1
Electron Microscope Unit, Faculty of Pharmacy, Basra University, Basra, Iraq
2
Department of Pharmacology and Toxicology, Faculty of Pharmacy, Basra University, Basra, Iraq
Abstract
Aims: There is a relationship between environmental pollutants, particularly heavy metals, the risk of water pollution, and diseases in numerous areas. This study aimed to assess the water quality by measuring physio-chemical properties and heavy metals contents at two water stations in Basra city, Iraq.
Materials & Methods: The water samples were collected from two main water stations of Al-Baradi’yah and Al-Jubaila. The pH values, turbidity, and TDS of the water samples were measured, and the heavy metals analysis of Cd, Cr, and Cu was done by the direct extraction/air acetylene flame method using a flame atomic absorption spectrometer. The results of the parameters were compared with the safe limits of WHO.
Findings: The turbidity and total TDS for both stations showed a significant difference, whereas the pH values were not, referring to the raw and tap water at both stations being acidic (pH<7). A significant difference was observed between the level of Cr and Cd in the raw and tap water samples within the acceptable levels of WHO. A significant difference was observed in the Cu levels in Al-Bharatiya (p<0.05).Whereas, no significant difference was observed between the chromium levelin the water samples of the Al-Jubaila station (p>0.05).The amount of the Pb was shown a slight increase from the acceptable levels in the tap water at Al-Baradi’yah station and the raw and tap water at the Al-Jubaila site.
Conclusion: A part of the chemical parameters is within the WHO acceptable limits, except water turbidity and Pb levels.
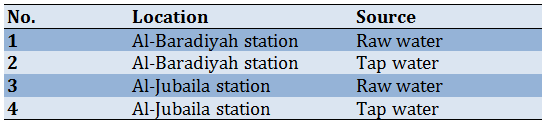
Introduction Pure drinking water has been recognized as an essential right of human beings. It plays a vital role in human health and welfare [1]. Harmful effects on living organisms can occur due to any change in physical, chemical, or biological properties of water quality (pollution) [2]. Plants, fish, birds, humans, and other animals, are all affected by water pollution [2]. Water pollution can be defined as an alteration in the components of the watercourse due to human activities, which produce less appropriate drinking water for domestic uses [3]. Geological conditions and industrial, agricultural, and water treatment plant activities may be considered potential sources of water contamination [1]. Characteristics of drinking water, including physical, biological, and chemical properties have great importance on human health [4]. It is necessary to investigate water's different physicochemical parameters before its usage for drinking, domestic, agricultural, or industrial purposes [5]. Numerous physical parameters such as pH, total solids, total dissolved solids, and total suspensions should be assessed to test water quality and purity [6]. Water turbidity is an indicator of water pollution due to the deterioration of organic matter and the improper disposal of domestic and industrial solid wastes and wastewater [6]. To obtain water with good quality and high purity, it is necessary to check out its heavy metal and organic contents, which is residues of pesticides [5]. Different biochemical and physiological functions in living organisms depend on the presence of metals in trace amounts; nevertheless, they convert to harmful ones following their excess acceptable limits [7]. Toxicity by heavy metals can reduce energy levels and impair the normal function of essential organs such as the brain, lungs, kidney, liver, blood components, and other substantial organs with subsequent organ damage [7]. Cadmium targets the kidney to be accumulated in the proximal tubular cells in excessive concentrations [7]. Long-term exposure to cadmium in trace amounts leads to its gradual accumulation inside the kidney and causes lung and bone disorders [4]. Copper has a central role as a fundamental trace element in the biochemistry of all living organisms, and it has an impact on enzymes activity as a cofactor or ingredient of various metalloenzymes such as superoxide dismutase, ceruloplasmin, lysyl oxidase, cytochrome oxidase, and tyrosinase [8]. Therefore, physiological activities, including neurotransmission, biosynthesis of tissue, free-radical defense, and cellular respiration, depend on copper availability [8]. Lead, the bluish-gray highly toxic metal, exists naturally in trace levels in the earth’s superficial layer [9]. Widespread utilization of lead has resulted in widespread environmental pollution and diseases in numerous areas of the world [9]. Intoxication by lead was classified as a classic disease that targets the central nervous system and gastrointestinal tract of children and adults [10]. Tap water is considered one of the sources of lead poisoning [11]. It has been observed in children's dysfunctions, including hyperactivity, anorexia, decreased play activity, low intelligence quotient, and poor school performance when exposed to high lead levels [12]. Initially, the distribution of lead in the body depends on the blood flow into different tissues [12]. Skeletal bones are the deposition place of more than 95% of lead as an insoluble phosphate [13]. Lead exposure at a high level might result in abortion in pregnant women and can damage the organs of sperm generation in men [14]. Lead chronic exposure can cause mental retardation birth defects, psychosis, autism, allergies, dyslexia, weight loss, hyperactivity, paralysis, muscular weakness, brain damage, and kidney damage and can result in death [14]. Basra city is located in the far south-eastern region of Iraq, and it is characterized by a dry–desert climate according to the climate classification Koppen [15]. The primary source of water in Basra is the Shatt al-Arab and its freshwater canals [15]. Two of the main water stations in the city center of Basra (Al-Baradi’yah and Al-Jubaila) were chosen for water sampling since these stations have well-established projects for water treatment. These stations depend on the Shatt al-Arab to draw raw water for purification before pumping it to the residents of Basra. This study aimed to assess the water quality by measuring physio-chemical properties and heavy metals contents at two water stations in Basra city, Iraq. Materials & Methods This descriptive cross-sectional research was conducted for one year (2021) in two main water stations (Al-Baradi’yah and Al-Jubaila) in the center of Basra city, Iraq. The samples of raw and tap water were collected through the mentioned stations with the assistance of the Basra water directorate staff. The water samples were collected in clean plastic bottles and then labeled and numbered according to their locations and sources (Table 1). The samples were kept at 4°C to avoid the effects of temperature and light. The collected water samples were analyzed to determine pH, turbidity, and total dissolved solids. The pH values of water samples were measured using a portable digital pH meter (8686 AZ Water Quality Testing pH Meter; GEXEX Laboratories; USA). After turning on the meter and submerging its probe in the water samples to be held for a moment, the values of each sample were recorded after stabilization. To measure water turbidity, standard procedures were followed using a turbidity meter. The meter holder was used to pour water samples to keep them inside for a few minutes. The result of each sample was noted following completing the reading stability. Regarding the total dissolved solids characteristics, the collected water samples were measured using one apparatus. The probe was calibrated using a standard solution. The total dissolved solids values were recorded following submerging of the probe in the water samples and the disappearance of the stability indicator. Following each measurement, the probe was rinsed with deionized water to avoid cross-contamination among different samples. The standard digestion method was followed by transferring 50 ml of each water sample into clean beakers. Then, 10 ml of concentrated HNO3 was added to each water sample to be shaken well [16]. Then, the hot plate was used to boil and evaporate the water samples to the lowest possible volume to be cooled at room temperature. For dilution, 25 ml of distilled water was then added to each water sample. The diluted samples were then shifted to 50ml clean plastic containers to be foiled and kept at 4°C until the analysis of the mentioned heavy metals [16]. The heavy metals analysis of Cd, Cr, and Cu, was done by following the direct extraction/air acetylene flame method using Flame Atomic Absorption Spectrometer (FAAS, AA7000, Shimadzu, Japan), available at Marine Science Centre of Basra University [16]. Before heavy metals analysis for each water sample, the standard solution for each tested element was prepared according to its concentration and utilized for system calibration. Automatically, the obtained heavy metal concentrations were recorded using a computer connected to the FAAS system. The findings were analyzed using paired t-test through SPSS 25 software. Table 1) Collected water samples locations and their sources
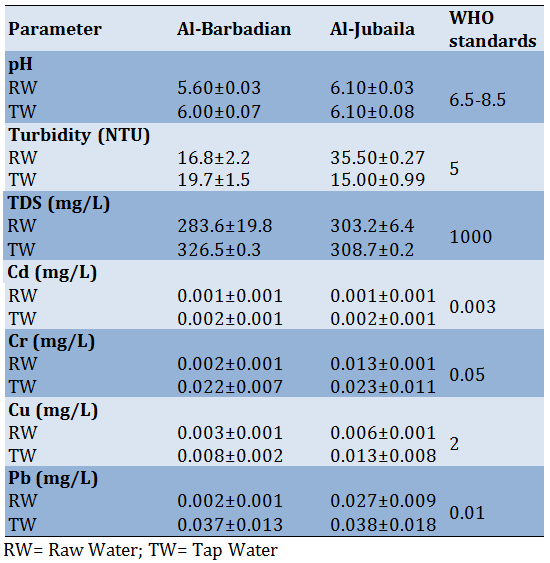
Findings There was no significant difference between the pH level in raw and tap water samples in Al-Baradiyah (p>0.05) and Al-Jubaila stations (p>0.05). The pH level showed acidic water in the stations (pH<7). Table 2) Physiochemical characteristics and the heavy metals concentrations (mean±SD) of the water samples
A significant difference was observed between the water turbidity in the raw and the tap water samples in Al-Baradiyah (p=0.003) and Al-Jubaila stations (p=0.002). The possible reason for the tap water turbidity elevation at Al-Baradiyah station (mean=19.7) is the poor purification system. The raw water turbidity at Al-Jubaila station (mean=35.5) is very high compared to its value at Al-Baradiyah station. This might be because the Al-Jubaila site draws the raw water from the deep surface of the Shatt al-Arab to be affected by the tap water turbidity. In addition, there was a significant difference between the level of dissolved solids outcomes between the raw and tap waters in the Al-Baradiyah station (p=0.026) and Al-Jubaila station (p=0.04), which were within the safe limits of WHO (<1000mg/L). In terms of heavy metals, a significant difference was observed between the level of copper and cadmium in the raw and tap water samples in the Al-Baradiyah station (p=0.001) and Al-Jubaila station (p=0.001), which level of copper and cadmium were within WHO acceptable levels less than 0.003 mg/L and 2 mg/L, respectively. A significant difference was observed in the chromium levels of the samples in Al-Baradiyah (p=0.047), whereas no significant difference was observed between the chromium level in the raw and tap water samples in Al-Jubaila station (p=0.08). The mean of the chromium level in the studied stations was within the world health organization's acceptable levels. There was a significant difference between the lead content in the raw and tap water samples in Al-Baradiyah (p=0.001) and Al-Jubaila stations (p=0.003). The lead content of the raw (0.027 mg/L), and the tap water samples (0.038 mg/L) in Al-Jubaila station, and tap water sample in Al-Baradiyah was higher than the allowable limits of WHO (0.01 mg/L). Discussion In this study, the water quality of two stations of Al-Jubaila and Al-Baradiyah in Basra, Iraq, was studied to evaluate the extent of water pollution. The mean pH values varied from 6.11 to 8.37, which indicated that the water was slightly acidic to alkaline. The findings of this study revealed slight acidity of drinking water, although the ideal pH for human consumption is stated to be 7.4 [17]. World Health Organization suggested a controlled pH of the water to reduce the contamination of drinking water. Several factors, including rock and soil composition and the presence of organic materials or other chemicals, affected the pH level of water. Napacho and Manyele [18] found that pH values in shallow tubewells varied between 6.7 and 8.3 due to dissolved minerals in the soil and rocks. They explained higher alkalinity by the presence of two common minerals, calcium and magnesium, affecting the hardness of the water. Water with low pH values shows the acidic condition of the water. Saadilong et al. [19] found that the relationship between water pH and other water quality parameters is different in different water systems and can be influenced by the presence of other parameters. Effective reduction of turbidity is one of the primary goals, especially for drinking water due to the negative effects on consumer acceptance. The results of this study showed turbidity elevation at the tap and row water samples in Al-Baradiyah and Al-Jubaila sites, respectively. Turbidity might interfere with filtration by clogging the filter prematurely. It can interfere with chemical disinfection by creating oxidant demand, UV irradiation by blocking light transmission, and reduce the efficacy of both by protecting microbes in aggregates or internal to other particles. Turbidity also has negative impacts on consumer acceptance of water. Turbidity is not a direct measure of microbial contamination, whereas microbes are often associated with particles in water. So, the purification of turbidity removes some microbes while reducing the levels of organic matter and other particles. Gauthier et al. [20] stated the increasing concentration of suspended particles in treated water during turbid events resulted in higher bacterial aerobic spore concentration for raw, treated, and distributed water. So, they emphasize the need to carefully monitor raw and treated water quality for utilities using “high-quality” water resources with limited treatment barriers, especially when such water resources are affected by even slight turbidity variations. The main ingredients of water TDS are the cat ions such as potassium, calcium, and magnesium and the anions such as carbonate bicarbonate, chloride sulfate, nitrate, etc. The level of TDS in the studied stations was within the standard limit by WHO (<1000mg/L). TDS in drinking water originates from resources such as sewage, urban run-offs, natural sources, chemicals in the water treatment process, industrial wastewater, or chemical fertilizers used in the garden. Water is a universal solvent and can dissolve these particles quickly. Although elevated levels of TDS in drinking water are not a health hazard, it does lend the water a bitter, salty, or brackish taste. Calcium and magnesium, two minerals commonly found in TDS, can also cause water hardness. Among the contents of TDS, dissolved calcium and magnesium in the water are called “Hardness”. Some mentioned ions are essential, whereas some ions are toxic to human health. For example, Islam et al. [21] found the alarming low TDS in drinking water. So, water purification to control the standard limits of TDS, especially for drinking water, is essential. In this study, the level of heavy metals in water samples in the two sites was within the acceptable limits by WHO. Several studies have evaluated the level of toxic metals in drinking water and reported that the concentrations of these metals are below permissible limits [22, 23]. However, emphasizing comparisons with standards is not enough to quantitatively assess the health risk of toxic element exposure via the consumption of drinking water. Based on the human health risk assessment models, exposure to toxic elements could increase the incidence of adverse effects on human health [24]. Heavy metals and arsenic contamination in drinking water are serious threats to human life because of their toxicity, persistence in the environment, and bio-accumulative nature [25]. The heavy metals contaminate the groundwater and surface water through natural processes and anthropogenic activities [26]. According to the World Health Organization (WHO) report in 2015, 71% of the global population uses safely managed drinking water sources [27]. This includes piped treated water that is located on the premises and protected dug wells [28]. However, safely managed water sources can still be polluted by toxic elements because of the poor domestic treatment system, use of chemical materials in the water treatment system, pipeline corrosion, leaching of elements from pipes of water distribution, and use of improper storage containers, etc. [29]. Most developing countries are faced with this challenge, especially due to their limited economic capacities to use advanced technologies for heavy metal removal [23]. The findings of this study showed the higher lead content of the raw (0.027 mg/L) and the tap water samples (0.038 mg/L) in Al-Jubail station and tap water sample in Al-Baradiyah than the allowable limits of WHO (0.01mg/L). Contact with lead is associated with several adverse health outcomes [30]. Studies have also conclusively shown that minority and low-income communities have the highest levels of lead exposure compared to their more affluent counterparts [31]. The causal link between lead exposure and severe cognitive health effects has been well established, as have other outcomes such as memory loss, abdominal pain, kidney damage, high blood pressure, and weakness [32]. There is a critical need to better characterize the concentration of lead. Fawkes and Sanson [32] stated that detectable traces of lead in drinking water frequently arise from lead pipes, faucets, and fixtures. So they recommend monitoring existing pipe networks for water managers because changing the water chemistry can impact the exposure risks. Lead-contaminated drinking water, even at low levels, is harmful to human health. Great strides toward the elimination of lead in drinking water and educate the consumers to be sensitive to the quality of the used water are essential. To avoid the phenomenon of water pollution with other pollutants, such as toxic elements and to inhibit elevation of the described parameters, should be raised public awareness on proper use and precautions to preserve water quality through inhibition from contaminations by physical, chemical, or biological pollutants. High-efficient filtration systems should be available at water stations to remove water impurities using a physical barrier, chemical, and/or biological method. It is necessary to remove potential sources of water pollution and provide state-certified testing laboratories with different instruments and chemicals for water quality analysis. In the next studies, it is suggested to increase the pathological analysis such as histological technique and also to increase the water stations to include the cities near Basra. In addition, it is suggested to study the relationship between bisphenol and water pollution. Conclusion The level of lead, turbidity, and pH are versus the allowable limits of WHO standards at both water stations in Basra city, Iraq. The rest of these parameters related to heavy metals exhibited an interesting reduction of Cu at both water stations and Cd at Al-Jubaila one against the acceptable levels of the indicated organization standards. Regarding the effect of the mentioned factors in drinking water on human health, it suggests more control over water purification.
Acknowledgments: Nothing to report. Ethical Permissions: Nothing to report. Conflicts of Interests: Nothing to report. Authors’ Contributions: Abbood H.M. (First author), Introduction author/Main Researcher/Discussion author/Methodologist (50%); AL-Moziel M.S. (Second Author), Methodologist/Assistant (30%); Ghanim W.K. (Third Author), Statistical Analyst/Assistant (20%) Funding/Support: Nothing to report.
References
1. Muhanga MI, Malungo JR. The what, why and how of health literacy: a systematic review of literature. 2017.
2. Wångdahl J, Lytsy P, Mårtensson L, Westerling R. Health literacy among refugees in Sweden–a cross-sectional study. BMC public health. 2014;14(1):1-12.
3. Health WCoSDo, Organization WH. Closing the gap in a generation: health equity through action on the social determinants of health: Commission on Social Determinants of Health final report: World Health Organization; 2008.
4. Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC public health. 2012;12(1):1-13.
5. Parker R, Ratzan SC. Health Literacy: A Second Decade of Distinction for Americans. Journal of Health Communication. 2010;15(sup2):20-33.
6. Peerson A, Saunders M. Health literacy revisited: what do we mean and why does it matter? Health promotion international. 2009;24(3):285-96.
7. Zumbo B, Kelly K, Begoray D, Kazanjian A, Mullet J, Hayes M. The development and validation of measures of “Health Literacy” in different populations. UBC Institute of Health Promotion Research and UVic Community Health Promotion Research: University of British Columbia. 2006.
8. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International. 2000;15(3):259-67.
9. Nutbeam D. The evolving concept of health literacy. Social science & medicine. 2008;67(12):2072-8.
10. Frisch A-L, Camerini L, Diviani N, Schulz PJ. Defining and measuring health literacy: how can we profit from other literacy domains? Health promotion international. 2012;27(1):117-26.
11. Berkman ND, Davis TC, McCormack L. Health Literacy: What Is It? Journal of Health Communication. 2010;15(sup2):9-19.
12. Dumenci L, Matsuyama R, Riddle DL, Cartwright LA, Perera RA, Chung H, et al. Measurement of cancer health literacy and identification of patients with limited cancer health literacy. Journal of health communication. 2014;19(sup2):205-24.
13. Leung AYM, Cheung MKT, Lou VWQ, Chan FHW, Ho CKY, Do TL, et al. Development and validation of the Chinese Health Literacy Scale for chronic care. Journal of health communication. 2013;18(sup1):205-22.
14. Kim MT, Song H-J, Han H-R, Song Y, Nam S, Nguyen TH, et al. Development and validation of the high blood pressure-focused health literacy scale. Patient education and counseling. 2012;87(2):165-70.
15. Nath CR, Sylvester ST, Yasek V, Gunel E. Development and validation of a literacy assessment tool for persons with diabetes. The Diabetes Educator. 2001;27(6):857-64.
16. Ghaffari M, Rakhshanderou S, Ramezankhani A, Mehrabi Y, Safari-Moradabadi A. Protocol of the TOHLA instrument: A Test of Oral Health Literacy in Adults. Journal of education and health promotion. 2020;9.
17. Williams KP, Templin TN, Hines RD. Answering the call: a tool that measures functional breast cancer literacy. J Health Commun. 2013;18(11):1310-25.
18. Bollweg TM, Okan O, Pinheiro P, Bröder J, Bruland D, Freţian AM, et al. Adapting the European Health Literacy Survey for Fourth-Grade Students in Germany: Questionnaire Development and Qualitative Pretest. HLRP: Health Literacy Research and Practice. 2020;4(2):e119-e28.
19. Davis TC, Wolf MS, Arnold CL, Byrd RS, Long SW, Springer T, et al. Development and validation of the Rapid Estimate of Adolescent Literacy in Medicine (REALM-Teen): a tool to screen adolescents for below-grade reading in health care settings. Pediatrics. 2006;118(6):e1707-14.
20. Teufl L, Vrtis D, Felder-Puig R. QUIGK-K: Quiz zur Erhebung von Gesundheitskompetenz bei Kindern. Prävention und Gesundheitsförderung. 2020;15(3):250-5.
21. Batterham RW, Hawkins M, Collins P, Buchbinder R, Osborne RH. Health literacy: applying current concepts to improve health services and reduce health inequalities. Public health. 2016;132:3-12.
22. Ancker JS, Grossman LV, Benda NC. Health Literacy 2030: Is It Time to Redefine the Term? Journal of general internal medicine. 2020;35(8):2427-30.
23. Brach C, Keller D, Hernandez LM, Baur C, Parker R, Dreyer B, et al. Ten attributes of health literate health care organizations. NAM Perspectives. 2012.
24. Kripalani S, Wallston K, Cavanaugh KL, Osborn C, Mulvaney S, McDougald Scott A, et al. Measures to assess a health-literate organization. Vanderbilt Center for Effective Health Communication. 2014.
25. Farmanova E, Bonneville L, Bouchard L. Organizational health literacy: review of theories, frameworks, guides, and implementation issues. INQUIRY: The Journal of Health Care Organization, Provision, and Financing. 2018;55:0046958018757848.
26. Koh HK, Brach C, Harris LM, Parchman ML. A proposed ‘health literate care model’would constitute a systems approach to improving patients’ engagement in care. Health affairs. 2013;32(2):357-67.
27. Palumbo R, Annarumma C, editors. The importance of being health literate: An organizational health literacy approach. EISIC-Ex Toulon-Verona Conference; 2014: Liverpool John Moores University.
28. Hayran O, Özer O. Organizational health literacy as a determinant of patient satisfaction. Public Health. 2018;163:20-6.
29. Weaver NL, Wray RJ, Zellin S, Gautam K, Jupka K. Advancing organizational health literacy in health care organizations serving high-needs populations: a case study. Journal of health communication. 2012;17(sup3):55-66.
30. Hayran O, Özer O. Organizational health literacy as a determinant of patient satisfaction. Public Health. 2018;163:20-6.
31. Abrams MA, Kurtz-Rossi S, Riffenburgh A, Savage B. Building health literate organizations: A guidebook to achieving organizational change. Journal of Research and Practice for Adult Literacy, Secondary, and Basic Education. 2014:69.
32. Baur C. The national action plan to improve health literacy. US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. 2010.
33. Ernstmann N, Halbach S, Kowalski C, Pfaff H, Ansmann L. Measuring attributes of health literate health care organizations from the patients’ perspective: Development and validation of a questionnaire to assess health literacy-sensitive communication (HL-COM). Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen. 2017;121:58-63.
34. Lloyd JE, Song HJ, Dennis SM, Dunbar N, Harris E, Harris MF. A paucity of strategies for developing health literate organisations: A systematic review. PloS one. 2018;13(4):e0195018.
35. Henrard G, Vanmeerbeek M, Buret L, Rademakers J. Dealing with health literacy at the organisational level, French translation and adaptation of the Vienna health literate organisation self-assessment tool. BMC health services research. 2019;19(1):1-9.
36. Palumbo R, Annarumma C. Empowering organizations to empower patients: An organizational health literacy approach. International Journal of Healthcare Management. 2018;11(2):133-42.
37. Brach C, Harris LM. Healthy People 2030 health literacy definition tells organizations: make information and services easy to find, understand, and use. Journal of General Internal Medicine. 2021;36(4):1084-5.
38. Sim D, Yuan SE, Yun JH. Health literacy and physician-patient communication: a review of the literature. Int J Commun Health. 2016;10:101-14.
39. Price-Haywood EG, Roth KG, Shelby K, Cooper LA. Cancer risk communication with low health literacy patients: a continuing medical education program. Journal of general internal medicine. 2010;25(2):126-9.
40. Yin HS, Jay M, Maness L, Zabar S, Kalet A. Health literacy: an educationally sensitive patient outcome. Journal of general internal medicine. 2015;30(9):1363-8.
41. Sany SBT, Behzhad F, Ferns G, Peyman N. Communication skills training for physicians improves health literacy and medical outcomes among patients with hypertension: a randomized controlled trial. BMC health services research. 2020;20(1):1-10.
42. Mabachi NM, Cifuentes M, Barnard J, Brega AG, Albright K, Weiss BD, et al. Demonstration of the health literacy universal precautions toolkit: Lessons for quality improvement. The Journal of ambulatory care management. 2016;39(3):199.
43. Allenbaugh J, Spagnoletti CL, Rack L, Rubio D, Corbelli J. Health literacy and clear bedside communication: a curricular intervention for internal medicine physicians and medicine nurses. MedEdPORTAL. 2019;15.
44. Nielsen-Bohlman L, Panzer A, Kindig D. Committee on Health Literacy. Health Literacy: A Prescription to End Confusion, 2004. The National Academies Press; 2006.
45. Developing Physician Communication Skills For Patient-Centered Care. Health Affairs. 2010;29(7):1310-8.
46. Khan A, Spector ND, Baird JD, Ashland M, Starmer AJ, Rosenbluth G, et al. Patient safety after implementation of a coproduced family centered communication programme: multicenter before and after intervention study. bmj. 2018;363.
47. Negarandeh R, Mahmoodi H, Noktehdan H, Heshmat R, Shakibazadeh E. Teach back and pictorial image educational strategies on knowledge about diabetes and medication/dietary adherence among low health literate patients with type 2 diabetes. Primary Care Diabetes. 2013;7(2):111-8.
48. Centrella-Nigro AM, Alexander C. Using the teach-back method in patient education to improve patient satisfaction. The Journal of Continuing Education in Nursing. 2017;48(1):47-52.
49. McCaffery KJ, Holmes-Rovner M, Smith SK, Rovner D, Nutbeam D, Clayman ML, et al. Addressing health literacy in patient decision aids. BMC Medical Informatics and Decision Making. 2013;13(2):S10.
50. Brabers AEM, Rademakers JJDJM, Groenewegen PP, van Dijk L, de Jong JD. What role does health literacy play in patients' involvement in medical decision-making? PLOS ONE. 2017;12(3):e0173316.
51. Muscat DM, Smith J, Mac O, Cadet T, Giguere A, Housten AJ, et al. Addressing Health Literacy in Patient Decision Aids: An Update from the International Patient Decision Aid Standards. Medical Decision Making. 2021;41(7):848-69.
52. Cadoret CA, Garcia RI. Health Disparities and the Multicultural Imperative. Journal of Evidence Based Dental Practice. 2014;14:160-70.e1.
53. Gupta A, Speer ME. Health Literacy and Effective Health Communication in Pediatric Practices and Health Systems: Creating Shame-Free Environments and Patient-Friendly Institutions. In: Connelly RA, Turner T, editors. Health Literacy and Child Health Outcomes: Promoting Effective Health Communication Strategies to Improve Quality of Care. Cham: Springer International Publishing; 2017. p. 51-6.
54. Lee S-YD, Arozullah AM, Cho YI. Health literacy, social support, and health: a research agenda. Social Science & Medicine. 2004;58(7):1309-21.
55. Zarcadoolas C, Pleasant A, Greer DS. Understanding health literacy: an expanded model. Health Promotion International. 2005;20(2):195-203.
56. Speros C. Health literacy: concept analysis. Journal of advanced nursing. 2005;50(6):633-40.
57. Manganello JA. Health literacy and adolescents: a framework and agenda for future research. Health education research. 2008;23(5):840-7.
58. Safari-Moradabadi A, Rakhshanderou S, Ramezankhani A, Ghaffari M. Explaining the concept of oral health literacy: Findings from an exploratory study. Community Dentistry and Oral Epidemiology.n/a(n/a).
59. Amaya-Castellanos MA, Gómez-Acosta LM, Gómez-Humaran IM, Shamah-Levy T. Validation of an Instrument for Measuring Nutrition Literacy in Adolescents. Creative Education. 2021;12(9):2146-58.
60. Williams KP, Templin TN, Hines RD. Answering the Call: A Tool That Measures Functional Breast Cancer Literacy. Journal of Health Communication. 2013;18(11):1310-25.
61. Chiang C, Yang S, Hsu W. Development and validation of the e-health literacy scale and investigation of the relationships between e-health literacy and healthy behavior among undergraduate students in Taiwan. Formosa J Ment Health. 2015;28(3):389-420.
62. Brown SL, Teufel JA, Birch DA. Early adolescents perceptions of health and health literacy. Journal of School Health. 2007;77(1):7-15.
63. Massey PM, Prelip M, Calimlim BM, Quiter ES, Glik DC. Contextualizing an expanded definition of health literacy among adolescents in the health care setting. Health Education Research. 2012;27(6):961-74.
64. Ayre J, Costa DSJ, McCaffery KJ, Nutbeam D, Muscat DM. Validation of an Australian parenting health literacy skills instrument: The parenting plus skills index. Patient Education and Counseling. 2020;103(6):1245-51.
Rahmanian N, Ali SHB, Homayoonfard M, Ali NJ, Rehan M, Sadef Y, et al. Analysis of physiochemical parameters to evaluate the drinking water quality in the State of Perak, Malaysia. J Chem. 2015;2015:716125. [Link] [DOI:10.1155/2015/716125]
Ali H, Akhtar MS. Peoples perception about poor quality of drinking water and its impact on human health in rural areas of tehsil Samundri Pakistan. Int J Sci Res. 2015;4(10):523-8. [Link]
Al-Khatib IA, Eshkair AA, Manasreh NK. Factors affecting water quality in the west bank and Gaza strip of Palestine. DIRASAT. 2008;35(2):131-41. [Arabic] [Link]
Haydar S, Arshad M, Aziz JA. Evaluation of drinking water quality in urban areas of Pakistan: A case study of Southern Lahore. Pak J Engg Appl Sci. 2009;5:16-23. [Link]
Patil PN, Sawant DV, Deshmukh RN. Physico-chemical parameters for testing of water-a review. Int J Environ Sci. 2012;3(3):1194-207. [Link]
Daghara A, Al-Khatib IA, Al-Jabari M. Quality of drinking water from springs in Palestine: West bank as a case study. J Environ Public Health. 2019:8631732. [Link] [DOI:10.1155/2019/8631732]
Jaishankar M, Tseten T, Anbalagan N, Mathew BB, Beeregowda KN. Toxicity, mechanism and health effects of some heavy metals. Interdiscip Toxicol. 2014;7(2):60-7. [Link] [DOI:10.2478/intox-2014-0009]
Hefnawy A, El-Khaiat H. The importance of copper and the effects of its deficiency and toxicity in animal health. Int J Livest Res. 2015;5(12):1-20. [Link] [DOI:10.5455/ijlr.20151213101704]
Tchounwou PB, Yedjou CG, Patlolla AK, Sutton DJ. Heavy metal toxicity and the environment. Exp Suppl. 2012;101:133-64. [Link] [DOI:10.1007/978-3-7643-8340-4_6]
Brochin R, Leone S, Phillips D, Shepard N, Zisa D, Angerio A. The cellular effect of lead poisoning and its clinical picture. GU J Health Sci. 2008;5(2):1-8. [Link]
Papanikolaou NC, Hatzidaki EG, Belivanis S, Tzanakakis GN, Tsatsakis AM. Lead toxicity update (A brief review). Med Sci Monit. 2005;11(10):RA329-36. [Link]
Philip AT, Gerson B. Lead poisoning-part 1: Incidence, etiology, and toxicokinetics. Clin Lab Med. 1994;14(2):423-44. [Link] [DOI:10.1016/S0272-2712(18)30386-X]
Martin S, Griswold W. Human health effects of heavy metals. Environ Sci Technol Brief Citizen. 2009;15:1-6. [Link]
Almahmood HK. Water resources in Basra and its recent problems. Basra: Dar Al-Kutub; 2019. [Link]
American Public Health Association. Standard methods for the examination of water and wastewater. 20th Edition. Washington DC: Amer Public Health Assn; 1999. [Link]
Akter T, Jhohura FT, Akter F, Chowdhury TR, Mistry SK, Dey D, et al. Water quality index for measuring drinking water quality in rural Bangladesh: A cross-sectional study. J Health Popul Nutr. 2016;35(4):1-12. [Link] [DOI:10.1186/s41043-016-0041-5]
Napacho ZA, Manyele SV. Quality assessment of drinking water in Temeke district (Part 2): Characterization of chemical parameters. Afr J Environ Sci Technol. 2010;4(11):775-89. [Link]
Saalidong BM, Aram SA, Otu S, Lartey PO. Examining the dynamics of the relationship between water pH and other water quality parameters in ground and surface water systems. PLoS ONE. 2022;17(1):e0262117. [Link] [DOI:10.1371/journal.pone.0262117]
Gauthier V, Barbeau B, Tremblay G, Millette R, Bernier AN. Impact of raw water turbidity fluctuations on drinking water quality in a distribution system. J Environ Eng Sci. 2003;2(4);281-91. [Link] [DOI:10.1139/s03-026]
Rafiqul Islam M, Islam Sarkar MK, Afrin T, Rahman SS, Islam Talukder R, Kanti Howlader B, et al. A study on the total dissolved solids and hardness level of drinking mineral water in Bangladesh. American J Apple Chemist. 2016;4(5):164-9. [Link] [DOI:10.11648/j.ajac.20160405.11]
Wang D, Shimoda Y, Wang S, Wang Z, Liu J, Liu X, et al. Total arsenic and speciation analysis of saliva and urine samples from individuals living in a chronic arsenicosis area in China. Environ Health Prev Med. 2017;22:45. [Link] [DOI:10.1186/s12199-017-0652-5]
Alidadi H, Tavakoly Sany SB, Zarif Garaati Oftadeh B, Tafaghodi M, Shamszadeh H, Fakhari M. Health risk assessments of arsenic and toxic heavy metal exposure in drinking water in northeast Iran. Environ Health Prev Med. 2019;24(59). [Link] [DOI:10.1186/s12199-019-0812-x]
Sany SBT, Hashim R, Salleh A, Rezai M, Safari O. Ecological quality assessment based on macrobenthic assemblages indices along West Port, Malaysia coast. Environ Earth Sci. 2015;74:1331-41. [Link] [DOI:10.1007/s12665-015-4122-3]
Ahmad N, Jaafar MS, Alsaffar MS. Study of radon concentration and toxic elements in drinking and irrigated water and its implications in Sungai Petani, Kedah, Malaysia. J Radiat Res Appl Sci. 2015;8(3):294-9. [Link] [DOI:10.1016/j.jrras.2015.04.003]
Hashemi M. Sadeghi A, Saghi M, Aminzare M, Raeisi M, Rezayi M, Sany SBT. Health risk assessment for human exposure to trace metals and arsenic via consumption of hen egg collected from the largest poultry industry in Iran. Biol Trace Elem Res. 2019;188(2):485-93. [Link] [DOI:10.1007/s12011-018-1437-4]
World Health Organization. Guidelines for drinking-water quality [Internet]. Geneva: WHO Publications; 2011 [cited 2022 May 15]. Available from: https://www.who.int/publications/i/item/9789241549950 [Link]
Geremew A, Mengistie B, Mellor J, Lantagne DS, Elemayehu E, Sahilu G. Appropriate household water treatment methods in Ethiopia: Household use and associated factors based on 2005, 2011, and 2016 EDHS data. Environ Health Prev Med. 2018;23(1):46. [Link] [DOI:10.1186/s12199-018-0737-9]
Saha N, Safur Rahman M, Boshir Ahmad M, Zhou JL, Hao Ngo H, Geo W. Industrial metal pollution in water and probabilistic assessment of human health risk. J Environ Manag. 2017;185:70-8. [Link] [DOI:10.1016/j.jenvman.2016.10.023]
Davis AD, Webb CJ, Sorensen JL, Dixon DJ, Hudson R. Geochemical thermodynamics of lead removal from water with limestone. Water Air Soil Pollut. 2018;229:177. [Link] [DOI:10.1007/s11270-018-3824-z]
Benfer EA. Contaminated childhood: How the United States failed to prevent the chronic lead poisoning of low-income children and communities of color. Harv Environ Law Rev. 2017;41:493-561. [Link] [DOI:10.2139/ssrn.2823342]
Fawkes L, Sansom G. Preliminary study of lead-contaminated drinking water in public parks-an assessment of equity and exposure risks in two Texas communities. Int J Environ Res Public Health. 2021;18(12):6443. [Link] [DOI:10.3390/ijerph18126443]
Abbood,H , AL-Moziel,M and Ghanim,W . (2025). Water Quality Assessment by Measuring Physio-chemical Properties and Heavy Metals Contents at Water Stations in Basra City, Iraq. Health Education and Health Promotion, 10(1), 129-135.
MLA
Abbood,H , , AL-Moziel,M , and Ghanim,W . "Water Quality Assessment by Measuring Physio-chemical Properties and Heavy Metals Contents at Water Stations in Basra City, Iraq", Health Education and Health Promotion, 10, 1, 2025, 129-135.
HARVARD
Abbood H, AL-Moziel M, Ghanim W. (2025). 'Water Quality Assessment by Measuring Physio-chemical Properties and Heavy Metals Contents at Water Stations in Basra City, Iraq', Health Education and Health Promotion, 10(1), pp. 129-135.
CHICAGO
H Abbood, M AL-Moziel and W Ghanim, "Water Quality Assessment by Measuring Physio-chemical Properties and Heavy Metals Contents at Water Stations in Basra City, Iraq," Health Education and Health Promotion, 10 1 (2025): 129-135,
VANCOUVER
Abbood H, AL-Moziel M, Ghanim W. Water Quality Assessment by Measuring Physio-chemical Properties and Heavy Metals Contents at Water Stations in Basra City, Iraq. Health Education and Health Promotion. 2025;10(1):129-135.