



Volume 11, Issue 1 (2023)
Health Educ Health Promot 2023, 11(1): 147-152 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Suryanti Y, Suryani S, Heryani N, Nasution A. Effect of Integrated Health Education on improving the Knowledge of Pregnant Women to Detect High-risk Pregnancies. Health Educ Health Promot 2023; 11 (1) :147-152
URL: http://hehp.modares.ac.ir/article-5-67654-en.html
URL: http://hehp.modares.ac.ir/article-5-67654-en.html

1- Department of Midwifery, Health Polytechnic of Jambi, Jambi, Indonesia
Keywords: High Risk Pregnancy [MeSH], Pregnant Women [MeSH], Video-Audio Media [MeSH], Brochures [MeSH], Education [MeSH], Knowledge [MeSH]
Full-Text [PDF 3930 kb]
(289 Downloads)
| Abstract (HTML) (618 Views)
Introduction
Findings
Full-Text: (155 Views)
Introduction
High-risk pregnant women are women with a history of previous bad pregnancies and childbirth, height less than 145 cm, low body weight, age less than 20 years or more than 35 years, having three or more children, less spacing of pregnancies, history of anemia or lack of blood, bleeding in pregnancy, blood pressure, fetal position abnormalities and history of chronic disease [1].
A high-risk pregnancy is a deviation from normal conditions that directly cause morbidity and death for the mother and fetus [2, 3]. Early detection of pregnancy with risk factors is an effort to identify pregnant women with risk factors and obstetric complications [1, 4]. Detection of risk factors in the mother, both by health workers and the community, is essential in preventing maternal death and morbidity [5, 6].
In developing countries, maternal mortality and morbidity are still significant health problems [7, 8]. In 2018, World Health Organization (WHO) reported that 830 mothers died from complications of pregnancy and childbirth per day around the world. The Maternal mortality rate in Singapore in 2017 was 8, in Malaysia 29, in Thailand 37, and in Indonesia 305 per 100.000 live births [9, 10]. The maternal mortality rate in Jambi Province in 2020 was 96 per 100,000 live births [11].
The direct causes of maternal death are bleeding (28%), high-risk pregnancy (24%), infection (11%), abortion (5%), and prolonged labor (5%). Bleeding occupies the highest percentage as a cause of maternal death, while anemia and Chronic Energy Deficiency (CED) in pregnant women are the leading causes of bleeding and infection [6, 12, 13].
In 2015, the high-risk pregnancy group in Indonesia was about 34%, which included maternal age over 34 years at 3.8%, birth interval less than 24 months at 5.2%, and number of children over 3 at 9.4% [4]. Complications will tend to increase in pregnant women who have risk factors. It is estimated that 15% of pregnancies will face high-risk conditions and obstetric complications that can be dangerous for the mother and fetus if not treated adequately [14].
Prevention of high-risk pregnancies requires good management of the mother during pregnancy. Pregnant women need to know about detecting high-risk pregnancies because, with early detection, treatment will be immediate. Pregnant women will be better at determining attitudes and behaviors to prevent, avoid or overcome pregnancy risk problems [14, 15].
Every pregnant woman should receive health education about the dangerous signs of pregnancy and be encouraged to immediately seek help from a health worker if she experience one or more of the dangerous signs of pregnancy [1, 2, 5]. Effective health education focuses on efforts to change health behavior based on theory, research, and integrated learning models and materials. Dynamic health education needs to be carried out through various strategies involving a team of health workers, the use of conventional methods, and the use of assistive technology and media [16, 17].
Based on this phenomenon, the present study aimed to investigate the effect of integrated health education on improving the knowledge of pregnant women to detect high-risk pregnancies in Jambi City.
Materials and Methods
Study design
This research is a quasi-experimental study with a pre-test and post-test design.
Participants
This study included 90 pregnant women in the third trimester of pregnancy, referring to the Delima Midwife Clinic in Jambi, Indonesia, from July 2020 to March 2021. These women were randomly selected and divided into three groups of 30 samples. The inclusion criteria consisted of women who had never participated in a study with the same theme and 3rd trimester pregnant women without pregnancy complications. In contrast, pregnant women who did not have an Android cell phone were excluded. Randomization began by collecting data on patients' families who met the inclusion criteria. All prospective respondents randomly chose a number rolled up on paper in the container provided. The researcher then announced that all respondents who got an even number would participate in this study.
Sample size
This study involved 90 participants who were divided into three groups. This figure was obtained from calculations based on the Slovin formula [18]. In detail, the population was 117, and d=0.05, so a sample size of 90 was obtained.
Intervention
The research sample was divided into three groups, 30 participants received the Maternal and Child Health (MCH) Handbook method, 30 others received videos, and 30 others received brochures. The authors developed the videos and brochures independently, while the MCH book was taken from the Delima Midwife Clinic.
The MCH Handbook education group was divided into three small groups of 10 people each and received explanations from research members regarding detecting high-risk pregnancies. The video education group was gathered in a room and then given a video containing descriptions of seeing high-risk pregnancies. Then in the brochure education group, brochures were also collected in a room and then explained detecting high-risk pregnancies.
Before administering the intervention, the researcher distributed the questionnaires consisting of 15 questions about the knowledge of detecting high-risk pregnancies. It then continued providing educational interventions to pregnant women. Each session lasted for 1 hour with a distribution of 45 minutes of material giving and the next 15 minutes of discussion. After the discussion session, 15 minutes later, a post-test was carried out, namely distributing the knowledge questionnaire again to be filled out by pregnant women.
Instrument
Before and after the intervention, participants' knowledge was assessed using a questionnaire consisting of 15 questions with true and false choices based on the Guttman scale. The score for a "True" answer was 1, and the score for a "false" answer was 0. The knowledge variable was divided into two categories: if the scores were 0-8 (≤60%), the respondent's knowledge was poor, and if the scores were 9-15 (60-100%), the respondent's knowledge was good. The author developed the questionnaire based on the author's experience in several health studies and the preparation of numerous questionnaires. An instrumented test was carried out to maintain the quality of the research instrument. If the coefficient between items and total items equals or exceeds 0.3, then the item is declared valid. Still, if the correlation value is below 0.3, the item is declared invalid and must be corrected. If the correlation is 0.7, then the object is said to provide sufficient reliability. Conversely, if the correlation value is below 0.7, then the item is said to be less reliable. To find the coefficient value, the researcher used the Pearson product-moment test [19, 20].
This questionnaire was tried on ten mothers with the result that there were two invalid questions or r<0.3 and had to be revised while the "Cronbach Alpha" value of all questionnaires was >0.7 so that it was declared reliable.
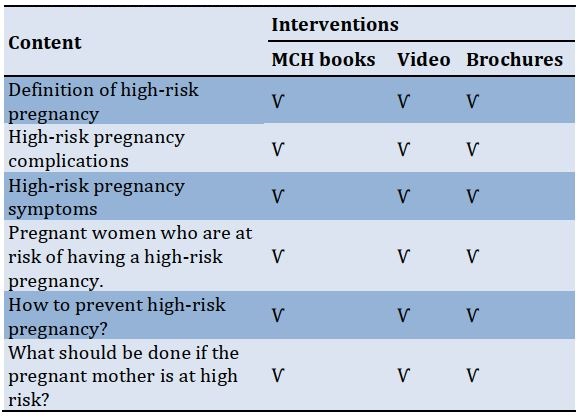
Intervention content
The content of the educational intervention used in the study is presented in Table 1.
Table 1) Research intervention content matrix
Outcomes
This study compared the results of educational methods using MCH books, videos, and brochures on mothers' knowledge in detecting high-risk pregnancies.
Statistical analysis
Data were presented as numbers and percentages for categorical variables. Continuous data were expressed as mean ± Standard Deviation (SD) or median with Interquartile Range (IQR). The Kolmogorov-Smirnov test was used to examine the distribution of research data. Then the Wilcoxon test was used to determine the effect of the MCH books, videos, and brochures interventions on knowledge. Moderated regression analysis was used to determine the influence of moderating variables in strengthening or weakening the relationship between the independent and dependent variables. All tests with p<0.05 were considered significant. Statistical analysis was performed using SPSS 16.0 software.
Findings
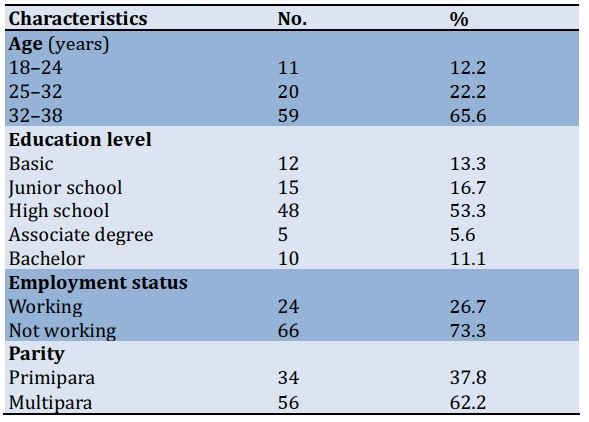
Most of the respondents were aged 32-38 years (65.6%). Most of the respondents' education had a high school degree (53.3%). 73.3% did not work, and 62.2% of women were multipara (Table 2).
Table 2) Frequency distribution of pregnant women’s characteristics (n=90)
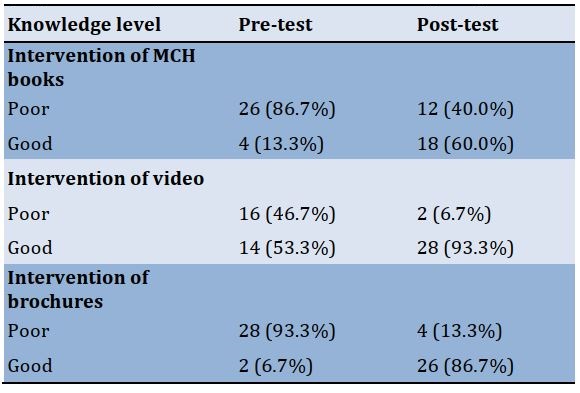
Most of the respondents' knowledge before the intervention of MCH books was in the Poor category (86.7%). After the intervention, the knowledge of pregnant women was mainly in the Good category (60%). Before the video intervention, most of the respondents' knowledge was poor (46.7%); after the intervention, it was in the Good category (93.3%). Likewise, before the brochure intervention, most of the respondents had poor knowledge (93.3%), and after the intervention, most of them (86.7%) had good knowledge (Table 3).
Table 3) Frequency distribution of the knowledge levels in pregnant women, before and after interventions (n=90)
The distribution of the data was normal in the pre-test, but in the post-test, the data did not have a normal distribution (Table 4).
After the implementation of the interventions, the mean score of knowledge increased significantly compared to before the interventions (p<0.001; Table 5).
Table 4) Normality test results of knowledge, in pre-test and posttest

Table 5) Comparing the mean score of knowledge in pregnant women before and after the intervention

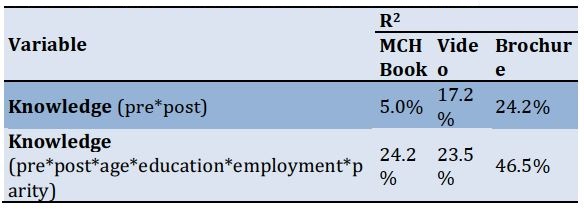
In the MCH book group, R2 between pre and post knowledge was 5%, which after adding moderate variables (age, education, employment, and parity), increased to 24.2%, meaning that these variables are moderators and strengthened the effect of the intervention on increasing knowledge. In the video group, there was also an increase in knowledge after adding moderator variables from 17.2% to 23.5%. In the brochure group, there was also an increase in knowledge after adding moderator variables from 24.2% to 46.5% (Table 6).
Table 6) The results of moderated regression analysis
Discussion
A high-risk pregnancy is a pregnancy with a greater risk than usual (both for the mother and the baby), which can result in illness or death before or after delivery [2, 4]. Early pregnancy detection can be used to prevent high-risk pregnancies for pregnant women [21, 22]. This study aims to analyze the effect of providing integrated health education in increasing the knowledge of pregnant women to detect high-risk pregnancies.
The current study found that before the intervention of health education through MCH books, videos, and brochures, most respondents had insufficient knowledge about high-risk pregnancies, including the spacing of pregnancies, related factors, seeking helpers, and causes of events.
The level of education may influence one's knowledge and mindset to accept and understand problems, especially during pregnancy [13]. The level of education affects the opportunity to obtain and receive health information. Respondents with a higher education level are expected to receive and understand the information conveyed by health workers [23]. The situation is different for people with low levels of education, where there is a tendency for them not to understand the information that health workers have conveyed. In this study, most respondents were in the category of low education (elementary-high school).
After the health education intervention through the MCH Handbook, videos, and brochures, the knowledge of pregnant women increased. However, some respondents still did not know about high-risk pregnancies.
There was a significant difference in the level of knowledge of pregnant women before and after the intervention of the MCH Handbook, videos, and brochures (p<0.001). These findings reinforce Jamil and Sari research [24], which states that there is a significant relationship between knowledge about high-risk pregnancies and regular prenatal care. The better the knowledge of pregnant women about high-risk pregnancies, the more routine pregnant women will have their pregnancies checked. In line with Yuni et al. research [25], the group who received counseling using flipchart media experienced an increase in attitude by 91.66%, while in the group who received counseling using VCD (Video Compact Disk) playback media, all respondents (100%) experienced an increase.
This finding reinforces Sihombing et al. research [26], which reports an increase in pregnant women's knowledge about high-risk pregnancies from 52% to 63.6%. It is possible because this study was conducted with counseling using PowerPoint visual media, debriefing with doctors and experts, and distributing brochures containing high-risk pregnancies and their prevention.
Media and props are essential in conveying messages in providing information. The counseling target will absorb less information when the target only listens to the speaker's presentation. Conversely, when the target sees and hears the material presented, she will get more information [27].
Health education using audio-visual media is starting to be used frequently. It is considered more effective in conveying messages because it can provide a more authentic experience than what is conveyed compared to health education using lecture media and still conventional discussions. Audio-visual media can stimulate the senses of hearing and sight, so that the results obtained are maximized [28]. Audio-visual media is the most accessible media for the audience to understand because it contains interesting elements, both in terms of shooting and editing [29].
The impact of lack of knowledge of pregnant women about the dangers of high-risk pregnancies is one of the reasons for the still high maternal mortality rate. It is in line with research by D'Antonio et al. [30], which states that if pregnant women have low knowledge about high-risk pregnancy factors, they will not change their attitude and behavior. Giving interventions through video media with exciting animations and several concepts to be conveyed made respondents more quickly grasp the information provided [15].
In line with research conducted by Syahda [31], if a pregnant woman has more knowledge about high-risk pregnancy, she will likely think about determining attitudes and behaviors to prevent, avoid or overcome the problem of the risk of pregnancy.
There are several limitations to this study. First, the evaluation of knowledge is only carried out once immediately after the intervention is given. In contrast, it might be better if this evaluation is repeated a few weeks or months after the intervention. Second, validation was not carried out on the MCH book used in the intervention, where the content in the book may have needed to meet the standards adapted to the conditions of the local community.
Conclusion
MCH books, video media, and brochures effectively increase pregnant women's knowledge to detect high-risk pregnancies. Health workers can implement this method of health education on detecting high-risk pregnancies using the MCH Handbook, video media, and brochures to support the success of programs designed for pregnant women.
Acknowledgements: We would like to express our gratitude to the head of the Delima clinic for their cooperation in carrying out this research intervention.
Ethical Permission: No economic incentives were offered or provided for participation in this study. The study was performed in accordance with the ethical considerations of the Helsinki Declaration. This study obtained ethical feasibility under the Health Research Ethics Commission of the Ministry of Health, Jambi, and registration number: LB.02.06/2/225/2020.
Conflict of Interests: There is no conflict of interest for this study.
Authors’ Contribution:
Suryanti Y (First Author), Introduction Writer/Main Researcher/Discussion Writer (45%); Suryani S (Second Author), Methodologist/Discussion Writer (30%); Heryani N (Third Author), Statistical Analyst/Discussion Writer (15%); Nasution AFD (Fourth Author), Introduction Writer/Statistical Analyst (10%)
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Article Type: Original Research |
Subject:
Technology of Health Education
Received: 2022/12/24 | Accepted: 2023/03/8 | Published: 2023/03/19
Received: 2022/12/24 | Accepted: 2023/03/8 | Published: 2023/03/19
References
1. Nuraisya W. Deteksi Risiko Tinggi Kehamilan Pada Pelayanan ANC Terpadu di Puskesmas Bendo Kabupaten Kediri. Jurnal Kesehatan Andalas. 2018;7(2):240-5. [Indonesian] [Link] [DOI:10.25077/jka.v7i2.808]
2. Gilbert ES. Manual of high risk pregnancy and delivery. 5th Edition. St. Louis, MO: Elsevier Health Sciences; 2010. [Link]
3. Fourianalistyawati E, Caninsti R. Kualitas hidup pada ibu dengan kehamilan risiko tinggi. In: Konferensi Nasional II Psikologi Kesehatan Universitas YARSI. Jakarta: Universitas YARSI: 2014. [Indonesian] [Link]
4. Yuniarti F, Ratnawati L, Ivantarina D. Deteksi Dini Kehamilan Risiko Tinggi Melalui Edukasi dan Skrining Pada Ibu Hamil di Masa Pandemi Covid-19. Jurnal Pengabdian kepada Masyarakat Nusantara. 2022;3(1):89-101. [Indonesian] [Link] [DOI:10.55338/jpkmn.v3i1.290]
5. Purwanti IA, Indrawati ND, Adhiatma AT. Penyuluhan tentang Kehamilan Risiko Tinggi. Jurnal Pengabdian Kesehatan. 2018;1(2):1-5. [Indonesian] [Link] [DOI:10.31596/jpk.v1i2.11]
6. Hitatami E, Lestari B, Hilmanto D, Judistiani T, Sunjaya D, Wirakusumah F. Pengaruh Pendidikan Kesehatan tentang Kehamilan Risiko Tinggi melalui Layanan Pesan Singkat terhadap Peningkatan Pengetahuan dan Sikap Ibu Hamil. Jurnal Pendidikan dan Pelayanan Kebidanan Indonesia. 2014;1(1):48-55. [Indonesian] [Link] [DOI:10.24198/ijemc.v1i1.82]
7. Villar J, Farnot U, Barros F, Victora C, Langer A, Belizan JM. A randomized trial of psychosocial support during high-risk pregnancies. N Engl J Med. 1992;327(18):1266-71. [Link] [DOI:10.1056/NEJM199210293271803]
8. Stark MA, Brinkley RL. The relationship between perceived stress and health-promoting behaviors in high-risk pregnancy. J Perinat Neonatal Nurs. 2007;21(4):307-14. [Link] [DOI:10.1097/01.JPN.0000299788.01420.6e]
9. Takemoto MLS, Menezes MO, Andreucci CB, Knobel R, Sousa LAR, Katz L, et al. Maternal mortality and COVID-19. J Matern Fetal Neonatal Med. 2022;35(12):2355-61. [Link] [DOI:10.1080/14767058.2020.1786056]
10. Ozimek JA, Kilpatrick SJ. Maternal mortality in the twenty-first century. Obstet Gynecol Clin North Am. 2018;45(2):175-86. [Link] [DOI:10.1016/j.ogc.2018.01.004]
11. Dinas Kesehatan Provinsi Jambi. Profil Kesehatan Provinsi Jambi Tahun [Internet]. Jambi: Dinas Kesehatan Provinsi Jambi; 2020 [cited 2022 Dec 12]. Available from: https://dinkes.jambiprov.go.id/file/informasi_publik/MTY0MTIyOTA3NA_Wkt1641229074_XtLnBkZg.pdf [Indonesian] [Link]
12. Nursal DGA. Kehamilan Risiko Tinggi Di Puskesmas Lubuk Gadang Kabupaten Solok Selatan. Jurnal Kesehatan Masyarakat Andalas. 2014;9(1):23-8. [Indonesian] [Link] [DOI:10.24893/jkma.v9i1.414]
13. Corneles SM, Losu FN. Hubungan tingkat pendidikan dengan pengetahuan ibu hamil tentang kehamilan risiko tinggi. Jurnal Ilmiah Bidan. 2015;3(2):51-5. [Indonesian] [Link]
14. Jeihooni AK, Jamshidi H, Kashfi SM, Avand A, Khiyali Z. The effect of health education program based on health belief model on oral health behaviors in pregnant women of Fasa City, Fars Province, South of Iran. J Int Soc Prev Community Dent. 2017;7(6):336-43. [Link] [DOI:10.4103/jispcd.JISPCD_339_17]
15. Belizán J, Barros F, Langer A, Farnot U, Victora C, Villar J. Impact of health education during pregnancy on behavior and utilization of health resources. Am J Obstet Gynecol. 1995;173(3 Pt 1):894-9. [Link] [DOI:10.1016/0002-9378(95)90362-3]
16. Mawaddah F, Widiyastuti D. The effect of health education on pregnant women's knowledge level about Covid-19 in main clinic Cideng medical center regency of Cirebon in 2020. Int Semin Gender Equity Matern Child Health. 2021;(11):61-79. [Link] [DOI:10.34305/gemic.v1i1.314]
17. Kamau M, Mirie W, Kimani S, Mugoya I. Effect of community based health education on knowledge and attitude towards iron and folic acid supplementation among pregnant women in Kiambu County, Kenya: A quasi experimental study. PloS One. 2019;14(11):e0224361. [Link] [DOI:10.1371/journal.pone.0224361]
18. Candra V, Simarmata NIP, Mahyuddin M, Purba B, Purba S, Chaerul M, et al. Pengantar Metodologi Penelitian. Yayasan Kita Menulis; 2021. [Indonesian] [Link]
19. Brink Y, Louw QA. Clinical instruments: reliability and validity critical appraisal. J Eval Clin Pract. 2012;18(6):1126-32. [Link] [DOI:10.1111/j.1365-2753.2011.01707.x]
20. Salmond SS. Evaluating the reliability and validity of measurement instruments. Orthop Nurs. 2008;27(1):28-30. [Link] [DOI:10.1097/01.NOR.0000310608.00743.54]
21. Browner CH, Preloran M, Press NA. The effects of ethnicity, education and an informational video on pregnant women's knowledge and decisions about a prenatal diagnostic screening test. Patient Educ Couns. 1996;27(2):135-46. [Link] [DOI:10.1016/0738-3991(95)00796-2]
22. Whitworth M, Dowswell T. Routine pre‐pregnancy health promotion for improving pregnancy outcomes. Cochrane Database Syst Rev. 2009;(4):CD007536.. [Link] [DOI:10.1002/14651858.CD007536]
23. Rangkuti NA, Harahap MA. Hubungan pengetahuan dan usia ibu hamil dengan kehamilan risiko tinggi di puskesmas labuhan rasoki. J Educ Dev. 2020;8(4):513. [Indonesian] [Link]
24. Jamil M, Sari CK. Hubungan Pengetahuan dengan Keteraturan Antenatal Care (ANC) Pada Ibu Hamil di Karangsari Agung Boyo Karangtengah Demak. In: Prosiding Seminar Nasional Widya Husada. 2019. [Indonesian] [Link]
25. Yuni MS, Ruwayda R, Herinawati H. Efektifitas Lembar Balik dan Video Animasi Terhadap Pengetahuan Primigravida tentang Persiapan Persalinan. Jurnal Kesehatan Komunitas. 2021;7(3):288-95. [Indonesian] [Link] [DOI:10.25311/keskom.Vol7.Iss3.1039]
26. Sihombing R, Ahmad N, Sagita DK. Epidemiologi Faktor-Faktor Yang Mempengaruhi Kejadian Kehamilan Risiko Tinggi di Puskesmas Padasukan Cimahi. Prosiding Pertemuan Ilmiah Nasional Penelitian dan Pengabdian Masyarakat I (PINLITAMAS 1). 2018;1(1):348-52. [Indonesian] [Link]
27. HD SR. Efektifitas pendidikan kesehatan tentang kehamilan resiko tinggi terhadap pengetahuan ibu hamil. Jurnal Online Mahasiswa (JOM) Bidang Ilmu Keperawatan. 2014;1(2):1-8. [Indonesian] [Link]
28. Yakti L, Christin Hiyana TD, Widatiningsih S, Mid M. Efektivitas Pendidikan Kesehatan Dengan Media Video Terhadap Pengetahuan Ibu Hamil Tentang Kehamilan Risiko Tinggi. DIV Kebidanan Magelang. 2021. [Indonesian] [Link]
29. Prabandari AW, Hastuti S, Widyastuti Y. Pengaruh pemberian penyuluhan dengan media video dan booklet terhadap tingkat pengetahuan kesehatan reproduksi remaja di SMK 2 Muhammadiyah Bantul [Dissertation]. Poltekkes Kemenkes Yogyakarta; 2018. [Indonesian] [Link]
30. D'Antonio F, Sen C, Di Mascio D, Galindo A, Villalain C, Herraiz I, et al. Maternal and perinatal outcomes in high compared to low risk pregnancies complicated by severe acute respiratory syndrome coronavirus 2 infection (phase 2): the World Association of Perinatal Medicine working group on coronavirus disease 2019. Ame J Obstet Gynecol MFM. 2021;3(4):100329. [Link] [DOI:10.1016/j.ajogmf.2021.100329]
31. Syahda S. Hubungan Pengetahuan Dan Sikap Ibu Hamiltentang Risiko Tinggi Dalam Kehamilan Dengan Kejadian Risiko Tinggi Dalam Kehamilan Diwilayah Kerja Puskesmas Kampar. Jurnal Doppler. 2018;2(2):1-8. [Indonesian] [Link]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |