



Volume 10, Issue 3 (2022)
Health Educ Health Promot 2022, 10(3): 603-608 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Haghdoost Z, Bostani Khalesi Z, Maroufizadeh S. Effect of an Educational Program Based on the BASNEF Model on Women Sexual Health. Health Educ Health Promot 2022; 10 (3) :603-608
URL: http://hehp.modares.ac.ir/article-5-60464-en.html
URL: http://hehp.modares.ac.ir/article-5-60464-en.html
1- Social Determinants of Health Research Center, Guilan University of Medical Sciences, Rasht, Iran
2- Department of Midwifery, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran
3- Department of Statistics, School of Health, Guilan University of Medical Sciences, Rasht, Iran
2- Department of Midwifery, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran
3- Department of Statistics, School of Health, Guilan University of Medical Sciences, Rasht, Iran
Full-Text [PDF 923 kb]
(961 Downloads)
| Abstract (HTML) (823 Views)
Full-Text: (128 Views)
Introduction
Sexual health is one of the main aspects of people’s health and the basis of physical-emotional health and well-being of individuals, couples, and families, affecting all people at all ages and all stages of life [1]. In addition, sexual health not only plays a critical role in the family’s overall health and hygiene but also is expressed as a need and strategy to achieve the millennium development goals [2]. Promoting sexual health, similar to other aspects of health, requires full and continuous access to information, educational opportunities, as well as basic support through interconnected and effective social activities in the fields of prioritizations, decision-making, and planning strategies and their implementation to achieve better health [3], and all individuals, social groups, health care providers, and the government are responsible for it [4]. Sexual health education is the process of empowering individuals to increase control over their sexual health and aims to improve the sexual health of the general population, especially vulnerable groups [5]. Sexual health education focuses on maintaining or developing sexual health, prevention/treatment, and care, and works to build a secure structure in a supportive environment, access information and life skills, and create opportunities to choose healthy options [6]. Individuals cannot reach their maximum sexual health capacity unless they have control over these components [7].
However, despite the importance of this issue and the emphasis of the World Health Organization (WHO) on sexual health education as a human right and a necessity for development, there is still no comprehensive program for sexual health education in Iran [8], and many of individuals’ needs in this area have remained unanswered [9].
In recent years, the transfer of Western culture and thoughts to Iran has exposed Iranian culture to changing behavioral values and patterns, which the spread of divorce and sexually transmitted diseases have been among its consequences [10]. The increase in these consequences in Iranians is an alarm making it necessary to provide sexual health education to inform, correct attitudes, and prevent these harms [11].
Having a suitable and capable model for behavior change has a special priority to have effective education in the field of health [12]. Choosing a health education model is also the first step in the process of designing an educational program [5]. In conducting educational interventions aiming to change behavior, the use of behavioral theories such as the behavioral intention model, the beliefs, attitudes, subjective norms, and enabling factors (BASNEF) model, and predisposing, reinforcing, and enabling constructs in the educational/environmental diagnosis and evaluation (PRECEDE) model can create a potential capacity for the effectiveness of these educations [13]. Today, one of the most practical educational models for creating and changing behavior around the world, especially in developing countries, is the BASNEF model [14]. This model is applied to study behavior, plan to change it, and determine the factors that are influential in individuals’ decision to perform a behavior [13]. Factors affecting behavior in this model include beliefs, attitudes, subjective norms, and enabling factors, and the word BASNEF is made up of the initial letters of the mentioned words [12].
Despite the importance of promoting sexual health, especially in women, an educational program is not yet provided comprehensively, organized, or based on a specific educational model and pattern, and most women do not gain the ability to understand the information they receive during the educational program. Therefore, creating a comprehensive program to promote sexual health based on an educational model seems essential. This study aimed to determine the effect of educational intervention based on the BASNEF model on promoting the sexual health of married women of reproductive age.
Material and Methods
This research was a quasi-experimental study (educational intervention) in which 52 eligible married women of reproductive age participated. In the present study, the sample size was calculated using G*Power statistical software version 3/1. To determine the sample size, the first type error was considered 0.05, and the second type error (power 0.8) was considered 0.2. According to the above information, the sample size was 26 people in each group, which given the possible loss of samples and for increasing the accuracy of the study, 40 people were finally included in each group the study (Figure1).
Sampling was performed using the stratified random cluster sampling method. First, 24 comprehensive health centers under the auspices of Guilan University of Medical Sciences, Rasht, Iran, were classified into four clusters based on 4 geographical regions north, south, east, and west. Then, using a table of random numbers, 4 centers were selected by allocating 1 center in each region according to the allocated ratio. Within each center, married women of reproductive age referring to that center were divided into the intervention and control groups using the table of random numbers if they met the inclusion criteria. The inclusion criteria included living with a spouse, having reading and writing literacy, no history of attending training or counseling classes focused on sexual function, not using alcohol and drugs, not having chronic diseases, not using medications that affect sexual function, not having known mental and psychological illnesses, not taking drugs affecting individuals’ sexual function, having a cell phone and using text messages or social networks, and not studying in medical fields. Spouse death, divorce, pregnancy, pregnancy, breastfeeding, and unwillingness to continue participating in the study at any stage of the educational intervention were the exclusion criteria. Participants were recruited via advertisements (posters) in comprehensive health centers. We compared eligible married women of reproductive age in the intervention group (n=26 individuals) to married women of reproductive age in the control group (n=26 individuals). The sexual health educational content based on the BASNEF model(4 sessions of two hours) by a faculty member researcher, was recorded through the camtasia2020 software, and then per week was sent to the participants of the intervention group via email or virtual systems (Telegram, WhatsApp, etc.).
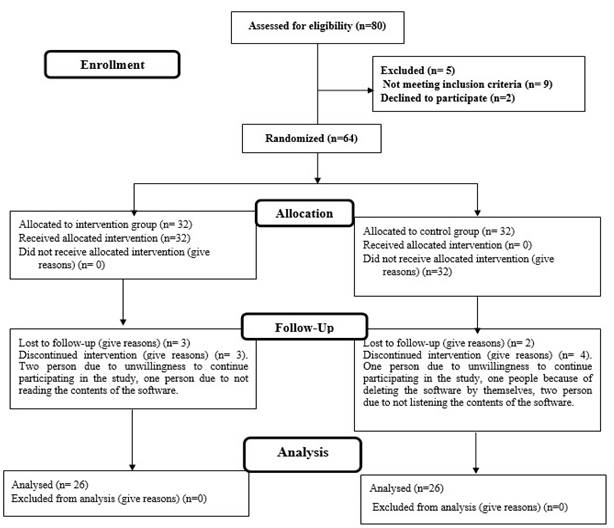
Figure 1) Consort flow diagram
Sexual health is one of the main aspects of people’s health and the basis of physical-emotional health and well-being of individuals, couples, and families, affecting all people at all ages and all stages of life [1]. In addition, sexual health not only plays a critical role in the family’s overall health and hygiene but also is expressed as a need and strategy to achieve the millennium development goals [2]. Promoting sexual health, similar to other aspects of health, requires full and continuous access to information, educational opportunities, as well as basic support through interconnected and effective social activities in the fields of prioritizations, decision-making, and planning strategies and their implementation to achieve better health [3], and all individuals, social groups, health care providers, and the government are responsible for it [4]. Sexual health education is the process of empowering individuals to increase control over their sexual health and aims to improve the sexual health of the general population, especially vulnerable groups [5]. Sexual health education focuses on maintaining or developing sexual health, prevention/treatment, and care, and works to build a secure structure in a supportive environment, access information and life skills, and create opportunities to choose healthy options [6]. Individuals cannot reach their maximum sexual health capacity unless they have control over these components [7].
However, despite the importance of this issue and the emphasis of the World Health Organization (WHO) on sexual health education as a human right and a necessity for development, there is still no comprehensive program for sexual health education in Iran [8], and many of individuals’ needs in this area have remained unanswered [9].
In recent years, the transfer of Western culture and thoughts to Iran has exposed Iranian culture to changing behavioral values and patterns, which the spread of divorce and sexually transmitted diseases have been among its consequences [10]. The increase in these consequences in Iranians is an alarm making it necessary to provide sexual health education to inform, correct attitudes, and prevent these harms [11].
Having a suitable and capable model for behavior change has a special priority to have effective education in the field of health [12]. Choosing a health education model is also the first step in the process of designing an educational program [5]. In conducting educational interventions aiming to change behavior, the use of behavioral theories such as the behavioral intention model, the beliefs, attitudes, subjective norms, and enabling factors (BASNEF) model, and predisposing, reinforcing, and enabling constructs in the educational/environmental diagnosis and evaluation (PRECEDE) model can create a potential capacity for the effectiveness of these educations [13]. Today, one of the most practical educational models for creating and changing behavior around the world, especially in developing countries, is the BASNEF model [14]. This model is applied to study behavior, plan to change it, and determine the factors that are influential in individuals’ decision to perform a behavior [13]. Factors affecting behavior in this model include beliefs, attitudes, subjective norms, and enabling factors, and the word BASNEF is made up of the initial letters of the mentioned words [12].
Despite the importance of promoting sexual health, especially in women, an educational program is not yet provided comprehensively, organized, or based on a specific educational model and pattern, and most women do not gain the ability to understand the information they receive during the educational program. Therefore, creating a comprehensive program to promote sexual health based on an educational model seems essential. This study aimed to determine the effect of educational intervention based on the BASNEF model on promoting the sexual health of married women of reproductive age.
Material and Methods
This research was a quasi-experimental study (educational intervention) in which 52 eligible married women of reproductive age participated. In the present study, the sample size was calculated using G*Power statistical software version 3/1. To determine the sample size, the first type error was considered 0.05, and the second type error (power 0.8) was considered 0.2. According to the above information, the sample size was 26 people in each group, which given the possible loss of samples and for increasing the accuracy of the study, 40 people were finally included in each group the study (Figure1).
Sampling was performed using the stratified random cluster sampling method. First, 24 comprehensive health centers under the auspices of Guilan University of Medical Sciences, Rasht, Iran, were classified into four clusters based on 4 geographical regions north, south, east, and west. Then, using a table of random numbers, 4 centers were selected by allocating 1 center in each region according to the allocated ratio. Within each center, married women of reproductive age referring to that center were divided into the intervention and control groups using the table of random numbers if they met the inclusion criteria. The inclusion criteria included living with a spouse, having reading and writing literacy, no history of attending training or counseling classes focused on sexual function, not using alcohol and drugs, not having chronic diseases, not using medications that affect sexual function, not having known mental and psychological illnesses, not taking drugs affecting individuals’ sexual function, having a cell phone and using text messages or social networks, and not studying in medical fields. Spouse death, divorce, pregnancy, pregnancy, breastfeeding, and unwillingness to continue participating in the study at any stage of the educational intervention were the exclusion criteria. Participants were recruited via advertisements (posters) in comprehensive health centers. We compared eligible married women of reproductive age in the intervention group (n=26 individuals) to married women of reproductive age in the control group (n=26 individuals). The sexual health educational content based on the BASNEF model(4 sessions of two hours) by a faculty member researcher, was recorded through the camtasia2020 software, and then per week was sent to the participants of the intervention group via email or virtual systems (Telegram, WhatsApp, etc.).
Figure 1) Consort flow diagram
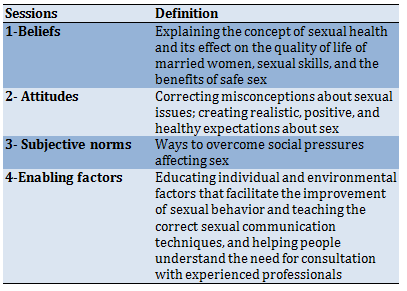
Data collection tools included a demographic information questionnaire (age, age of spouse, education level, education level of spouse, employment status, occupation of spouse, duration of marriage, and economic status) and a researcher-made questionnaire based on BASNEF structures. The BASNEF questionnaire is composed of 37 items in 6 subscales including knowledge questions (15 items) that refer to the knowledge about the concept of sexual health and its effect on the quality of life of married women. Behavioral beliefs questions (5 items) refer to the individual beliefs about outcomes of unhealthy sexual behavior, and the importance of sexual skills in marital satisfaction). Attitude questions (6 items) refer to the attitude one has toward the positive and respectful approach to sexuality and sexual relationships importance of misconceptions and the role of positive, and healthy expectations in sexual health. Subjective norms questions (6 items) evaluate the importance of approving or disapproving important referents about behavior and ways to overcome social pressures affecting sex, sexually transmitted infections (STIs); unwanted pregnancies; unsafe abortions, etc.). Enabling factors questions (2 items) refer to evaluating characteristics of the environment that facilitate or impede healthy behavior and behavioral intention questions (5 items: the perceived likelihood of performing the behavior). Questions of behavioral beliefs, attitudes, and subjective norms in the form of a 5-point Likert scale, strongly agree (5 points) to strongly disagree (1 point) and questions of awareness in the form of each question have 4 options with only one correct answer and enabling factors in the form of yes/ no and to some extent in order (3, 2, 1) were scored. To design questionnaires and extract questions, the available sources and focused group discussions with several experts were used. The demographic information form was given to 8 faculty members to check the face validity, and after applying the viewpoints, the final correction was made to it. To determine the face validity of the questionnaire, two qualitative and quantitative methods of face validity were used. To evaluate the quantitative content validity, “content validity ratio” and “content validity index” were used. The reliability of the instrument was confirmed by two methods of determining internal consistency and test-retest. The total content validity index and the total content validity ratio of the questionnaire were obtained at 0.92 and 0.87, respectively. The reliability of the instrument was confirmed by Cronbach’s alpha coefficient of 0.882, and the stability of the instrument after retesting was confirmed with a correlation coefficient of 0.842.
First, a pretest was performed using the research tool in both intervention and control groups. After the pretest, the sexual health educational content based on the BASNEF model was sent to the intervention group. The educational intervention was performed in the form of presenting the educational content (Table 1) through e-learning based on the BASNEF model during 4 sessions of two hours per week. The educational content was presented by a faculty member researcher, was recorded through the camtasia2020 software, and then was sent to the participants of the intervention group via email or virtual systems (Telegram, WhatsApp, etc.). The educational content was collected using valid sources and was approved by 8 faculty members of Guilan University of Medical Sciences. Eight weeks after the intervention, the questionnaire was completed again in two groups. The data before and after the intervention were compared in the intervention and control groups according to the aim of the study. During these 8 weeks, the researcher answered the questions of the participants of the intervention group by phone (at least twice a week).
To compare individual and social variables between the control and intervention groups, the independent t-test was used for quantitative variables, and the chi-square test (or Fisher’s exact test) was used for qualitative variables. The mean scores of beliefs, attitudes, and subjective norms were compared between the control and intervention groups before education using the independent t-test. The paired t-test was used to compare the mean scores of beliefs, attitudes, and subjective norms in each intervention group before and after the intervention. The mean scores of beliefs, attitudes, and subjective norms were compared between the two intervention groups after the intervention using analysis of covariance (ANCOVA). The ratio of the values of the two-state variables between the two groups was compared using the chi-square test (and Fisher’s exact test). Data were analyzed using SPSS software version 16, and the significance level was considered 0.05.
Table 1) Educational program
Findings
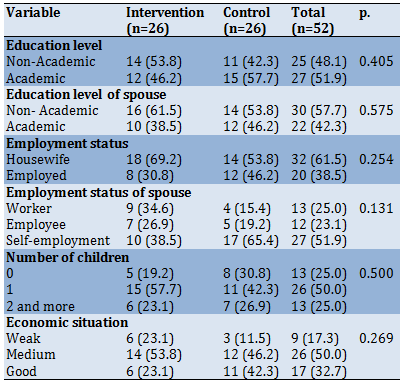
The mean±SDs of participants and their spouses' age were 30.60±5.28, and 35.33±5.62, respectively. Their Duration of married life was 8.40±4.17 years. There was no significant difference between the two groups regarding age and married duration (p>0.05). Other social characteristics of the study participants are shown in Table 2.
Table 2) Frequency results of demographic variables in the Intervention and control groups (Numbers in the parenthesis are in percent)
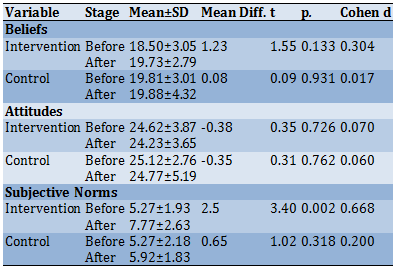
There were no statistically significant differences between the mean scores of beliefs, and Attitudes of women in the control and intervention groups (p>0.05). As shown in Table 3, the mean scores of these items increased in the intervention group in the post-intervention stage but this increase was not statistically significant (p>0.05). Just in the intervention group, the mean scores of subjective norms of the participants were significantly higher after the intervention than before it (p<0.05).
Table 3) The comparison of the mean scores of beliefs, attitudes, and Subjective norms of participants before and after the intervention in the control and educational groups
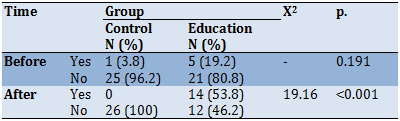
Before the education, there was no statistically significant difference between the intention to refer to sexual counseling centers during the next 6 months in the control and education groups. After the education, the intention to refer to sexual counseling centers during the next 6 months was significantly higher in the intervention group than in the control group (Table 4).
Table 4) The comparison of intention to refer to sexual counseling centers during the next 6 months between the control and education groups before and after the intervention
Discussion
Statistical tests showed that there was no statistically significant difference between the two groups of control and intervention in terms of all individual and social variables and structures of the BASNEF model; therefore, the difference in sexual health of the two groups was due to the effect of educational method. Based on the results of the present study, after the education, the mean scores of beliefs of the participants in the intervention group increased. The findings of this study are consistent with the results of the studies [15, 16] that show sex education affects individuals’ sexual awareness and can help them better understand sexual issues.
In general, the BASNEF model is a useful framework for changing beliefs and attitudes [17]. Although in the present study the educational intervention based on the BASNEF model did not make any statistically significant change in the participants’ scores of attitudes, the results of Shahbazi’s [18] study showed that the educational intervention based on the BASNEF model can improvement of beliefs and attitudes of women regarding sexual health. The difference in the results of the attitudes can be due to the difference in the participants.
In the intervention group, the mean scores of subjective norms of participants were significantly higher after the education than before it. The results of the present study were in line with the results of a study [18]. They showed that subjective norms of women regarding sexual health improved after education. Of course, in a study carried out to evaluate the effect of sex education based on the theory of planned behavior on sexual function in women, there was no significant difference in the subjective norms of the two groups after the intervention.
Also, the results of this study showed that after the education, the rate of referral to sexual counseling centers was significantly higher in the intervention group than in the control group. Research results have shown that educational programs based on the BASNEF model are usually successful in changing behaviors [13, 14, 19]. According to the BASNEF model, when attitudes and subjective norms are effective for a particular behavior, if the enabling factors act as mediators, the behavioral intention leads to the desired behavior [20]. Indeed, if a woman has a positive attitude toward sexual health and the important people in life encourage her in this regard, she can be remarkably successful in sexual function [21]. In some countries, sexual issues face cultural resistance and are taboo, and negative attitudes toward sexual issues are considered shameful in women [22]. Therefore, it seems that this issue should be considered in designing interventions related to improving attitudes toward sexual health in countries such as Iran.
In the Iranian culture, asking and investigating about sex is not something about which you can easily ask the community to talk and comment; so, one of the limitations of this project was merely selecting individuals who were interested in participating in the research.
Conclusion
The present study thus showed that the education provided based on the BASNEF model had the greatest effect on women’s sexual awareness and subjective norms. Therefore, based on the BASNEF model, intervention could improve sexual health among women. If the theories and behavior change models are correctly applied in educational programs, then useful results will be obtained.
Acknowledgments: The researchers sincerely appreciate the cooperation and support of the Department of Research and Technology of Guilan University of Medical Sciences. The authors would like to thank the women who had full cooperation with us.
Ethical Permissions: This study was approved by the Ethics Committee of Guilan University of Medical Sciences (Ethics Committee: IR.GUMS.REC.1400.047).
Conflicts of Interest: There are no conflicts of interest.
Authors' Contributions: Haghdoost Z (First Author), Introduction Writer/Methodologist/Discussion Writer (40%); Bostani Khalesi Z (Second Author), Introduction Writer/Statistical analyst/Discussion Writer (40%); Maroufizadeh S (Third Author), Methodologist/Statistical Analyst (20%)
Funding/Sources: None declared.
First, a pretest was performed using the research tool in both intervention and control groups. After the pretest, the sexual health educational content based on the BASNEF model was sent to the intervention group. The educational intervention was performed in the form of presenting the educational content (Table 1) through e-learning based on the BASNEF model during 4 sessions of two hours per week. The educational content was presented by a faculty member researcher, was recorded through the camtasia2020 software, and then was sent to the participants of the intervention group via email or virtual systems (Telegram, WhatsApp, etc.). The educational content was collected using valid sources and was approved by 8 faculty members of Guilan University of Medical Sciences. Eight weeks after the intervention, the questionnaire was completed again in two groups. The data before and after the intervention were compared in the intervention and control groups according to the aim of the study. During these 8 weeks, the researcher answered the questions of the participants of the intervention group by phone (at least twice a week).
To compare individual and social variables between the control and intervention groups, the independent t-test was used for quantitative variables, and the chi-square test (or Fisher’s exact test) was used for qualitative variables. The mean scores of beliefs, attitudes, and subjective norms were compared between the control and intervention groups before education using the independent t-test. The paired t-test was used to compare the mean scores of beliefs, attitudes, and subjective norms in each intervention group before and after the intervention. The mean scores of beliefs, attitudes, and subjective norms were compared between the two intervention groups after the intervention using analysis of covariance (ANCOVA). The ratio of the values of the two-state variables between the two groups was compared using the chi-square test (and Fisher’s exact test). Data were analyzed using SPSS software version 16, and the significance level was considered 0.05.
Table 1) Educational program
Findings
The mean±SDs of participants and their spouses' age were 30.60±5.28, and 35.33±5.62, respectively. Their Duration of married life was 8.40±4.17 years. There was no significant difference between the two groups regarding age and married duration (p>0.05). Other social characteristics of the study participants are shown in Table 2.
Table 2) Frequency results of demographic variables in the Intervention and control groups (Numbers in the parenthesis are in percent)
There were no statistically significant differences between the mean scores of beliefs, and Attitudes of women in the control and intervention groups (p>0.05). As shown in Table 3, the mean scores of these items increased in the intervention group in the post-intervention stage but this increase was not statistically significant (p>0.05). Just in the intervention group, the mean scores of subjective norms of the participants were significantly higher after the intervention than before it (p<0.05).
Table 3) The comparison of the mean scores of beliefs, attitudes, and Subjective norms of participants before and after the intervention in the control and educational groups
Before the education, there was no statistically significant difference between the intention to refer to sexual counseling centers during the next 6 months in the control and education groups. After the education, the intention to refer to sexual counseling centers during the next 6 months was significantly higher in the intervention group than in the control group (Table 4).
Table 4) The comparison of intention to refer to sexual counseling centers during the next 6 months between the control and education groups before and after the intervention
Discussion
Statistical tests showed that there was no statistically significant difference between the two groups of control and intervention in terms of all individual and social variables and structures of the BASNEF model; therefore, the difference in sexual health of the two groups was due to the effect of educational method. Based on the results of the present study, after the education, the mean scores of beliefs of the participants in the intervention group increased. The findings of this study are consistent with the results of the studies [15, 16] that show sex education affects individuals’ sexual awareness and can help them better understand sexual issues.
In general, the BASNEF model is a useful framework for changing beliefs and attitudes [17]. Although in the present study the educational intervention based on the BASNEF model did not make any statistically significant change in the participants’ scores of attitudes, the results of Shahbazi’s [18] study showed that the educational intervention based on the BASNEF model can improvement of beliefs and attitudes of women regarding sexual health. The difference in the results of the attitudes can be due to the difference in the participants.
In the intervention group, the mean scores of subjective norms of participants were significantly higher after the education than before it. The results of the present study were in line with the results of a study [18]. They showed that subjective norms of women regarding sexual health improved after education. Of course, in a study carried out to evaluate the effect of sex education based on the theory of planned behavior on sexual function in women, there was no significant difference in the subjective norms of the two groups after the intervention.
Also, the results of this study showed that after the education, the rate of referral to sexual counseling centers was significantly higher in the intervention group than in the control group. Research results have shown that educational programs based on the BASNEF model are usually successful in changing behaviors [13, 14, 19]. According to the BASNEF model, when attitudes and subjective norms are effective for a particular behavior, if the enabling factors act as mediators, the behavioral intention leads to the desired behavior [20]. Indeed, if a woman has a positive attitude toward sexual health and the important people in life encourage her in this regard, she can be remarkably successful in sexual function [21]. In some countries, sexual issues face cultural resistance and are taboo, and negative attitudes toward sexual issues are considered shameful in women [22]. Therefore, it seems that this issue should be considered in designing interventions related to improving attitudes toward sexual health in countries such as Iran.
In the Iranian culture, asking and investigating about sex is not something about which you can easily ask the community to talk and comment; so, one of the limitations of this project was merely selecting individuals who were interested in participating in the research.
Conclusion
The present study thus showed that the education provided based on the BASNEF model had the greatest effect on women’s sexual awareness and subjective norms. Therefore, based on the BASNEF model, intervention could improve sexual health among women. If the theories and behavior change models are correctly applied in educational programs, then useful results will be obtained.
Acknowledgments: The researchers sincerely appreciate the cooperation and support of the Department of Research and Technology of Guilan University of Medical Sciences. The authors would like to thank the women who had full cooperation with us.
Ethical Permissions: This study was approved by the Ethics Committee of Guilan University of Medical Sciences (Ethics Committee: IR.GUMS.REC.1400.047).
Conflicts of Interest: There are no conflicts of interest.
Authors' Contributions: Haghdoost Z (First Author), Introduction Writer/Methodologist/Discussion Writer (40%); Bostani Khalesi Z (Second Author), Introduction Writer/Statistical analyst/Discussion Writer (40%); Maroufizadeh S (Third Author), Methodologist/Statistical Analyst (20%)
Funding/Sources: None declared.
Article Type: Original Research |
Subject:
Health Education and Health Behavior
Received: 2022/03/28 | Accepted: 2022/06/21 | Published: 2022/07/24
Received: 2022/03/28 | Accepted: 2022/06/21 | Published: 2022/07/24
References
1. World Health Organization. Defining sexual health: report of a technical consultation on sexual health 2002. Geneva: World Health Organization; 2006. [Link]
2. Savoy M, O'Gurek D, Brown-James A. Sexual health history: techniques and tips. Am Fam Physician. 2020;101(5):286-93. [Link]
3. Coleman E. Promoting sexual health and responsible sexual behavior: an introduction. J Sex Res. 2002;39(1):3-6. [Link] [DOI:10.1080/00224490209552111]
4. Pitts RA, Greene RE. Promoting positive sexual health. Am J Public Health. 2020;110(2):149-50. [Link] [DOI:10.2105/AJPH.2019.305336]
5. Roden RC, Schmidt EK, Holland-Hall C. Sexual health education for adolescents and young adults with intellectual and developmental disabilities: recommendations for accessible sexual and reproductive health information. Lancet Child Adolesc Health. 2020;4(9):699-708. [Link] [DOI:10.1016/S2352-4642(20)30098-5]
6. Pampati S, Johns MM, Szucs LE, Bishop MD, Mallory AB, Barrios LC, et al. Sexual and gender minority youth and sexual health education: a systematic mapping review of the literature. J Adolesc Health. 2021;68(6):1040-52. [Link] [DOI:10.1016/j.jadohealth.2020.09.032]
7. Marotta C, Lochoro P, Pizzol D, Putoto G, Mazzucco W, Saracino A, et al. Capacity assessment for provision of quality sexual reproductive health and HIV-integrated services in Karamoja, Uganda. Afr Health Sci. 2020;20(3):1053-65. [Link] [DOI:10.4314/ahs.v20i3.8]
8. Rakhshaee Z, Maasoumi R, Nedjat S, Khakbazan Z. Sexual health literacy, a strategy for the challenges of sexual life of infertile women: a qualitative study. Galen Med J. 2020;9:e1862. [Link] [DOI:10.31661/gmj.v9i0.1862]
9. Farahani FK. Adolescents and young people's sexual and reproductive health in Iran: a conceptual review. J Sex Res. 2020;57(6):743-80. [Link] [DOI:10.1080/00224499.2020.1768203]
10. Javadnoori M, Hajizadeh M, Javadifar N, Hossein Haghighizadeh M. Sexual and reproductive healthcare needs of Iranian men: a cross-sectional study. Int J Reprod Biomed. 2018;16(12). [Link] [DOI:10.18502/ijrm.v16i12.3681]
11. Khani S, Moghaddam-Banaem L, Mohamadi E, Vedadhir AA, Hajizadeh E. Women's sexual and reproductive health care needs assessment: an Iranian perspective. East Mediterr Health J. 2018;24(7):637-43. [Link] [DOI:10.26719/2018.24.7.637]
12. Arlinghaus KR, Johnston CA. Advocating for behavior change with education. Am J Lifestyle Med. 2017;12(2):113-6. [Link] [DOI:10.1177/1559827617745479]
13. Shahnazi H, Bee Koon P, Abd Talib R, Lubis SH, Ganjali Dashti M, Khatooni E, et al. Can the BASNEF model help to develop self-administered healthy behavior in Iranian youth?. Iran Red Crescent Med J. 2016;18(3):e23847. [Link] [DOI:10.5812/ircmj.23847]
14. Hubley J. Understanding behavior: the key to successful health education. Trop Doct. 1988;18(3):134-8. [Link] [DOI:10.1177/004947558801800316]
15. Leung H, Shek DTL, Leung E, Shek EYW. Development of contextually-relevant sexuality education: lessons from a comprehensive review of adolescent sexuality education across cultures. Int J Environ Res Public Health. 2019;16(4):621. [Link] [DOI:10.3390/ijerph16040621]
16. Kumar R, Goyal A, Singh P, Bhardwaj A, Mittal A, Yadav SS. Knowledge attitude and perception of sex education among school going adolescents in Ambala district, Haryana, India: a cross-sectional study. J Clin Diagn Res. 2017;11(3):LC01-4. [Link] [DOI:10.7860/JCDR/2017/19290.9338]
17. Glanz K, Rimer BK, Viswanath K. Health behavior and health education: theory, research, and practice. 6th Edition. San Francisco (CA): John Wiley & Sons; 2020. [Link]
18. Shahbazi A, Behboodi Moghadam Z, Maasoumi R, Saffari M, Mohammadi S, Montazeri A. Effect of a health-education program based on the basnef model of overall sexual health satisfaction and satisfaction with quality of sexual relationship among women with infertility. Int J Womens Health. 2020;12:975-82. [Link] [DOI:10.2147/IJWH.S248734]
19. Barimani Aboksari Z, Ganji J, Mousavinasab N, Rezaei M, Khani S. A review study on educational interventions promoting sexual health of children under 12 years. J Pediatr Rev. 2020;8(2):107-20. [Link] [DOI:10.32598/jpr.8.2.107]
20. Bandehelahi K, Khoshravesh S, Barati M, Tapak L. Psychological and sociodemographic predictors of fertility intention among childbearing-aged women in Hamadan, west of Iran: an application of the BASNEF Model. Korean J Fam Med. 2019;40(3):182-7. [Link] [DOI:10.4082/kjfm.18.0008]
21. Behboodi Moghadam Z, Rezaei E, Khaleghi Yalegonbadi F, Montazeri A, Arzaqi SM, Tavakol Z, et al. The effect of sexual health education program on women sexual function in Iran. J Res Health Sci. 2015;15(2):124-8. [Link]
22. Ebrahimipour H, Jalambadany Z, Peyman N, Ismaili H, Vafaii Najjar A. Effect of sex education, based on the theory of planned behavior, on the sexual function of the woman attending Mashhad health centers. J Birjand Univ Med Sci. 2013;20:58-67. [Persian] [Link]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |