxiety and, therefore, reduces the imaging quality [10].
Lack of familiarity with the course of treatment and causing concern in patients leads to frequent questions from medical staff, leading to burnout in the long term. The staff of different treatment and diagnostic departments can take the necessary measures such as familiarizing the patient with the environment, providing the necessary training before each operation, which will play an important role in reducing their anxiety [11].
Today, education and training in the field of health seem to be essential. Because education and training to individuals and society lead them to maintain and promote health and cause a person to adapt to any situation [12]. In education, the patient is taught a combination of different teaching methods and behavior modification techniques, and finally, it promotes healthy behavior in the patient [13]. Education and training give the patient sufficient information and make it easy to tolerate treatment during invasive and non-invasive treatments. In general, education leads to satisfaction and satisfaction with treatment according to the culture and personality of the patient [14]. One of the educational and training methods is using videotapes, which shows real live samples and is a valuable tool in understanding the clinical procedures and how to take care of yourself [15]. Therefore, by giving enough information and creating calm, the patient can be helped to endure the fears caused by unfamiliar situations [16].
In China, a study indicated training influenced on reduction of anxiety of gastroscopy patients [17]. Another research in children showed a reducing anxiety score due to gastroscopy-related stress in the experimental group [18]. Another study reported anxiety reduction due to standardized procedural information on patients' coping style on pre-gastroscopy [19]. In Iran, Momeni (2006), in a study in Tehran Heart Center Hospital, showed that training with two video and training booklet methods at two different times reduces preoperative anxiety in patients undergoing coronary artery bypass grafting [20]. A study indicated an educational video intervention about cardiac scan might effectively decrease anxiety levels before scanning [21].
Despite the importance of this issue, such a package for heart scan has not been prepared in Iran so far. Due to these points, not enough studies have been done in this area regarding psychological variables. There is still room for further research, even with various psychological variables, and evaluate the effectiveness of protocols on psychological aspects to determine the presence or absence of what kind of interventions are on the psychological state and their intensification and continuation. Thus, the purpose of this study was to investigate the efficacy of radiation therapy with written-visual training on the anxiety of heart scan in cardiovascular patients of Shahid Rajaei Heart Hospital. Accordingly, researchers seek to answer the following questions: Is a written-visual training package effective in reducing the anxiety of heart scan patients?
Materials & Methods
The present study was applied research, and its method was quasi-experimental with a pretest-posttest design with a control group. This study was performed on cardiovascular patients in Shahid Rajaei Cardiovascular Center in Tehran in 1398. One hundred patients were selected as at-reach and candidate sampling methods. Inclusion criteria were 25 to 50 years old, understanding Persian language fluency, having a sixth-grade education and above, and exclusion criteria were membership in medical and paramedical staff, history of cardiac scans, and known systemic or mental illness. Based on Cohen's formula and considering the error of the first and second types and the difference between the expected mean in the study groups, the sample size of Twelve people were used as a sample that Due to the size of the work, the drop-in participants, and the nature of the research, the researchers divided the two groups (50 in the control group, 50 in the written-video training). Intervention methods were performed on the experimental group. Before and after the training, all groups completed the Spielberger Anxiety Inventory.
Demographic questionnaire: that includes gender, age, the duration of illness, and so on.
Spielberger Anxiety Inventory: The Spielberger Anxiety Standardized Inventory showed the level of patient anxiety and was developed in 1970 by Berger et al. To determine situational and characteristic anxiety. This questionnaire consists of 40 questions, the first 20 questions assess the state of anxiety (overt anxiety), and the second 20 questions assess the vein of anxiety (covert anxiety). In another word, this questionnaire assesses general and normal anxiety. The answers are on the four-point Likert scale (from 1 to 4). In the end, the sum of the scores obtained for both the first part (overt anxiety) and the second part (covert anxiety) in one of the three groups of mild anxiety (score 20-39), moderate anxiety (score 59-40), severe anxiety (score 80-61) and 80 above is a very strong score. Scoring weights are inverse for expressions that indicate no anxiety. Items that are scored in reverse when scoring are Anxiety Scale: 20-19-16-15-11-10-8-5-2-1, Anxiety Vein Scale: 39-36-34-33-30-27-26-23-21.
There are two subscales: state and vein of anxiety. Some questions are scored in reverse. Therefore, each subscale scores between 20 and 80. Mehram in a study to standardize the Spielberger test and examined the reliability coefficient of the test in two groups of norm and criterion separately. Reliability for the normal group (n=600) in the overt and covert anxiety scale based on Cronbach's alpha was 0.91 and 0.90, respectively, and in the criterion group (n=130) was 0.94. The reliability of the test was calculated via the variance of real scores, and its value was recorded in the normal group of 0.94. The error of the standard of the measurement test is 4.64.
Moreover, the correlation of the observed scores with the true score was equal to 0.97, and the error scores were equal to 0.23. In the study of Khanipour et al., the homogeneity coefficient of this test was 0.66 by Cronbach's alpha method. In test standardization in Iran, the test-retest validity for the Anxiety Trait Scale was 0.65 to 0.86. Cronbach's alpha coefficient for the anxiety state was calculated to be 0.92 [22].
The implementation method was such that after obtaining moral and executive permission from the center officials and approving the subject of the research plan from the research unit and the officials of the hospital and the medical department of the research nucleus, the research began. Receiving a written referral letter from the hospital security unit to prepare an educational video in the nuclear medicine department was the next stage of the research process. This training package includes a figurative CD including all the stages of heart scan from the beginning, including admission, appointment, recovery, exercise test or in case of inability to perform exercise test, drug stress, then the imaging stage with gamma camera devices as SPECT was prepared. In the written training package, the same steps were prepared in the form of a booklet. All steps were explained to the participants in writing, and their satisfaction was expressed in writing, and the researcher undertook to observe ethical principles such as confidentiality of the participants' information. Participants read the video CD and text training between the first visit, the day of the appointment, and the scheduled time of the day, which is usually between 3-5 days. In addition to descriptive statistics, a one-way analysis of covariance was used to analyze the data.
Table 1) Patient training stages before myocardial perfusion scan
Data were analyzed by SPSS 23 software using the Pearson correlation test and linear regression analysis. At first, the normality of the distribution of variables was evaluated by the Kolmogorov-Smirnov test.
Findings
According to the findings on the distribution of demographic scores, out of 100 participants in this study, 46 were men, and 54 were women, of whom 33 were under 50. The mean age of patients in the study was 36.2±8.9 years old.
The mean scores of anxiety a are shown there are differences in pre and post-test (Table 2).
Table 2) Mean±SD of anxiety in pre and post-test
The results of the normality test via Kolmogorov-Smirnov indicated that there is normal distribution in participants' scores. In the end, the written-video training group's anxiety in pre and post-test was 86.28 and 78.04, respectively. This means that the mean of anxiety before admission does not show a difference between the two groups. However, after implementing training measures, the mean of anxiety decreased significantly (p<0.05). While in the control group, no significant change was observed in the mean of anxiety. Therefore, a significant difference was observed between the types of training in the two groups, and anxiety in cardiovascular patients reduced by this training.
Based on the results, the significance level of one-way analysis of variance shows that the repetition of the test, the differences between the means of the three significant groups, is significant (p<0/001).
Discussion
This study aimed to determine the effectiveness of presenting a written-video training package cardiac scan steps on anxiety in cardiovascular patients. The results showed that the mean of anxiety in the experimental group changed. Moreover, the results of one-way analysis of variance showed that there significant reducing anxiety after training. Therefore, the results of this study were based on a study by Callaghan that video and text education in Chinese outpatients reduced their anxiety. In contrast, testing [17] and Momeni that training with two video and training booklet methods at two different times affects preoperative anxiety in patients undergoing vascular transplantation [20] are consistent.
By explaining this finding, it can be stated that although being aware of an unknown situation is associated with a decrease in anxiety. However, if too much or too little is said about a situation and the patient is given too much or too little information about it, it causes anxiety in the patient [22]. However, since the heart scan is associated with specific physical activities, providing video tutorials that show the whole process with regular images allows the person to do all the movement activity they need in advance and when they can see them all beforehand [23]. This helps the patient better understand and follow the instructions provided by the nurse later in the test (heart scan) [24]. In addition, as seen in the effect on anxiety, written-figurative training is effective, but there is no preference between these teaching methods. Therefore, it can be concluded that in cases of planning for education and reducing costs, video training has a better effect than increasing training on increasing the level of anxiety of patients [25].
This study is not without limitations, including that this variable has not been investigated in larger samples with different and the sampling method was purposive. Therefore, it is recommended that future studies provide a more comprehensive study with a higher sample size and probabilistic sampling in order to generalize the findings. Another limitation of this study is the cross-sectional nature study. Therefore, it is suggested that in future studies, the sampling method for cardiac patients is used and if access to the sample, follow-up steps be added to the study.
Conclusion
To conclude, it seems that training patients before performing a myocardial perfusion scan has a significant effect on reducing patients' anxiety and leads to better results and less time wasted. Moreover, there are no significant differences between the groups.
Acknowledgments: The authors announce their gratitude and appreciation to all participants who contribute to this study.
Ethical Permissions: In this study, all ethical principles were respected. The target and procedures of the study were explained for the participants, and the consent form was signed by all participants. This manuscript was taken from a master's thesis and had an ethical code.
Conflict of Interests: The authors declare that there is no interest in confidence.
Authors' Contributions: Asadi Z. (First author), Original researcher (30%); Raiisi F. (Second author), Introduction author/Methodologist/Discussion author (20%); Amini F. (Third author), Assistant (30%); Esmaili Nasab M. (Forth author), Assistant (20%).
Funding/Sources: No declared.
Article Type: Original Research |
Subject:
Health Education and Health Behavior
Received: 2020/10/20 | Accepted: 2021/01/25 | Published: 2021/05/17
Received: 2020/10/20 | Accepted: 2021/01/25 | Published: 2021/05/17
References
1. Kwok CS, Pradhan A, Khan MA, Anderson SG, Keavney BD, Myint PK, et al. Bariatric surgery and its impact on cardiovascular disease and mortality: A systematic review and meta-analysis. Int J Cardiol. 2014;173(1):20-8. [Link] [DOI:10.1016/j.ijcard.2014.02.026] [PMID]
2. Sarrafzadegan N, Mohammadifard N. Cardiovascular disease in Iran in the last 40 years:Prevalence, mortality, morbidity, challenges and strategies for cardiovascular prevention. Arch Iran Med. 2019;22(4):204-10. [Link]
3. Motlagh B, O'Donnell M, Yusuf S. Prevalence of cardiovascular risk factors in the Middle East:a systematic review. Eur J Cardiovasc Prev Rehabil. 2009;16(3):268-80. [Link] [DOI:10.1097/HJR.0b013e328322ca1b] [PMID]
4. Hoseinzadeh T, Paryad A, Asiri Sh, Kazemnezhad Leili E. Relationship between perception of illness and general self-efficacy in coronary artery disease patients. J Holist Nurs Midwifery. 2012;22(1):1-8. [Persian] [Link]
5. Allgulander C. Anxiety as a risk factor in cardiovascular disease. Curr Opin Psychiatry. 2016;29(1):13-7. [Link] [DOI:10.1097/YCO.0000000000000217] [PMID]
6. Reiner IC, Tibubos AN, Werner AM, Ernst M, Brähler E, Wiltinket J, et al. The association of chronic anxiousness with cardiovascular disease and mortality in the community:results from the Gutenberg Health Study. Sci Rep. 2020;10:12436. [Link] [DOI:10.1038/s41598-020-69427-8] [PMID] [PMCID]
7. Sacks FM, Lichtenstein AC, WU JHY, Appel LJ. Creager MA, Kris-Etherton PM, Miller M, Rimm EB. Rudel LL, et al. Dietary fats and cardiovascular disease: A presidential advisory from the American Heart Association. Circulation. 2017;136:e1-23. [Link] [DOI:10.1161/CIR.0000000000000510] [PMID]
8. Henkin RE. Nuclear medicine. 2nd Volume. Baltimore: Mosby Elsevier; 2006. [Link]
9. Ell PJ, Gambhir S. Nuclear medicine in clinical diagnosis and treatment. Radiology. 2005;236(3). [Link] [DOI:10.1148/radiol.2363052522]
10. Nightingale JM, Murphy FJ, Blakeley C. 'I thought it was just an X-ray': A qualitative investigation of patient experiences in cardiac SPECT-CT imaging. Nucl Med Commun. 2012;33(3):246-54. [Link] [DOI:10.1097/MNM.0b013e32834f90c6] [PMID]
11. Zaret BL, Beller G. Clinical nuclear cardiology: State of the art and future directions. 4th Edition. Baltimore: Mosby Elsevier; 2010. [Link]
12. Ogden J. Health psychology: A textbook. New York: McGraw-Hill Education; 2012. [Link]
13. Urden L, Stacy K, Lough ME. Critical care nursing: Diagnosis and management. 8th Edition. Baltimore: Mosby Elsevier; 2017. [Link]
14. Phyllis M. Community health nursing. Am J Nurs. 2009;109:19. [Link] [DOI:10.1097/01.NAJ.0000343102.62178.80]
15. Eslami Akbar R, Elahi N, Mohammadi E, Fallahi Khoshknab M. How do the nurses cope with job stress? A study with grounded theory approach. J Caring Sci. 2017;6(3):199-211. [Link] [DOI:10.15171/jcs.2017.020] [PMID] [PMCID]
16. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. Heart disease and stroke statistics--2014 update: A report from the American Heart Association. Circulation. 2014;129(3):e28-292. [Link]
17. Callaghan P, Chan HC. The effect of videotaped or written information on Chinese gastroscopy patients' clinical outcomes. Patient Educ Couns. 2001;42(3):225-30. [Link] [DOI:10.1016/S0738-3991(00)00125-7]
18. Volkan B, Bayrak NA, Ucar C, Kara D, Yıldız S. Preparatory information reduces gastroscopy-related stress in children as confirmed by salivary cortisol. Saudi J Gastroenterol. 2019;25(4):262-7. [Link] [DOI:10.4103/sjg.SJG_493_18] [PMID] [PMCID]
19. Liu YY, Liu YQ, Petrini MA. Effect of information of patients' coping style on pre-gastroscopy anxiety. Gastroenterol Nurs. 2018;41(1):47-58. [Link] [DOI:10.1097/SGA.0000000000000302] [PMID]
20. Moemeni L, Najaf Yarandi A, Haghani H. Comparative study of the effects of education using VCD and booklet in two different times on pre-operative anxiety. Iran J Nurs. 2009;21(56):81-93. [Persian] [Link]
21. Ayasrah SM, Ahmad MM. Educational video intervention effects on peri-procedural anxiety levels among cardiac catheterization patients: A randomized clinical trial. Res Theory Nurs Practi. 2016;30(1):70-84. [Link] [DOI:10.1891/1541-6577.30.1.70] [PMID]
22. Khani Pour H, Mohammad Khani P, Tabatabaii S. Strategies for controlling anxiety and anxiety traits: Predictors of morbid anxiety in the nonclinical sample. Behav Sci J. 5(2):173-8. [Persian] [Link]
23. Tooth L, McKenna K. Cardiac patient teaching: Application to patients undergoing coronary angioplasty and their partners. Patient Educ Couns. 1995;25(1):1-8. [Link] [DOI:10.1016/0738-3991(94)00659-A]
24. Asilioglo K , Celik S. The effect of preoperative education on anxiety of open cardiac surgery patient. Patient Educ Couns. 2004;53:62-70. [Link] [DOI:10.1016/S0738-3991(03)00117-4]
25. Nobahar M. Competence of nurses in the intensive cardiac care unit. Electron Physician. 2016;8(5):2395-404. [Link] [DOI:10.19082/2395] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |