



Volume 10, Issue 4 (2022)
Health Educ Health Promot 2022, 10(4): 703-709 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alkhawarah R, Esteki T, Shirinabadi Farahani A, Babaie M, Nasiri M. Mothers’ Performance in Feeding a Toddler with Diarrhea and its Related Factors. Health Educ Health Promot 2022; 10 (4) :703-709
URL: http://hehp.modares.ac.ir/article-5-59865-en.html
URL: http://hehp.modares.ac.ir/article-5-59865-en.html
1- Department of Pediatric Nursing, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Department of Basic Sciences, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3- Department of Pediatric & Neonatal Intensive Care Nursing, School of Nursing & Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- “Student Research Committee” and “Department of Pediatric & Neonatal Intensive Care Nursing, School of Nursing & Midwifery”, Shahid Beheshti University of Medical Sciences, Tehran, Iran
5- Department of Biostatistics, School of Nursing & Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Department of Basic Sciences, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3- Department of Pediatric & Neonatal Intensive Care Nursing, School of Nursing & Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- “Student Research Committee” and “Department of Pediatric & Neonatal Intensive Care Nursing, School of Nursing & Midwifery”, Shahid Beheshti University of Medical Sciences, Tehran, Iran
5- Department of Biostatistics, School of Nursing & Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Full-Text [PDF 918 kb]
(3438 Downloads)
| Abstract (HTML) (2117 Views)
Full-Text: (442 Views)
Introduction
Diarrhea is the second leading cause of death in children under the age of five. Every year, around 1.5 billion diarrhea occurrences occur over the world, resulting in 1.5 to 2.5 million deaths, accounting for more than 20% of all deaths [1]. It was responsible for about 1.3 million deaths worldwide in 2015, and its impact was estimated to be 71.59 million Disability Adjusted Life Years [2]. It is also the second leading cause of death in children under 5 in India, which causes severe anxiety in parents [3].
According to studies, this disease occurs in underdeveloped countries of Africa and Asia [4-6], among people with poor health, workers, low-income people, and the homeless, and among impoverished populations, who lack access to adequate drinking water [6-8]. Also, pediatric diarrhea incidence has been proven to be inversely connected to socioeconomic class, with children in poverty being considerably more sensitive to acute diarrheal episodes and more severe and longer-lasting sickness. In a research conducted in South Africa, children living in poverty were 10 times more likely than their more wealthy counterparts to die from diarrhea [6]. In other words, poor hygiene is a serious threat to the health of children because, in this situation, it is often these children who suffer from diarrhea through various microorganisms [8].
Previous studies show that under adverse health conditions, the most common cause of childhood gastrointestinal infections is human rotavirus, which causes 125 million cases of diarrhea and more than 600,000 childhood deaths worldwide each year [9, 10]. This virus is also considered the main microorganism causing diarrhea in Iranian children [4, 9].
Literature shows that in these children, diarrhea is exacerbated by contaminated food, weaning, hazardous feeding techniques, a lack of clean water, incorrect hand washing, restricted sanitary waste disposal, poor housing circumstances, and a lack of access to adequate and inexpensive health care [7, 9, 11].
In most third-world nations, children under the age of three have three episodes of diarrhea each year on average which has a profound impact on childhood nutrition and development. Diarrhea is a major cause of malnutrition in children under the age of five. Although total worldwide mortality rates for diarrhea diseases have decreased in recent decades, diarrhea morbidity has not [12]. Dehydration and electrolyte imbalance related to diarrhea still affect many young children which remains one of the leading causes of mortality in children worldwide [13].
Diarrhea can be treated and prevented at home by primary caregivers [3, 5, 14]. The fact that diarrhea begins at home and continues at home after being examined at a health institution emphasizes the necessity of home management of diarrhea. Specific UNICEF guidelines, such as rice water, soup, yogurt, and Oral Rehydration Salt (ORS), are vital [15]. Feeding the infant should continue, especially with plenty of nutritious food, to prevent any growth loss that may occur during and after the diarrhea episode [3]. Traditional ways of diarrhea management are frequently preferred by mothers, who seek medical help only when such approaches fail [15]. In Iran, it is believed that ORS is a low-cost treatment that can be conveniently delivered by mothers at home as soon as a bout of diarrhea begins [1].
The nutritional and food requirements of toddlers differ greatly from other peers and older children. Energy, protein, fat, iron, calcium, vitamin A, vitamin D, fiber, and salt are among the essential nutrients for children aged 1 to 5 [16]. In other words, the quality and quantity of food, as well as other nutrition-related aspects, are also important in the care and development of diarrheic children. In this aspect, maternal knowledge and performance are crucial [3, 14, 17].
Diarrhea in itself is not dangerous; however, mothers' lack of awareness, bad habits, and pessimism, as well as their misguided attitude to its care and prevention, contribute to a high degree of serious dehydration and, eventually, mortality [11]. Because mothers are the major healthcare providers, their awareness of the causes of diarrhea is important. In other words, it's critical to recognize and identify particular symptoms or signs in order to get medical help as soon as possible [15].
Since the mothers are in charge of determining the type of food to nourish the child as well as the disease's overall management, their knowledge and attitudes about the causes of diarrhea are crucial in taking appropriate action on time [3, 14]. Because mothers' knowledge of health, disease, and preventive services serves as a gauge to measure the family, community, and country's progress. Inadequate use of accessible health services can result from a lack of awareness. The mother's healthy habits can improve a child's health and reduce morbidity and death in children under the age of five. Since the child is unable to carry out his or her own daily activities, mothers' knowledge and their children's health are linked [1, 18].
Various factors can influence their awareness of childhood diarrhea treatment, including their education position, past disease management experience, and even ethnicity. In addition, variables like mothers' occupation, husbands' job status, family income, family size, and mothers' attitudes and behaviors are linked to mothers' awareness of diarrhea and its management [1, 19]. On the other hand, maternal weak education, poor sanitation, contaminated water supply, duration of breastfeeding, failure to wash hands, lack of vaccination, child's age, and improper food hygiene diarrheal disease recurrence in children under the age of five years [20].
Studies have been conducted on diarrhea prevention activities in caregivers of children under five years of age. For example, in Indonesia, this research was conducted using the health belief model as a conceptual framework [21]. Despite the high incidence of diarrhea in Iran, there are not enough studies to comprehensively examine mothers' performance in toddlers with diarrhea. Consequently, it is essential to study the mothers' performance in nutrition and other related factors such as breastfeeding, ORS, complementary foods, vaccination, hygiene, and sanitation status and beliefs. Finding this information helps to design appropriate intervention strategies to prevent diarrhea and decrease the cost of its treatment. Therefore, this study was performed to investigate the factors affecting mothers' performance in feeding a toddler with diarrhea.
Instruments and Methods
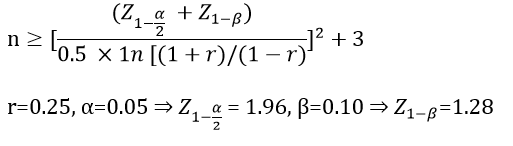
This cross-sectional descriptive study was performed on 210 mothers who had toddlers (1-3 years old) with diarrhea, referred to Loqman, Mofid, Imam Hussein, and Shohada Hospitals affiliated with Shahid Beheshti University of Medical Sciences, Tehran, Iran in 2021. The sample size was obtained according to the following formula 189, considering 10% loss (incomplete questionnaires), 210 samples can be considered.
Therefore, all mothers who had hospitalized a toddler due to diarrhea in the last 2 weeks or with a history of diarrhea up to 6 months before and were willing to participate in the study were included in the study, and those who were unable to hear and speak were excluded from the study.
The research protocol was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran. Permission was obtained from both the university and the hospitals. Due to the difference between the researcher's language and the mothers, a Persian-speaking person who was trained helped the researcher. The purpose and method of the study and the confidentiality of information were explained to the participants and then informed consent was obtained. The participants were assured of their right to withdraw from the research at any time. The questionnaire was completed by each of the mothers in a face-to-face interview. Data collection took 56 days from 12 July 2021 to 5 September 2021, and each questionnaire took an average of 10 to 15 minutes. The researcher was present in each hospital in the morning and evening shifts.
Socio-Demographic Questionnaire: The demographic questionnaire included the mother's age (years), number of children, mother's marital status, type of pregnancy, mother and father's education level, mother and father’s job, residence, referral setting, child's age (months), child’s gender, birth order in the family and the number of episodes of acute diarrhea in the past year.
Mother’s Performance Questionnaire: It is a researcher-made close-ended questionnaire in the Persian language, which was prepared based on studies of various scientific sources on the mothers’ performance related to diarrhea children in the nutrition, breastfeeding, ORS, hygiene principles, and common beliefs [1, 22, 23]. This questionnaire includes 4 dimensions: Nutrition (24 items), Breastfeeding (5 items), ORS (5 items), Hygiene principles, and Common beliefs (11 items) in the 5-point Likert scale from “always” (5) to “never” (1). The minimum and maximum scores are 45 and 225.
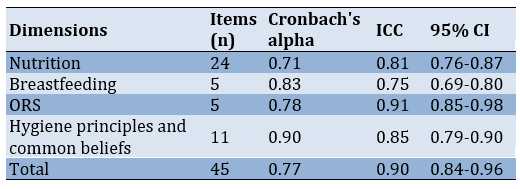
Validity and reliability: Content Validity Index (CVI) and Content Validity Ratio (CVR) values were calculated for all questions more than 0.7. Also, the qualitative content validity with the judgment of 10 faculty members of Shahid Beheshti University of Medical Sciences and experts in the fields of child nursing and nutrition were done, and the required changes were applied. Before use, all questions were pretested for reliability with 25 mothers with inclusion criteria. The data of the pretest were deleted from the main analysis. According to the feedback of the participants, modifications were made in the questionnaire. Cronbach's alpha was conducted to determine internal consistency. Also, the Intra-Class Correlation (ICC) coefficient was used for stability reliability. The results related to the reliability of the questionnaire are shown in Table 1.
Table 1) The reliability of the mother performance questionnaire
Date analysis: Chi-square test, paired–sample t-test, independent-sample t-test, Analysis of Variance (ANOVA), and Pearson correlation coefficient was used to determine the correlation between variables using SPSS 20 software. A p-value less than 0.05 was considered statistically significant.
Findings
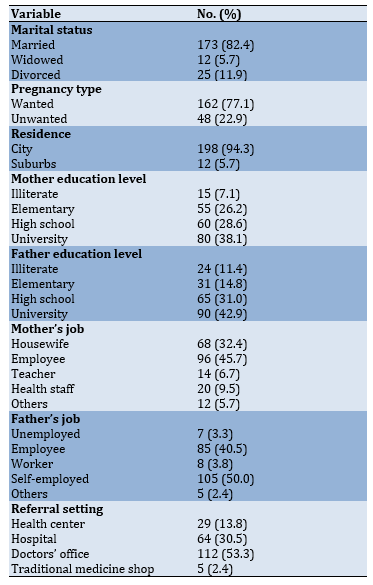
Data from 210 questionnaires completed by mothers with toddlers with diarrhea were analyzed. The mean age of mothers was 32.69±6.67 years in the range of 19-50 years. Also, the mean age of the toddlers was 23.97±7.24 months in the range of 12-36 months. 51.4% of the toddlers were boys. Other clinical and socio-demographic findings of toddlers and their parents are presented in Tables 2 and 3.
Table 2) The clinical and socio-demographic findings of toddlers (n=210)
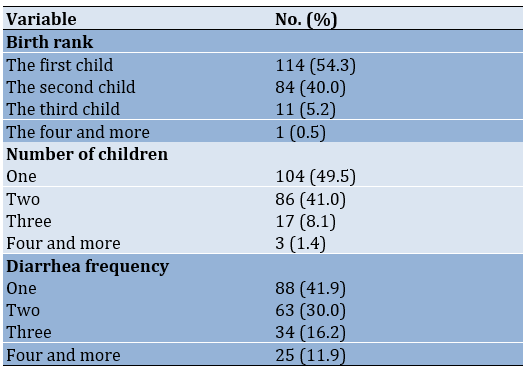
Table 3) The clinical and socio-demographic findings of mothers and fathers (n=210)
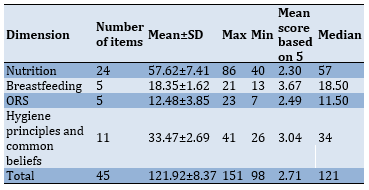
The mean score of mothers’ performance with toddlers with diarrhea was 121.92±8.37. The mean scores of mothers' performance in any of the dimensions of nutrition, breastfeeding, ORS, hygiene principles and common beliefs are presented in Table 4.
Table 4) Descriptive statistics of maternal performance dimensions
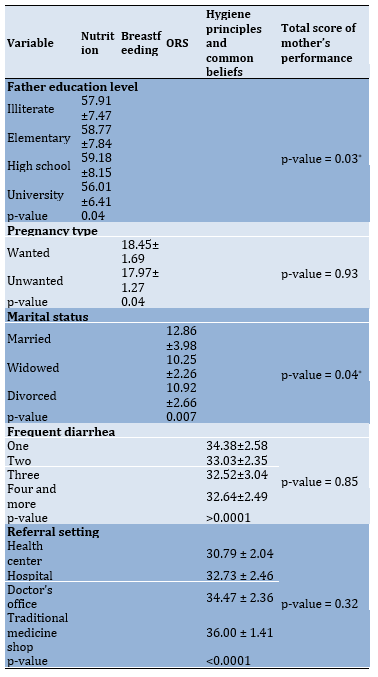
Comparing the mean scores of the mother's performance with the variables showed that there is a significant difference between the mean scores in the type of pregnancy, the father's education level, marital status, frequent diarrhea, and referral setting (Table 5).
Table 5) Comparison of mean scores of mother's performance among significant variables
Discussion
This study aimed to investigate the variables of mothers' performance in feeding a toddler with diarrhea and its related factors. Based on the results, mothers had a good performance in using household fluids during diarrhea, and at least half of them were breastfeeding at the time of diarrhea. Diarrhea harms a child's nutritional status due to reduced food intake caused by anorexia [12, 24]. To reduce mortality, dehydration, and minimize the effects of diarrhea on nutritional status, mothers are encouraged to progress their eating habits, especially by giving their children more fluids and food than usual [25].
However, mothers' performance was poor in some aspects. The use of sugar in a child with diarrhea and reduced consumption of foods such as rice, potatoes, bread, and yogurt were other weak aspects of the mother's performance. The use of carbonated beverages for children with diarrhea was another misconception that a large percentage of mothers used for their children.
In the present study, when mothers were asked if they were feeding their children with diarrhea, 46.2% of mothers answered that they do that sometimes. 43.8% of mothers reported that their diarrhea child often consumed family food. A study showed caregivers maintained their child’s usual food intake (34%), which is in line with the present study [8]. Some caregivers offer their children fewer quantities of fluid and food during diarrheal episodes than the quantity they usually provide. Some mothers even refute children anything to eat or drink during such conditions, which exposes the children to dehydration and death [4]. A research in Nepal showed that most respondents stated that foods and fluids should be limited during diarrhea. One-third of all respondents said that drinking plain water was enough when they had diarrhea [22].
Also, more than half of mothers breastfed their children, and less than half of them did not consume homemade salt and sugar solution to treat their toddlers, and the majority experienced the use of ORS during diarrhea. Most mothers performed well on ORS during childhood diarrhea, but performed poorly on the maintenance method. The study of Dodicho [15] is consistent with this result. Out of the 466 respondents who were aware of ORS solution preparation, 72.5% of mothers were able to describe the correct method of its.
A study stated that the greater rates of episodes of child diarrhea are related to poor sanitary conditions and hand-washing practices [9]. In the present study, maternal hygiene was poor, such as never washing their baby's bottle with boiling water or washing their hands before preparing milk. Few mothers washed their hands with soap after each defecation of the child with diarrhea. About 78.1% of them agreed that teething cause diarrhea, which is similar to the study conducted in Eastern Ethiopia [6]. Despite health recommendations, especially hand washing, the results of a study showed that hand washing by mothers had no impact on the occurrence of diarrhea in their children [7].
Numerous studies have acknowledged that the mother's level of education is an important and effective factor in reducing their child's diarrhea [1, 5]. However, in the present study, although most mothers had high school education and university degrees, their child's incidence of diarrhea was not low.
Moreover, according to studies, the occupation of the mother and father is related significantly to diarrheal diseases [24]. This is similarly supported by other studies done on the occupation of parents [26]. But in the present study, parental employment was not an effective and significant factor in improving mothers' performance in caring for a toddler with diarrhea.
The number of children was not significantly associated with mothers’ performance. Regarding the relationship between maternal performance scores and frequent diarrhea, there was significant differences in the hygiene principles and common beliefs dimension. This result is consistent with a study in Nigeria that shows the prevention of infectious diarrhea is associated with improved hygiene, clean drinking water, and hand washing with soap [27]. Generally, the mother's experience in managing a child with diarrhea seems to reduce the child's subsequent infection.
Regarding marital status, it was observed that ORS was significantly used in married mothers than divorced mothers, as well as widowed ones. It is because married mothers are supported by their spouses [28] in this situation, and it contributes significantly to their better performance in caring for a child with diarrhea.
In the current study, another variable, which was significant in the breastfeeding dimension of maternal performance, was the pregnancy type. Because in wanted pregnancy, mothers were more inclined to breastfeed. In this way, children who have a married mother that lives with her spouse and intends to get pregnant are less likely to have diarrhea [28]. Breastfeeding is a very important factor in reducing the incidence of diarrhea.
Regarding maternal performance and referral setting variables, significant differences were observed in the traditional medicine stores compared to other healthcare. The present study is in line with a study conducted by Cunnama and Honda in 2016. They found that when mothers choose healthcare providers to treat children with diarrhea, the decisions are made based on mothers' beliefs that are deeply rooted in their culture [17].
Various studies reveal that diarrhea disease remains the main cause of mortality and morbidity among children under five years old [18]. But most of the children who participated in this study were between 12 and 24 months old.
Regarding the gender of toddlers with diarrhea, most of them were boys. It is in line with a study that reported a high prevalence of diarrhea in boys [1]. While in the study of Stephen et al., more than half of the children were girls [29].
Rates of diarrhea were considerably higher among the first children in the family, which is in agreement with the result of a recent study [30]. The inexperience of the mother and unawareness of the risk factors related to diarrhea and its transmission is leading to a rise in diarrheal infections in first child care.
According to the results of this study, it is highly proposed that mothers, especially those who do not currently use any public health services, should be included and addressed in health education programs and mass media. Moreover, healthcare providers play a critical role in increasing the mother's awareness of the correct and efficient adoption of specific diets.
In this study, only mothers with toddlers were examined. It recommended that children of other developmental ages also be studied, considering the importance of the subject. It is highly suggested that mothers, especially those who do not currently use any public health services, be included and addressed in health education programs and mass media.
Conclusion
The mothers’ performance regarding diarrhea and its dietary management is low, and less than half of them have a good level of knowledge. So it is necessary to improve and implement relevant policies to control and manage diarrhea.
Acknowledgements: The authors would like to appreciate all the authorities in the hospitals under study and the mothers who participated in this research.
Ethical Permission: This article was approved by the Research Deputy of Shahid Beheshti University of Medical Sciences (The ethics code: IR.SBMU.PHARMACY.REC.1399.365).
Authors Contribution: Alkhawarah R.H. (First author), Introduction author/ Original researcher (20%); Esteki T. (Second author), Introduction author/ Methodologist (25%); Shirinabadi Farahani A. (Third author), Methodologist/ Discussion author (25%); Babaie M. (Fourth author), Introduction author/ Discussion author (15%), Nasiri M. (Fifth author), Statistical analysis (15%).
Conflicts of Interest: The authors declare no conflict of interest in this study.
Funding: This article is a part of a nursing master's thesis funded by Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Diarrhea is the second leading cause of death in children under the age of five. Every year, around 1.5 billion diarrhea occurrences occur over the world, resulting in 1.5 to 2.5 million deaths, accounting for more than 20% of all deaths [1]. It was responsible for about 1.3 million deaths worldwide in 2015, and its impact was estimated to be 71.59 million Disability Adjusted Life Years [2]. It is also the second leading cause of death in children under 5 in India, which causes severe anxiety in parents [3].
According to studies, this disease occurs in underdeveloped countries of Africa and Asia [4-6], among people with poor health, workers, low-income people, and the homeless, and among impoverished populations, who lack access to adequate drinking water [6-8]. Also, pediatric diarrhea incidence has been proven to be inversely connected to socioeconomic class, with children in poverty being considerably more sensitive to acute diarrheal episodes and more severe and longer-lasting sickness. In a research conducted in South Africa, children living in poverty were 10 times more likely than their more wealthy counterparts to die from diarrhea [6]. In other words, poor hygiene is a serious threat to the health of children because, in this situation, it is often these children who suffer from diarrhea through various microorganisms [8].
Previous studies show that under adverse health conditions, the most common cause of childhood gastrointestinal infections is human rotavirus, which causes 125 million cases of diarrhea and more than 600,000 childhood deaths worldwide each year [9, 10]. This virus is also considered the main microorganism causing diarrhea in Iranian children [4, 9].
Literature shows that in these children, diarrhea is exacerbated by contaminated food, weaning, hazardous feeding techniques, a lack of clean water, incorrect hand washing, restricted sanitary waste disposal, poor housing circumstances, and a lack of access to adequate and inexpensive health care [7, 9, 11].
In most third-world nations, children under the age of three have three episodes of diarrhea each year on average which has a profound impact on childhood nutrition and development. Diarrhea is a major cause of malnutrition in children under the age of five. Although total worldwide mortality rates for diarrhea diseases have decreased in recent decades, diarrhea morbidity has not [12]. Dehydration and electrolyte imbalance related to diarrhea still affect many young children which remains one of the leading causes of mortality in children worldwide [13].
Diarrhea can be treated and prevented at home by primary caregivers [3, 5, 14]. The fact that diarrhea begins at home and continues at home after being examined at a health institution emphasizes the necessity of home management of diarrhea. Specific UNICEF guidelines, such as rice water, soup, yogurt, and Oral Rehydration Salt (ORS), are vital [15]. Feeding the infant should continue, especially with plenty of nutritious food, to prevent any growth loss that may occur during and after the diarrhea episode [3]. Traditional ways of diarrhea management are frequently preferred by mothers, who seek medical help only when such approaches fail [15]. In Iran, it is believed that ORS is a low-cost treatment that can be conveniently delivered by mothers at home as soon as a bout of diarrhea begins [1].
The nutritional and food requirements of toddlers differ greatly from other peers and older children. Energy, protein, fat, iron, calcium, vitamin A, vitamin D, fiber, and salt are among the essential nutrients for children aged 1 to 5 [16]. In other words, the quality and quantity of food, as well as other nutrition-related aspects, are also important in the care and development of diarrheic children. In this aspect, maternal knowledge and performance are crucial [3, 14, 17].
Diarrhea in itself is not dangerous; however, mothers' lack of awareness, bad habits, and pessimism, as well as their misguided attitude to its care and prevention, contribute to a high degree of serious dehydration and, eventually, mortality [11]. Because mothers are the major healthcare providers, their awareness of the causes of diarrhea is important. In other words, it's critical to recognize and identify particular symptoms or signs in order to get medical help as soon as possible [15].
Since the mothers are in charge of determining the type of food to nourish the child as well as the disease's overall management, their knowledge and attitudes about the causes of diarrhea are crucial in taking appropriate action on time [3, 14]. Because mothers' knowledge of health, disease, and preventive services serves as a gauge to measure the family, community, and country's progress. Inadequate use of accessible health services can result from a lack of awareness. The mother's healthy habits can improve a child's health and reduce morbidity and death in children under the age of five. Since the child is unable to carry out his or her own daily activities, mothers' knowledge and their children's health are linked [1, 18].
Various factors can influence their awareness of childhood diarrhea treatment, including their education position, past disease management experience, and even ethnicity. In addition, variables like mothers' occupation, husbands' job status, family income, family size, and mothers' attitudes and behaviors are linked to mothers' awareness of diarrhea and its management [1, 19]. On the other hand, maternal weak education, poor sanitation, contaminated water supply, duration of breastfeeding, failure to wash hands, lack of vaccination, child's age, and improper food hygiene diarrheal disease recurrence in children under the age of five years [20].
Studies have been conducted on diarrhea prevention activities in caregivers of children under five years of age. For example, in Indonesia, this research was conducted using the health belief model as a conceptual framework [21]. Despite the high incidence of diarrhea in Iran, there are not enough studies to comprehensively examine mothers' performance in toddlers with diarrhea. Consequently, it is essential to study the mothers' performance in nutrition and other related factors such as breastfeeding, ORS, complementary foods, vaccination, hygiene, and sanitation status and beliefs. Finding this information helps to design appropriate intervention strategies to prevent diarrhea and decrease the cost of its treatment. Therefore, this study was performed to investigate the factors affecting mothers' performance in feeding a toddler with diarrhea.
Instruments and Methods
This cross-sectional descriptive study was performed on 210 mothers who had toddlers (1-3 years old) with diarrhea, referred to Loqman, Mofid, Imam Hussein, and Shohada Hospitals affiliated with Shahid Beheshti University of Medical Sciences, Tehran, Iran in 2021. The sample size was obtained according to the following formula 189, considering 10% loss (incomplete questionnaires), 210 samples can be considered.
Therefore, all mothers who had hospitalized a toddler due to diarrhea in the last 2 weeks or with a history of diarrhea up to 6 months before and were willing to participate in the study were included in the study, and those who were unable to hear and speak were excluded from the study.
The research protocol was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran. Permission was obtained from both the university and the hospitals. Due to the difference between the researcher's language and the mothers, a Persian-speaking person who was trained helped the researcher. The purpose and method of the study and the confidentiality of information were explained to the participants and then informed consent was obtained. The participants were assured of their right to withdraw from the research at any time. The questionnaire was completed by each of the mothers in a face-to-face interview. Data collection took 56 days from 12 July 2021 to 5 September 2021, and each questionnaire took an average of 10 to 15 minutes. The researcher was present in each hospital in the morning and evening shifts.
Socio-Demographic Questionnaire: The demographic questionnaire included the mother's age (years), number of children, mother's marital status, type of pregnancy, mother and father's education level, mother and father’s job, residence, referral setting, child's age (months), child’s gender, birth order in the family and the number of episodes of acute diarrhea in the past year.
Mother’s Performance Questionnaire: It is a researcher-made close-ended questionnaire in the Persian language, which was prepared based on studies of various scientific sources on the mothers’ performance related to diarrhea children in the nutrition, breastfeeding, ORS, hygiene principles, and common beliefs [1, 22, 23]. This questionnaire includes 4 dimensions: Nutrition (24 items), Breastfeeding (5 items), ORS (5 items), Hygiene principles, and Common beliefs (11 items) in the 5-point Likert scale from “always” (5) to “never” (1). The minimum and maximum scores are 45 and 225.
Validity and reliability: Content Validity Index (CVI) and Content Validity Ratio (CVR) values were calculated for all questions more than 0.7. Also, the qualitative content validity with the judgment of 10 faculty members of Shahid Beheshti University of Medical Sciences and experts in the fields of child nursing and nutrition were done, and the required changes were applied. Before use, all questions were pretested for reliability with 25 mothers with inclusion criteria. The data of the pretest were deleted from the main analysis. According to the feedback of the participants, modifications were made in the questionnaire. Cronbach's alpha was conducted to determine internal consistency. Also, the Intra-Class Correlation (ICC) coefficient was used for stability reliability. The results related to the reliability of the questionnaire are shown in Table 1.
Table 1) The reliability of the mother performance questionnaire
Date analysis: Chi-square test, paired–sample t-test, independent-sample t-test, Analysis of Variance (ANOVA), and Pearson correlation coefficient was used to determine the correlation between variables using SPSS 20 software. A p-value less than 0.05 was considered statistically significant.
Findings
Data from 210 questionnaires completed by mothers with toddlers with diarrhea were analyzed. The mean age of mothers was 32.69±6.67 years in the range of 19-50 years. Also, the mean age of the toddlers was 23.97±7.24 months in the range of 12-36 months. 51.4% of the toddlers were boys. Other clinical and socio-demographic findings of toddlers and their parents are presented in Tables 2 and 3.
Table 2) The clinical and socio-demographic findings of toddlers (n=210)
Table 3) The clinical and socio-demographic findings of mothers and fathers (n=210)
The mean score of mothers’ performance with toddlers with diarrhea was 121.92±8.37. The mean scores of mothers' performance in any of the dimensions of nutrition, breastfeeding, ORS, hygiene principles and common beliefs are presented in Table 4.
Table 4) Descriptive statistics of maternal performance dimensions
Comparing the mean scores of the mother's performance with the variables showed that there is a significant difference between the mean scores in the type of pregnancy, the father's education level, marital status, frequent diarrhea, and referral setting (Table 5).
Table 5) Comparison of mean scores of mother's performance among significant variables
Discussion
This study aimed to investigate the variables of mothers' performance in feeding a toddler with diarrhea and its related factors. Based on the results, mothers had a good performance in using household fluids during diarrhea, and at least half of them were breastfeeding at the time of diarrhea. Diarrhea harms a child's nutritional status due to reduced food intake caused by anorexia [12, 24]. To reduce mortality, dehydration, and minimize the effects of diarrhea on nutritional status, mothers are encouraged to progress their eating habits, especially by giving their children more fluids and food than usual [25].
However, mothers' performance was poor in some aspects. The use of sugar in a child with diarrhea and reduced consumption of foods such as rice, potatoes, bread, and yogurt were other weak aspects of the mother's performance. The use of carbonated beverages for children with diarrhea was another misconception that a large percentage of mothers used for their children.
In the present study, when mothers were asked if they were feeding their children with diarrhea, 46.2% of mothers answered that they do that sometimes. 43.8% of mothers reported that their diarrhea child often consumed family food. A study showed caregivers maintained their child’s usual food intake (34%), which is in line with the present study [8]. Some caregivers offer their children fewer quantities of fluid and food during diarrheal episodes than the quantity they usually provide. Some mothers even refute children anything to eat or drink during such conditions, which exposes the children to dehydration and death [4]. A research in Nepal showed that most respondents stated that foods and fluids should be limited during diarrhea. One-third of all respondents said that drinking plain water was enough when they had diarrhea [22].
Also, more than half of mothers breastfed their children, and less than half of them did not consume homemade salt and sugar solution to treat their toddlers, and the majority experienced the use of ORS during diarrhea. Most mothers performed well on ORS during childhood diarrhea, but performed poorly on the maintenance method. The study of Dodicho [15] is consistent with this result. Out of the 466 respondents who were aware of ORS solution preparation, 72.5% of mothers were able to describe the correct method of its.
A study stated that the greater rates of episodes of child diarrhea are related to poor sanitary conditions and hand-washing practices [9]. In the present study, maternal hygiene was poor, such as never washing their baby's bottle with boiling water or washing their hands before preparing milk. Few mothers washed their hands with soap after each defecation of the child with diarrhea. About 78.1% of them agreed that teething cause diarrhea, which is similar to the study conducted in Eastern Ethiopia [6]. Despite health recommendations, especially hand washing, the results of a study showed that hand washing by mothers had no impact on the occurrence of diarrhea in their children [7].
Numerous studies have acknowledged that the mother's level of education is an important and effective factor in reducing their child's diarrhea [1, 5]. However, in the present study, although most mothers had high school education and university degrees, their child's incidence of diarrhea was not low.
Moreover, according to studies, the occupation of the mother and father is related significantly to diarrheal diseases [24]. This is similarly supported by other studies done on the occupation of parents [26]. But in the present study, parental employment was not an effective and significant factor in improving mothers' performance in caring for a toddler with diarrhea.
The number of children was not significantly associated with mothers’ performance. Regarding the relationship between maternal performance scores and frequent diarrhea, there was significant differences in the hygiene principles and common beliefs dimension. This result is consistent with a study in Nigeria that shows the prevention of infectious diarrhea is associated with improved hygiene, clean drinking water, and hand washing with soap [27]. Generally, the mother's experience in managing a child with diarrhea seems to reduce the child's subsequent infection.
Regarding marital status, it was observed that ORS was significantly used in married mothers than divorced mothers, as well as widowed ones. It is because married mothers are supported by their spouses [28] in this situation, and it contributes significantly to their better performance in caring for a child with diarrhea.
In the current study, another variable, which was significant in the breastfeeding dimension of maternal performance, was the pregnancy type. Because in wanted pregnancy, mothers were more inclined to breastfeed. In this way, children who have a married mother that lives with her spouse and intends to get pregnant are less likely to have diarrhea [28]. Breastfeeding is a very important factor in reducing the incidence of diarrhea.
Regarding maternal performance and referral setting variables, significant differences were observed in the traditional medicine stores compared to other healthcare. The present study is in line with a study conducted by Cunnama and Honda in 2016. They found that when mothers choose healthcare providers to treat children with diarrhea, the decisions are made based on mothers' beliefs that are deeply rooted in their culture [17].
Various studies reveal that diarrhea disease remains the main cause of mortality and morbidity among children under five years old [18]. But most of the children who participated in this study were between 12 and 24 months old.
Regarding the gender of toddlers with diarrhea, most of them were boys. It is in line with a study that reported a high prevalence of diarrhea in boys [1]. While in the study of Stephen et al., more than half of the children were girls [29].
Rates of diarrhea were considerably higher among the first children in the family, which is in agreement with the result of a recent study [30]. The inexperience of the mother and unawareness of the risk factors related to diarrhea and its transmission is leading to a rise in diarrheal infections in first child care.
According to the results of this study, it is highly proposed that mothers, especially those who do not currently use any public health services, should be included and addressed in health education programs and mass media. Moreover, healthcare providers play a critical role in increasing the mother's awareness of the correct and efficient adoption of specific diets.
In this study, only mothers with toddlers were examined. It recommended that children of other developmental ages also be studied, considering the importance of the subject. It is highly suggested that mothers, especially those who do not currently use any public health services, be included and addressed in health education programs and mass media.
Conclusion
The mothers’ performance regarding diarrhea and its dietary management is low, and less than half of them have a good level of knowledge. So it is necessary to improve and implement relevant policies to control and manage diarrhea.
Acknowledgements: The authors would like to appreciate all the authorities in the hospitals under study and the mothers who participated in this research.
Ethical Permission: This article was approved by the Research Deputy of Shahid Beheshti University of Medical Sciences (The ethics code: IR.SBMU.PHARMACY.REC.1399.365).
Authors Contribution: Alkhawarah R.H. (First author), Introduction author/ Original researcher (20%); Esteki T. (Second author), Introduction author/ Methodologist (25%); Shirinabadi Farahani A. (Third author), Methodologist/ Discussion author (25%); Babaie M. (Fourth author), Introduction author/ Discussion author (15%), Nasiri M. (Fifth author), Statistical analysis (15%).
Conflicts of Interest: The authors declare no conflict of interest in this study.
Funding: This article is a part of a nursing master's thesis funded by Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Article Type: Descriptive & Survey |
Subject:
Health Literacy
Received: 2022/02/26 | Accepted: 2022/07/25 | Published: 2022/10/1
Received: 2022/02/26 | Accepted: 2022/07/25 | Published: 2022/10/1
References
1. Shafizadeh F, Nasiri-Amiri F, Sayyari A, Imanzadeh F. Mothers' knowledge and perception of childhood diarrhea and its management with diet in north and east of Tehran. Caspian J Pediatr. 2019;5(1):342-9. [Link]
2. Moradi G, Piroozi B, Safari H, Alinia C, Gouya MM, Aghili N, et al. Incidence, mortality, and burden of acute watery diarrhea and its geographical distribution in Iran during 2009-2016. Iran J Public Health. 2019;48(Supple 1):36-43. [Link]
3. Kumar S, Kumar SS, Subramanian V. Knowledge, attitude and practice regarding diarrheal disease and the use of oral rehydration therapy among mothers attending outpatient at a tertiary care hospital: A descriptive cross sectional study. J Clin Transl Neonatol. 2020;1(1):11-6. [Link]
4. Jalilvand S, Roohvand F, Arashkia A, Shoja Z. Update on epidemiology and circulating genotypes of rotavirus in Iranian children with severe diarrhea: 1986-2015. Int J Travel Med Global Health. 2018;6(1):7-10. [Link] [DOI:10.15171/ijtmgh.2018.02]
5. Kishore E, Umamahesh RM, Matli VV, Nagaram PP. Feeding practice during diarrheal episode among children aged between 6 to 23 months in Nellore District, Andhra Pradesh, South India. Int J Health Clin Res. 2021;4(6):43-6. [Link]
6. Mokomane M, Kasvosve I, Melo Ed, Pernica JM, Goldfarb DM. The global problem of childhood diarrhoeal diseases: emerging strategies in prevention and management. Ther Adv Infect Dis. 2018;5(1):29-43. [Link] [DOI:10.1177/2049936117744429]
7. Florez ID, Niño-Serna LF, Beltrán-Arroyave CP. Acute infectious diarrhea and gastroenteritis in children. Curr Infect Dis Rep. 2020;22(2):4. [Link] [DOI:10.1007/s11908-020-0713-6]
8. Sayyahfar S, Latifian M, Esmaeili P, Baseri N, Bagheri Amiri F, Bakhshi B, et al. Tropheryma whipplei in the stool samples of children with acute diarrhea: a study from Tehran, Iran. BMC Infect Dis. 2022;22(1):193. [Link] [DOI:10.1186/s12879-022-07198-5]
9. Asadi L, Pourlak T, Ahmadi B, Aghamali M, Asgharzadeh M, Aghazadeh M, et al. Etiological Agents of Pediatric Diarrhea in Ardebil, Northwestern Iran. Arch Pediatr Infect Dis. 2018;6(1):e11771. [Link] [DOI:10.5812/pedinfect.11771]
10. Azaran A, Makvandi M, Samarbafzadeh A, Neisi N, Hoseinzadeh M, Rasti M, et al. Study on Rotavirus infection and its genotyping in children below 5 years in south west Iran. Iran J Pediatr. 2016;26(2):e2080. [Link] [DOI:10.5812/ijp.2080]
11. Workie HM, Sharifabdilahi AS, Addis EM. Mothers' knowledge, attitude and practice towards the prevention and home-based management of diarrheal disease among under-five children in Diredawa, Eastern Ethiopia, 2016: a cross-sectional study. BMC Pediatr. 2018;18(1):358. [Link] [DOI:10.1186/s12887-018-1321-6]
12. Osonwa Kalu O, Eko Jimmy E, Ema S. Utilization of oral rehydration therapy in the management of diarrhea in children among nursing mothers in Odukpani local government area of cross River State, Nigeria. Am J Public Health Res. 2016;4(1):28-37. [Link]
13. Ahmad MS, Wahid A, Ahmad M, Mahboob N, Mehmood R. Prevalence of electrolyte disorders among cases of diarrhea with severe dehydration and correlation of electrolyte levels with age of the patients. J Coll Physicians Surg Pak. 2016;26(5):394-8. [Link]
14. Wekem Kukeba M, Lukman S, Darcha R, Doat A-R. Caregivers' knowledge, attitude and practice regarding diarrhoea in children under five years old in Sub-Saharan Africa: An integrative narrative review. Asian J Pediatr Res. 2021;7(4):1-27. [Link] [DOI:10.9734/ajpr/2021/v7i430220]
15. Dodicho T. Knowledge and practice of mothers/caregivers on home management of diarrhea in under five children in Mareka district, Southern Ethiopia. J Health Med Nurs. 2016;27:71-9. [Link]
16. Dietitians B. Guidelines for good nutrition in Bradford and Airedale nutrition and 1-5 years, old [Internet]. Scotland: Bradford; 2013 [cited 2021 July 6]. Available from: https://www.bradford.gov.uk/media/1908/7-nutrition-guidelines-1-to-5-years.pdf [Link]
17. Omole VN, Wamyil-Mshelia TM, Nmadu GA, Usman NO, Andeyantso EA, Adiri F. Knowledge, attitude and practice of home management of diarrhoea among mothers of under-fives in Samaru, Kaduna State, Nigeria. Port Harcourt Med J. 2019;13(1):19-25. [Link] [DOI:10.4103/phmj.phmj_23_18]
18. Padhy S, Sethi RK, Behera N. Mother's knowledge, attitude and practice regarding prevention and management of diarrhoea in children in Southern Odisha. Int J Contemp Pediatr. 2017;4(3):966-71. [Link] [DOI:10.18203/2349-3291.ijcp20171708]
19. Mohammed SI, Sabry AT, Sabry DT, Mohammed BH. Knowledge and malpractices in pediatrics diarrhea management by Iraqi mothers. Asian J Pharm Clin Res. 2018;10(8):503-7. [Link] [DOI:10.22159/ajpcr.2018.v11i8.27454]
20. Gedamu G, Kumie A, Haftu D. Magnitude and associated factors of diarrhea among under five children in Farta wereda, North West Ethiopia. Qual Prim Care. 2017;25(4):199-207. [Link]
21. Rumbo H, Sanguanprasit B, Wichaikull S. Factors influencing preventive behaviors of mothers for diarrhea in children Aged 1-5 years in Buol district, Indonesia. Sociol Stud. 2016;6(12):745-53. [Link] [DOI:10.17265/2159-5526/2016.12.001]
22. Subedi S, KumarShah S, Shah U, Mathias J, RajGautam K. Knowlege and Attitude on Diarrhea among the Mothers of under Five Year Children Living in Jajarkot, Nepal. Global J Res Analy. 2019;8(4):1-6. [Link]
23. World Health Organization. Clinical management of acute diarrhoea: WHO/UNICEF joint statement [Internet]. Geneva: World Health Organization; 2004 [cited 2021 Apr 22]. Available from: https://apps.who.int/iris/handle/10665/68627 [Link]
24. Hockenberry MJ, Wilson D. Wong's nursing care of infants and children-E-book. 11th Edition. St. Louis, Missouri: Elsevier Health Sciences; 2018. [Link]
25. Saggino A, Kline P. Item factor analysis of the Italian version of the Death Anxiety Scale. J Clin Psychol. 1996;52(3):329-33.
https://doi.org/10.1002/(SICI)1097-4679(199605)52:3<329::AID-JCLP11>3.0.CO;2-K [Link] [DOI:10.1002/(SICI)1097-4679(199605)52:33.0.CO;2-K]
26. Zahedinia F, Akaberian S, Mirzaei K, Azodi P, Dowlatkhah HR, Jahanpour F. Mothers knowledge, attitudes, and performance toward household accidents at home in children 1 5 years old: An intervention study. Nation J Physiol Pharm Pharmacol. 2018;8(5):1-6. [Link] [DOI:10.5455/njppp.2018.8.1248103012018]
27. Rosyida DAC, Hidayatunnikmah N. Maternal attitude in the handling of diarrhea in infant. Jurnal Medicoeticolegal Dan Manajemen Rumah Sakit. 2020;9(1):23-9. [Link] [DOI:10.18196/jmmr.91113]
28. Mutalik AV, Raje VV. Relationship between maternal education and socioeconomic status on knowledge, attitude and practice of mother and her child regarding acute diarrhoeal diseases. Int J Commun Med Public Health. 2017;4(12):4472-6. [Link] [DOI:10.18203/2394-6040.ijcmph20175155]
29. Stephen B, Apidechkul T, Suma Y, Suttana W. Maternal knowledge, attitude and practices related to diarrhea in children aged less than five years in Kabarole district, Uganda. J Public Health Dev. 2016;14(2):33-48. [Link]
30. Asfaha KF, Tesfamichael FA, Fisseha GK, Misgina KH, Weldu MG, Welehaweria NB, et al. Determinants of childhood diarrhea in Medebay Zana District, Northwest Tigray, Ethiopia: A community based unmatched case-control study. BMC Pediatr. 2018;18(1):1-9. [Link] [DOI:10.1186/s12887-018-1098-7]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |