



Volume 10, Issue 2 (2022)
Health Educ Health Promot 2022, 10(2): 359-367 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alirezaei S, Sharifi F, Latifnejad Roudsari R. Midwives’ Knowledge, Attitude and Practice towards COVID-19 Essential Health Care Services in Pregnancy, Childbirth, and Lactation. Health Educ Health Promot 2022; 10 (2) :359-367
URL: http://hehp.modares.ac.ir/article-5-60500-en.html
URL: http://hehp.modares.ac.ir/article-5-60500-en.html
1- Department of Midwifery, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran
2- Student Research Committee, Mashhad University of Medical Sciences, Mashhad, Iran
3- “Nursing and Midwifery Care Research Center” and “Department of Midwifery, School of Nursing and Midwifery”, Mashhad University of Medical Sciences, Mashhad, Iran
2- Student Research Committee, Mashhad University of Medical Sciences, Mashhad, Iran
3- “Nursing and Midwifery Care Research Center” and “Department of Midwifery, School of Nursing and Midwifery”, Mashhad University of Medical Sciences, Mashhad, Iran
Full-Text [PDF 904 kb]
(1154 Downloads)
| Abstract (HTML) (717 Views)
Table 2) Knowledge, attitude, and practice of midwives working in Mashhad regarding the provision of services related to COVID-19
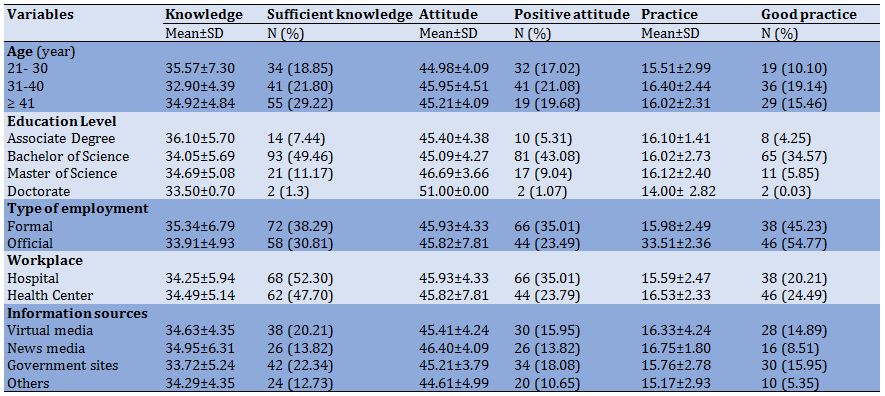
Table 3) Knowledge of midwives working in Mashhad regarding the provision of services related to COVID-19 (N=188)
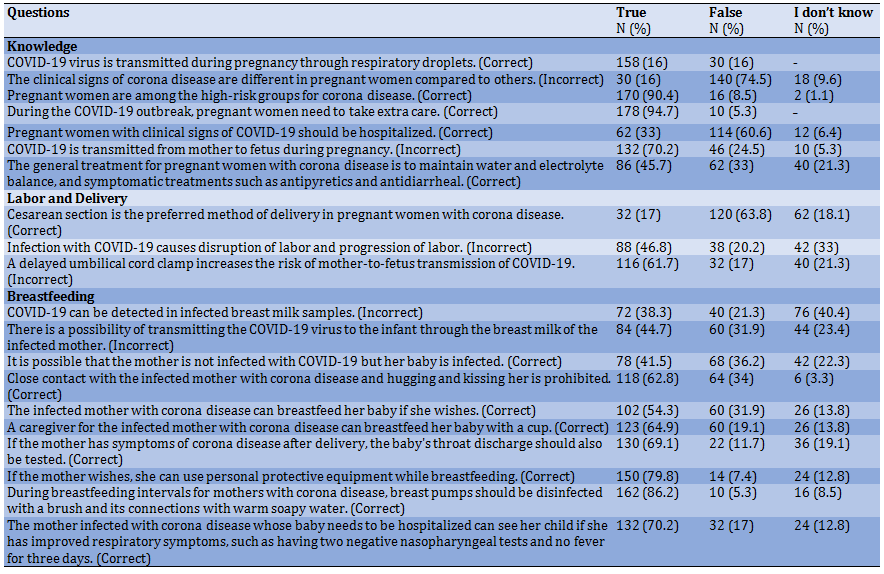
Table 4) Attitude of midwives working in Mashhad regarding the provision of services related to COVID-19 (N=188)
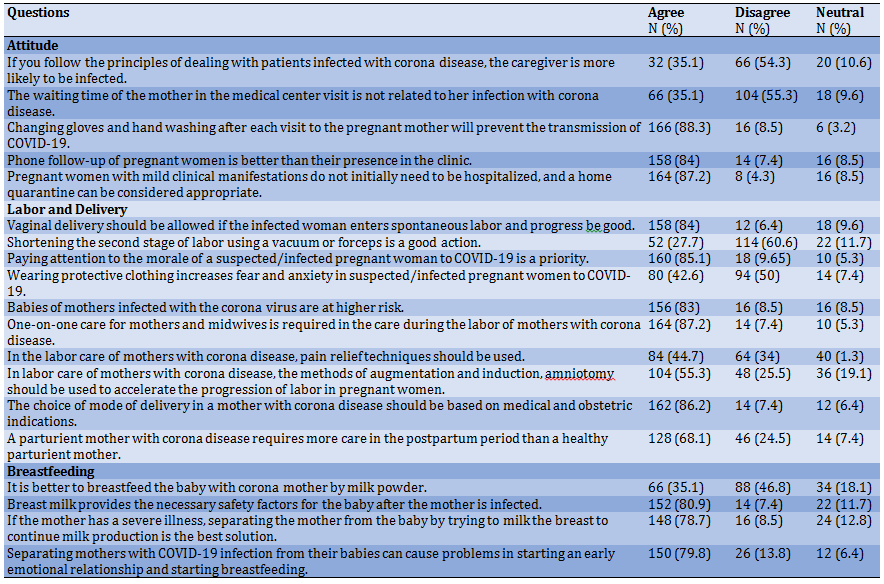
Table 5) Practice of midwives working in Mashhad regarding the provision of services related to COVID-19 (N=188)
The results of the Spearman test showed a positive and direct correlation between the variables such as midwives' place of work (p≤0.046; rs=0.14) and the status of employment (p≤0.028; rs=0.16). On the other hand, a negative and indirect correlation was reported between practice and available information sources (p≤0.01; rs=-0.18). Also, there was a positive and direct correlation between practice and knowledge (p≤0.01; rs=0.14), but no correlation was found between practice and attitude).
Discussion
The aim of this study was to examine the knowledge, attitude, and practice of midwives working in government centers in providing services related to COVID-19 during pregnancy, childbirth, and lactation.
The results of the present study showed that generally, the knowledge and attitude of the midwives about COVID-19 during pregnancy, childbirth, and lactation was moderate. While the men's knowledge score was not significantly different between the midwives working in different wards of the hospital or between the midwives working in hospitals or health centers. In a study by Homer et al. in Australia, the findings showed that midwives working in the private ward had good knowledge about COVID-19, and were looking for new information [30]. In another study by Simanjuntak et al. in the Bekasi region, the findings showed that midwives in this region had good knowledge in this field [31]. In the case of healthcare providers, the study by Uzuntarla in Turkey also showed that 85% of healthcare workers had a moderate level of knowledge about COVID-19, which is consistent with the findings of the present study; although 87% of them had a high attitude in this regard [32]. In a systematic review by Hesaraki et al., most health care providers had good knowledge and attitudes about dealing with the COVID-19 disease [33]. In addition, in the study in Utopia, Nigeria, and northern Uganda, health care workers had good knowledge and attitude about dealing with the COVID-19 virus [24, 34-36]. At the beginning of the present study, data collection started from the beginning of the COVID-19 epidemic, when the level of individuals' awareness was not yet sufficient, while the questionnaire used in the present study contained specialized questions in the field of COVID-19 disease during pregnancy, childbirth, and lactation. It seems that the type of questionnaire affects the response rate of participants and their scores. Studies focusing specifically on a group of health care providers, or focusing on a specific topic in the field of COVID-19, have reported low levels of knowledge, including the study by Tadesse et al., which focused on the knowledge, attitude, and practice of health workers in the proper use of face masks and its related factors in police health facilities in Adis Ababa, Ethiopia. They found that the level of knowledge and attitude towards the use of face masks was relatively low [37]. In addition, in the study conducted by Kulthe et al. in India on the evaluation of nursing students' knowledge, the results showed that the majority of participants (72%) had a moderate level of knowledge related to COVID-19 [38]. In the study by Jindal et al., regarding the knowledge, anxiety, and use of hydroxychloroquine prophylaxis among students and health care professionals about COVID-19, the results showed that knowledge about the proper use of personal protective equipment is low among all groups of health workers and students [39]. Based on this, it seems that obtaining the mean score in the knowledge and attitude of midwives working in government centers in Mashhad related to COVID-19 can be due to the specialization of the type of questionnaire. The highest positive attitude was among midwives working in urban health centers. It seems that in the present study since the participants included midwives working in different wards, their attitudes were affected by the sensitivity of the workplace and the possibility of dealing with patients with corona disease.
In the present study, although midwives' practice was very well in the field of personal protection in dealing with the coronavirus, in the study of Tadesse et al., the practice of health workers in the proper use of face masks was relatively low [37]. However, it is noteworthy that in the present study, less than half of the midwives had a positive and appropriate practice in dealing with a pregnant mother with corona disease. However, in the study of Simanjuntak et al., the findings showed that the midwives had good knowledge and implemented health care protocols well [31]. In addition, in the systematic review of Hesaraki et al., most health care providers had good practice in the field of COVID-19 [33]. In two studies, the practice and readiness of health care workers regarding COVID-19 were good [32, 34]. However, in the present study, according to the moderate knowledge of midwives in Mashhad in dealing with COVID-19, this type of practice was also expected and it seems that is related to the new emergence of COVID-19 and low experience of people when dealing with this disease in pregnant, delivered or lactating women infected with the virus. Another important issue that may have caused this discrepancy in the results is the use of different tools in measuring the knowledge, attitude, and practice of participants in different studies.
The limitation of the present study was that the study was performed at the beginning of the COVID-19 outbreak and the number of exposure and experience of the disease was limited. Another point is that because this disease is new, the information about it is constantly updated, and this may affect the level of knowledge and practice of individuals. The strong point of the study was conducting it in different health centers and evaluating the knowledge, attitude, and practice of midwives working at different levels of providing service from the health center to subspecialty hospitals.
With more time passing since the onset of the corona pandemic, it is recommended that further studies be conducted to assess the current knowledge, attitudes, and practice of health care providers and midwives regarding the COVID-19 epidemic.
Conclusion
Given the moderate level of midwifes' knowledge of the COVID-19 pandemic, it is essential that midwives increase their knowledge, so that they can implement COVID-19-related guidelines in midwifery services. Therefore, improving awareness through receiving health education, participating in scientific programs and in-service training, using up-to-date content on the website of the World Health Organization and other related organizations, as well as studying the evidence and achievements of research are some of the approaches that can be used by midwives during the COVID-19 outbreak to improve their knowledge, attitude and practice. To adequately answer to the prevalence of COVID-19, health officials and policymakers should provide the necessary resources so that health care providers and midwives can provide health care in a safe environment; and also design training programs, reward models, and employee registration to increase the desire of midwives to perform with high quality in high-risk groups of mothers and infants infected with COVID-19, especially during the pandemic. Due to the importance of midwives' practice, it is recommended that international standard tools be designed and used to measure the knowledge, attitude, and practice of midwives in dealing with and managing COVID-19 disease.
Acknowledgments: The authors thank the Vice Chancellor for Research and the Ethics Committee of the University of Medical Sciences and the National Corona Headquarters. They also thank all the participants for participating in this research.
Ethical Permissions: This article was approved by the Research Ethics Committee of Mashhad University Medical Sciences, with the code of ethics IR.MUMS.REC.1399.034.
Conflicts of interest: This study is taken from a research project entitled “Evaluation of knowledge, attitude and practice of midwives in Mashhad in providing services related to COVID-19 in pregnancy, childbirth and lactation”.
Authors’ Contributions: Alirezaei S (First author), Introduction writer/Methodologist/Statistical analyst/
Discussion writer (60%); Sharifi F (Second author), Assistant researcher (40%); Latifnejad Roudsari R (Third author), Introduction writer /Assistant researcher/
Discussion author (10%)
Funding/Source: Mashhad University of Medical Sciences financially supported this study from the budget related to COVID-19 disease projects (grant number 990022(.
Full-Text: (157 Views)
Introduction
Coronavirus outbreak is currently a major global health concern. In December 2019, Wuhan, Hubei Province, China, became the center of a pneumonia outbreak of unknown cause, raising a serious concern not only in China but also internationally. The disease has now become a pandemic [1-3]. It is reported that about 209 countries in the world are affected by COVID-19 [4]. In the current pandemic, health care professionals, are at the forefront of the virus and are relatively more exposed to the patients infected with the disease, and have made every effort to provide maximum care to patients with the disease. However, the direct participation of these specialists has affected their physical and mental health. Several recent studies have shown that primary care staff involved in the diagnosis, treatment, and direct care of patients with COVID-19 is associated with a higher risk of depressive symptoms, post-traumatic stress disorder, and other mental health issues. Lack of personal protective equipment, heavy workload, inadequate medication, fear of being infected with the disease, and lack of skilled training have put the front-line health care workers under unimaginable stress [5]. Due to the widespread prevalence, the number of deaths of front-line health care professionals has also increased [5, 6]. The danger was such that during the virus outbreak, some medical providers were reluctant to continue their treatment activity, some private centers were closed [7] and even some feared financial compensation due to working with high-risk patients and this was the reason for not wanting to care for patients with COVID-19 [8]. Prevention of COVID-19 is affected by several factors, one of which is knowledge. To date, knowledge about COVID-19 infection associated with pregnancy and fetus is still limited [9]. Management of pregnant women with COVID-19 can be a complex issue [3]. Now, it is not known to what extent COVID-19 causes problems during pregnancy or affects the newborn’s health after birth. Systematic reviews have shown that the disease may be associated with increased risks of preeclampsia, preterm delivery, and other adverse pregnancy outcomes [10-12]. In addition, it is not clear what pregnant women should do to prevent infection and treatment of the disease, or how much more care they need compared to the general population [13, 14]. It is also not clear to what extent, or to what intensity a pregnant woman with COVID-19 can transmit the virus, which causes COVID-19 during pregnancy or childbirth to her fetus or newborn [10, 15, 16]. In limited studies on women with COVID-19 and a similar coronavirus infection, such as Acute Respiratory Syndrome (SARS-CoV), the microorganism has not been detected in breast milk. However, it is not clear whether mothers with COVID-19 can transmit the virus through breast milk. There is much discussion on the role of breast milk in the development of the infant's immune system and protection against infection by other respiratory viruses, focusing on the anti-inflammatory role of antibodies, microbes, and viruses present in the infant and breast milk and its association with COVID-19 [10, 17-19]. One of the dangerous cases in epidemics is medical environments and transmission through the hospital and its staff [20]. In addition, the transmission of disease to health care workers has been one of the common features in cases of disease outbreaks such as SARS [21, 22]. Accordingly, the high level of knowledge and attitude, and practice of health care providers is one of the important issues in solving health problems. Psychologists believe that behavior is the result of a decision and a decision is based on knowledge and attitude. In other words, it is accepted that a person first knows or gathers information about things, then forms a feeling and tendency through the flow of thought, which may lead to acting the favorite behavior in action.
Knowledge or awareness through influencing a person's beliefs, interests, and actions increases his decision-making power and helps him to control his behavior. Thus, the principle of measuring attitudes, beliefs, and awareness can help to understand the behavioral stages that lead to changing health habits in a population [23]. In a cross-sectional study by Iyal et al. titled the knowledge and practice of Nigeria Kaduna State health care providers on prevention and control of infection during COVID-19 outbreaks, there was a positive correlation between the health care provider's knowledge of COVID-19 and preventive measures and controlling the infection [24]. In the study of Nashwan et al., it was found that the level of nurses' knowledge has a positive and significant relationship with nurses' desire to care for patients with COVID-19 [8]. Upadhyaya et al. in a study on the knowledge and understanding of COVID-19 health care personnel and desire to work during the outbreak of the disease in Nepal reported that 17.2% had insufficient knowledge about COVID-19 and 35.9% were reluctant to work during the pandemic [25]. In a meta-synthesis by Shorey & Valerie, pregnant women, midwives, and nurses experienced negative psychological responses during the epidemic. In addition, they expressed the need for more information, and emotional, and financial support during the epidemic [26]. In the study by Pallangyo et al. entitled the impact of COVID-19 on midwifes' practice in Kenya, Uganda, and Tanzania, the findings showed that maternal and neonatal mortality rates are consistently high in these countries, but the epidemic of COVID-19 has exacerbated this problem. However, continuing all efforts is essential to provide safe delivery and high-quality midwifery care and stop obtaining the goals of sustainable development [27].
In a cross-sectional study in Turkey by Yörük et al.
to study the relationship between mental resilience, job burnout, stress, and socio-demographic factors with depression in nurses and midwives during COVID‐19, the results showed that one-third of midwives and nurses had depressive symptoms, but the risk of depression in midwives was 1.92 times higher than nurses [28]. In this regard, attention to this group of health service providers as people who manage both their health and the health of mother and infant in the critical time of pandemic is very important. Also due to providing services for pregnant and postpartum women and guaranteeing the health of the community, the midwives should be the focus of attention in these sensitive moments.
The level of knowledge, attitude, and practice of midwives about the methods of prevention of infection and transmission of COVID-19 can be effective in the proper function and observing the principles of prevention and treatment in the field of disease. Therefore, based on the current world priority in solving the problems related to the COVID-19 pandemic, as well as the lack of a study available on the knowledge, attitude, and practice of midwives about COVID-19 pandemic in the country, the present study was performed to examine the knowledge, attitude and practice of midwives in Mashhad in providing essential health care services related to COVID-19 during pregnancy, childbirth, and lactation.
Instrument and Methods
The present study was a cross-sectional online survey, which was conducted in April 2020 in Mashhad, Iran. The study population included 360 midwives working in all teaching hospitals (Imam Reza (AS), Ghaem (AS), Hasheminejad, and Dr. Shariati hospitals) as well as all health centers (Health Center No. 1, 2, 3, 5, and Samen) in Mashhad, who participated in the research after informed consent. Invitations to participate in the study were sent to midwives working in different groups of hospitals or health centers who were already members of the WhatsApp service.
Data collection tools were designed and implemented online. The questionnaire consisted of two parts. The first part consisted of demographic data including 12 initial questions and the subsequent part included the questions measuring the knowledge, attitude, and practice of midwives. Knowledge-related questions included 18 three-choice questions (true, false, and I do not know) about clinical manifestations, methods of transmission, prevention, and control of COVID-19 during pregnancy, labor, delivery, and lactation) that one score was considered for each correct answer and zero for each wrong answer. The higher score showed the higher midwives' knowledge in this field. The attitude was assessed with 11 five-point Likert scale statements. Responses included strongly disagreed, disagreed, disagreed, agreed, and strongly agreed. In order to reduce the respondent's bias, some questions were designed negatively and with a reverse score. The practice was also assessed through 12 questions using a two-choice scale of always or never, about the measures needed during pregnancy, labor, and lactation in cases of COVID-19 exposure. One score was considered for each correct answer and zero for each wrong answer. Content validity was used to determine the validity of the self-structured questionnaire. Thus, the questionnaire, which was designed based on the objectives of the research through a review of scientific literature after the approval of the research team, was sent by e-mail to seven specialists (three reproductive health specialists, one gynecologist, one neonatologist, one infectious disease specialist and one statistician) and after review, the necessary corrections were made. Test-retest was used to determine the reliability of the questionnaire. In this way, the researchers sent the questionnaire to 10 subjects to answer, and after one week, the questionnaire was sent again to the same people and they were asked to complete it. The correlation coefficient was calculated based on Cronbach's alpha, which was 0.86.
The researchers started sampling after obtaining permission from the Vice Chancellor for Research, Mashhad University of Medical Sciences, and an introduction letter from Mashhad School of Nursing and Midwifery. The questionnaire was made using Porsline software, which is a new way of conducting digital surveys [29]. Then, the questionnaire link was sent to all identified and registered people via WhatsApp messenger. The participants were told to contact the researchers if there was any ambiguity in the questions and to leave the study whenever they wished if they were unwilling to continue answering.
Data analysis was performed by SPSS software version 25. Descriptive statistical methods, which included frequency, mean and standard deviation, were used to describe the characteristics of the subjects. Inferential statistical methods were used to analyze the relationship between knowledge, attitude, and practice with demographic variables. The level of first type error in all tests was considered 0.05.
Findings
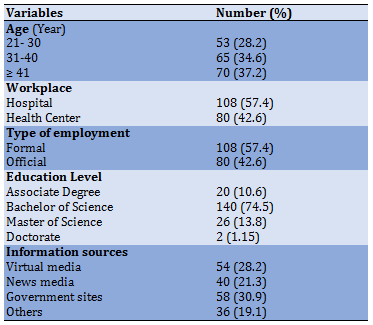
Out of 360 working midwives, 188 answered the questionnaire (response rate: 52.22%). The mean age of participants was 34.70±9.42 (out of 54). The highest number of participating midwives was those working in the maternity ward and the lowest number was the midwives working in rural health centers. Among the participants, 75.5% had a bachelor of science in midwifery. The main source used in COVID-19 was the international information resources and the Ministry of Health of Iran (Table 1).
Table 1) Frequency results of demographic information
The mean knowledge score of 188 respondents was 34.35±5.59. Among them, 69.1% (n=130) obtained 80% or more scores from sufficient knowledge about COVID-19 (Table 2).
There was no statistically significant difference between the mean knowledge score between the midwives working in different wards of the hospital or between midwives working in the hospital or health centers. Participants' level of knowledge was not related to their educational degree. The most correct answers showed the knowledge of midwives about the placement of pregnant and lactating mothers in the high-risk group, the possibility of vertical transmission, and methods of care and prevention. Wrong answers also indicated that midwives are insufficiently aware of the clinical signs of COVID-19 during pregnancy, lactation, and the management method of mothers with labor during lactation (Table 3).
The result of the Spearman test showed that only the demographic variable of age was positively and directly correlated with the level of midwives' knowledge so the older age of employees was associated with the higher level of their knowledge (p≤0.01; rs= 0.18).
The mean attitude score of 188 participants was 45.40±4.24 (out of 53) Among them, 110 (58.5%) midwives had a positive attitude towards COVID-19 (Table 2). The highest positive attitude was among midwives working in urban health centers (73.1%). The provided answers showed that the most positive attitudes were related to home quarantine, remote follow-up of pregnant and lactating mothers, and the protected separation of mothers from their infants. The negative attitude of midwives was regarding the use of vacuum and forceps during the delivery process, reducing pain techniques and feeding the infants of infected mothers with milk powder (Table 4).
The results of the Spearman test showed that attitude has a positive and direct correlation with the level of knowledge so that with increasing knowledge, the attitude of working midwives has also increased (p≤0.01; rs=0.25), but no correlation with other demographic variables was observed.
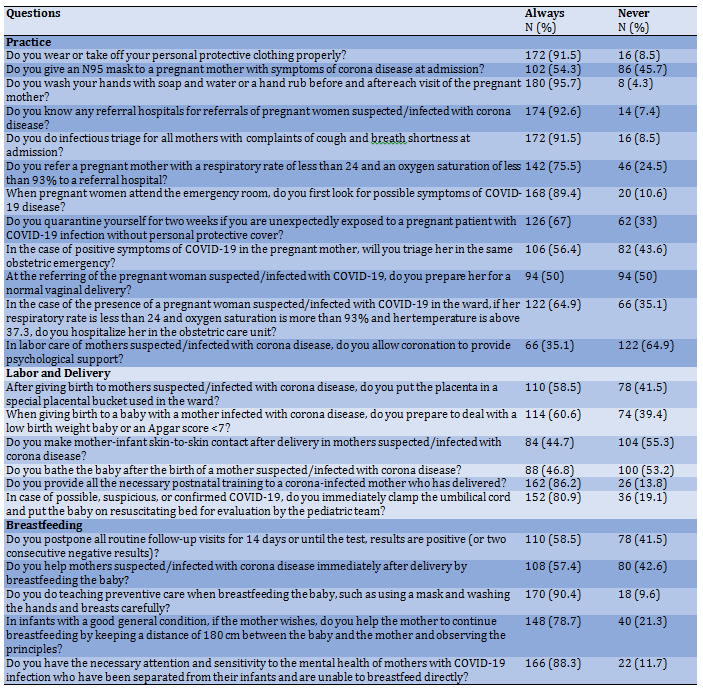
Moreover, 91.5% of midwives correctly used personal protective equipment and 95.5% of them observed hand hygiene in contact with the pregnant mother and her infant. However, only 44.7% of midwives had good practice in dealing with a pregnant mother with COVID-19. The results showed that the strength of midwives' practice was related to observing the principles of hand hygiene and the use of personal protective equipment, referral system, and hospital triage of infected mothers and providing the necessary training to mothers in the postpartum period. However, they reported weakness in their practice in providing psychological support to hospitalized infected mothers and providing services such as mother and infant skin-to-skin contact and breastfeeding immediately after delivery (Table 5).
Coronavirus outbreak is currently a major global health concern. In December 2019, Wuhan, Hubei Province, China, became the center of a pneumonia outbreak of unknown cause, raising a serious concern not only in China but also internationally. The disease has now become a pandemic [1-3]. It is reported that about 209 countries in the world are affected by COVID-19 [4]. In the current pandemic, health care professionals, are at the forefront of the virus and are relatively more exposed to the patients infected with the disease, and have made every effort to provide maximum care to patients with the disease. However, the direct participation of these specialists has affected their physical and mental health. Several recent studies have shown that primary care staff involved in the diagnosis, treatment, and direct care of patients with COVID-19 is associated with a higher risk of depressive symptoms, post-traumatic stress disorder, and other mental health issues. Lack of personal protective equipment, heavy workload, inadequate medication, fear of being infected with the disease, and lack of skilled training have put the front-line health care workers under unimaginable stress [5]. Due to the widespread prevalence, the number of deaths of front-line health care professionals has also increased [5, 6]. The danger was such that during the virus outbreak, some medical providers were reluctant to continue their treatment activity, some private centers were closed [7] and even some feared financial compensation due to working with high-risk patients and this was the reason for not wanting to care for patients with COVID-19 [8]. Prevention of COVID-19 is affected by several factors, one of which is knowledge. To date, knowledge about COVID-19 infection associated with pregnancy and fetus is still limited [9]. Management of pregnant women with COVID-19 can be a complex issue [3]. Now, it is not known to what extent COVID-19 causes problems during pregnancy or affects the newborn’s health after birth. Systematic reviews have shown that the disease may be associated with increased risks of preeclampsia, preterm delivery, and other adverse pregnancy outcomes [10-12]. In addition, it is not clear what pregnant women should do to prevent infection and treatment of the disease, or how much more care they need compared to the general population [13, 14]. It is also not clear to what extent, or to what intensity a pregnant woman with COVID-19 can transmit the virus, which causes COVID-19 during pregnancy or childbirth to her fetus or newborn [10, 15, 16]. In limited studies on women with COVID-19 and a similar coronavirus infection, such as Acute Respiratory Syndrome (SARS-CoV), the microorganism has not been detected in breast milk. However, it is not clear whether mothers with COVID-19 can transmit the virus through breast milk. There is much discussion on the role of breast milk in the development of the infant's immune system and protection against infection by other respiratory viruses, focusing on the anti-inflammatory role of antibodies, microbes, and viruses present in the infant and breast milk and its association with COVID-19 [10, 17-19]. One of the dangerous cases in epidemics is medical environments and transmission through the hospital and its staff [20]. In addition, the transmission of disease to health care workers has been one of the common features in cases of disease outbreaks such as SARS [21, 22]. Accordingly, the high level of knowledge and attitude, and practice of health care providers is one of the important issues in solving health problems. Psychologists believe that behavior is the result of a decision and a decision is based on knowledge and attitude. In other words, it is accepted that a person first knows or gathers information about things, then forms a feeling and tendency through the flow of thought, which may lead to acting the favorite behavior in action.
Knowledge or awareness through influencing a person's beliefs, interests, and actions increases his decision-making power and helps him to control his behavior. Thus, the principle of measuring attitudes, beliefs, and awareness can help to understand the behavioral stages that lead to changing health habits in a population [23]. In a cross-sectional study by Iyal et al. titled the knowledge and practice of Nigeria Kaduna State health care providers on prevention and control of infection during COVID-19 outbreaks, there was a positive correlation between the health care provider's knowledge of COVID-19 and preventive measures and controlling the infection [24]. In the study of Nashwan et al., it was found that the level of nurses' knowledge has a positive and significant relationship with nurses' desire to care for patients with COVID-19 [8]. Upadhyaya et al. in a study on the knowledge and understanding of COVID-19 health care personnel and desire to work during the outbreak of the disease in Nepal reported that 17.2% had insufficient knowledge about COVID-19 and 35.9% were reluctant to work during the pandemic [25]. In a meta-synthesis by Shorey & Valerie, pregnant women, midwives, and nurses experienced negative psychological responses during the epidemic. In addition, they expressed the need for more information, and emotional, and financial support during the epidemic [26]. In the study by Pallangyo et al. entitled the impact of COVID-19 on midwifes' practice in Kenya, Uganda, and Tanzania, the findings showed that maternal and neonatal mortality rates are consistently high in these countries, but the epidemic of COVID-19 has exacerbated this problem. However, continuing all efforts is essential to provide safe delivery and high-quality midwifery care and stop obtaining the goals of sustainable development [27].
In a cross-sectional study in Turkey by Yörük et al.
to study the relationship between mental resilience, job burnout, stress, and socio-demographic factors with depression in nurses and midwives during COVID‐19, the results showed that one-third of midwives and nurses had depressive symptoms, but the risk of depression in midwives was 1.92 times higher than nurses [28]. In this regard, attention to this group of health service providers as people who manage both their health and the health of mother and infant in the critical time of pandemic is very important. Also due to providing services for pregnant and postpartum women and guaranteeing the health of the community, the midwives should be the focus of attention in these sensitive moments.
The level of knowledge, attitude, and practice of midwives about the methods of prevention of infection and transmission of COVID-19 can be effective in the proper function and observing the principles of prevention and treatment in the field of disease. Therefore, based on the current world priority in solving the problems related to the COVID-19 pandemic, as well as the lack of a study available on the knowledge, attitude, and practice of midwives about COVID-19 pandemic in the country, the present study was performed to examine the knowledge, attitude and practice of midwives in Mashhad in providing essential health care services related to COVID-19 during pregnancy, childbirth, and lactation.
Instrument and Methods
The present study was a cross-sectional online survey, which was conducted in April 2020 in Mashhad, Iran. The study population included 360 midwives working in all teaching hospitals (Imam Reza (AS), Ghaem (AS), Hasheminejad, and Dr. Shariati hospitals) as well as all health centers (Health Center No. 1, 2, 3, 5, and Samen) in Mashhad, who participated in the research after informed consent. Invitations to participate in the study were sent to midwives working in different groups of hospitals or health centers who were already members of the WhatsApp service.
Data collection tools were designed and implemented online. The questionnaire consisted of two parts. The first part consisted of demographic data including 12 initial questions and the subsequent part included the questions measuring the knowledge, attitude, and practice of midwives. Knowledge-related questions included 18 three-choice questions (true, false, and I do not know) about clinical manifestations, methods of transmission, prevention, and control of COVID-19 during pregnancy, labor, delivery, and lactation) that one score was considered for each correct answer and zero for each wrong answer. The higher score showed the higher midwives' knowledge in this field. The attitude was assessed with 11 five-point Likert scale statements. Responses included strongly disagreed, disagreed, disagreed, agreed, and strongly agreed. In order to reduce the respondent's bias, some questions were designed negatively and with a reverse score. The practice was also assessed through 12 questions using a two-choice scale of always or never, about the measures needed during pregnancy, labor, and lactation in cases of COVID-19 exposure. One score was considered for each correct answer and zero for each wrong answer. Content validity was used to determine the validity of the self-structured questionnaire. Thus, the questionnaire, which was designed based on the objectives of the research through a review of scientific literature after the approval of the research team, was sent by e-mail to seven specialists (three reproductive health specialists, one gynecologist, one neonatologist, one infectious disease specialist and one statistician) and after review, the necessary corrections were made. Test-retest was used to determine the reliability of the questionnaire. In this way, the researchers sent the questionnaire to 10 subjects to answer, and after one week, the questionnaire was sent again to the same people and they were asked to complete it. The correlation coefficient was calculated based on Cronbach's alpha, which was 0.86.
The researchers started sampling after obtaining permission from the Vice Chancellor for Research, Mashhad University of Medical Sciences, and an introduction letter from Mashhad School of Nursing and Midwifery. The questionnaire was made using Porsline software, which is a new way of conducting digital surveys [29]. Then, the questionnaire link was sent to all identified and registered people via WhatsApp messenger. The participants were told to contact the researchers if there was any ambiguity in the questions and to leave the study whenever they wished if they were unwilling to continue answering.
Data analysis was performed by SPSS software version 25. Descriptive statistical methods, which included frequency, mean and standard deviation, were used to describe the characteristics of the subjects. Inferential statistical methods were used to analyze the relationship between knowledge, attitude, and practice with demographic variables. The level of first type error in all tests was considered 0.05.
Findings
Out of 360 working midwives, 188 answered the questionnaire (response rate: 52.22%). The mean age of participants was 34.70±9.42 (out of 54). The highest number of participating midwives was those working in the maternity ward and the lowest number was the midwives working in rural health centers. Among the participants, 75.5% had a bachelor of science in midwifery. The main source used in COVID-19 was the international information resources and the Ministry of Health of Iran (Table 1).
Table 1) Frequency results of demographic information
The mean knowledge score of 188 respondents was 34.35±5.59. Among them, 69.1% (n=130) obtained 80% or more scores from sufficient knowledge about COVID-19 (Table 2).
There was no statistically significant difference between the mean knowledge score between the midwives working in different wards of the hospital or between midwives working in the hospital or health centers. Participants' level of knowledge was not related to their educational degree. The most correct answers showed the knowledge of midwives about the placement of pregnant and lactating mothers in the high-risk group, the possibility of vertical transmission, and methods of care and prevention. Wrong answers also indicated that midwives are insufficiently aware of the clinical signs of COVID-19 during pregnancy, lactation, and the management method of mothers with labor during lactation (Table 3).
The result of the Spearman test showed that only the demographic variable of age was positively and directly correlated with the level of midwives' knowledge so the older age of employees was associated with the higher level of their knowledge (p≤0.01; rs= 0.18).
The mean attitude score of 188 participants was 45.40±4.24 (out of 53) Among them, 110 (58.5%) midwives had a positive attitude towards COVID-19 (Table 2). The highest positive attitude was among midwives working in urban health centers (73.1%). The provided answers showed that the most positive attitudes were related to home quarantine, remote follow-up of pregnant and lactating mothers, and the protected separation of mothers from their infants. The negative attitude of midwives was regarding the use of vacuum and forceps during the delivery process, reducing pain techniques and feeding the infants of infected mothers with milk powder (Table 4).
The results of the Spearman test showed that attitude has a positive and direct correlation with the level of knowledge so that with increasing knowledge, the attitude of working midwives has also increased (p≤0.01; rs=0.25), but no correlation with other demographic variables was observed.
Moreover, 91.5% of midwives correctly used personal protective equipment and 95.5% of them observed hand hygiene in contact with the pregnant mother and her infant. However, only 44.7% of midwives had good practice in dealing with a pregnant mother with COVID-19. The results showed that the strength of midwives' practice was related to observing the principles of hand hygiene and the use of personal protective equipment, referral system, and hospital triage of infected mothers and providing the necessary training to mothers in the postpartum period. However, they reported weakness in their practice in providing psychological support to hospitalized infected mothers and providing services such as mother and infant skin-to-skin contact and breastfeeding immediately after delivery (Table 5).
Table 2) Knowledge, attitude, and practice of midwives working in Mashhad regarding the provision of services related to COVID-19
Table 3) Knowledge of midwives working in Mashhad regarding the provision of services related to COVID-19 (N=188)
Table 4) Attitude of midwives working in Mashhad regarding the provision of services related to COVID-19 (N=188)
Table 5) Practice of midwives working in Mashhad regarding the provision of services related to COVID-19 (N=188)
The results of the Spearman test showed a positive and direct correlation between the variables such as midwives' place of work (p≤0.046; rs=0.14) and the status of employment (p≤0.028; rs=0.16). On the other hand, a negative and indirect correlation was reported between practice and available information sources (p≤0.01; rs=-0.18). Also, there was a positive and direct correlation between practice and knowledge (p≤0.01; rs=0.14), but no correlation was found between practice and attitude).
Discussion
The aim of this study was to examine the knowledge, attitude, and practice of midwives working in government centers in providing services related to COVID-19 during pregnancy, childbirth, and lactation.
The results of the present study showed that generally, the knowledge and attitude of the midwives about COVID-19 during pregnancy, childbirth, and lactation was moderate. While the men's knowledge score was not significantly different between the midwives working in different wards of the hospital or between the midwives working in hospitals or health centers. In a study by Homer et al. in Australia, the findings showed that midwives working in the private ward had good knowledge about COVID-19, and were looking for new information [30]. In another study by Simanjuntak et al. in the Bekasi region, the findings showed that midwives in this region had good knowledge in this field [31]. In the case of healthcare providers, the study by Uzuntarla in Turkey also showed that 85% of healthcare workers had a moderate level of knowledge about COVID-19, which is consistent with the findings of the present study; although 87% of them had a high attitude in this regard [32]. In a systematic review by Hesaraki et al., most health care providers had good knowledge and attitudes about dealing with the COVID-19 disease [33]. In addition, in the study in Utopia, Nigeria, and northern Uganda, health care workers had good knowledge and attitude about dealing with the COVID-19 virus [24, 34-36]. At the beginning of the present study, data collection started from the beginning of the COVID-19 epidemic, when the level of individuals' awareness was not yet sufficient, while the questionnaire used in the present study contained specialized questions in the field of COVID-19 disease during pregnancy, childbirth, and lactation. It seems that the type of questionnaire affects the response rate of participants and their scores. Studies focusing specifically on a group of health care providers, or focusing on a specific topic in the field of COVID-19, have reported low levels of knowledge, including the study by Tadesse et al., which focused on the knowledge, attitude, and practice of health workers in the proper use of face masks and its related factors in police health facilities in Adis Ababa, Ethiopia. They found that the level of knowledge and attitude towards the use of face masks was relatively low [37]. In addition, in the study conducted by Kulthe et al. in India on the evaluation of nursing students' knowledge, the results showed that the majority of participants (72%) had a moderate level of knowledge related to COVID-19 [38]. In the study by Jindal et al., regarding the knowledge, anxiety, and use of hydroxychloroquine prophylaxis among students and health care professionals about COVID-19, the results showed that knowledge about the proper use of personal protective equipment is low among all groups of health workers and students [39]. Based on this, it seems that obtaining the mean score in the knowledge and attitude of midwives working in government centers in Mashhad related to COVID-19 can be due to the specialization of the type of questionnaire. The highest positive attitude was among midwives working in urban health centers. It seems that in the present study since the participants included midwives working in different wards, their attitudes were affected by the sensitivity of the workplace and the possibility of dealing with patients with corona disease.
In the present study, although midwives' practice was very well in the field of personal protection in dealing with the coronavirus, in the study of Tadesse et al., the practice of health workers in the proper use of face masks was relatively low [37]. However, it is noteworthy that in the present study, less than half of the midwives had a positive and appropriate practice in dealing with a pregnant mother with corona disease. However, in the study of Simanjuntak et al., the findings showed that the midwives had good knowledge and implemented health care protocols well [31]. In addition, in the systematic review of Hesaraki et al., most health care providers had good practice in the field of COVID-19 [33]. In two studies, the practice and readiness of health care workers regarding COVID-19 were good [32, 34]. However, in the present study, according to the moderate knowledge of midwives in Mashhad in dealing with COVID-19, this type of practice was also expected and it seems that is related to the new emergence of COVID-19 and low experience of people when dealing with this disease in pregnant, delivered or lactating women infected with the virus. Another important issue that may have caused this discrepancy in the results is the use of different tools in measuring the knowledge, attitude, and practice of participants in different studies.
The limitation of the present study was that the study was performed at the beginning of the COVID-19 outbreak and the number of exposure and experience of the disease was limited. Another point is that because this disease is new, the information about it is constantly updated, and this may affect the level of knowledge and practice of individuals. The strong point of the study was conducting it in different health centers and evaluating the knowledge, attitude, and practice of midwives working at different levels of providing service from the health center to subspecialty hospitals.
With more time passing since the onset of the corona pandemic, it is recommended that further studies be conducted to assess the current knowledge, attitudes, and practice of health care providers and midwives regarding the COVID-19 epidemic.
Conclusion
Given the moderate level of midwifes' knowledge of the COVID-19 pandemic, it is essential that midwives increase their knowledge, so that they can implement COVID-19-related guidelines in midwifery services. Therefore, improving awareness through receiving health education, participating in scientific programs and in-service training, using up-to-date content on the website of the World Health Organization and other related organizations, as well as studying the evidence and achievements of research are some of the approaches that can be used by midwives during the COVID-19 outbreak to improve their knowledge, attitude and practice. To adequately answer to the prevalence of COVID-19, health officials and policymakers should provide the necessary resources so that health care providers and midwives can provide health care in a safe environment; and also design training programs, reward models, and employee registration to increase the desire of midwives to perform with high quality in high-risk groups of mothers and infants infected with COVID-19, especially during the pandemic. Due to the importance of midwives' practice, it is recommended that international standard tools be designed and used to measure the knowledge, attitude, and practice of midwives in dealing with and managing COVID-19 disease.
Acknowledgments: The authors thank the Vice Chancellor for Research and the Ethics Committee of the University of Medical Sciences and the National Corona Headquarters. They also thank all the participants for participating in this research.
Ethical Permissions: This article was approved by the Research Ethics Committee of Mashhad University Medical Sciences, with the code of ethics IR.MUMS.REC.1399.034.
Conflicts of interest: This study is taken from a research project entitled “Evaluation of knowledge, attitude and practice of midwives in Mashhad in providing services related to COVID-19 in pregnancy, childbirth and lactation”.
Authors’ Contributions: Alirezaei S (First author), Introduction writer/Methodologist/Statistical analyst/
Discussion writer (60%); Sharifi F (Second author), Assistant researcher (40%); Latifnejad Roudsari R (Third author), Introduction writer /Assistant researcher/
Discussion author (10%)
Funding/Source: Mashhad University of Medical Sciences financially supported this study from the budget related to COVID-19 disease projects (grant number 990022(.
Article Type: Descriptive & Survey |
Subject:
Health Promotion Approaches
Received: 2022/02/6 | Accepted: 2022/04/12 | Published: 2022/06/15
Received: 2022/02/6 | Accepted: 2022/04/12 | Published: 2022/06/15
References
1. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. lancet. 2020;395(10223):470-3. [Link] [DOI:10.1016/S0140-6736(20)30185-9]
2. Health World Organization. Coronavirus disease (COVID-19) situation reports. Geneva: Health World Organization; 2020. [Link]
3. Sahu KK, Lal A, Mishra AK. COVID-2019 and pregnancy: a plea for transparent reporting of all cases. Acta Obstet Gynecol Scand. 2020;99(7):951. [Link] [DOI:10.1111/aogs.13850]
4. Hussain I, Majeed A, Imran I, Ullah M, Hashmi FK, Saeed H, et al. Knowledge, attitude, and practices toward COVID-19 in primary healthcare providers: a cross-sectional study from three tertiary care hospitals of Peshawar, Pakistan. J Community Health. 2021;46(3):441-9. [Link] [DOI:10.1007/s10900-020-00879-9]
5. Das S, Singh T, Varma R, Arya YK. Death and mourning process in frontline health care professionals and their families during COVID-19. Front Psychiatry. 2021;12:624428. [Link] [DOI:10.3389/fpsyt.2021.624428]
6. World Health Organization. World Health Organization COVID-19 essential supplies forecasting tool (COVID-19 ESFT): an overview of the structure, methodology, and assumptions used: interim guidance, 7 April 2021. Geneva: World Health Organization; 2021. [Link]
7. Tysiąc-Miśta M, Dziedzic A. The attitudes and professional approaches of dental practitioners during the COVID-19 outbreak in Poland: a cross-sectional survey. Int J Environ Res Public Health. 2020;17(13):4703. [Link] [DOI:10.3390/ijerph17134703]
8. Nashwan AJ, Abujaber AA, Mohamed AS, Villar RC, Al‐Jabry MM. Nurses' willingness to work with COVID‐19 patients: the role of knowledge and attitude. Nurs Open. 2021;8(2):695-701. [Link] [DOI:10.1002/nop2.674]
9. Johar SA. Knowledge relations of midwives to the handling of corona virus infection (COVID-19) on maternity mothers in hospital X. STRADA JURNAL ILMIAH KESEHATAN. 2020;9(1):297-302. [Link] [DOI:10.30994/sjik.v9i1.324]
10. Berveiller P, Guerby P, Garabedian C. COVID19 and breastfeeding: not that simple. J Hum Lact. 2020;36(2):369-70. [Link] [DOI:10.1177/0890334420917102]
11. Wei SQ, Bilodeau-Bertrand M, Liu S, Auger N. The impact of COVID-19 on pregnancy outcomes: a systematic review and meta-analysis. CMAJ. 2021;193(16):E540-8. [Link] [DOI:10.1503/cmaj.202604]
12. Elsaddig M, Khalil A. Effects of the COVID pandemic on pregnancy outcomes. Best Pract Res Clin Obstet Gynaecol. 2021;73:125-36. [Link] [DOI:10.1016/j.bpobgyn.2021.03.004]
13. Pountoukidou A, Potamiti-Komi M, Sarri V, Papapanou M, Routsi E, Tsiatsiani AM, et al. Management and prevention of COVID-19 in pregnancy and pandemic obstetric care: a review of current practices. Healthcare (Basel). 2021;9(4):467. [Link] [DOI:10.3390/healthcare9040467]
14. Larki M, Sharifi F, Latifnejad Roudsari R. Women's reproductive health and rights through the lens of the COVID-19 pandemic. Sultan Qaboos Univ Med J. 2021;21(2):e166-71. [Link] [DOI:10.18295/squmj.2021.21.02.003]
15. Vardhelli V, Pandita A, Pillai A, Badatya SK. Perinatal COVID-19: review of current evidence and practical approach towards prevention and management. Europ J Pediatr. 2021;180(4):1009-31. [Link] [DOI:10.1007/s00431-020-03866-3]
16. Lokot M, Avakyan Y. Intersectionality as a lens to the COVID-19 pandemic: implications for sexual and reproductive health in development and humanitarian contexts. Sex Reprod Health Matters. 2020;28(1):1764748. [Link] [DOI:10.1080/26410397.2020.1764748]
17. Latifnejad Roudsari R. The possibility of COVID-19 vertical transmission: could it be excluded?. J Midwifery Reprod Health. 2020;8(3):2264-6. [Persian] [Link]
18. Vassilopoulou E, Feketea G, Koumbi L, Mesiari C, Berghea EC, Konstantinou GN. Breastfeeding and COVID-19: from nutrition to immunity. Front immunol. 2021;12:661806. [Link] [DOI:10.3389/fimmu.2021.661806]
19. Larki M, Sharifi F, Latifnejad Roudsari R. Models of maternity care for pregnant women during the COVID-19 pandemic. East Mediterr Health J. 2020;26(9):994-8. [Link] [DOI:10.26719/emhj.20.097]
20. Memish ZA, Zumla AI, Assiri A. Middle East respiratory syndrome coronavirus infections in health care workers. N En J Med. 2013;369(9):884-6. [Link] [DOI:10.1056/NEJMc1308698]
21. Peiris JSM, Chu CM, Cheng VCC, Chan KS, Hung IFN, Poon LLM, et al. Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: a prospective study. Lancet. 2003;361(9371):1767-72. [Link] [DOI:10.1016/S0140-6736(03)13412-5]
22. Cheng PKC, Wong DA, Tong LKL, Ip SM, Lo ACT, Lau CS, et al. Viral shedding patterns of coronavirus in patients with probable severe acute respiratory syndrome. Lancet. 2004;363(9422):1699-700. [Link] [DOI:10.1016/S0140-6736(04)16255-7]
23. Abaszadeh F, Eslami J, Bazrafcan L. Knowledge, attitude, and performance of operating room personnel about occupational exposure to blood-borne infections. J Adv Pharm Educ Res. 2020;4:6. [Link]
24. Iyal HA, Ishaku SG, Zakari A, Ibrahim S, Olasinde T, Ejembi CL, et al. Knowledge and practice of Kaduna state health care providers on infection prevention and control during COVID-19 pandemic. J Med Basic Scic Res. 2021;1(1):27-41. [Link]
25. Upadhyaya DP, Paudel R, Acharya D, Khoshnood K, Lee K, Park JH, et al. Frontline healthcare workers' knowledge and perception of COVID-19, and willingness to work during the pandemic in Nepal. Healthcare 2020;8(4):554. [Link] [DOI:10.3390/healthcare8040554]
26. Shorey S, Chan V. Lessons from past epidemics and pandemics and a way forward for pregnant women, midwives and nurses during COVID-19 and beyond: A meta-synthesis. Midwifery. 2020;90:102821. [Link] [DOI:10.1016/j.midw.2020.102821]
27. Pallangyo E, Nakate MG, Maina R, Fleming V. The impact of COVID-19 on midwives' practice in Kenya, Uganda and Tanzania: A reflective account. Midwifery. 2020;89:102775. [Link] [DOI:10.1016/j.midw.2020.102775]
28. Yörük S, Güler D. The relationship between psychological resilience, burnout, stress, and sociodemographic factors with depression in nurses and midwives during the COVID‐19 pandemic: a cross‐sectional study in Turkey. Perspect Psychiatr Care. 2021;57(1):390-8. [Link] [DOI:10.1111/ppc.12659]
29. Beigzadeh A, Adibi P, Bahaadinbeigy K, Yamani N. Strategies for teaching in clinical rounds: A systematic review of the literature. J Res Med Sci. 2019;24:33. [Link] [DOI:10.4103/jrms.JRMS_460_18]
30. Homer CS, Davies-Tuck M, Dahlen HG, Scarf VL. The impact of planning for COVID-19 on private practising midwives in Australia. Women Birth. 2021;34(1):e32-7. [Link] [DOI:10.1016/j.wombi.2020.09.013]
31. Simanjuntak H, Rohmah HN. Relationship practical experince and knowledge with implementing health protocol during pandemic COVID-19 among midwives in Bekasi district. Adv Health Sci Res. 2020 Nov. [Link] [DOI:10.2991/ahsr.k.201125.035]
32. Uzuntarla Y, Ceyhan S. Knowledge, attitude and behavior towards COVID-19 among the Turkish healthcare workers. J Clin Med Kaz. 2020;6(60):93-8. [Link] [DOI:10.23950/jcmk/9271]
33. Hesaraki M, Akbarizadeh M, Ahmadidarrehsima S, Moghadam MP, Izadpanah F. Knowledge, attitude, practice and clinical recommendations of health care workers towards COVID-19: a systematic review. Rev Environ Health. 2021;36(3):345-57. [Link] [DOI:10.1515/reveh-2020-0099]
34. Kanu S, James PB, Jawo Bah A, Alimamy Kabba J, Salieu Kamara M, Elleanor Williams CE, et al. Healthcare workers' knowledge, attitude, practice and perceived health facility preparedness regarding COVID-19 in Sierra Leone. J Multidiscip Healthc. 2021;14:67-80. [Link] [DOI:10.2147/JMDH.S287156]
35. Kassie BA, Adane A, Tilahun YT, Kassahun EA, Ayele AS, Belew AK. Knowledge and attitude towards COVID-19 and associated factors among health care providers in Northwest Ethiopia. PloS One. 2020;15(8):e0238415. [Link] [DOI:10.1371/journal.pone.0238415]
36. Amanya SB, Nyeko R, Obura B, Acen J, Nabasirye C, Nakaziba R, et al. Knowledge and compliance with COVID-19 infection prevention and control measures among health workers in regional referral hospitals in Northern Uganda: A cross-sectional online survey. F1000Research. 2021;10(136):136. [Link] [DOI:10.12688/f1000research.51333.2]
37. Tadesse T, Tesfaye T, Alemu T, Haileselassie W. Healthcare worker's knowledge, attitude, and practice of proper face mask utilization, and associated factors in police health facilities of Addis Ababa, Ethiopia. J Multidiscip Healthc. 2020;13:1203-13. [Link] [DOI:10.2147/JMDH.S277133]
38. Kulthe V. A study to assess the basic knowledge about Corona virus (COVID-19) among undergraduate nursing students in selected educational institution in India. Int J Curr Res. 2020. [Link]
39. Jindal V, Mittal S, Kaur T, Bansal AS, Kaur P, Kaur G, et al. Knowledge, anxiety and the use of hydroxychloroquine prophylaxis among health care students and professionals regarding COVID-19 pandemic. Adv Respir Med. 2020;88(6):520-30. [Link] [DOI:10.5603/ARM.a2020.0163]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |