Document Type : Original Research
Authors
1
“Department of Echocardiography, School of Medicine” and “Atherosclerosis Research Center”, Baqiyatallah University of Medical Sciences, Tehran, Iran
2
Student Research Committee, Baqiyatallah University of Medical Sciences, Tehran, Iran
3
Biostatistics Department, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
4
“Department of Echocardiography, School of Medicine” and “Department of Cardiology, School of Medicine”, Baqiyatallah University of Medical Sciences, Tehran, Iran
5
Health Management Research Center, Baqiyatallah University of Medical Sciences, Tehran, Iran
6
Faculty of Medicine, Tehran Medical Sciences Branch, Islamic Azad University, Tehran, Iran
Abstract
Aims: Considering the importance of mortality management in the control of COVID-19 disease, this study was performed to investigate the risk factors of mortality of adult inpatients with Covid-19 in Tehran, Iran using a retrospective cohort study.
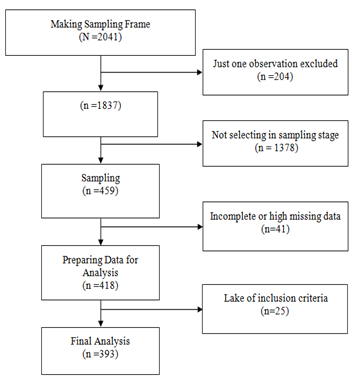
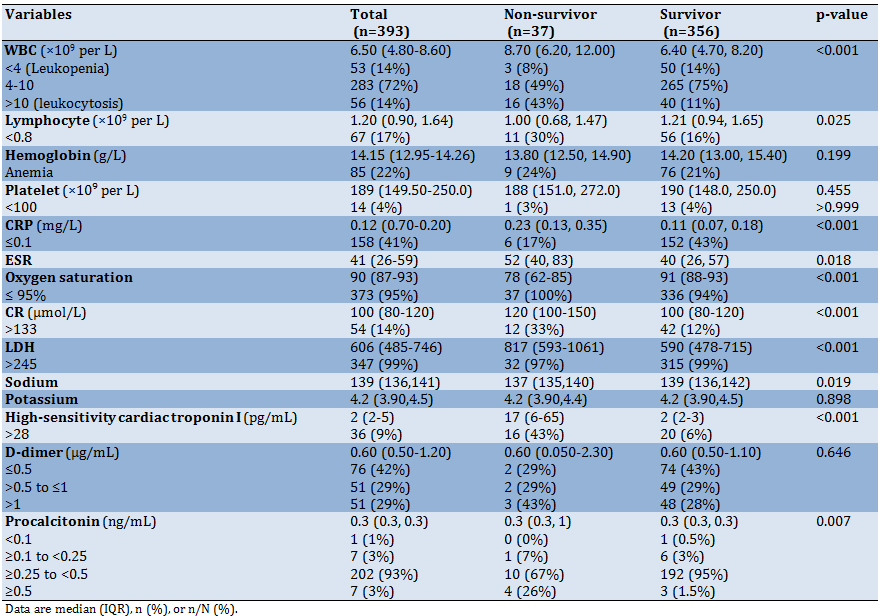
Material & Methods: This retrospective cohort study was performed among a random sample of confirmed COVID-19 hospitalized patients, in a main general military hospital in Tehran city (Iran). Laboratory data, clinical sign and symptom, treatment and demographic data were collected and compared between survivors and non-survivors patients.
Findings: Among 393 patients who contributed in this study, 37 (9.4%) with 95% confidence interval (6.7% to 12.7%) died during hospitalization. The result of this study also showed that comorbidity like hypertension and CHF, vital sign like dyspnea, RR>24 and Oxygen saturation also laboratory variable like white blood cell, Lymphocyte, C-reactive protein, CR, ESR, Lactate dehydrogenase, Sodium, troponin, Procalcitonin in addition lesion type shown the significant relationship with patients death. The findings of this study showed that the use of drug including Kaltra, Vancomycin, Ribavirin, Meropenem, Levofloxasin, and Methyiprednisolon increased the risk of death but use of drug like Azithromycin, Hydroxychloroquin and Naproxen decrease risk of death in COVID-19 hospitalized patients. More results also showed that ARDS, acute kidney injury and intubation are the most cause of death among patients.
Conclusion: According to the risk factors identified in this study, patients with a higher chance of death can be identified and the necessary treatment measures can be taken to reduce the risk of COVID-19 hospitalized patients.
Keywords
Subjects