



Volume 11, Issue 1 (2023)
Health Educ Health Promot 2023, 11(1): 95-109 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bagheri M, Somi M, Dehghani G, Ghaffarifar S. Determinants of Patient-centered Communication Based on the Views of Physicians, Students, and Patients: A Qualitative Study. Health Educ Health Promot 2023; 11 (1) :95-109
URL: http://hehp.modares.ac.ir/article-5-65420-en.html
URL: http://hehp.modares.ac.ir/article-5-65420-en.html

1- “Medical Education Research Center” and “Health Management and Safety Promotion Research Institute”, Tabriz University of Medical Sciences, Tabriz, Iran
2- Liver and Gastrointestinal Diseases Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
3- “Research Center for Evidence-Based Medicine” and “Health Management and Safety Promotion Research Institute”, Tabriz University of Medical Sciences, Tabriz, Iran
2- Liver and Gastrointestinal Diseases Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
3- “Research Center for Evidence-Based Medicine” and “Health Management and Safety Promotion Research Institute”, Tabriz University of Medical Sciences, Tabriz, Iran
Keywords: Physician-Patient Relations [MeSH], Patient-Centered Care [MeSH], Qualitative Research [MeSH], Medicine [MeSH]
Full-Text [PDF 1845 kb]
(255 Downloads)
| Abstract (HTML) (584 Views)
Full-Text: (136 Views)
Introduction
For many years, establishing an effective Physician-Patient Relationship (PPR) has been a vital component of successful health care [1], and integration of the patient’s perceptions with a biomedical perspective has been considered suitable for the 21st century [2]. In this regard, the doctor-patient communication model has reformed from paternalism and biomedical style to individualism and Patient-Centered Communication (PCC) [3].
In PCC, medical doctors discover and unite patients’ wants, feelings, illness beliefs, concerns, preferences, and expectations [4]. Today, it is accepted that PCC is the cornerstone of clinical and medical education at all levels and areas of medical sciences [5], and many favorable health outcomes have been attributed to it [6].
Despite the informed benefits of PCC, problems in the implementation of the PCC have been reported, and it has been employed in about 45%–62% of visits [7]. The variation in reported rates of PCC implementation can be related to different attributes of patients and the health system, diverse patterns of interaction, and various perspectives in defining PCC [7]. Although PCC has been one of the preferred models for patient care [8], evidence for the influence of PCC on medical consequences has been diverse, and some interventions to develop PCC amongst medical doctors have failed to increase medical outcomes and patient satisfaction [4]. PCC has not been common practice all the time [3], and different barriers to PCC have been reported [9-11]. Similarly, despite the global emphasis on improving physicians’ clinical communication skills, opportunities have not been fully provided for communication skills training [12]. Communication skills training has not achieved its true official position at most universities of medical sciences [13]. In some cases, efforts have failed to revise the curricula and implement communication skills programs [14]. That is why maximum optimal therapeutic results and health outcomes have not been achieved, and 70% of patients' complaints are still related to the poor communication skills of physicians [15].
Several studies have been done in different settings to assess PCC and identify its barriers. In some institutions, quantitative and qualitative research approaches are combined [12]. In Indonesia, a conflict between ideal and reality has been reported regarding PPR, and additional studies have been recommended to study ways to modify the prevailing communication style into a preferred method [10]. In China, physicians’ communication skills have been surveyed, and further examination of the effectiveness of physicians' communication skills based on examining the perspectives of both patients and physicians and receiving feedback from them has been recommended [16].
The state of PPR has been analyzed in many Iranian studies. The findings of a qualitative inquiry study revealed that the physician-patient communication style in Iran is perceived as considerably physician-oriented. Integrating communication skills into medical curricula in Iran with due consideration to religious issues and ethnical and cultural concerns was recommended as a real educational need for the Iranian society [17]. Since then, given the encouraging effects of PCC and the mentioned recommendations, in many medical schools in Iran [18], medical students have been taught to apply and master communication skills in practice.
Communication barriers have been investigated in a study at the capital of Iran [9]. In Tabriz University of Medical Sciences (TUOMS), where most of the patients in the northwest of Iran receive the required medical services in teaching hospitals affiliated to it, based on the results of the assessment of communication skills of 198 medical residents by 488 patients in 2016 in the largest teaching and academic center in the northwest of Iran, the patients’ satisfaction with participating residents’ communication skills was not acceptable (the mean of the patients’ normalized total satisfaction score was 48.8±18 out of 100) [19]. However, the reasons for patients' dissatisfaction with physicians' communication skills in our institution had not been previously investigated.
It is necessary to pay attention to several important points: 1) The concerns around effective patient-physician communication and providing training related to PCC vary across societies depending on the educational context, norms, beliefs, cultures, and governing social relations; 2) A deeper understanding about the strengths, weaknesses, opportunities, and challenges in every educational context can be provided by conducting a qualitative study; 3) As qualitative research has a contextual nature, the possible transferability of its results to other sociocultural situations should be carefully and cautiously considered [20]; and 4) Up to the time of the present study, no qualitative study has been conducted to explore the perceptions of faculty members, medical students and patients about PCC at TUOMS. Hence, we intended to analyze the status of patient-physician relationships at TUOMS and explore the tips for improving PPR and PCC from the viewpoint of faculty members, students (medical residents and interns), and patients through a qualitative content analysis study.
The results of the present study can be utilized in revising curricula, setting educational priorities, and planning for proper educational interventions. Another important point about this study is that in the current study, alongside the perspectives of patients and physicians, the perspectives of medical interns and residents have also been explored. Based on this part of the study findings, some research hypotheses can be proposed to compare the physicians’ communication skills during the education with a post-graduation period.
Participants and Methods
Study design
In this qualitative content analysis study, the meanings from qualitative data were uncovered and organized to deeply explore the perspectives of patients and physicians, medical interns and residents regarding patient- physician relationship and infer the tips for improving PPR and PCC at teaching hospitals affiliated to Tabriz University of Medical Sciences, Tabriz, Iran. In this research, an in-depth description of performances and perspectives of participants and their behavior patterns within their actual context was provided by interviewing them, observing their behavior and gathering some relevant items. Data were gathered through face-to-face interviews, group discussions, and field observations, and conclusions were drawn through a thematic and manifest summative analysis [21, 22].
Researchers’ characteristics and roles
The interviewer researcher (MB), who was a medical doctor familiar with the study context, studying for a master's degree in Medical Education at the time of this research, always tried to be an active listener. He adopted an open and emotionally neutral body language, looked interested, smiled, employed encouraging body language whenever necessary, and avoided leading questions. He just moderated and facilitated the Focus Group Discussions (FGDs). Group dynamics in FGDs were observed by a second researcher (SGH) to enhance the analysis of interactions, whether verbally or non-verbally. SGH was an MD, Ph.D. She was an MSc graduate in Medical Education and a Ph.D. graduate in Health Education and Health Promotion. At the time of this research, she was a faculty member at the Medical Education group of the Tabriz University of Medical Sciences. Both MB and SGH had attended qualitative studies courses and workshops during their medical/health education studies. Research on communication skills was one of SGH's research interests. SGH had previously participated in qualitative studies as a supervisor or advisor and had published qualitative articles in the PPR field.
At the beginning of the research, bracketing was performed, and the researchers wrote down all their assumptions, perspectives, and hypotheses about the subject and put them aside so that they would not influence data collection and interpretation. Reflexivity was fully handled throughout both data collection and data analysis. Reflexivity journals were prepared by MB and SGH and were checked by peers to share their experiences and perspectives. There was no previous relationship between the researchers and the participants, except for the point that both researchers were working in the same university as the participating faculty members, residents and interns.
In addition to harness personal reflexivity by reflexive writing about participants' explanations and researcher's views, memos and constantly appraising their subjectivity declaration, collaborative reflexivity was ensured by team reflexive dialogue in order to question each other’s perspective, assumption and decisions throughout all the research. The research team made their best to understand the impacts of their presence in the field, either positive or negative, on the context.
Study context
This study was conducted in 2018 at Tabriz University of Medical Sciences (TUOMS). TUOMS is located in the northwest of Iran, and its affiliated hospitals, as referral hospitals, provide diagnostic and treatment services to patients from all cities and villages in the region. In the teaching hospitals affiliated to TUOMS, as the largest and most equipped hospitals in northwestern Iran, patients from different cities in the northwestern region of the country with different ethnicities, such as Fars, Turks, Kurds and sometimes Lors or Arabs are admitted.
At the time of the present study, there was no formal communication skills’ training for medical interns and residents at TUOMS. Most of the communication skills training at TUOMS were limited to vicarious learning (observing the communication behavior of faculty members in the wards and clinics). Residents also had an opportunity to attend a one-day educational workshop, which was held at the beginning of their first year of study.
Participants and sampling strategy
Participants in this study were patients, faculty members, medical interns and residents, who were selected, based on their interest and willingness to express their experiences in PCC, as key informants. Considering the informational needs, no criteria were established to determine the number of informants and field observations. Data collection was continued until data and theme saturation. Participants were selected based on purposive sampling. Indeed, through a non-probability sampling technique, participants who had the desired characteristics were invited to participate. No one refused the researchers' invitation to participate in the study. Criteria for participation in the study were: the inclination to participate and lack of any clinical condition or illness that may disrupt the interview process between the researcher and the participant. Vulnerable groups such as patients with impaired consciousness, the elderly, pregnant women, and children were excluded from participating.
The main researcher (MB) introduced himself and the second researcher (SGH). He stated the objectives of the research and invited potential participants. MB started interviewing patients, faculty members, and medical students in clinical settings (in-patient or out-patient) at teaching hospitals affiliated with TUOMS. He simultaneously observed patient-physician interactions in those settings. Maximum variation of sampling [23], in terms of participants’ gender or their working/presence setting at the time of the study, was used to warrant a broad range of participants’ perceptions and experiences. Negative case sampling was also considered to explain inconsistent and unexpected responses in the data analysis process [21, 24].
Data collection
Data collection methods included in-depth open Face to Face (F2F) individual narrative semi-structured interviews, focus group discussions, and field observations. By doing so, method triangulation [25] was employed to ensure credibility in data collection.
The initial interview guide, including the steps of starting, directing and ending the interview, key interview questions, strategies to probe the answers of the participants, the ways to change the questions after the transcription, and analysis of the text of the previous interviews, was prepared by the research team. The interview guideline was piloted on three participants to ensure clarity of questions, and it was developed further throughout the interview process.
A total of 31 participants were interviewed. No one refused to continue participation, and each interview lasted 40-60 minutes. When possible, the interviews were conducted at participants’ preferred time and place, at clinics, wards or inpatient rooms, after prior coordination and without the presence of a third person.
F2F individual interviews were started with an open-ended question such as “Can you tell me your story about patient-physician relationships you have experienced?” After that, probing and progression upon the participants’ initial responses were done. The flexibility of semi-structured interviews made it possible for the interviewer researcher to discover or elaborate the important information to participants. During the interview, participants were encouraged to express their experiences easily, freely and in full detail. Based on the participants’ permission, the content of the interviews was audio- recorded and transcribed. No repeat interview was carried-out.
To make a rich understanding of participants' collective views and to obtain common contextual information about PCC, five 90–120-minute FGDs were held with 8-12 participants in each group. Group discussion sessions were held after individual F2F interviews. Participants of the group discussion sessions were different from the participants of the individual interviews. The purpose of holding FGDs was a deeper exploration of the participants' perceptions and understandings, a better explanation of the sociocultural factors, and beliefs and meanings which affect the participants’ approaches and behaviors [26].
The composition of the groups was homogenous in terms of the participants’ backgrounds. MB moderated the discussions and facilitated the group dynamics to better understand some specific data gathered through F2F interviews. SGH took notes of participants’ non-verbal communications and interactions.
The composition of the groups was homogenous in terms of the participants’ backgrounds. MB moderated the discussions and facilitated the group dynamics to better understand some specific data gathered through F2F interviews. SGH took notes of participants’ non-verbal communications and interactions.
To have a deeper understanding of the influencing conditions and also to confirm the obtained data about PCC, participants’ actions and contextual realities were observed by MB in inpatient wards during twenty-one sessions. The duration of the sessions varied between 15 and 90 minutes, depending on the patient or ward conditions. Field notes were fully transcribed, and they were checked with the previously transcribed data.
Data collection was continued until data and themes saturation. Saturation was recognized when researchers were confident that no redundant code or categories emerged from the data and the emergent categories matched all the data.
Data analysis
The data from each interview, FGD or field observation was transcribed and coded for analysis immediately after it was collected (before conducting the next interview, FGD or observation). No software was used to manage the data. Analyzing transcripts were done through a thematic and manifest summative analysis [21, 22].
MB and SGH read the transcripts of F2F interviews many times until complete understanding was achieved. They (MB and SGH) separately coded the data and compared various codes based on similarities and differences (constant comparison) in order to make sure that all perspectives were presented by thematic analysis. They discussed emerging codes and categories and resolved disagreements until an optimal level of inter-rater agreement was realized.
Data analysis was performed in four stages:
Stage 1) Decontextualization: Through an open coding process, 119 meaning units or codes were identified. The codes were generated deductively based on the PCC conceptual framework. It was performed repeatedly by two different coders. No computer-program was used to speed up the coding process.
Stage 2) Recontextualization: Unimportant data that did not match the study objective were left out.
Stage 3) Categorization: To categorize the data, the number of words in each meaning unit was condensed without losing its content. To do so, the sense of the data was extracted, and the coded material was divided into subcategories under the previously established categories of the PCC conceptual framework.
Stage 4) Compilation: As a manifest analysis, the research team worked through each identified category, not themes. It means that they often used participants’ words, and they gradually referred back to the original words in the transcripts and stayed closer to the meanings. The research team went back to the participants and presented the extracted data in order to attain their agreement (Member check). A peer was asked to read the transcripts and the meaning units and then critic whether they were sensible or not.
PCC in different settings has been defined with different perspectives, including patient, the economic public policy perspective, and clinical practice perspective. The conceptual framework for the analysis of the research findings in the present study has been organized and reflected based on the definition of the Institute for Patient- and Family-Centered Care [27]. This definition is one of the most complete definitions available, which comprehensively defines PCC with a combination of the above four approaches. The core concepts of the Patient-Centered Communication framework include 1) Respect and dignity, 2) Information sharing, 3) Participation, and 4) Collaboration [7].
Respect and dignity refer to listening to patients and their families, honoring their knowledge, choices, feelings, and beliefs, and incorporating their values, perspectives, and cultural backgrounds into the planning and care processes by healthcare providers [7].
Information sharing refers to sharing timely, useful, supporting, unprejudiced, accurate, and complete information with patients and their families to provide them with opportunities to participate in decision-making and care processes [7].
Participation refers to encouraging and supporting the patients and their families in participating in decision-making and care processes as much as they are interested [7].
Collaboration refers to collaborating with patients, their families, healthcare providers, and leaders in policy and program development, implementation, evaluation, facility design, professional education, and research, as well as the delivery of care [7].
A copy of the primary analysis was sent to participants to validate the emergent codes within the categories and subcategories. It was asked for their comments to achieve their agreement on the correctness of interpretations (member checks). Memos were used to track changes in the coding and recoding processes.
A deductive approach was applied to analyze the content of FGDs to support the predetermined coding structure. Where there was no consensus about some factors influencing the PCC, the data was supplemented with observational ones. A similar deductive approach was used to analyze the field notes of the observer researcher (MB).
Standards for methodological rigor
Standards for methodological rigor were enhanced through different strategies. The credibility of the data was enhanced by data triangulation, member checks, verbatim or direct quotations, and negative case sampling. Data trustworthiness was improved by inter-rater and intra-rater agreements. Transferability was enhanced by maximum variation sampling, rich and thick description of the participant’s perceptions and experiences, description limitations, and detailed description of methods [28].
All methods were performed in accordance with the relevant guidelines, regulations, and ethical standards of the responsible committee approving the research at Tabriz University of Medical Sciences and with the Declaration of Helsinki, as revised in 2000.
Findings
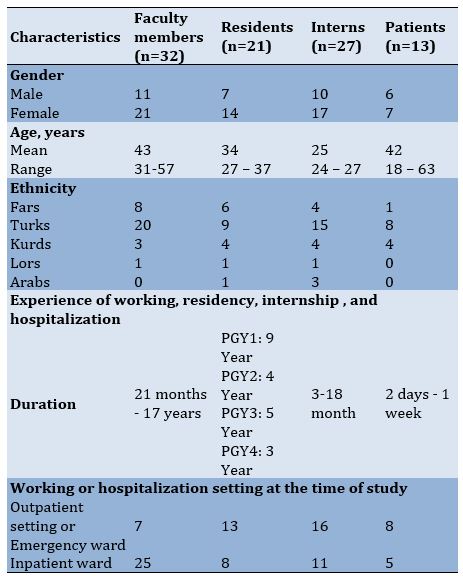
Data saturation was achieved after 31 F2F interviews (13 patients, 6 faculty members, 7 interns, and 5 residents), 9 FGDs with faculty members, interns, and residents (three FGDs in each group), and 21 sessions of field observation. Participants consisted of 13 patients (13 in F2F interviews), 32 faculty members (6 in F2F interviews and 26 in FGDs), 27 medical interns (7 in F2F interviews and 20 in FGDs), and 21 residents (5 in F2F interviews and 16 in FGDs). Participants’ baseline characteristics are revealed in Table 1.
Table 1) Baseline characteristics of study participants
For many years, establishing an effective Physician-Patient Relationship (PPR) has been a vital component of successful health care [1], and integration of the patient’s perceptions with a biomedical perspective has been considered suitable for the 21st century [2]. In this regard, the doctor-patient communication model has reformed from paternalism and biomedical style to individualism and Patient-Centered Communication (PCC) [3].
In PCC, medical doctors discover and unite patients’ wants, feelings, illness beliefs, concerns, preferences, and expectations [4]. Today, it is accepted that PCC is the cornerstone of clinical and medical education at all levels and areas of medical sciences [5], and many favorable health outcomes have been attributed to it [6].
Despite the informed benefits of PCC, problems in the implementation of the PCC have been reported, and it has been employed in about 45%–62% of visits [7]. The variation in reported rates of PCC implementation can be related to different attributes of patients and the health system, diverse patterns of interaction, and various perspectives in defining PCC [7]. Although PCC has been one of the preferred models for patient care [8], evidence for the influence of PCC on medical consequences has been diverse, and some interventions to develop PCC amongst medical doctors have failed to increase medical outcomes and patient satisfaction [4]. PCC has not been common practice all the time [3], and different barriers to PCC have been reported [9-11]. Similarly, despite the global emphasis on improving physicians’ clinical communication skills, opportunities have not been fully provided for communication skills training [12]. Communication skills training has not achieved its true official position at most universities of medical sciences [13]. In some cases, efforts have failed to revise the curricula and implement communication skills programs [14]. That is why maximum optimal therapeutic results and health outcomes have not been achieved, and 70% of patients' complaints are still related to the poor communication skills of physicians [15].
Several studies have been done in different settings to assess PCC and identify its barriers. In some institutions, quantitative and qualitative research approaches are combined [12]. In Indonesia, a conflict between ideal and reality has been reported regarding PPR, and additional studies have been recommended to study ways to modify the prevailing communication style into a preferred method [10]. In China, physicians’ communication skills have been surveyed, and further examination of the effectiveness of physicians' communication skills based on examining the perspectives of both patients and physicians and receiving feedback from them has been recommended [16].
The state of PPR has been analyzed in many Iranian studies. The findings of a qualitative inquiry study revealed that the physician-patient communication style in Iran is perceived as considerably physician-oriented. Integrating communication skills into medical curricula in Iran with due consideration to religious issues and ethnical and cultural concerns was recommended as a real educational need for the Iranian society [17]. Since then, given the encouraging effects of PCC and the mentioned recommendations, in many medical schools in Iran [18], medical students have been taught to apply and master communication skills in practice.
Communication barriers have been investigated in a study at the capital of Iran [9]. In Tabriz University of Medical Sciences (TUOMS), where most of the patients in the northwest of Iran receive the required medical services in teaching hospitals affiliated to it, based on the results of the assessment of communication skills of 198 medical residents by 488 patients in 2016 in the largest teaching and academic center in the northwest of Iran, the patients’ satisfaction with participating residents’ communication skills was not acceptable (the mean of the patients’ normalized total satisfaction score was 48.8±18 out of 100) [19]. However, the reasons for patients' dissatisfaction with physicians' communication skills in our institution had not been previously investigated.
It is necessary to pay attention to several important points: 1) The concerns around effective patient-physician communication and providing training related to PCC vary across societies depending on the educational context, norms, beliefs, cultures, and governing social relations; 2) A deeper understanding about the strengths, weaknesses, opportunities, and challenges in every educational context can be provided by conducting a qualitative study; 3) As qualitative research has a contextual nature, the possible transferability of its results to other sociocultural situations should be carefully and cautiously considered [20]; and 4) Up to the time of the present study, no qualitative study has been conducted to explore the perceptions of faculty members, medical students and patients about PCC at TUOMS. Hence, we intended to analyze the status of patient-physician relationships at TUOMS and explore the tips for improving PPR and PCC from the viewpoint of faculty members, students (medical residents and interns), and patients through a qualitative content analysis study.
The results of the present study can be utilized in revising curricula, setting educational priorities, and planning for proper educational interventions. Another important point about this study is that in the current study, alongside the perspectives of patients and physicians, the perspectives of medical interns and residents have also been explored. Based on this part of the study findings, some research hypotheses can be proposed to compare the physicians’ communication skills during the education with a post-graduation period.
Participants and Methods
Study design
In this qualitative content analysis study, the meanings from qualitative data were uncovered and organized to deeply explore the perspectives of patients and physicians, medical interns and residents regarding patient- physician relationship and infer the tips for improving PPR and PCC at teaching hospitals affiliated to Tabriz University of Medical Sciences, Tabriz, Iran. In this research, an in-depth description of performances and perspectives of participants and their behavior patterns within their actual context was provided by interviewing them, observing their behavior and gathering some relevant items. Data were gathered through face-to-face interviews, group discussions, and field observations, and conclusions were drawn through a thematic and manifest summative analysis [21, 22].
Researchers’ characteristics and roles
The interviewer researcher (MB), who was a medical doctor familiar with the study context, studying for a master's degree in Medical Education at the time of this research, always tried to be an active listener. He adopted an open and emotionally neutral body language, looked interested, smiled, employed encouraging body language whenever necessary, and avoided leading questions. He just moderated and facilitated the Focus Group Discussions (FGDs). Group dynamics in FGDs were observed by a second researcher (SGH) to enhance the analysis of interactions, whether verbally or non-verbally. SGH was an MD, Ph.D. She was an MSc graduate in Medical Education and a Ph.D. graduate in Health Education and Health Promotion. At the time of this research, she was a faculty member at the Medical Education group of the Tabriz University of Medical Sciences. Both MB and SGH had attended qualitative studies courses and workshops during their medical/health education studies. Research on communication skills was one of SGH's research interests. SGH had previously participated in qualitative studies as a supervisor or advisor and had published qualitative articles in the PPR field.
At the beginning of the research, bracketing was performed, and the researchers wrote down all their assumptions, perspectives, and hypotheses about the subject and put them aside so that they would not influence data collection and interpretation. Reflexivity was fully handled throughout both data collection and data analysis. Reflexivity journals were prepared by MB and SGH and were checked by peers to share their experiences and perspectives. There was no previous relationship between the researchers and the participants, except for the point that both researchers were working in the same university as the participating faculty members, residents and interns.
In addition to harness personal reflexivity by reflexive writing about participants' explanations and researcher's views, memos and constantly appraising their subjectivity declaration, collaborative reflexivity was ensured by team reflexive dialogue in order to question each other’s perspective, assumption and decisions throughout all the research. The research team made their best to understand the impacts of their presence in the field, either positive or negative, on the context.
Study context
This study was conducted in 2018 at Tabriz University of Medical Sciences (TUOMS). TUOMS is located in the northwest of Iran, and its affiliated hospitals, as referral hospitals, provide diagnostic and treatment services to patients from all cities and villages in the region. In the teaching hospitals affiliated to TUOMS, as the largest and most equipped hospitals in northwestern Iran, patients from different cities in the northwestern region of the country with different ethnicities, such as Fars, Turks, Kurds and sometimes Lors or Arabs are admitted.
At the time of the present study, there was no formal communication skills’ training for medical interns and residents at TUOMS. Most of the communication skills training at TUOMS were limited to vicarious learning (observing the communication behavior of faculty members in the wards and clinics). Residents also had an opportunity to attend a one-day educational workshop, which was held at the beginning of their first year of study.
Participants and sampling strategy
Participants in this study were patients, faculty members, medical interns and residents, who were selected, based on their interest and willingness to express their experiences in PCC, as key informants. Considering the informational needs, no criteria were established to determine the number of informants and field observations. Data collection was continued until data and theme saturation. Participants were selected based on purposive sampling. Indeed, through a non-probability sampling technique, participants who had the desired characteristics were invited to participate. No one refused the researchers' invitation to participate in the study. Criteria for participation in the study were: the inclination to participate and lack of any clinical condition or illness that may disrupt the interview process between the researcher and the participant. Vulnerable groups such as patients with impaired consciousness, the elderly, pregnant women, and children were excluded from participating.
The main researcher (MB) introduced himself and the second researcher (SGH). He stated the objectives of the research and invited potential participants. MB started interviewing patients, faculty members, and medical students in clinical settings (in-patient or out-patient) at teaching hospitals affiliated with TUOMS. He simultaneously observed patient-physician interactions in those settings. Maximum variation of sampling [23], in terms of participants’ gender or their working/presence setting at the time of the study, was used to warrant a broad range of participants’ perceptions and experiences. Negative case sampling was also considered to explain inconsistent and unexpected responses in the data analysis process [21, 24].
Data collection
Data collection methods included in-depth open Face to Face (F2F) individual narrative semi-structured interviews, focus group discussions, and field observations. By doing so, method triangulation [25] was employed to ensure credibility in data collection.
The initial interview guide, including the steps of starting, directing and ending the interview, key interview questions, strategies to probe the answers of the participants, the ways to change the questions after the transcription, and analysis of the text of the previous interviews, was prepared by the research team. The interview guideline was piloted on three participants to ensure clarity of questions, and it was developed further throughout the interview process.
A total of 31 participants were interviewed. No one refused to continue participation, and each interview lasted 40-60 minutes. When possible, the interviews were conducted at participants’ preferred time and place, at clinics, wards or inpatient rooms, after prior coordination and without the presence of a third person.
F2F individual interviews were started with an open-ended question such as “Can you tell me your story about patient-physician relationships you have experienced?” After that, probing and progression upon the participants’ initial responses were done. The flexibility of semi-structured interviews made it possible for the interviewer researcher to discover or elaborate the important information to participants. During the interview, participants were encouraged to express their experiences easily, freely and in full detail. Based on the participants’ permission, the content of the interviews was audio- recorded and transcribed. No repeat interview was carried-out.
To make a rich understanding of participants' collective views and to obtain common contextual information about PCC, five 90–120-minute FGDs were held with 8-12 participants in each group. Group discussion sessions were held after individual F2F interviews. Participants of the group discussion sessions were different from the participants of the individual interviews. The purpose of holding FGDs was a deeper exploration of the participants' perceptions and understandings, a better explanation of the sociocultural factors, and beliefs and meanings which affect the participants’ approaches and behaviors [26].
The composition of the groups was homogenous in terms of the participants’ backgrounds. MB moderated the discussions and facilitated the group dynamics to better understand some specific data gathered through F2F interviews. SGH took notes of participants’ non-verbal communications and interactions.
The composition of the groups was homogenous in terms of the participants’ backgrounds. MB moderated the discussions and facilitated the group dynamics to better understand some specific data gathered through F2F interviews. SGH took notes of participants’ non-verbal communications and interactions.
To have a deeper understanding of the influencing conditions and also to confirm the obtained data about PCC, participants’ actions and contextual realities were observed by MB in inpatient wards during twenty-one sessions. The duration of the sessions varied between 15 and 90 minutes, depending on the patient or ward conditions. Field notes were fully transcribed, and they were checked with the previously transcribed data.
Data collection was continued until data and themes saturation. Saturation was recognized when researchers were confident that no redundant code or categories emerged from the data and the emergent categories matched all the data.
Data analysis
The data from each interview, FGD or field observation was transcribed and coded for analysis immediately after it was collected (before conducting the next interview, FGD or observation). No software was used to manage the data. Analyzing transcripts were done through a thematic and manifest summative analysis [21, 22].
MB and SGH read the transcripts of F2F interviews many times until complete understanding was achieved. They (MB and SGH) separately coded the data and compared various codes based on similarities and differences (constant comparison) in order to make sure that all perspectives were presented by thematic analysis. They discussed emerging codes and categories and resolved disagreements until an optimal level of inter-rater agreement was realized.
Data analysis was performed in four stages:
Stage 1) Decontextualization: Through an open coding process, 119 meaning units or codes were identified. The codes were generated deductively based on the PCC conceptual framework. It was performed repeatedly by two different coders. No computer-program was used to speed up the coding process.
Stage 2) Recontextualization: Unimportant data that did not match the study objective were left out.
Stage 3) Categorization: To categorize the data, the number of words in each meaning unit was condensed without losing its content. To do so, the sense of the data was extracted, and the coded material was divided into subcategories under the previously established categories of the PCC conceptual framework.
Stage 4) Compilation: As a manifest analysis, the research team worked through each identified category, not themes. It means that they often used participants’ words, and they gradually referred back to the original words in the transcripts and stayed closer to the meanings. The research team went back to the participants and presented the extracted data in order to attain their agreement (Member check). A peer was asked to read the transcripts and the meaning units and then critic whether they were sensible or not.
PCC in different settings has been defined with different perspectives, including patient, the economic public policy perspective, and clinical practice perspective. The conceptual framework for the analysis of the research findings in the present study has been organized and reflected based on the definition of the Institute for Patient- and Family-Centered Care [27]. This definition is one of the most complete definitions available, which comprehensively defines PCC with a combination of the above four approaches. The core concepts of the Patient-Centered Communication framework include 1) Respect and dignity, 2) Information sharing, 3) Participation, and 4) Collaboration [7].
Respect and dignity refer to listening to patients and their families, honoring their knowledge, choices, feelings, and beliefs, and incorporating their values, perspectives, and cultural backgrounds into the planning and care processes by healthcare providers [7].
Information sharing refers to sharing timely, useful, supporting, unprejudiced, accurate, and complete information with patients and their families to provide them with opportunities to participate in decision-making and care processes [7].
Participation refers to encouraging and supporting the patients and their families in participating in decision-making and care processes as much as they are interested [7].
Collaboration refers to collaborating with patients, their families, healthcare providers, and leaders in policy and program development, implementation, evaluation, facility design, professional education, and research, as well as the delivery of care [7].
A copy of the primary analysis was sent to participants to validate the emergent codes within the categories and subcategories. It was asked for their comments to achieve their agreement on the correctness of interpretations (member checks). Memos were used to track changes in the coding and recoding processes.
A deductive approach was applied to analyze the content of FGDs to support the predetermined coding structure. Where there was no consensus about some factors influencing the PCC, the data was supplemented with observational ones. A similar deductive approach was used to analyze the field notes of the observer researcher (MB).
Standards for methodological rigor
Standards for methodological rigor were enhanced through different strategies. The credibility of the data was enhanced by data triangulation, member checks, verbatim or direct quotations, and negative case sampling. Data trustworthiness was improved by inter-rater and intra-rater agreements. Transferability was enhanced by maximum variation sampling, rich and thick description of the participant’s perceptions and experiences, description limitations, and detailed description of methods [28].
All methods were performed in accordance with the relevant guidelines, regulations, and ethical standards of the responsible committee approving the research at Tabriz University of Medical Sciences and with the Declaration of Helsinki, as revised in 2000.
Findings
Data saturation was achieved after 31 F2F interviews (13 patients, 6 faculty members, 7 interns, and 5 residents), 9 FGDs with faculty members, interns, and residents (three FGDs in each group), and 21 sessions of field observation. Participants consisted of 13 patients (13 in F2F interviews), 32 faculty members (6 in F2F interviews and 26 in FGDs), 27 medical interns (7 in F2F interviews and 20 in FGDs), and 21 residents (5 in F2F interviews and 16 in FGDs). Participants’ baseline characteristics are revealed in Table 1.
Table 1) Baseline characteristics of study participants
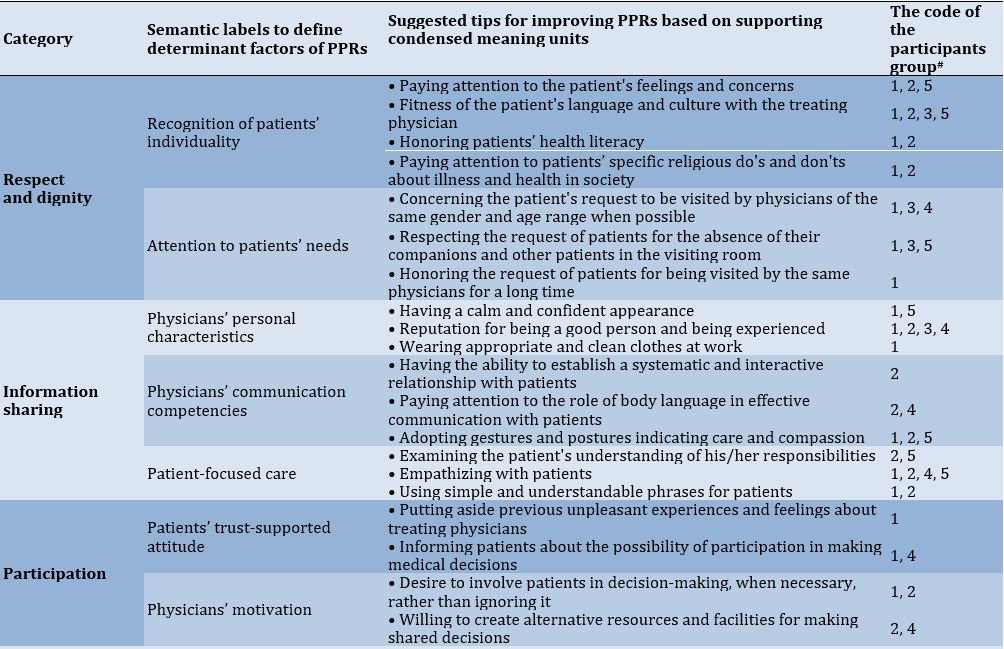
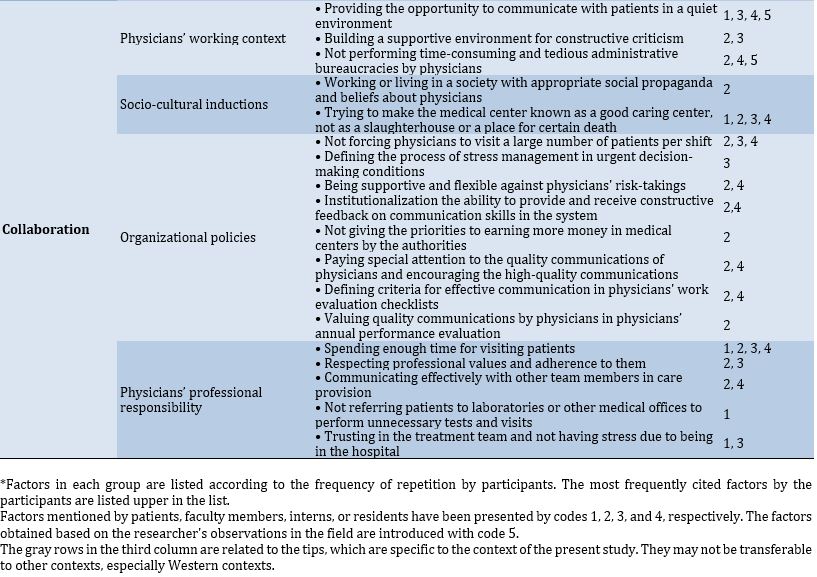
All findings were confirmed by participants’ feedback and their member checking. The emergent categories, semantic labels to define factors determining PPR, and tips for improving PPR and PCC based on supporting condensed meaning units were summarized in Table 2. Factors in each group were listed according to the frequency of repetition by participants. The most frequently cited factors by the participants are listed upper in the list. The gray rows in the third column of Table 2 are related to the tips, which are specific to the context of the present study. They may not be transferable to other contexts, especially Western contexts.
Data analysis resulted in four categories matched with four core concepts of PCC: 1) Respect and dignity, 2) Information sharing, 3) Participation, and 4) Collaboration.
1. Respect and dignity
Factors in this category were divided into two sub-categories including recognition of patients’ individuality and attention to patients’ needs.
1.1. Recognition of patients’ individuality
Many participating patients stated that paying attention to their requests and their feelings and concerns while they had been able to protest could have been easily overshadowed by the PCC (Patients 1, 2, 4, 7, 8, 10, 13).
According to both patients and faculty members, as emotional understanding was another reinforcer of making a PCC, physicians should be trained about empathy and apply it in their daily visits (Faculty members 7, 15; Patients 3, 10).
Paying attention to specific religious do's and don'ts about illness and health in society was introduced as another reinforcing factor of the PPR (Patient10; Faculty member 30).
A faculty member believed that in the setting of this study, a range of physicians and patients from Fars, Turkish, Kurdish and other ethnicities had to communicate with each other. In this regard, that faculty member said that he always had advised his students to spend enough time studying the cultural characteristics of patients and their team members. Otherwise, some of their advice in the absence of respect for beliefs and cultural values of the patients and other members of the medical team might cause serious problems in their relationships (Faculty member 26).
One participating intern who lived in the university dormitory believed that she was able to communicate more well with patients than her other friends because she was roommates with students from different cultures and was familiar with different cultural values (Intern 19).
Patients' levels of education and health literacy were stated to be important factors in reinforcing the patient-physician relationship from the viewpoint of many physicians and some patients. Patients' readiness to establish participatory communication was dependent on their levels of education and health literacy for the most part. Three of the patients participating in the study stated that when they sought, studied, and understood useful and credible information about their medical problems before being visited by a physician and tried to use that information in practice, they adhered more to medical instructions because they trusted more in the abilities of their physicians in such conditions (Patients 5, 8, 11).
In this regard, many faculty members believed that establishing relationships with patients with high health literacy, who did not attribute the reasons for the failure of the physicians' diagnostic and treatment plan to the poor competencies of their physicians, was easier. Those faculty members declared that they were willing to spend more time with patients with higher health literacy because communicating with those patients did not waste their energy and interest (Faculty members 2, 6, 13, 24, 31).
Data analysis resulted in four categories matched with four core concepts of PCC: 1) Respect and dignity, 2) Information sharing, 3) Participation, and 4) Collaboration.
1. Respect and dignity
Factors in this category were divided into two sub-categories including recognition of patients’ individuality and attention to patients’ needs.
1.1. Recognition of patients’ individuality
Many participating patients stated that paying attention to their requests and their feelings and concerns while they had been able to protest could have been easily overshadowed by the PCC (Patients 1, 2, 4, 7, 8, 10, 13).
According to both patients and faculty members, as emotional understanding was another reinforcer of making a PCC, physicians should be trained about empathy and apply it in their daily visits (Faculty members 7, 15; Patients 3, 10).
Paying attention to specific religious do's and don'ts about illness and health in society was introduced as another reinforcing factor of the PPR (Patient10; Faculty member 30).
A faculty member believed that in the setting of this study, a range of physicians and patients from Fars, Turkish, Kurdish and other ethnicities had to communicate with each other. In this regard, that faculty member said that he always had advised his students to spend enough time studying the cultural characteristics of patients and their team members. Otherwise, some of their advice in the absence of respect for beliefs and cultural values of the patients and other members of the medical team might cause serious problems in their relationships (Faculty member 26).
One participating intern who lived in the university dormitory believed that she was able to communicate more well with patients than her other friends because she was roommates with students from different cultures and was familiar with different cultural values (Intern 19).
Patients' levels of education and health literacy were stated to be important factors in reinforcing the patient-physician relationship from the viewpoint of many physicians and some patients. Patients' readiness to establish participatory communication was dependent on their levels of education and health literacy for the most part. Three of the patients participating in the study stated that when they sought, studied, and understood useful and credible information about their medical problems before being visited by a physician and tried to use that information in practice, they adhered more to medical instructions because they trusted more in the abilities of their physicians in such conditions (Patients 5, 8, 11).
In this regard, many faculty members believed that establishing relationships with patients with high health literacy, who did not attribute the reasons for the failure of the physicians' diagnostic and treatment plan to the poor competencies of their physicians, was easier. Those faculty members declared that they were willing to spend more time with patients with higher health literacy because communicating with those patients did not waste their energy and interest (Faculty members 2, 6, 13, 24, 31).
Table 2) The emergent categories, semantic labels, and supporting condensed meaning units, defining factors* determining patient-physician relationship and patient-centered communication
1.2 Attention to patients’ needs
Patients stated that when they had been visited by physicians with the same gender and age range, they had shared more information with their physicians. The gender difference was stated as an important factor influencing the physician-patient relationship. This factor was stated to be even more prominent in Iranian society. According to participants, the age difference between the physician and patients could affect their relationship. Elderly patients, in particular, found it easier to communicate with physicians in the same age group (Patients 2, 10).
In this study, the need for patient-physician gender matching was raised by participating patients, interns, and residents. Gender appropriateness was even more important in the case of female patients during urology and gynecology appointments.
According to the participants, gender matching was true to the situations in which the treating physicians with the same gender had communicated with patients' language and had paid attention to the patients' culture (Patients 7, 10, Interns 2, 5, 6, 14, Residents 19).
Some participating patients stated that they had not known how to describe some of their problems in a language other than their mother tongue. Therefore, when the treating physician had not spoken to them in their mother tongue, they preferred to refrain from reporting some of their problems (Patients. 3, 9, 10).
According to a participating faculty member, the familiarity of a physician with a patient's language was more important when patients were not able to communicate with the national spoken language in the country (Faculty member 7).
2. Information sharing
Three semantic labels, including physicians’ personal characteristics, physicians’ communication competencies, and patient-centered practice, emerged to define factors determining PPRs in this category.
2.1. Physicians’ personal characteristics
A patient believed that physicians’ confidence and charisma could easily affect the PCC (Patient 4).
The punctuality of physicians was stated as one of the main factors by a few patients that could cause a sense of respect (Patients 3, 8).
2.2. Physicians’ communication competencies
According to the participating patients, doubts and hesitations of physicians could be reflected in their tone of voice and even in their gazes (Patients 4, 13). Patients often could understand such hints and were very sensitive to even a minor reaction, which may not be taken seriously by physicians (Faculty member 3).
Another reinforcing factor of the PCC emphasized by most faculty members, was training medical students to be capable of initiating communication in interviewing with patients and in breaking bad news while being supervised (Faculty members 4, 9, 14, 18, 22, 25, 30).
In this regard, most interns and residents believed that the communication skills of faculty members should also be sharpened (Interns 5, 8; Residents 2, 19).
2.3. Patient-focused care
Some of the patients participating in this study complained that most of the treating physicians did not understand their concerns (Patients 7, 11).
The field observations of the main researcher also confirmed that most physicians and students did not empathize with patients. Some participating faculty members and residents believed that they did not have the opportunity to empathize with patients (Faculty members 3, 8, 20; Residents 1, 5, 12, 13, 20).
A patient mentioned: “I did not feel good when a doctor told me that nothing was wrong with my test results because later he told me that I had GERD (Gastro-Esophageal Reflux Disease), I felt that he was just thinking about his work” (Patient 4).
One of the faculty members believed that interns and residents should patiently give patients any necessary information. Then they should question those patients about the actions they should take themselves because many times, patients do not realize the responsibilities they have to personally take to get better (Faculty member 9).
3. Participation
Two semantic labels, patients’ trust-supported attitude and physicians’ motivation, emerged to define determinant factors in this category.
3.1. Patients’ trust-supported attitude
According to participants, putting aside previous unpleasant experiences by the patients and not involving them in accepting the diagnosis and treatment of the treating physicians could significantly decrease the denial of diagnoses and refusal of medical treatments by patients. One participating patient in this study noted that after his father died, he was visited by the same physician as his father when he was hospitalized. He said he is very happy that he ignored the unpleasant memories of his father's hospitalization and also the doubts of his family members about that doctor's abilities, trusted that doctor and his abilities, and got a very good result from his treatment (Patient 4).
3.2. Physicians’ motivation
Patients stated that they had increasingly wanted physicians to consider their role in making treatment decisions while showing authority. According to those patients, when physicians had not prevented them from being involved in decision-making and had respected their rights in this regard, and had not considered their involvement as interference with their scientific position and capability to treat, they had enjoyed their relationship and were open to provide any details about their history of the disease (Patients 6, 9, 11).
According to the participants, if the process of stress management in urgent decision-making conditions were defined and educated, working in stressful environments such as an emergency department would not induce stress, and the PPR would not be easily impaired. In this regard, many interns stated that physicians visiting the emergency department should be aware of the specific needs of the patients who are directly discharged from the emergency department and not hospitalized later because experiencing good communication and the needs being addressed would reinforce patients' later PPRs (Interns 3, 6, 7, 11, 15, 20, 21).
In all, faculty members mentioned that they were more motivated to build effective relationships with patients in inpatient wards compared to the patients in emergency or outpatient wards (Faculty members 3, 7, 24).
4. Collaboration
Factors in this category were divided into four sub-categories, including physicians’ working context, socio-cultural induction, organizational policies, and physicians’ professional responsibility.
4.1. Physicians’ working context
The role of supportiveness and flexibility in the working context against physicians' risk-taking was highlighted as a reinforcing factor of PCC by one intern. He mentioned that with the encouragement of one of the faculty members, he had volunteered to do an abdominal tapping for an inpatient as the first person in their group. He said he had not changed his mind about volunteering because he had been sure he would not have been held accountable for any possible errors due to his teacher's presence. In addition, due to the successful completion of the procedure under the auspices of that teacher, the next day, he communicated with his patient with more confidence (Intern 15).
Participating residents highlighted the role of allocating sufficient time to consult with each patient in the success of communication. According to them, not being forced to perform time-consuming administrative bureaucracies such as "getting patients' lab-tests results by interns and attaching them to the patients' files or taking the radiology reports to other wards to show the faculty members", which could be easily completed by staff of the wards, could be of great help in this regard (Residents 9, 17).
Most interns stated that communicating with patients in an environment away from the hustle and bustle, where patients' companions and other patients were absent during the visit, helped patients communicate more openly and with more trust (Interns 5, 7, 10, 14, 20, 21, 25).
Most of the participating patients believed that respecting their privacy while they were consulted in a convenient and supportive environment had increased their motivation to provide a more complete history to physicians (Patients.1, 3, 4, 7, 9, 10, 12, 13).
Many patients believed that feeling mutual respect and being in an environment supportive of constructive criticism made them satisfied and ultimately increased their trust in physicians (Patients 1, 2, 8, 9, and 10).
Many interns believed that if they had been supervised by well-trained supportive mentors and had received constructive feedback on their communication content and process, they would have made more effective relationships with patients (Interns 4, 7, 10, 15, 17, 18, 20, 24).
Another context-related reinforcing factor raised in the present study by faculty members was the power of the working environment to motivate the health care providers to analyze the existing strengths and weaknesses, to analyze the previously defined working processes or hidden patterns and bureaucracies in the working context, to find problems around, and to plan solutions to them. Indeed, planning for resolving the problems such as delayed admission, poor medical filings, errors in submitting documents for health insurance coverage, etc., would decrease the waste of patients’ time and energy, their exhaustion and dissatisfaction, which would consequently affect their future relationships with physicians (Faculty members 1, 8, 20).
4.2. Socio-cultural inductions
In this study, working or living in a context with appropriate social propaganda and favorable beliefs about physicians in which there are no provocations against the health system was stated as one of the most important socio-cultural factors influencing the PPR. Some participating patients in this study believed that physicians were affluent people who usually could not understand many of patients' socioeconomic problems. They clarified that they usually preferred not to talk to doctors about many of these problems (Patients 4, 5, 9).
Two participating faculty members defined this issue as social propaganda about physicians in Iran. They attributed this propaganda to the differences in physicians' income levels and marked differences in their lifestyles with other people in Iranian society (Faculty members 5, 19).
Participants declared that the reputation of a medical center of being a good caring center, not as a slaughterhouse, could significantly affect patients' and their companions' trust in the physicians' capability in improving their health status; otherwise, social misbeliefs would gradually grow, and breaking them would be more difficult, and their pertinent unpredictable consequences would be experienced. Some inpatients in this study believed that some hospitals had a bad reputation for being a place for certain death. Those patients thought that if they were admitted to those hospitals, they would surely die. For this reason, some patients believed that inpatients did not trust the treatment team in those hospitals and would not be motivated to communicate effectively with their physicians (Patients1, 6, 11).
A participating faculty member also referred to the notion of the reputation of some hospitals as a slaughterhouse among people. He believed that those hospitals were mainly referral hospitals and most complicated cases were admitted in those hospitals (Faculty member 3).
4.3. Organizational policies
According to a participating resident, other factors, such as the resident’s rational working hours and not being fatigued, not being forced to visit a high number of patients in each working shift, and not using medical terms unknown to patients, could significantly affect the physician-patient relationship (Resident 5).
All participating faculty members noted that not forcing physicians to visit a large number of patients per shift was a key to their PCC. Some interns and residents emphasized the need to change the regulations regarding the visit of the high number of patients per shift (Interns 3. 8.19; Residents 2, 17, 19).
One of the participating residents stated that in a few departments, rules had been set so that junior residents were not forced to do all the work of the wards alone. He added that in those settings, one of the faculty members had supervised adherence to the rules and collaboration of the junior and senior residents in performing the ward works. He believed that in such wards he had more easily and effectively communicated with patients (Resident 21).
Participating residents believed that paying special attention to the quality communications of health care providers and encouraging high quality communications could motivate all members of a treatment team to establish more interactive relationships with patients (Residents1, 8, 15).
According to them, in this regard, priorities should be given to building effective relationships, not earning just more money, by authorities in medical centers. Defining criteria for effective communication with patients in physicians' work evaluation checklists to distinguish between quality and non-quality communications of physicians in annual evaluations should be considered a very important reinforcing factor of the PRR.
4.4. Physicians’ professional responsibility
All participants stated that spending enough time in the consultation process by physicians had been the main factor affecting the PCC. A participant said: “A hasty examination of patients not only can induce stress but also may lead to a feeling of not understanding in patients.” (Faculty member 8). A patient said: “When I feel to have enough time, I do trust my physician, and I disclose my history of the disease completely.” (Patient 3).
According to many participants, the pre-coordinated and supervised collaboration of the medical team has been crucial for engaging patients in an interactive relationship (Faculty member 4; Residents 6, 12, 21; Interns 1, 2, 9, 14; Patients 7, 11, 13).
The positive outcome of such proper coordination could be realized when patients needed to be physically examined by medical students, interns, residents, and faculty members at different stages. When this intended coordination was performed, it could decrease fatigue and dissatisfaction among patients (Patients 1, 5, 8, 10; interns 3, 4, 6).
From the participating patients' and faculty members’ viewpoints, hierarchical supervision of residents, interns, and medical students’ performance could inhibit repetitive physical examinations and consequently could increase patients’ satisfaction and cooperation (Faculty members 1, 7, 10; Patients 5, 10, 12).
Communicating effectively with other team members in care provision, i.e. optimal physician-physician, physician-nurse, and physician-medical staff communications, was described as another important factor affecting the PCC by a participating faculty member (Faculty member 21).
A resident believed that “When a treating physician forces a patient to go to a specific center that he or she recommends for taking paraclinical tests, the patient usually thinks that the treating physician has a conflict of interest and only pays attention to the financial benefits of his colleagues.” (Resident 5).
The majority of participating physicians in this study believed that requests for only necessary consultations and paraclinical tests not only could cease any delay in fulfilling the diagnostic processes but also could prohibit wasting energy and decrease the workload of the consulting physicians, which ultimately could result in patient satisfaction and affect the PCC (Faculty members 11, 12, 21, 26, 28; Residents 1, 5, 10, 15, 18, 20).
Coordination between a physician and a nurse could decrease delays or errors in the execution of physician orders. A faculty member mentioned: “Failure to inject the prescribed anticoagulant to the patient before his surgery had resulted in deep vein thrombosis.” He declared: “The head nurse was present when ordering the injection of the anticoagulant, but my order had been missed.” (Faculty member 17).
According to participants, the acceptable status of the patient's health and not having stress induced by the presence in a medical environment could affect the PCC too (Patients 7, 11; Intern 2).
This outcome could be obvious in critically ill patients and traumatic cases in stressful situations. In such circumstances, the ability to manage such challenging conditions and pay attention to the reactions of patients and companions to even minor issues resulted in a PCC (Interns 2, 15).
In this regard, one of the participating interns stated that to decrease his patients and their companions’ concerns and stress about the hours and days the patients would be hospitalized, he had routinely asked his patients and their companions about their concerns and had tried to clearly explain hospitalization-related processes to them. He believed that when he had assured his patients and companions that he would always be there to hear their concerns and provide the necessary information, they reported less stress during hospitalization (Intern 15).
Discussion
In this study, data analysis resulted in four categories matched with four core concepts of PCC: 1) Respect and dignity, 2) Information sharing, 3) Participation, and 4) Collaboration. Being explored by content analysis, 38 pieces of advice to improve the PPR and PCC were inferred. They were classified into 4 categories and 11 sub-categories.
In this study, the target audiences of the 16 tips of the 38 proposed tips are only physicians. So, it is not possible to improve the quality of PPRs without the empowerment of physicians and improving their knowledge, attitude, or skills. The implementation of these 16 tips does not require any other systemic changes and preparations. This finding seems to be noteworthy according to research, in which the conclusions of recent reviews and research were reviewed [29]. In this review, reinforcers of the quality of the PPR are discussed. It has been declared that physician factors, except for the physicians’ empathic abilities, have been studied very little in previous studies.
Among the studies which have taken physician-related factors into account, most studies have focused on just the verbal communication behavior of physicians. The non-verbal dimension of communication has been less highlighted [29] and has been less analyzed. In this review, the difficulties in the analysis have been attributed to “the social and technological changes” [29], while the participants of the present study attributed the success of the PPR mainly to the physicians' non-verbal communication, such as their facial expressions, type of clothing, body language, posture, and gesture.
The importance and the necessity of analysis of physicians’ non-verbal communication have been well illustrated and published following a presentation at the American College of Surgeons, 102nd Annual Clinical Congress in 2016. In this publication, reliance on the physicians’ character and professional competencies, their strengths and their truth has been mentioned as the keystone of the PPR. In other words, integrity and stability of physicians’ relationships with patients, team members, and themselves have been stated to be dependent on trust as the so-called keystone. Non-verbal communication has been declared as the most preferred relationship, which could efficiently and effectively engender trust [30].
The two most frequently cited determinant factors of the PPR and PCC, from the viewpoints of participants in this study, were not forcing physicians to visit a large number of patients per shift and spending enough time visiting each patient.
These findings are in line with those in the study by Rees et al., in which participating students stated that clinical mentors had not allowed them to build effective communication due to the created time constraints [31]. The findings of the study by Claramita et al. are also consistent with ours. In their study, the high number of patients had significantly delayed effective communication with physicians [10].
The results of the present study showed that paying attention to the patient's feelings and concerns and involving patients in decision-making is an important determinant factor of PCC. This finding is similar to the findings of a study conducted in Turkey in 2020 in which the effect of the PPR on the obedience of 399 adult patients to diagnosis and treatment plans and the mediating role of shared decision-making in that effect have been reported [32].
Our participants declared that patients with acceptable health literacy become more involved in building and maintaining participatory communication. Indeed, patients with higher levels of education and health literacy communicate more effectively with their physicians.
In a study by Claramita et al., patient unpreparedness for participatory communication was introduced as one of the three main barriers to physician-patient communication. They noted that patients with higher education are more prepared to maintain participatory communication [10].
According to the findings of a study in the U.S. Southeast [33], more than half of 3176 rural patients had seen the same physician for more than five years. Those patients’ satisfaction and confidence in their physicians were higher compared to the satisfaction and confidence of the patients who had shorter continuity of care. Non-white and less educated patients with no health insurance and those with income lesser than $25,000 had seen the same physicians for less than five years. These findings confirm that trust and confidence in doctors and, as a result, the effectiveness of PPRs, in addition to some doctor-related factors, also depend on various patient-related factors. That is why to enhance the outcomes of patient satisfaction with care, trying to establish long-term PPR is recommended [33].
Over the past decade, patients are more informed by social media and the internet, and they are less reliant on physicians to acquire health-related information and necessary medical resources. This worldwide change has significantly influenced the PPR in a way that medical paternalism has been rejected in favor of admiration of patients’ autonomy [34]. It means that in line with the findings of our study, the PPR has been affected by patients’ health literacy. As if, in the new era of patients’ autonomy [34], rethinking physicians’ role in the PPR is highly needed, and physicians are still required to exercise their professional agency to provide counseling, procedural expertise, and access to limited health services for patients [34].
Appropriateness of the patients’ age and gender and fitness of their language and culture with those of their treating physicians were mentioned as the most important patient-related factors determining PCC in this study. In a study at Johns Hopkins Bloomberg School of Public Health, physicians’ self-reported cultural competence was reported to be highly associated with the quality of the PPR and patients’ participation in care. In that study, physicians with superior attitudes, whose frequency of culturally proficient behavior was sophisticated based on their self-assessment, had more reflected cultural competence in their clinical behaviors. They developed more participative and higher-quality relationships with their patients in low to middle-class populations [35]. Their patients had been more satisfied, had perceived their physicians had been more facilitative, and had searched for and shared more information with their physicians [35].
As mentioned in previous studies, the gender difference between a patient and a physician could truly affect the quality of their relationship. Previous studies show that gender matches between a patient and a physician could lead to a more successful relationship, especially when they both are females. In a study in China, some patients, who were referred to a male urologist, were asked to describe their experience in this regard. Most of them reported their experience as unpleasant because of a feeling of a deep gap in their relationship induced by just gender differences. In that study, patients related their other unpleasant experiences to their induced stress, lack of physician seriousness in treatment, not respecting their autonomy, and the lack of their physicians’ empathy skills [36]. The gender difference was even more noteworthy from the viewpoints of the participants of the present study, considering the Iranian socio-cultural context.
In our study, paying attention to specific religious do's and don'ts about illness and health in society was stated as one of the most important socio-cultural factors determining PCC. This finding is in line with those of a study in Japan, in which communication styles were declared to be different in Western countries and Japan. In that study, Japanese patients preferred the model of mutual participation as the ideal model of the PPR, and four cultural characteristics, including collectivism, high context, masculinity, and Confucianism [37], were strongly related to the characteristics of the PPR in Japan. It was contended that to achieve fruitful relationships, socio-cultural factors in the Japanese context should be pursued to design a mutual participatory model of PPR for Japan [37], and patient autonomy should be advocated and appreciated. For these reasons, the researchers concluded that socio-culturally tailored communication models, not exactly the same as Western models, are needed in contemporary Japan [37].
Similar to the conclusion of the above-mentioned Japanese study, the results of the present study remind us of the necessity of designing a socio-culturally tailored communication model for Eastern societies and even a model specific to Iranian society. Eighteen of the tips raised by the participants to improve PPR and PCC, which are highlighted in gray in the third column of Table 2, were not already mentioned in the literature. It seems that these recommendations are specific to Iranian society.
These specific tips are related to some features of our context in this research, which can be similar to those in some Eastern countries. These tips, proposed based on the findings of this research, indicate the necessity of interventions to change them.
In our context, the referral of patients by family physicians to specialist physicians is done to a very limited extent, and the selection of the specialist physicians is mainly done by the patients themselves. There is no limit on the number of patient visits by specialist physicians, which in turn imposes a very high volume of work on Iranian medical physicians. In most cases, the place of hospitalization of the patients is chosen by the patients themselves because some third-level hospitals, where mostly sick and referred patients from nearby cities are admitted there, are known as slaughterhouses, and patients usually avoid hospitalization in those hospitals.
In the checklists for evaluation of physicians' performance in medical training centers in our context, there are no items for evaluation of their communication skills. Therefore, physicians' payments have nothing to do with their effective communication with their patients. This can be one of the reasons for the low motivation of physicians to involve their patients in making shared decisions.
Of course, in Iran, due to cultural reasons, the willingness of patients to participate in decision-making has been low for a long time. Unlike in the western countries, most patients prefer their companions to participate in making shared decisions with physicians rather than themselves. The next difference between our context and other contexts is related to the possibility of the presence of companions and even other patients at the visit room. The tip pointed out by our participants in this research about the necessity of the absence of companions and other patients in the visit room is indicating this difference. This tip may not make any sense to some international readers, but it reminds us of the need for any planning and intervention to fix it in our context.
In our context, while patients can usually directly refer to specialist physicians, according to some participants, some physicians recommend patients refer to specific paraclinical centers or specific physicians to receive additional services. Some patients consider these instructions and recommendations unnecessary. Physicians mention the high quality of their services of those centers or physicians compared to other centers and physicians as the reason for recommending those centers or physicians. In all these cases, some patients are worried about the possible conflict of interest between their treating physicians and the proposed paraclinical centers or physicians.
As reported by previous studies, today's socio-cultural expectations require physicians to understand patients’ feelings and show empathy [38]. This issue would be a challenge for physicians believing that they should maintain a professional distance from their patients in terms of emotions [39].
Most participating medical students and residents in this study stated that if they had received any practical or theoretical training in a predefined formal program, they would have made better relationships with patients and other members of the treatment team. In all, according to the participants of this study, the current situation of the PPR at TUOMS was not satisfying. Taking into account all reinforcing factors identified in this research could help in designing comprehensive educational interventions in this regard.
Similar to other qualitative studies, it was not possible to investigate any causal relationship between the PPR and the factors explored in this study. However, as the factors determining the PPR have been explored in our context, researchers can focus on the factors explored in this study in their future experimental studies.
Limitations
The target audiences of the 16 tips of the 38 proposed tips are only physicians. As previously mentioned, according to the results of a review study, physician-related factors have been less explored in previous studies. Therefore, we had limitations in comparing the results of this study on some physician-related factors with the results of other studies. Therefore, it is recommended that similar studies be conducted in other countries in the future, especially in countries with different contextual and socio-cultural factors, to be able to compare and synthesize the findings of qualitative studies.
Patients admitted to the wards and students participating in the study were repeatedly reassured that the content of their interviews would not be made available to their care providers or the people in charge of education at TUOMS in any way. However, considering some of their nonverbal behaviors, such as pausing or changing the course of their speech when they decided to refer to the existing weaknesses, one could have noticed that they were probably concerned about the possible reactions of their care providers or the people in charge of education to some of their statements. So, the possibility of such a bias in the participants’ answers has been present in this qualitative study, like other qualitative studies, albeit to a small extent.
Conclusion
Patient-centered communication can be characterized by honoring patients’ individuality, paying attention to patients’ needs, focusing on physicians’ proper personal characteristics in continuing medical education, enhancing physicians’ communication competencies, institutionalization of patient-focused care, creating trust-supported attitudes among patients, increasing physicians’ motivation, regulating physicians’ working context, serious attention to social and cultural inductions, making supportive organizational policies, and evaluating physicians’ professional responsibilities. Most of the characteristics of the PCC mentioned by the participants of this study can be the focus of some educational interventions to improve patient-physician relationships, even in similar Eastern societies.
Acknowledgements: We would like to extend our sincere gratitude to all patients and scholars for their invaluable participation in this study. Without their active participation, the study could not have been completed.
Ethical Permission: The ethical committee board at Tabriz University of Medical Sciences approved this study (The approval code number: IR.TBZMED.REC.1395.1129). All methods were performed in accordance with the relevant guidelines, regulations, and ethical standards of the responsible committee approving the research at Tabriz University of Medical Sciences and with the Declaration of Helsinki, as revised in 2000. Permission to attend in and out-patient settings was given by heads of departments. All participants provided written informed consent to participate. The aim and learning objectives of the study were clearly shared with participants. A unique code was assigned to each participant. The participants were told that all the research data would be saved confidential. They were granted the right to withdraw from the study whenever they wanted.
Conflict of Interests: The authors declare that they have no competing interests except for the point that the corresponding author, SGH, is the scientific editor of the HEHP.
Authors’ Contribution: Bagheri M (First Author), Introduction Writer/Main Researcher/Discussion Writer (35%); Somi MH (Second Author), Introduction Writer/Methodologist/Statistical Analyst/Discussion Writer (15%); Dehghani Gh (Third Author), Introduction Writer/Discussion Writer (15%); Ghaffarifar S (Fourth Author), Introduction Writer/Methodologist/Statistical Analyst/Discussion Writer (35%)
Funding: Tabriz University of Medical Sciences funded and supported this study. (Grant No.: 5/d/497328).
1.2 Attention to patients’ needs
Patients stated that when they had been visited by physicians with the same gender and age range, they had shared more information with their physicians. The gender difference was stated as an important factor influencing the physician-patient relationship. This factor was stated to be even more prominent in Iranian society. According to participants, the age difference between the physician and patients could affect their relationship. Elderly patients, in particular, found it easier to communicate with physicians in the same age group (Patients 2, 10).
In this study, the need for patient-physician gender matching was raised by participating patients, interns, and residents. Gender appropriateness was even more important in the case of female patients during urology and gynecology appointments.
According to the participants, gender matching was true to the situations in which the treating physicians with the same gender had communicated with patients' language and had paid attention to the patients' culture (Patients 7, 10, Interns 2, 5, 6, 14, Residents 19).
Some participating patients stated that they had not known how to describe some of their problems in a language other than their mother tongue. Therefore, when the treating physician had not spoken to them in their mother tongue, they preferred to refrain from reporting some of their problems (Patients. 3, 9, 10).
According to a participating faculty member, the familiarity of a physician with a patient's language was more important when patients were not able to communicate with the national spoken language in the country (Faculty member 7).
2. Information sharing
Three semantic labels, including physicians’ personal characteristics, physicians’ communication competencies, and patient-centered practice, emerged to define factors determining PPRs in this category.
2.1. Physicians’ personal characteristics
A patient believed that physicians’ confidence and charisma could easily affect the PCC (Patient 4).
The punctuality of physicians was stated as one of the main factors by a few patients that could cause a sense of respect (Patients 3, 8).
2.2. Physicians’ communication competencies
According to the participating patients, doubts and hesitations of physicians could be reflected in their tone of voice and even in their gazes (Patients 4, 13). Patients often could understand such hints and were very sensitive to even a minor reaction, which may not be taken seriously by physicians (Faculty member 3).
Another reinforcing factor of the PCC emphasized by most faculty members, was training medical students to be capable of initiating communication in interviewing with patients and in breaking bad news while being supervised (Faculty members 4, 9, 14, 18, 22, 25, 30).
In this regard, most interns and residents believed that the communication skills of faculty members should also be sharpened (Interns 5, 8; Residents 2, 19).
2.3. Patient-focused care
Some of the patients participating in this study complained that most of the treating physicians did not understand their concerns (Patients 7, 11).
The field observations of the main researcher also confirmed that most physicians and students did not empathize with patients. Some participating faculty members and residents believed that they did not have the opportunity to empathize with patients (Faculty members 3, 8, 20; Residents 1, 5, 12, 13, 20).
A patient mentioned: “I did not feel good when a doctor told me that nothing was wrong with my test results because later he told me that I had GERD (Gastro-Esophageal Reflux Disease), I felt that he was just thinking about his work” (Patient 4).
One of the faculty members believed that interns and residents should patiently give patients any necessary information. Then they should question those patients about the actions they should take themselves because many times, patients do not realize the responsibilities they have to personally take to get better (Faculty member 9).
3. Participation
Two semantic labels, patients’ trust-supported attitude and physicians’ motivation, emerged to define determinant factors in this category.
3.1. Patients’ trust-supported attitude
According to participants, putting aside previous unpleasant experiences by the patients and not involving them in accepting the diagnosis and treatment of the treating physicians could significantly decrease the denial of diagnoses and refusal of medical treatments by patients. One participating patient in this study noted that after his father died, he was visited by the same physician as his father when he was hospitalized. He said he is very happy that he ignored the unpleasant memories of his father's hospitalization and also the doubts of his family members about that doctor's abilities, trusted that doctor and his abilities, and got a very good result from his treatment (Patient 4).
3.2. Physicians’ motivation
Patients stated that they had increasingly wanted physicians to consider their role in making treatment decisions while showing authority. According to those patients, when physicians had not prevented them from being involved in decision-making and had respected their rights in this regard, and had not considered their involvement as interference with their scientific position and capability to treat, they had enjoyed their relationship and were open to provide any details about their history of the disease (Patients 6, 9, 11).
According to the participants, if the process of stress management in urgent decision-making conditions were defined and educated, working in stressful environments such as an emergency department would not induce stress, and the PPR would not be easily impaired. In this regard, many interns stated that physicians visiting the emergency department should be aware of the specific needs of the patients who are directly discharged from the emergency department and not hospitalized later because experiencing good communication and the needs being addressed would reinforce patients' later PPRs (Interns 3, 6, 7, 11, 15, 20, 21).
In all, faculty members mentioned that they were more motivated to build effective relationships with patients in inpatient wards compared to the patients in emergency or outpatient wards (Faculty members 3, 7, 24).
4. Collaboration
Factors in this category were divided into four sub-categories, including physicians’ working context, socio-cultural induction, organizational policies, and physicians’ professional responsibility.
4.1. Physicians’ working context
The role of supportiveness and flexibility in the working context against physicians' risk-taking was highlighted as a reinforcing factor of PCC by one intern. He mentioned that with the encouragement of one of the faculty members, he had volunteered to do an abdominal tapping for an inpatient as the first person in their group. He said he had not changed his mind about volunteering because he had been sure he would not have been held accountable for any possible errors due to his teacher's presence. In addition, due to the successful completion of the procedure under the auspices of that teacher, the next day, he communicated with his patient with more confidence (Intern 15).
Participating residents highlighted the role of allocating sufficient time to consult with each patient in the success of communication. According to them, not being forced to perform time-consuming administrative bureaucracies such as "getting patients' lab-tests results by interns and attaching them to the patients' files or taking the radiology reports to other wards to show the faculty members", which could be easily completed by staff of the wards, could be of great help in this regard (Residents 9, 17).
Most interns stated that communicating with patients in an environment away from the hustle and bustle, where patients' companions and other patients were absent during the visit, helped patients communicate more openly and with more trust (Interns 5, 7, 10, 14, 20, 21, 25).
Most of the participating patients believed that respecting their privacy while they were consulted in a convenient and supportive environment had increased their motivation to provide a more complete history to physicians (Patients.1, 3, 4, 7, 9, 10, 12, 13).
Many patients believed that feeling mutual respect and being in an environment supportive of constructive criticism made them satisfied and ultimately increased their trust in physicians (Patients 1, 2, 8, 9, and 10).
Many interns believed that if they had been supervised by well-trained supportive mentors and had received constructive feedback on their communication content and process, they would have made more effective relationships with patients (Interns 4, 7, 10, 15, 17, 18, 20, 24).
Another context-related reinforcing factor raised in the present study by faculty members was the power of the working environment to motivate the health care providers to analyze the existing strengths and weaknesses, to analyze the previously defined working processes or hidden patterns and bureaucracies in the working context, to find problems around, and to plan solutions to them. Indeed, planning for resolving the problems such as delayed admission, poor medical filings, errors in submitting documents for health insurance coverage, etc., would decrease the waste of patients’ time and energy, their exhaustion and dissatisfaction, which would consequently affect their future relationships with physicians (Faculty members 1, 8, 20).
4.2. Socio-cultural inductions
In this study, working or living in a context with appropriate social propaganda and favorable beliefs about physicians in which there are no provocations against the health system was stated as one of the most important socio-cultural factors influencing the PPR. Some participating patients in this study believed that physicians were affluent people who usually could not understand many of patients' socioeconomic problems. They clarified that they usually preferred not to talk to doctors about many of these problems (Patients 4, 5, 9).
Two participating faculty members defined this issue as social propaganda about physicians in Iran. They attributed this propaganda to the differences in physicians' income levels and marked differences in their lifestyles with other people in Iranian society (Faculty members 5, 19).
Participants declared that the reputation of a medical center of being a good caring center, not as a slaughterhouse, could significantly affect patients' and their companions' trust in the physicians' capability in improving their health status; otherwise, social misbeliefs would gradually grow, and breaking them would be more difficult, and their pertinent unpredictable consequences would be experienced. Some inpatients in this study believed that some hospitals had a bad reputation for being a place for certain death. Those patients thought that if they were admitted to those hospitals, they would surely die. For this reason, some patients believed that inpatients did not trust the treatment team in those hospitals and would not be motivated to communicate effectively with their physicians (Patients1, 6, 11).
A participating faculty member also referred to the notion of the reputation of some hospitals as a slaughterhouse among people. He believed that those hospitals were mainly referral hospitals and most complicated cases were admitted in those hospitals (Faculty member 3).
4.3. Organizational policies
According to a participating resident, other factors, such as the resident’s rational working hours and not being fatigued, not being forced to visit a high number of patients in each working shift, and not using medical terms unknown to patients, could significantly affect the physician-patient relationship (Resident 5).
All participating faculty members noted that not forcing physicians to visit a large number of patients per shift was a key to their PCC. Some interns and residents emphasized the need to change the regulations regarding the visit of the high number of patients per shift (Interns 3. 8.19; Residents 2, 17, 19).
One of the participating residents stated that in a few departments, rules had been set so that junior residents were not forced to do all the work of the wards alone. He added that in those settings, one of the faculty members had supervised adherence to the rules and collaboration of the junior and senior residents in performing the ward works. He believed that in such wards he had more easily and effectively communicated with patients (Resident 21).
Participating residents believed that paying special attention to the quality communications of health care providers and encouraging high quality communications could motivate all members of a treatment team to establish more interactive relationships with patients (Residents1, 8, 15).
According to them, in this regard, priorities should be given to building effective relationships, not earning just more money, by authorities in medical centers. Defining criteria for effective communication with patients in physicians' work evaluation checklists to distinguish between quality and non-quality communications of physicians in annual evaluations should be considered a very important reinforcing factor of the PRR.
4.4. Physicians’ professional responsibility
All participants stated that spending enough time in the consultation process by physicians had been the main factor affecting the PCC. A participant said: “A hasty examination of patients not only can induce stress but also may lead to a feeling of not understanding in patients.” (Faculty member 8). A patient said: “When I feel to have enough time, I do trust my physician, and I disclose my history of the disease completely.” (Patient 3).
According to many participants, the pre-coordinated and supervised collaboration of the medical team has been crucial for engaging patients in an interactive relationship (Faculty member 4; Residents 6, 12, 21; Interns 1, 2, 9, 14; Patients 7, 11, 13).
The positive outcome of such proper coordination could be realized when patients needed to be physically examined by medical students, interns, residents, and faculty members at different stages. When this intended coordination was performed, it could decrease fatigue and dissatisfaction among patients (Patients 1, 5, 8, 10; interns 3, 4, 6).
From the participating patients' and faculty members’ viewpoints, hierarchical supervision of residents, interns, and medical students’ performance could inhibit repetitive physical examinations and consequently could increase patients’ satisfaction and cooperation (Faculty members 1, 7, 10; Patients 5, 10, 12).
Communicating effectively with other team members in care provision, i.e. optimal physician-physician, physician-nurse, and physician-medical staff communications, was described as another important factor affecting the PCC by a participating faculty member (Faculty member 21).
A resident believed that “When a treating physician forces a patient to go to a specific center that he or she recommends for taking paraclinical tests, the patient usually thinks that the treating physician has a conflict of interest and only pays attention to the financial benefits of his colleagues.” (Resident 5).
The majority of participating physicians in this study believed that requests for only necessary consultations and paraclinical tests not only could cease any delay in fulfilling the diagnostic processes but also could prohibit wasting energy and decrease the workload of the consulting physicians, which ultimately could result in patient satisfaction and affect the PCC (Faculty members 11, 12, 21, 26, 28; Residents 1, 5, 10, 15, 18, 20).
Coordination between a physician and a nurse could decrease delays or errors in the execution of physician orders. A faculty member mentioned: “Failure to inject the prescribed anticoagulant to the patient before his surgery had resulted in deep vein thrombosis.” He declared: “The head nurse was present when ordering the injection of the anticoagulant, but my order had been missed.” (Faculty member 17).
According to participants, the acceptable status of the patient's health and not having stress induced by the presence in a medical environment could affect the PCC too (Patients 7, 11; Intern 2).
This outcome could be obvious in critically ill patients and traumatic cases in stressful situations. In such circumstances, the ability to manage such challenging conditions and pay attention to the reactions of patients and companions to even minor issues resulted in a PCC (Interns 2, 15).
In this regard, one of the participating interns stated that to decrease his patients and their companions’ concerns and stress about the hours and days the patients would be hospitalized, he had routinely asked his patients and their companions about their concerns and had tried to clearly explain hospitalization-related processes to them. He believed that when he had assured his patients and companions that he would always be there to hear their concerns and provide the necessary information, they reported less stress during hospitalization (Intern 15).
Discussion
In this study, data analysis resulted in four categories matched with four core concepts of PCC: 1) Respect and dignity, 2) Information sharing, 3) Participation, and 4) Collaboration. Being explored by content analysis, 38 pieces of advice to improve the PPR and PCC were inferred. They were classified into 4 categories and 11 sub-categories.
In this study, the target audiences of the 16 tips of the 38 proposed tips are only physicians. So, it is not possible to improve the quality of PPRs without the empowerment of physicians and improving their knowledge, attitude, or skills. The implementation of these 16 tips does not require any other systemic changes and preparations. This finding seems to be noteworthy according to research, in which the conclusions of recent reviews and research were reviewed [29]. In this review, reinforcers of the quality of the PPR are discussed. It has been declared that physician factors, except for the physicians’ empathic abilities, have been studied very little in previous studies.
Among the studies which have taken physician-related factors into account, most studies have focused on just the verbal communication behavior of physicians. The non-verbal dimension of communication has been less highlighted [29] and has been less analyzed. In this review, the difficulties in the analysis have been attributed to “the social and technological changes” [29], while the participants of the present study attributed the success of the PPR mainly to the physicians' non-verbal communication, such as their facial expressions, type of clothing, body language, posture, and gesture.
The importance and the necessity of analysis of physicians’ non-verbal communication have been well illustrated and published following a presentation at the American College of Surgeons, 102nd Annual Clinical Congress in 2016. In this publication, reliance on the physicians’ character and professional competencies, their strengths and their truth has been mentioned as the keystone of the PPR. In other words, integrity and stability of physicians’ relationships with patients, team members, and themselves have been stated to be dependent on trust as the so-called keystone. Non-verbal communication has been declared as the most preferred relationship, which could efficiently and effectively engender trust [30].
The two most frequently cited determinant factors of the PPR and PCC, from the viewpoints of participants in this study, were not forcing physicians to visit a large number of patients per shift and spending enough time visiting each patient.
These findings are in line with those in the study by Rees et al., in which participating students stated that clinical mentors had not allowed them to build effective communication due to the created time constraints [31]. The findings of the study by Claramita et al. are also consistent with ours. In their study, the high number of patients had significantly delayed effective communication with physicians [10].
The results of the present study showed that paying attention to the patient's feelings and concerns and involving patients in decision-making is an important determinant factor of PCC. This finding is similar to the findings of a study conducted in Turkey in 2020 in which the effect of the PPR on the obedience of 399 adult patients to diagnosis and treatment plans and the mediating role of shared decision-making in that effect have been reported [32].
Our participants declared that patients with acceptable health literacy become more involved in building and maintaining participatory communication. Indeed, patients with higher levels of education and health literacy communicate more effectively with their physicians.
In a study by Claramita et al., patient unpreparedness for participatory communication was introduced as one of the three main barriers to physician-patient communication. They noted that patients with higher education are more prepared to maintain participatory communication [10].
According to the findings of a study in the U.S. Southeast [33], more than half of 3176 rural patients had seen the same physician for more than five years. Those patients’ satisfaction and confidence in their physicians were higher compared to the satisfaction and confidence of the patients who had shorter continuity of care. Non-white and less educated patients with no health insurance and those with income lesser than $25,000 had seen the same physicians for less than five years. These findings confirm that trust and confidence in doctors and, as a result, the effectiveness of PPRs, in addition to some doctor-related factors, also depend on various patient-related factors. That is why to enhance the outcomes of patient satisfaction with care, trying to establish long-term PPR is recommended [33].
Over the past decade, patients are more informed by social media and the internet, and they are less reliant on physicians to acquire health-related information and necessary medical resources. This worldwide change has significantly influenced the PPR in a way that medical paternalism has been rejected in favor of admiration of patients’ autonomy [34]. It means that in line with the findings of our study, the PPR has been affected by patients’ health literacy. As if, in the new era of patients’ autonomy [34], rethinking physicians’ role in the PPR is highly needed, and physicians are still required to exercise their professional agency to provide counseling, procedural expertise, and access to limited health services for patients [34].
Appropriateness of the patients’ age and gender and fitness of their language and culture with those of their treating physicians were mentioned as the most important patient-related factors determining PCC in this study. In a study at Johns Hopkins Bloomberg School of Public Health, physicians’ self-reported cultural competence was reported to be highly associated with the quality of the PPR and patients’ participation in care. In that study, physicians with superior attitudes, whose frequency of culturally proficient behavior was sophisticated based on their self-assessment, had more reflected cultural competence in their clinical behaviors. They developed more participative and higher-quality relationships with their patients in low to middle-class populations [35]. Their patients had been more satisfied, had perceived their physicians had been more facilitative, and had searched for and shared more information with their physicians [35].
As mentioned in previous studies, the gender difference between a patient and a physician could truly affect the quality of their relationship. Previous studies show that gender matches between a patient and a physician could lead to a more successful relationship, especially when they both are females. In a study in China, some patients, who were referred to a male urologist, were asked to describe their experience in this regard. Most of them reported their experience as unpleasant because of a feeling of a deep gap in their relationship induced by just gender differences. In that study, patients related their other unpleasant experiences to their induced stress, lack of physician seriousness in treatment, not respecting their autonomy, and the lack of their physicians’ empathy skills [36]. The gender difference was even more noteworthy from the viewpoints of the participants of the present study, considering the Iranian socio-cultural context.
In our study, paying attention to specific religious do's and don'ts about illness and health in society was stated as one of the most important socio-cultural factors determining PCC. This finding is in line with those of a study in Japan, in which communication styles were declared to be different in Western countries and Japan. In that study, Japanese patients preferred the model of mutual participation as the ideal model of the PPR, and four cultural characteristics, including collectivism, high context, masculinity, and Confucianism [37], were strongly related to the characteristics of the PPR in Japan. It was contended that to achieve fruitful relationships, socio-cultural factors in the Japanese context should be pursued to design a mutual participatory model of PPR for Japan [37], and patient autonomy should be advocated and appreciated. For these reasons, the researchers concluded that socio-culturally tailored communication models, not exactly the same as Western models, are needed in contemporary Japan [37].
Similar to the conclusion of the above-mentioned Japanese study, the results of the present study remind us of the necessity of designing a socio-culturally tailored communication model for Eastern societies and even a model specific to Iranian society. Eighteen of the tips raised by the participants to improve PPR and PCC, which are highlighted in gray in the third column of Table 2, were not already mentioned in the literature. It seems that these recommendations are specific to Iranian society.
These specific tips are related to some features of our context in this research, which can be similar to those in some Eastern countries. These tips, proposed based on the findings of this research, indicate the necessity of interventions to change them.
In our context, the referral of patients by family physicians to specialist physicians is done to a very limited extent, and the selection of the specialist physicians is mainly done by the patients themselves. There is no limit on the number of patient visits by specialist physicians, which in turn imposes a very high volume of work on Iranian medical physicians. In most cases, the place of hospitalization of the patients is chosen by the patients themselves because some third-level hospitals, where mostly sick and referred patients from nearby cities are admitted there, are known as slaughterhouses, and patients usually avoid hospitalization in those hospitals.
In the checklists for evaluation of physicians' performance in medical training centers in our context, there are no items for evaluation of their communication skills. Therefore, physicians' payments have nothing to do with their effective communication with their patients. This can be one of the reasons for the low motivation of physicians to involve their patients in making shared decisions.
Of course, in Iran, due to cultural reasons, the willingness of patients to participate in decision-making has been low for a long time. Unlike in the western countries, most patients prefer their companions to participate in making shared decisions with physicians rather than themselves. The next difference between our context and other contexts is related to the possibility of the presence of companions and even other patients at the visit room. The tip pointed out by our participants in this research about the necessity of the absence of companions and other patients in the visit room is indicating this difference. This tip may not make any sense to some international readers, but it reminds us of the need for any planning and intervention to fix it in our context.
In our context, while patients can usually directly refer to specialist physicians, according to some participants, some physicians recommend patients refer to specific paraclinical centers or specific physicians to receive additional services. Some patients consider these instructions and recommendations unnecessary. Physicians mention the high quality of their services of those centers or physicians compared to other centers and physicians as the reason for recommending those centers or physicians. In all these cases, some patients are worried about the possible conflict of interest between their treating physicians and the proposed paraclinical centers or physicians.
As reported by previous studies, today's socio-cultural expectations require physicians to understand patients’ feelings and show empathy [38]. This issue would be a challenge for physicians believing that they should maintain a professional distance from their patients in terms of emotions [39].
Most participating medical students and residents in this study stated that if they had received any practical or theoretical training in a predefined formal program, they would have made better relationships with patients and other members of the treatment team. In all, according to the participants of this study, the current situation of the PPR at TUOMS was not satisfying. Taking into account all reinforcing factors identified in this research could help in designing comprehensive educational interventions in this regard.
Similar to other qualitative studies, it was not possible to investigate any causal relationship between the PPR and the factors explored in this study. However, as the factors determining the PPR have been explored in our context, researchers can focus on the factors explored in this study in their future experimental studies.
Limitations
The target audiences of the 16 tips of the 38 proposed tips are only physicians. As previously mentioned, according to the results of a review study, physician-related factors have been less explored in previous studies. Therefore, we had limitations in comparing the results of this study on some physician-related factors with the results of other studies. Therefore, it is recommended that similar studies be conducted in other countries in the future, especially in countries with different contextual and socio-cultural factors, to be able to compare and synthesize the findings of qualitative studies.
Patients admitted to the wards and students participating in the study were repeatedly reassured that the content of their interviews would not be made available to their care providers or the people in charge of education at TUOMS in any way. However, considering some of their nonverbal behaviors, such as pausing or changing the course of their speech when they decided to refer to the existing weaknesses, one could have noticed that they were probably concerned about the possible reactions of their care providers or the people in charge of education to some of their statements. So, the possibility of such a bias in the participants’ answers has been present in this qualitative study, like other qualitative studies, albeit to a small extent.
Conclusion
Patient-centered communication can be characterized by honoring patients’ individuality, paying attention to patients’ needs, focusing on physicians’ proper personal characteristics in continuing medical education, enhancing physicians’ communication competencies, institutionalization of patient-focused care, creating trust-supported attitudes among patients, increasing physicians’ motivation, regulating physicians’ working context, serious attention to social and cultural inductions, making supportive organizational policies, and evaluating physicians’ professional responsibilities. Most of the characteristics of the PCC mentioned by the participants of this study can be the focus of some educational interventions to improve patient-physician relationships, even in similar Eastern societies.
Acknowledgements: We would like to extend our sincere gratitude to all patients and scholars for their invaluable participation in this study. Without their active participation, the study could not have been completed.
Ethical Permission: The ethical committee board at Tabriz University of Medical Sciences approved this study (The approval code number: IR.TBZMED.REC.1395.1129). All methods were performed in accordance with the relevant guidelines, regulations, and ethical standards of the responsible committee approving the research at Tabriz University of Medical Sciences and with the Declaration of Helsinki, as revised in 2000. Permission to attend in and out-patient settings was given by heads of departments. All participants provided written informed consent to participate. The aim and learning objectives of the study were clearly shared with participants. A unique code was assigned to each participant. The participants were told that all the research data would be saved confidential. They were granted the right to withdraw from the study whenever they wanted.
Conflict of Interests: The authors declare that they have no competing interests except for the point that the corresponding author, SGH, is the scientific editor of the HEHP.
Authors’ Contribution: Bagheri M (First Author), Introduction Writer/Main Researcher/Discussion Writer (35%); Somi MH (Second Author), Introduction Writer/Methodologist/Statistical Analyst/Discussion Writer (15%); Dehghani Gh (Third Author), Introduction Writer/Discussion Writer (15%); Ghaffarifar S (Fourth Author), Introduction Writer/Methodologist/Statistical Analyst/Discussion Writer (35%)
Funding: Tabriz University of Medical Sciences funded and supported this study. (Grant No.: 5/d/497328).
Article Type: Original Research |
Subject:
Health Education and Health Behavior
Received: 2022/11/13 | Accepted: 2023/03/2 | Published: 2023/03/17
Received: 2022/11/13 | Accepted: 2023/03/2 | Published: 2023/03/17
References
1. Shumway JM, Harden R. AMEE Guide No. 25: The assessment of learning outcomes for the competent and reflective physician. Med Teach. 2003;25(6):569-84. [Link] [DOI:10.1080/0142159032000151907]
2. Roter D. The enduring and evolving nature of the patient-physician relationship. Patient Educ Couns. 2000;39(1):5-15. [Link] [DOI:10.1016/S0738-3991(99)00086-5]
3. Ha JF, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010;10(1):38-43. [Link]
4. Swenson SL, Buell S, Zettler P, White M, Ruston DC, Lo B. Patient-centered communication. J Gen Intern Med. 2004;19(11):1069-79. [Link] [DOI:10.1111/j.1525-1497.2004.30384.x]
5. Kurtz SM. Doctor-patient communication: principles and practices. Can J Neurol Sci. 2002;29 Suppl 2:S23-9. [Link] [DOI:10.1017/S0317167100001906]
6. Shafati M, Zahedi MJ. Physician-patient relationship: ethnography of multiple patient visits at private offices of doctors. J Qual Res Health Sci. 2013;2(1):46-61. [Persian] [Link]
7. Robinson JH, Callister LC, Berry JA, Dearing KA. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract. 2008;20(12):600-7. [Link] [DOI:10.1111/j.1745-7599.2008.00360.x]
8. Siebinga VY, Driever EM, Stiggelbout AM, Brand PLP. Shared decision making, patient-centered communication and patient satisfaction - A cross-sectional analysis. Patient Educ Couns. 2022;105(7):2145-50. [Link] [DOI:10.1016/j.pec.2022.03.012]
9. Ghaffarifar S, Ghofranipour F, Ahmadi F, Khoshbaten M. Barriers to effective doctor-patient relationship based on PRECEDE PROCEED model. Glob J Health Sci. 2015;7(6):24-32. [Link] [DOI:10.5539/gjhs.v7n6p24]
10. Claramita M, Utarini A, Soebono H, Van Dalen J, Van der Vleuten C. Doctor-patient communication in a Southeast Asian setting: the conflict between ideal and reality. Adv Health Sci Educ Theory Pract. 2011;16(1):69-80. [Link] [DOI:10.1007/s10459-010-9242-7]
11. Guo C, Yan J, Zhao Y. Analysis of barriers on doctor-patient communication in China. Chinese Med Ethic. 2018;(6):845-50. [Link]
12. Møller JE, Kjaer LB, Helledie E, Nielsen LF, Malling BV. Transfer of communication teaching skills from university to the clinical workplace - does it happen? A mixed methods study. BMC Med Educ. 2021;21(1):433. [Link] [DOI:10.1186/s12909-021-02834-1]
13. Beran T. Advances in medical education: the importance of communication and collaboration. Can Med Educ J. 2012;3(1):e1-3. [Link] [DOI:10.36834/cmej.36593]
14. Ghaffarifar S, Khoshbaten M, Ghofranipour F, Kompani Mohammadi J. Residents' communication skills evaluation by OSCE: What Changes should be done in educational system? Shiraz E-Med J. 2013;14(4):e93961. [Link] [DOI:10.17795/semj16658]
15. Laidlaw TS, Kaufman DM, Macleod H, Sargeant J, Langille DB. Patients' satisfaction with their family physicians' communication skills: a Nova Scotia survey. Acad Med. 2001;76(10 Suppl):S77-9. [Link] [DOI:10.1097/00001888-200110001-00026]
16. Guo A, Wang P. The current state of doctors' communication skills in Mainland China from the perspective of doctors' self-evaluation and patients' evaluation: A cross-sectional study. Patient Educ Couns. 2021;104(7):1674-80. [Link] [DOI:10.1016/j.pec.2020.12.013]
17. Tavakol M, Murphy R, Torabi S. A needs assessment for a communication skills curriculum in Iran. Teach Learn Med. 2005;17(1):36-41. [Link] [DOI:10.1207/s15328015tlm1701_7]
18. Ministry of Health and Medical Education. The educational program of the general medical doctorate course [Internet]. Tehran: Educational Vice Site; 2017 [cited 2022 Nov 11]. Available from: https://hcmep.behdasht.gov.ir/uploads/369/doc/pezeshkiomoomi_96.pdf. [Link]
19. Nouri M, Ghaffarifar S, Sadeghi Bazargani H, Ghaffari R. Patients' satisfaction with medical residents'communication skills at the largest teaching and treatment center in North West Iran in 2016. Shiraz E-Med J. 2017;18(4):e60032. [Link]
20. Kuper A, Lingard L, Levinson W. Critically appraising qualitative research. BMJ. 2008;337:a1035. [Link] [DOI:10.1136/bmj.a1035]
21. Bengtsson M. How to plan and perform a qualitative study using content analysis. NursingPlus Open. 2016;2:8-14. [Link] [DOI:10.1016/j.npls.2016.01.001]
22. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277-88. [Link] [DOI:10.1177/1049732305276687]
23. Shaheen M, Pradhan S. Sampling in qualitative research. In: Gupta M, Shaheen M, Reddy KP, editors. Qualitative techniques for workplace data analysis. IGI Global; 2019. p. 25-51. [Link] [DOI:10.4018/978-1-5225-5366-3.ch002]
24. Mahoney J, Goertz G. The possibility principle: Choosing negative cases in comparative research. Am Polit Sci Rev. 2004;98(4):653-69. [Link] [DOI:10.1017/S0003055404041401]
25. Carter N, Bryant-Lukosius D, DiCenso A, Blythe J, Neville AJ. The use of triangulation in qualitative research. Oncol Nurs Forum. 2014;41(5):545-7. [Link] [DOI:10.1188/14.ONF.545-547]
26. Stalmeijer RE, Mcnaughton N, Van Mook WNIKKA. Using focus groups in medical education research: AMEE Guide No. 91. Med Teach. 2014;36(11):923-39. [Link] [DOI:10.3109/0142159X.2014.917165]
27. Institute for Patient- and Family-Centered Care. What is PFCC? [Internet]. Tehran: Institute for Patient- and Family-Centered Care; 2013 [cited 2022 Nov 11]. Available from: https://ipfcc.org/about/pfcc.html [Link]
28. Johnson JL, D. Adkins D, Chauvin S. A review of the quality indicators of rigor in qualitative research. Am J Pharm Educ. 2020;84(1):7120. [Link] [DOI:10.5688/ajpe7120]
29. Gómez G, Aillach E. Ways to improve the patient-physician relationship. Curr Opin Psychiatry. 2013;26(5):453-7. [Link] [DOI:10.1097/YCO.0b013e328363be50]
30. Pellegrini CA. Trust: the keystone of the patient-physician relationship. J Am Coll Surg. 2017;224(2):95-102. [Link] [DOI:10.1016/j.jamcollsurg.2016.10.032]
31. Rees C, Sheard C, McPherson A. Medical students' views and experiences of methods of teaching and learning communication skills. Patient Educ Couns. 2004;54(1):119-21. [Link] [DOI:10.1016/S0738-3991(03)00196-4]
32. Deniz S, Akbolat M, Çimen M, Ünal Ö. The mediating role of shared decision-making in the effect of the patient-physician relationship on compliance with treatment. J Patient Exp. 2021;8:23743735211018066. [Link] [DOI:10.1177/23743735211018066]
33. Donahue KE, Ashkin E, Pathman DE. Length of patient-physician relationship and patients' satisfaction and preventive service use in the rural south: a cross-sectional telephone study. BMC Fam Pract. 2005;6:40. [Link] [DOI:10.1186/1471-2296-6-40]
34. Kilbride MK, Joffe S. The new age of patient autonomy: implications for the patient-physician relationship. JAMA. 2018;320(19):1973-4. [Link] [DOI:10.1001/jama.2018.14382]
35. Paez KA, Allen JK, Beach MC, Carson KA, Cooper LA. Physician cultural competence and patient ratings of the patient-physician relationship. J Gen Intern Med. 2009;24(4):495-8. [Link] [DOI:10.1007/s11606-009-0919-7]
36. Siu JY-M. Communicating under medical patriarchy: gendered doctor-patient communication between female patients with overactive bladder and male urologists in Hong Kong. BMC Women Health 2015;15(1):44. [Link] [DOI:10.1186/s12905-015-0203-4]
37. Ishikawa H, Yamazaki Y. How applicable are western models of patient‐physician relationship in Asia? Changing patient‐physician relationship in contemporary Japan Int J Japanese Sociol. 2005;14(1):84-93. [Link] [DOI:10.1111/j.1475-6781.2005.00070.x]
38. Jeffrey D, Downie R. Empathy - can it be taught? J R Coll Physicians Edinb. 2016;46(2):107-12. [Link] [DOI:10.4997/jrcpe.2016.210]
39. Christie D, Glew S. A clinical review of communication training for haematologists and haemato-oncologists: a case of art versus science. Br J Haematol. 2017;178(1):11-9. [Link] [DOI:10.1111/bjh.14606]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |