



Volume 11, Issue 1 (2023)
Health Educ Health Promot 2023, 11(1): 3-10 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nabi Foodani M, Mohamadnejad Ostad F, Navab E, Bahrampouri S, Abbasi Dolatabadi Z. Self-care and Standard Precaution Observance in Intensive Care Nurses during COVID 19. Health Educ Health Promot 2023; 11 (1) :3-10
URL: http://hehp.modares.ac.ir/article-5-63080-en.html
URL: http://hehp.modares.ac.ir/article-5-63080-en.html

1- Department of Medical Surgical Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
2- Department of Anesthesiology, School of Nursing, North Khorasan University of Medical Sciences, Bojnurd, Iran
3- Department of Critical Care Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
2- Department of Anesthesiology, School of Nursing, North Khorasan University of Medical Sciences, Bojnurd, Iran
3- Department of Critical Care Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
Keywords: COVID-19 [MeSH], Epidemics [MeSH], Intensive Care [MeSH], Infectious Diseases [MeSH], Nurse [MeSH], Self-Care [MeSH], Personal Protective Equipment [MeSH]
Full-Text [PDF 1547 kb]
(779 Downloads)
| Abstract (HTML) (714 Views)
Full-Text: (295 Views)
Introduction
As a result of the COVID-19 pandemic, health care providers are today facing numerous obstacles and pressures. A substantial proportion of individuals with COVID-19 seek medical help in places, including hospitals, for a variety of life-threatening symptoms and issues. Staff shortages, limited personal protective equipment, out-of-role tasks, and worrying virus-related problems are some of the challenges in the health system [1]. One of the things that health system officials and members of the treatment team consider in these instances is protecting front-line healthcare staff [2]. Meanwhile, it is critical to safeguard the professional team that is responsible for giving care to patients who have been brought to the ICU (Intensive Care Unit). These staff, especially nurses, have the necessary knowledge, skills and experience to give critical care to their patients in stressful and difficult situations, using advanced equipment and critical thinking to save their lives [3]. As a result, one of the most significant steps in the management of the COVID-19 pandemic is to pay attention to sustaining and promoting human health resources in this area [2]. The nurses in the intensive care unit have the most exposure to the most severe and infected patients with COVID-19 because they spend the most time at the patient's bedside and perform procedures like suction, intubation, and cardiopulmonary resuscitation. Also, their work environment is one of the most polluted parts of the hospital. As a result, one of the pillars of medical services during the COVID-19 pandemic is the protection of nurses [4].
Individuals' self-care practices have a role in protecting and safeguarding personnel, especially nurses working in ICU in these situations. Self-care is a technique in which people use their knowledge, skills, and talents to enhance their health [5]. Physical, psychological, spiritual, emotional, and professional aspects of self-care can be used to examine self-care [6]. A healthy diet, exercise, a healthy lifestyle, organizational culture, and protection against occupational dangers such as biological and psychosocial hazards are all examples of nursing self-care to support their health [7]. Observing standard precautions is a part of ICU nurses' self-care to boost their safety during professional tasks [8]. The standard precautions are based on the most recent guidelines on self-care principles against occupational dangers, including infection management. While providing health treatment, basic precautions are done to reduce the risk of transmission of blood-borne diseases and other dangerous microbes [9]. Hand cleaning, the use of personal protective equipment (gloves, masks, goggles, gown) while performing procedures in close contact with the patient, and respiratory care with the creation of respiratory aerosols are all standard precautions for infectious diseases [10].
On the other hand, standard precautions are not always embraced by the nurses in ICUs setting and are impacted by several variables. In a study conducted in Cyprus on the factors affecting the observance of standard precautions among nurses, the lack of protective equipment and emergencies and enough time to use the equipment, and inefficient efficiency while performing procedures using protective equipment have been noted as barriers to standard precautions by nurses [11]. In addition, self-care is different among nurses in various fields and has not been considered by nurses to an acceptable level. Kong et al. showed that a significant proportion of healthcare providers in Wuhan developed mental health disorders during the epidemic. Support for this view is essential for staff, and self-care is not well done by nurses in this regard [12]. Jahangiri showed that nurses are at a low level in self-care [13].
COVID-19 affected the world, including Iran, which experienced six waves of patients up to November 10, 2021, according to available statistics. The above conditions have been more severe in some cities of the country due to their special characteristics compared to other parts. For example, Mashhad is one of the religious tourist cities of Iran [14].
Mashhad is a metropolis in northeastern Iran and the capital of Khorasan Razavi province, which is the second-largest city in Iran after Tehran [15]. Since the official announcement of the COVID-19 outbreak in the country, Mashhad has been declared five times a high-risk city in terms of infection and death [16]. Due to the specific pattern of the COVID-19 pandemic in Iran, the nurses working in ICUs get tired, and most of them get the disease at least once [17]. It is necessary to examine the various aspects of the activities of this group of nurses who specialize in this phenomenon in terms of self-care and standard precautions while caring for patients with COVID-19 due to their specialties and their special working setting for future action. Therefore, the present study aimed to examine the self-care and standard precaution observance in intensive care nurses during COVID-19.
Instruments and Methods
This descriptive-analytical study was conducted in Mashhad in 2020-2021. The sample size was calculated using the correlation analysis method in G*Power software version 3.1, taking into account the type 1 error of 5% and the power of the test at 80%. The minimum correlation level assumed is 0.3, which is a weak correlation level and results in calculating a high sample size. A total of 140 nurses were included in the study by the convenient sampling method. The inclusion criteria were willingness to participate in the study, nurses with at least a bachelor's degree, 6 months of experience in the intensive care unit before the onset of the COVID-19 outbreak, at least one month of activity in the intensive care unit during COVID-19 outbreak. The exclusion criterion was the change of the research unit during the research process. The study area was the teaching-therapeutic hospitals of Mashhad University of Medical Sciences, which were the hospitalization centre for COVID-19 patients.
The data were collected using three tools, including demographic survey questions, Self-Care Inventory-Revised (SCI-R), and Compliance with Standard Precautions Scale (CSPS).
The first tool was used to collect the data on age, sex, marital status, work experience in hospital, intensive care unit, and intensive care unit of Centre COVID, work experience in the private sector, level of education, employment status, shift type, history of affecting by COVID-19, quality, quantity, and place of personal protective equipment in each shift.
Self-Care Inventory-Revised (SCI-R) measures five dimensions of self-care (physical, spiritual, psychological, emotional, and professional). The scoring scale in this tool in each of the five dimensions was a 5-point Likert scale, and the answers to the questions were repeated from “frequently” to “it never happened to me”. The answers of “frequently”, “occasionally”, “rarely”, “never”, and “it never happened to me” had 5, 4, 3, 2, and 1 scores, respectively. The physical, psychological, emotional, professional, and spiritual self-care included 10, 7, 8, 10, and 8 questions. Therefore, this questionnaire consisted of 43 questions. The lowest score was 43, and the highest score was 215. The higher score indicates better self-care.
Compliance Standard Precautions Scale (CSPS) consisted of 20 questions. Out of 20 questions, 16 were positive, and four were negative (2, 4, 6, and 15), and answers to the questions were on a four-point Likert scale from "never" to "always". For 16 positive questions, only the answer "always" was given 1 point, the rest of the option was given 0 points, and for 4 negative questions, if the answer was "never", 1 point was given, and the other options were given 0 points. The highest and lowest scores in this tool were 0-20. The higher score showed the more standard indications.
Validity of the above tools was determined by the content validity method after translating. Then, the tool was provided to 10 experts in this field, and their opinions were applied to the tool. The study tools were provided to 20 nurses in the COVID-19 Intensive Care Unit, and questionnaires were completed to determine the reliability of self-care tools after obtaining informed written consent. Then, the questionnaires were given to the same people again after two weeks, and the questionnaires were completed for reliability. Pearson coefficient was calculated as 0.86.
In this study, participants were not included in the sampling process to determine the tool’s reliability. The questionnaires were provided to the research units in the form of Google Forms. The paper version of the tool was provided to the research units based on their willingness.
The collected data were entered into SPSS 20 software and statistically analyzed after testing their normal distribution using the Kolmogorov-Smirnov test. Parametric and nonparametric tests, including mean and standard deviation, simple regression, independent t-test, Kruskal Wallis test, and Mann-Whitney test, were used. P<0.05 was considered significant.
Findings
The mean age of the nurses was 32.34±5.977 years, of whom 62.1% were female, and 37.9% were male. In addition, 67% of the participating personnel were married, and 89.3% of the participants had a bachelor's degree. The night shift, with a frequency of 82 (58.6%), was the more common shift type, and was evening shift, with a frequency of 6 (4.3%), was the least frequent shift type (Table 1).
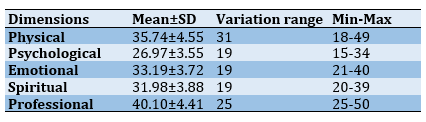
The highest self-care of the participants was in the professional dimension, with a mean of 40.10±4.41. (Table 2). The mean score of self-care in participants with a history of 16-20 years was higher than other participants. Moreover, the analysis of variance showed a significant difference between different groups in self-care according to the work experience in the hospital (p=0.039).
The highest and lowest scores of standard precautions were 20 and 3, and its mean score was 13.99±2.931, which indicates that the standard precautions were not at an acceptable level.
The mean rank of standard precautions in the night shift was higher than other shifts, with a mean of 88.91±3.23. The observed difference between the four mean scores based on the Kruskal-Wallis Test was significant (p=0.048), which indicates that the observance of standard precautions was different according to the shift type, and the standard precautions were higher in night shift participants.
Table 1) Univariate analysis between sociodemographic variables, self-care and standard precautions observance
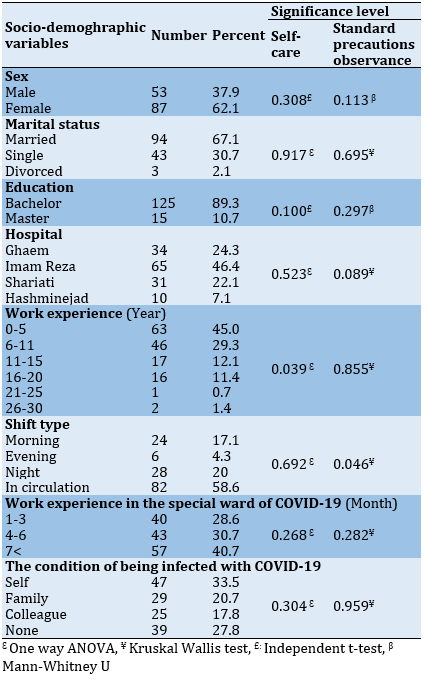
Table 2) Descriptive statistics related to participants' self-care dimensions
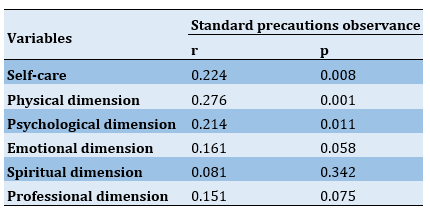
There was a positive and significant correlation between self-care and observance of standard precautions of nurses in the intensive care unit of Mashhad University of Medical Sciences in Covid-19 pandemic (p<0.05), which reveals that the observance of standard precautions increases by increasing the self-care score of nurses. Also, there was a positive and significant correlation between physical and psychological dimensions of self-care and standard precautions (p<0.05). However, no significant correlation was seen between emotional, spiritual, and professional dimensions and observance of standard precautions of nurses (p>0.05; Table 3).
Table 3) Correlation of self-care and its dimensions with standard precautions of nurses
The result of simple regression showed that the variable of self-care has a positive effect on the variable of Standard precautions observance
(Table 4).
Based on the regression model of the standard precautions observance variable and the self-care variable, a coefficient of determination equal to 0.041 was calculated, which shows that the self-care variable explains 4% of the changes related to the standard precautions observance by nurses in the ICU of Mashhad University of Medical Sciences hospitals during the Covid-19 pandemic (Table 5).
As a result of the COVID-19 pandemic, health care providers are today facing numerous obstacles and pressures. A substantial proportion of individuals with COVID-19 seek medical help in places, including hospitals, for a variety of life-threatening symptoms and issues. Staff shortages, limited personal protective equipment, out-of-role tasks, and worrying virus-related problems are some of the challenges in the health system [1]. One of the things that health system officials and members of the treatment team consider in these instances is protecting front-line healthcare staff [2]. Meanwhile, it is critical to safeguard the professional team that is responsible for giving care to patients who have been brought to the ICU (Intensive Care Unit). These staff, especially nurses, have the necessary knowledge, skills and experience to give critical care to their patients in stressful and difficult situations, using advanced equipment and critical thinking to save their lives [3]. As a result, one of the most significant steps in the management of the COVID-19 pandemic is to pay attention to sustaining and promoting human health resources in this area [2]. The nurses in the intensive care unit have the most exposure to the most severe and infected patients with COVID-19 because they spend the most time at the patient's bedside and perform procedures like suction, intubation, and cardiopulmonary resuscitation. Also, their work environment is one of the most polluted parts of the hospital. As a result, one of the pillars of medical services during the COVID-19 pandemic is the protection of nurses [4].
Individuals' self-care practices have a role in protecting and safeguarding personnel, especially nurses working in ICU in these situations. Self-care is a technique in which people use their knowledge, skills, and talents to enhance their health [5]. Physical, psychological, spiritual, emotional, and professional aspects of self-care can be used to examine self-care [6]. A healthy diet, exercise, a healthy lifestyle, organizational culture, and protection against occupational dangers such as biological and psychosocial hazards are all examples of nursing self-care to support their health [7]. Observing standard precautions is a part of ICU nurses' self-care to boost their safety during professional tasks [8]. The standard precautions are based on the most recent guidelines on self-care principles against occupational dangers, including infection management. While providing health treatment, basic precautions are done to reduce the risk of transmission of blood-borne diseases and other dangerous microbes [9]. Hand cleaning, the use of personal protective equipment (gloves, masks, goggles, gown) while performing procedures in close contact with the patient, and respiratory care with the creation of respiratory aerosols are all standard precautions for infectious diseases [10].
On the other hand, standard precautions are not always embraced by the nurses in ICUs setting and are impacted by several variables. In a study conducted in Cyprus on the factors affecting the observance of standard precautions among nurses, the lack of protective equipment and emergencies and enough time to use the equipment, and inefficient efficiency while performing procedures using protective equipment have been noted as barriers to standard precautions by nurses [11]. In addition, self-care is different among nurses in various fields and has not been considered by nurses to an acceptable level. Kong et al. showed that a significant proportion of healthcare providers in Wuhan developed mental health disorders during the epidemic. Support for this view is essential for staff, and self-care is not well done by nurses in this regard [12]. Jahangiri showed that nurses are at a low level in self-care [13].
COVID-19 affected the world, including Iran, which experienced six waves of patients up to November 10, 2021, according to available statistics. The above conditions have been more severe in some cities of the country due to their special characteristics compared to other parts. For example, Mashhad is one of the religious tourist cities of Iran [14].
Mashhad is a metropolis in northeastern Iran and the capital of Khorasan Razavi province, which is the second-largest city in Iran after Tehran [15]. Since the official announcement of the COVID-19 outbreak in the country, Mashhad has been declared five times a high-risk city in terms of infection and death [16]. Due to the specific pattern of the COVID-19 pandemic in Iran, the nurses working in ICUs get tired, and most of them get the disease at least once [17]. It is necessary to examine the various aspects of the activities of this group of nurses who specialize in this phenomenon in terms of self-care and standard precautions while caring for patients with COVID-19 due to their specialties and their special working setting for future action. Therefore, the present study aimed to examine the self-care and standard precaution observance in intensive care nurses during COVID-19.
Instruments and Methods
This descriptive-analytical study was conducted in Mashhad in 2020-2021. The sample size was calculated using the correlation analysis method in G*Power software version 3.1, taking into account the type 1 error of 5% and the power of the test at 80%. The minimum correlation level assumed is 0.3, which is a weak correlation level and results in calculating a high sample size. A total of 140 nurses were included in the study by the convenient sampling method. The inclusion criteria were willingness to participate in the study, nurses with at least a bachelor's degree, 6 months of experience in the intensive care unit before the onset of the COVID-19 outbreak, at least one month of activity in the intensive care unit during COVID-19 outbreak. The exclusion criterion was the change of the research unit during the research process. The study area was the teaching-therapeutic hospitals of Mashhad University of Medical Sciences, which were the hospitalization centre for COVID-19 patients.
The data were collected using three tools, including demographic survey questions, Self-Care Inventory-Revised (SCI-R), and Compliance with Standard Precautions Scale (CSPS).
The first tool was used to collect the data on age, sex, marital status, work experience in hospital, intensive care unit, and intensive care unit of Centre COVID, work experience in the private sector, level of education, employment status, shift type, history of affecting by COVID-19, quality, quantity, and place of personal protective equipment in each shift.
Self-Care Inventory-Revised (SCI-R) measures five dimensions of self-care (physical, spiritual, psychological, emotional, and professional). The scoring scale in this tool in each of the five dimensions was a 5-point Likert scale, and the answers to the questions were repeated from “frequently” to “it never happened to me”. The answers of “frequently”, “occasionally”, “rarely”, “never”, and “it never happened to me” had 5, 4, 3, 2, and 1 scores, respectively. The physical, psychological, emotional, professional, and spiritual self-care included 10, 7, 8, 10, and 8 questions. Therefore, this questionnaire consisted of 43 questions. The lowest score was 43, and the highest score was 215. The higher score indicates better self-care.
Compliance Standard Precautions Scale (CSPS) consisted of 20 questions. Out of 20 questions, 16 were positive, and four were negative (2, 4, 6, and 15), and answers to the questions were on a four-point Likert scale from "never" to "always". For 16 positive questions, only the answer "always" was given 1 point, the rest of the option was given 0 points, and for 4 negative questions, if the answer was "never", 1 point was given, and the other options were given 0 points. The highest and lowest scores in this tool were 0-20. The higher score showed the more standard indications.
Validity of the above tools was determined by the content validity method after translating. Then, the tool was provided to 10 experts in this field, and their opinions were applied to the tool. The study tools were provided to 20 nurses in the COVID-19 Intensive Care Unit, and questionnaires were completed to determine the reliability of self-care tools after obtaining informed written consent. Then, the questionnaires were given to the same people again after two weeks, and the questionnaires were completed for reliability. Pearson coefficient was calculated as 0.86.
In this study, participants were not included in the sampling process to determine the tool’s reliability. The questionnaires were provided to the research units in the form of Google Forms. The paper version of the tool was provided to the research units based on their willingness.
The collected data were entered into SPSS 20 software and statistically analyzed after testing their normal distribution using the Kolmogorov-Smirnov test. Parametric and nonparametric tests, including mean and standard deviation, simple regression, independent t-test, Kruskal Wallis test, and Mann-Whitney test, were used. P<0.05 was considered significant.
Findings
The mean age of the nurses was 32.34±5.977 years, of whom 62.1% were female, and 37.9% were male. In addition, 67% of the participating personnel were married, and 89.3% of the participants had a bachelor's degree. The night shift, with a frequency of 82 (58.6%), was the more common shift type, and was evening shift, with a frequency of 6 (4.3%), was the least frequent shift type (Table 1).
The highest self-care of the participants was in the professional dimension, with a mean of 40.10±4.41. (Table 2). The mean score of self-care in participants with a history of 16-20 years was higher than other participants. Moreover, the analysis of variance showed a significant difference between different groups in self-care according to the work experience in the hospital (p=0.039).
The highest and lowest scores of standard precautions were 20 and 3, and its mean score was 13.99±2.931, which indicates that the standard precautions were not at an acceptable level.
The mean rank of standard precautions in the night shift was higher than other shifts, with a mean of 88.91±3.23. The observed difference between the four mean scores based on the Kruskal-Wallis Test was significant (p=0.048), which indicates that the observance of standard precautions was different according to the shift type, and the standard precautions were higher in night shift participants.
Table 1) Univariate analysis between sociodemographic variables, self-care and standard precautions observance
Table 2) Descriptive statistics related to participants' self-care dimensions
There was a positive and significant correlation between self-care and observance of standard precautions of nurses in the intensive care unit of Mashhad University of Medical Sciences in Covid-19 pandemic (p<0.05), which reveals that the observance of standard precautions increases by increasing the self-care score of nurses. Also, there was a positive and significant correlation between physical and psychological dimensions of self-care and standard precautions (p<0.05). However, no significant correlation was seen between emotional, spiritual, and professional dimensions and observance of standard precautions of nurses (p>0.05; Table 3).
Table 3) Correlation of self-care and its dimensions with standard precautions of nurses
The result of simple regression showed that the variable of self-care has a positive effect on the variable of Standard precautions observance
(Table 4).
Based on the regression model of the standard precautions observance variable and the self-care variable, a coefficient of determination equal to 0.041 was calculated, which shows that the self-care variable explains 4% of the changes related to the standard precautions observance by nurses in the ICU of Mashhad University of Medical Sciences hospitals during the Covid-19 pandemic (Table 5).
Table 4) Result of simple regression

Table 5) Regression model to predict standard precautions observance of nurses in the intensive care unit

Table 5) Regression model to predict standard precautions observance of nurses in the intensive care unit
Discussion
Self-care nurses provide better quality care for patients and their families [18]. Nurses have the most important and main role in observing standard precautions because of their highest share in the treatment and care of patients. Practice, knowledge, and acceptance of nurses in compliance with standard precautions are essential to prevent nosocomial and occupational infections [10]. The study showed that nurses in intensive care units in critical situations such as the COVID-19 pandemic pay little attention to their self-care. However, self-care in the professional dimension is the essential dimension of self-care that receives relative attention, and self-care in the psychological dimension receives the least attention. The standard precautions in pandemic conditions of an infectious disease such as COVID-19 was not at an acceptable level, and there was a direct and positive correlation between self-care and observing standard precautions.
Sabourian et al. showed that the best self-care behavior was related to the individual's belief status, and the worst self-care behavior was related to the nutritional status of nurses, which is not consistent with the results of the present study [19]. Ahmadi et al. indicated that the mean score of self-care in the physical dimension (46.9±8.1) and mental dimension (47.7±8.0) was lower than in other dimensions of self-care. Moreover, the supportive relationships (51.6±9.1) were more than other dimensions, which these results are not consistent with the present study [20]. Jahangiri concluded that the highest self-care was in the spiritual dimension, with an average of 31.05, followed by the communication dimension, with an average of 24.94, and the lowest self-care was related to the overall balance, with an average of 4.51. These results are not consistent with those of the present study [13]. The inconsistency of the results of these three studies with the present study can be due to the non-uniformity of the nurses' work wards and also considering the critical conditions of Covid-19 in the present study.
Differences in the dimensions of self-care in various studies with the present study can show that in different situations, nurses' attention to the dimensions of self-care is different. In the present study, the psychological dimension had the lowest self-care among other dimensions, which could be due to the difficult and stressful conditions of the COVID-19 pandemic, which psychologically affected nurses. Kong et al. addressed the importance of the psychological dimension. In this study, 36% of medical staff had below-threshold mental health disorders, 34.4% had mild disorders, 22.4% had moderate disorders, and 6.2% had severe disorders. A significant proportion of health care providers in Wuhan developed mental health disorders during the epidemic, and support for this view is essential for staff [12] and is consistent with the results of the present study. In the present study, the psychological dimension had the lowest level of care among nurses.
The mean score of self-care in female participants (168.94) was higher than in males, but there was no significant difference between different groups in the level of self-care based on sex (p=0.308). According to Ahmadi et al., the self-care score was 245.3±32.3 in females and 244.1±35.4 in males. Lambda test results showed that sex could significantly affect self-care, which is not consistent with the present study [20]. This difference in the results can be due to the unequal ratio of women and men in the present study. In Ahmadi et al.'s study, the percentage of male and female participants was almost equal.
There was no significant relationship between self-care and demographic information, except for work experience, which was significantly (p=0.039) related to self-care. Jahangiri [13] found a statistically significant relationship between marital status, the number of children, and nurses' self-care, which is inconsistent with the results of the present study. This inconsistency can be due to the different conditions of the ICU ward compared to other hospital wards. However, there was no significant relationship between age, marital status, shift type, and self-care, which is consistent with the present study.
Sabourian et al. revealed that sex, marital status, shift type, and level of education had a significant relationship with self-care [19], which is not consistent with the present study. Ahmadi et al. found that the mean score of self-care in single, married, and divorced nurses was 243.7, 246.1, and 246.7 (p=0.18). Therefore, marital status could not be significantly related to self-care with a level of 95% confidence [20], which is consistent with the present study.
The maximum and minimum standard precaution score was 20 and 3, respectively, and the average precaution observance was 13.99±2.931. These values indicate that standard precautions were not at an acceptable level. Tajabadi et al. found that the minimum score was 30, and the maximum was 43. In addition, 66% of the units had moderate performance in observing standard precautions [10]. In addition, Alshammari et al. concluded that the observance of standard precautions among nursing students is moderate [21]. Kim and Park reported standard precautions in pre-graduate nursing students. In this study, the mean of standard precautions was 4.09, which indicates that the observance of precautions among nursing students in Korea is moderate and is not in line with the present study [22]. Vera et al. indicated that the general observance of standard precautions with an average of 4.28 was very high, which is not consistent with the present study [23]. The reason for this difference in the results can be due to the different cultures of self-care among nurses in different countries, as well as the ease of access to personal protective equipment. The reason for the unacceptability of standard precautions can be due to the lack of personal protective equipment during the COVID-19 pandemic compared to other normal conditions.
Demographic information such as age, sex, history, level of education, and employment status was not significantly related to standard precautions. The shift type had a significant relationship with the observance of standard precautions (P=0.046), and the observance of standard precautions in the night shift with an average of 86.91 was more than other shifts. Tajabadi et al. examined the level of standard precautions by nurses in special wards of Sabzevar hospitals. According to the results, 74% of the participants were female, 64% were in the age group of 22-30, and 58% of the total units were married. Most people (86%) had 1-7 years of work experience, and 84% had 1-5 years of experience in the ICU ward. According to the independent t-test, there was a negative relationship between performance and age and work experience in the ICU, but it was not significant. These results are consistent with those of the present study. The mean performance scores of men and women were 35.08 and 35.10, respectively, which were not significantly different, and this result is consistent with the present study. The performance scores of married and single people were 34.62 and 35.76, respectively, so there was no significant difference between the performance of married and single people, which is consistent with the present study [10]. In the study of Alshammari et al., standard precautions were significantly higher in female students than in males, and there was a significant relationship between sex and standard precautions. These results are not consistent with those of the present study [21].
There was a significant correlation between self-care and standard precautions of nurses in the intensive care unit of Mashhad University of Medical Sciences during the COVID-19 pandemic (p<0.05). A higher score in a self-care assessment and standard precautionary assessment tools indicates better self-care and more standard precaution. The positive value of the correlation coefficient (r=0.224) reveals that the observance of standard precautions increases by increasing the self-care score of nurses in the intensive care unit of Mashhad University of Medical Sciences. In other words, self-care has a significant effect on observing the standard precautions of nurses in the intensive care unit of hospitals of Mashhad University of Medical Sciences during the COVID-19 pandemic (p<0.05). There was a correlation between physical self-care and observance of standard precautions, so the observance of standard precautions increases with the increase of self-care in the physical dimension. Psychological self-care affected the standard precautions observance, so the standard precautions increase as psychological self-care increases. There was no correlation between emotional, spiritual, and professional self-care with standard precautions.
Our results also support the positive relationship between self-care and standard precaution observance found in previous studies. Nazario et al., in their study, examined occupational risks and adherence to standard precautions. According to the findings of this study, there is a positive relationship between self-care and adherence to precautions [24].
One of the limitations of this study is that there are very few studies on the self-care of nurses, especially intensive care unit nurses. Studies have been performed on standard precautions, but there is no study based on examining the relationship between these two variables. Therefore, there were limitations to collecting documents for analysis and interpretation. Attempts were made to use relevant articles as much as possible.
Future studies are recommended to identify effective strategies for promoting self-care and standard precautions by treatment team personnel, especially nurses. Nurses' knowledge about self-care, standard precautions, their effects, and the causes of self-care and standard precautions in nurses should be examined.
The results of the study revealed that self-care and standard precaution observance are not acceptable among nurses in COVID-19 conditions. Self-care and observance of standard precautions are important to maintain the health of nurses and the need for more physically and mentally healthy personnel, and the lack of human resource in the critical situation of COVID-19. Therefore, the results of this study can help policymakers, planners, health care members, and especially nurses to plan and promote the ICU nurses health in all aspects (physical, psychological, etc.).
Conclusion
Nurses in intensive care units in COVID-19 pandemic pay little attention to their self-care. Self-care in the professional dimension receives relative attention, and in the psychological dimension, receives the least attention. The standard precautions in COVID-19 pandemic is not at an acceptable level, and there is a direct and positive correlation between self-care and observing standard precautions.
Acknowledgments: The authors would like to thank the people who participated in this study.
Ethical Permission: Ethical considerations of the study included obtaining an ethics code from Tehran University of Medical Sciences (IR.TUMS.FNM.REC.1399.081), achieving the necessary referrals for sampling in the hospitals of Mashhad University of Medical Sciences, and gaining oral consent from the participants in the study. Ensuring the samples to keep personal information confidential and observing ethical principles in publishing research findings and all stages of the study are other cases in this field.
Conflict of interest: The authors declared no conflict of interest.
Authors' contributions: Nabi Foodani M (First Author), Introduction Writer/Main Researcher/Statistical Analyst (25%); Mohamadnejad Ostad F (Second Author), Main Researcher/Discussion Writer (25%); Navab E (Third Author), Assistant Researcher (15%); Bahrampouri S (Fourth Author), Statistical Analyst (10%); Abbasi Dolatabadi Z (Fifth Author), Methodologist/Main Researcher (25%)
Funding: This study is a part of a student thesis to obtain a master's degree in nursing which has been accepted in 2021.
Self-care nurses provide better quality care for patients and their families [18]. Nurses have the most important and main role in observing standard precautions because of their highest share in the treatment and care of patients. Practice, knowledge, and acceptance of nurses in compliance with standard precautions are essential to prevent nosocomial and occupational infections [10]. The study showed that nurses in intensive care units in critical situations such as the COVID-19 pandemic pay little attention to their self-care. However, self-care in the professional dimension is the essential dimension of self-care that receives relative attention, and self-care in the psychological dimension receives the least attention. The standard precautions in pandemic conditions of an infectious disease such as COVID-19 was not at an acceptable level, and there was a direct and positive correlation between self-care and observing standard precautions.
Sabourian et al. showed that the best self-care behavior was related to the individual's belief status, and the worst self-care behavior was related to the nutritional status of nurses, which is not consistent with the results of the present study [19]. Ahmadi et al. indicated that the mean score of self-care in the physical dimension (46.9±8.1) and mental dimension (47.7±8.0) was lower than in other dimensions of self-care. Moreover, the supportive relationships (51.6±9.1) were more than other dimensions, which these results are not consistent with the present study [20]. Jahangiri concluded that the highest self-care was in the spiritual dimension, with an average of 31.05, followed by the communication dimension, with an average of 24.94, and the lowest self-care was related to the overall balance, with an average of 4.51. These results are not consistent with those of the present study [13]. The inconsistency of the results of these three studies with the present study can be due to the non-uniformity of the nurses' work wards and also considering the critical conditions of Covid-19 in the present study.
Differences in the dimensions of self-care in various studies with the present study can show that in different situations, nurses' attention to the dimensions of self-care is different. In the present study, the psychological dimension had the lowest self-care among other dimensions, which could be due to the difficult and stressful conditions of the COVID-19 pandemic, which psychologically affected nurses. Kong et al. addressed the importance of the psychological dimension. In this study, 36% of medical staff had below-threshold mental health disorders, 34.4% had mild disorders, 22.4% had moderate disorders, and 6.2% had severe disorders. A significant proportion of health care providers in Wuhan developed mental health disorders during the epidemic, and support for this view is essential for staff [12] and is consistent with the results of the present study. In the present study, the psychological dimension had the lowest level of care among nurses.
The mean score of self-care in female participants (168.94) was higher than in males, but there was no significant difference between different groups in the level of self-care based on sex (p=0.308). According to Ahmadi et al., the self-care score was 245.3±32.3 in females and 244.1±35.4 in males. Lambda test results showed that sex could significantly affect self-care, which is not consistent with the present study [20]. This difference in the results can be due to the unequal ratio of women and men in the present study. In Ahmadi et al.'s study, the percentage of male and female participants was almost equal.
There was no significant relationship between self-care and demographic information, except for work experience, which was significantly (p=0.039) related to self-care. Jahangiri [13] found a statistically significant relationship between marital status, the number of children, and nurses' self-care, which is inconsistent with the results of the present study. This inconsistency can be due to the different conditions of the ICU ward compared to other hospital wards. However, there was no significant relationship between age, marital status, shift type, and self-care, which is consistent with the present study.
Sabourian et al. revealed that sex, marital status, shift type, and level of education had a significant relationship with self-care [19], which is not consistent with the present study. Ahmadi et al. found that the mean score of self-care in single, married, and divorced nurses was 243.7, 246.1, and 246.7 (p=0.18). Therefore, marital status could not be significantly related to self-care with a level of 95% confidence [20], which is consistent with the present study.
The maximum and minimum standard precaution score was 20 and 3, respectively, and the average precaution observance was 13.99±2.931. These values indicate that standard precautions were not at an acceptable level. Tajabadi et al. found that the minimum score was 30, and the maximum was 43. In addition, 66% of the units had moderate performance in observing standard precautions [10]. In addition, Alshammari et al. concluded that the observance of standard precautions among nursing students is moderate [21]. Kim and Park reported standard precautions in pre-graduate nursing students. In this study, the mean of standard precautions was 4.09, which indicates that the observance of precautions among nursing students in Korea is moderate and is not in line with the present study [22]. Vera et al. indicated that the general observance of standard precautions with an average of 4.28 was very high, which is not consistent with the present study [23]. The reason for this difference in the results can be due to the different cultures of self-care among nurses in different countries, as well as the ease of access to personal protective equipment. The reason for the unacceptability of standard precautions can be due to the lack of personal protective equipment during the COVID-19 pandemic compared to other normal conditions.
Demographic information such as age, sex, history, level of education, and employment status was not significantly related to standard precautions. The shift type had a significant relationship with the observance of standard precautions (P=0.046), and the observance of standard precautions in the night shift with an average of 86.91 was more than other shifts. Tajabadi et al. examined the level of standard precautions by nurses in special wards of Sabzevar hospitals. According to the results, 74% of the participants were female, 64% were in the age group of 22-30, and 58% of the total units were married. Most people (86%) had 1-7 years of work experience, and 84% had 1-5 years of experience in the ICU ward. According to the independent t-test, there was a negative relationship between performance and age and work experience in the ICU, but it was not significant. These results are consistent with those of the present study. The mean performance scores of men and women were 35.08 and 35.10, respectively, which were not significantly different, and this result is consistent with the present study. The performance scores of married and single people were 34.62 and 35.76, respectively, so there was no significant difference between the performance of married and single people, which is consistent with the present study [10]. In the study of Alshammari et al., standard precautions were significantly higher in female students than in males, and there was a significant relationship between sex and standard precautions. These results are not consistent with those of the present study [21].
There was a significant correlation between self-care and standard precautions of nurses in the intensive care unit of Mashhad University of Medical Sciences during the COVID-19 pandemic (p<0.05). A higher score in a self-care assessment and standard precautionary assessment tools indicates better self-care and more standard precaution. The positive value of the correlation coefficient (r=0.224) reveals that the observance of standard precautions increases by increasing the self-care score of nurses in the intensive care unit of Mashhad University of Medical Sciences. In other words, self-care has a significant effect on observing the standard precautions of nurses in the intensive care unit of hospitals of Mashhad University of Medical Sciences during the COVID-19 pandemic (p<0.05). There was a correlation between physical self-care and observance of standard precautions, so the observance of standard precautions increases with the increase of self-care in the physical dimension. Psychological self-care affected the standard precautions observance, so the standard precautions increase as psychological self-care increases. There was no correlation between emotional, spiritual, and professional self-care with standard precautions.
Our results also support the positive relationship between self-care and standard precaution observance found in previous studies. Nazario et al., in their study, examined occupational risks and adherence to standard precautions. According to the findings of this study, there is a positive relationship between self-care and adherence to precautions [24].
One of the limitations of this study is that there are very few studies on the self-care of nurses, especially intensive care unit nurses. Studies have been performed on standard precautions, but there is no study based on examining the relationship between these two variables. Therefore, there were limitations to collecting documents for analysis and interpretation. Attempts were made to use relevant articles as much as possible.
Future studies are recommended to identify effective strategies for promoting self-care and standard precautions by treatment team personnel, especially nurses. Nurses' knowledge about self-care, standard precautions, their effects, and the causes of self-care and standard precautions in nurses should be examined.
The results of the study revealed that self-care and standard precaution observance are not acceptable among nurses in COVID-19 conditions. Self-care and observance of standard precautions are important to maintain the health of nurses and the need for more physically and mentally healthy personnel, and the lack of human resource in the critical situation of COVID-19. Therefore, the results of this study can help policymakers, planners, health care members, and especially nurses to plan and promote the ICU nurses health in all aspects (physical, psychological, etc.).
Conclusion
Nurses in intensive care units in COVID-19 pandemic pay little attention to their self-care. Self-care in the professional dimension receives relative attention, and in the psychological dimension, receives the least attention. The standard precautions in COVID-19 pandemic is not at an acceptable level, and there is a direct and positive correlation between self-care and observing standard precautions.
Acknowledgments: The authors would like to thank the people who participated in this study.
Ethical Permission: Ethical considerations of the study included obtaining an ethics code from Tehran University of Medical Sciences (IR.TUMS.FNM.REC.1399.081), achieving the necessary referrals for sampling in the hospitals of Mashhad University of Medical Sciences, and gaining oral consent from the participants in the study. Ensuring the samples to keep personal information confidential and observing ethical principles in publishing research findings and all stages of the study are other cases in this field.
Conflict of interest: The authors declared no conflict of interest.
Authors' contributions: Nabi Foodani M (First Author), Introduction Writer/Main Researcher/Statistical Analyst (25%); Mohamadnejad Ostad F (Second Author), Main Researcher/Discussion Writer (25%); Navab E (Third Author), Assistant Researcher (15%); Bahrampouri S (Fourth Author), Statistical Analyst (10%); Abbasi Dolatabadi Z (Fifth Author), Methodologist/Main Researcher (25%)
Funding: This study is a part of a student thesis to obtain a master's degree in nursing which has been accepted in 2021.
Article Type: Descriptive & Survey |
Subject:
Self-Care
Received: 2022/07/22 | Accepted: 2023/01/1 | Published: 2023/01/30
Received: 2022/07/22 | Accepted: 2023/01/1 | Published: 2023/01/30
References
1. Li W, Khan AN. Investigating the impacts of information overload on psychological well-being of healthcare professionals: Role of COVID-19 stressor. Inquiry. 2022; 59:00469580221109677. [Link] [DOI:10.1177/00469580221109677]
2. Schaffer GE, Kilanowski L, Lee BE. A qualitative investigation of the impact of COVID-19 on United States' frontline health care workers and the perceived impact on their family members. Int J Environ Res Public Health. 2022;19(17):10483. [Link] [DOI:10.3390/ijerph191710483]
3. Webb S, Butler J, Williams E, Harbour K, Hammond N, Delaney A. Intensive care nurse practitioners in Australia: A description of a service model in an adult tertiary intensive care unit. Aust Crit Care. 2023;36(1):133-7. [Link] [DOI:10.1016/j.aucc.2022.10.017]
4. Chen W-Q, Ling W-H, Lu C-Y, Hao Y-T, Lin Z-N, Ling L, et al. Which preventive measures might protect health care workers from SARS? BMC Public Health. 2009;9:81. [Link] [DOI:10.1186/1471-2458-9-81]
5. Mehraeen E, Hayati B, Saeidi S, Heydari M, Seyedalinaghi S. Self-care instructions for people not requiring hospitalization for coronavirus disease 2019 (COVID-19). Arch Clin Infect Dis. 2020;15 (COVID-19):e102978. [Link] [DOI:10.5812/archcid.102978]
6. Martínez N, Connelly CD, Pérez A, Calero P. Self-care: A concept analysis. Int J Nurs Sci. 2021;8(4):418-25. [Link] [DOI:10.1016/j.ijnss.2021.08.007]
7. Ross A, Touchton-Leonard K, Perez A, Wehrlen L, Kazmi N, Gibbons S. Factors that influence health-promoting self-care in registered nurses: barriers and facilitators. ANS Adv Nurs Sci. 2019;42(4):358-73. [Link] [DOI:10.1097/ANS.0000000000000274]
8. Choi KR, Skrine Jeffers K, Cynthia Logsdon M. Nursing and the novel coronavirus: Risks and responsibilities in a global outbreak. J Adv Nurs. 2020;76(7):1486-7. [Link] [DOI:10.1111/jan.14369]
9. Cruz JP, Colet PC, Al-Otaibi JH, Soriano SS, Cacho GM, Cruz CP. Validity and reliability assessment of the Compliance with standard precautions scale arabic version in Saudi nursing students. J Infect Public Health. 2016;9(5):645-53. [Link] [DOI:10.1016/j.jiph.2016.01.010]
10. Tajabadi A, Parsaeimehr Z, Kashani E. Evaluation of compliance with standard precautions by ICU nurses of Sabzevar Hospitals. Sci J Nurs Midwifery Paramed Facul.2018;4(2):79-91. [Persian] [Link]
11. Efstathiou G, Papastavrou E, Raftopoulos V, Merkouris A. Factors influencing nurses' compliance with standard precautions in order to avoid occupational exposure to microorganisms: a focus group study. BMC Nurs. 2011;10:1. [Link] [DOI:10.1186/1472-6955-10-1]
12. Kang L, Ma S, Chen M, Yang J, Wang Y, Li Y, et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav Immun. 2020;87:11-7. [Link] [DOI:10.1016/j.bbi.2020.03.028]
13. Jahangiri M. Self - care strategies and its relationship with the professional quality of life of nurses working in educational hospitals affiliated to Tabriz and Sanandaj University of medical sciences in 2015. Tabriz Univ Med Sci. 2015. [Link]
14. Kalantar SH, Mortazavi SJ, Bagheri N, Manshadi SA, Moharrami A, Ariamloo P, et al. Prevalence of Coronavirus Disease-2019 among healthcare workers in Imam Khomeini Hospital Complex in Tehran, Iran. J Orthop Spine Trauma. 2020;6(2):30-2. [Link] [DOI:10.18502/jost.v6i2.4784]
15. Motagh M, Djamour Y, Walter T, Wetzel H-U, Zschau J, Arabi S. Land subsidence in Mashhad Valley, northeast Iran: Results from InSAR, levelling and GPS. Geophys J Int. 2007;168(2):518-26. [Link] [DOI:10.1111/j.1365-246X.2006.03246.x]
16. Irna. Mashhad also went through a red stage in terms of corona [Internet]. Tehran: Irna; 2021 [cited 2021 July 30]. Available from: https://www.irna.ir/news/83837807/. [Persian] [Link]
17. Kennedy A. ICN says worldwide death toll from COVID-19 among nurses estimated at 100 may be far higher [Internet]. International Council of Nurses; 2020 [cited 2021 Aug 19]. Available from: https://www.icn.ch/news/icn-says-worldwide-death-toll-covid-19-among-nurses-estimated-100-may-be-far-higher. [Link]
18. Chow J, Kalischuk RG. Self-care for caring practice: student nurses' perspectives. Int J Hum Caring. 2008;(3):31-7. [Link] [DOI:10.20467/1091-5710.12.3.31]
19. Sabourian Jouybari S, Mirani H, Jafar H, Motlagh F, Goudarzian A. Evaluating self-care behaviors in nurses of Mazandaran, Iran Cardiac Center in 2014. Tabari Biomed Stud Res J. 2016;2(2):36-43. [Link]
20. Ahmadi B, Rafiemanesh H, Shamlou R, Kor Y, Letafat Nezhad M, Mehtarpour M. Self-care behaviors and influential factors among nurses working in the hospitals of Tehran. Evid Based Health Policy Manag Econ. 2019;3(3):182-90. [Link] [DOI:10.18502/jebhpme.v3i3.1507]
21. Alshammar F, Cruz J, Alquwez N, Almazan J, Alsolam F, Alabdulaziz H, Felemban E. Compliance with standard precautions during clinical training of nursing students in Saudi Arabia: A multi-university study. J Infect Dev Countr. 2018; 12(11):937-45. [Link] [DOI:10.3855/jidc.10821]
22. Kim H, Park H. Compliance with infection prevention and control practice among prospective graduates of nursing school in South Korea. Int J Environ Res Public Health. 2021;18(5):2373. [Link] [DOI:10.3390/ijerph18052373]
23. Vera M, Nero F. Compliance with the standard precautions: An infection control measure of nurses in Ilocos Sur. Proceed Surabaya Int Health Confer. 2019;1(1):87-98. [Link]
24. Nazario EG, Camponogara S, Dias GL. Occupational risks and adherence to standard precautions in intensive care nursing work: workers' perceptions. Revista Brasileira de Saúde Ocupacional. 2017;42. [Link] [DOI:10.1590/2317-6369000009216]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |