



Volume 10, Issue 1 (2022)
Health Educ Health Promot 2022, 10(1): 145-153 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Izadirad H, Delshad M, Pourhaji F, Pourhaji F. Health Literacy and Self-Care in Diabetes Disease; a Systematic Review. Health Educ Health Promot 2022; 10 (1) :145-153
URL: http://hehp.modares.ac.ir/article-5-55088-en.html
URL: http://hehp.modares.ac.ir/article-5-55088-en.html
1- Department of Health, Khash School of Health, Zahedan University of Medical Sciences, Zahedan, Iran
2- “Department of Public Health, School of Health” and “Health Sciences Research Center”, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran
3- “Department of Health Promotion and Education, School of Health” and “Student Research Committee”, Mashhad University of Medical Sciences, Iran
2- “Department of Public Health, School of Health” and “Health Sciences Research Center”, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran
3- “Department of Health Promotion and Education, School of Health” and “Student Research Committee”, Mashhad University of Medical Sciences, Iran
Full-Text [PDF 510 kb]
(1034 Downloads)
| Abstract (HTML) (1098 Views)
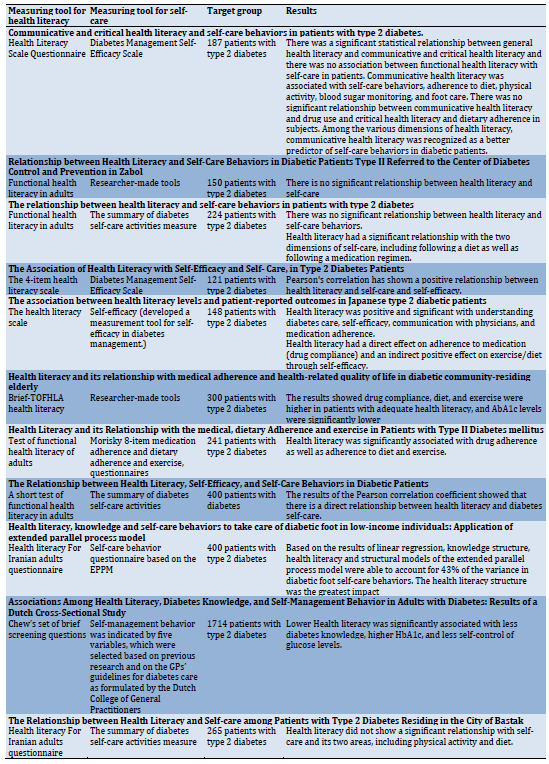
Table 1) Characteristics and information related to studies based on health literacy and self-care of diabetic patients

Continue of Table 1) Characteristics and information related to studies based on health literacy and self-care of diabetic patients
Discussion
the present study was conducted to review the relationship between health literacy and self-care of diabetic patients. One of the largest challenges is the increasing burden of chronic diseases such as diabetes in today's world.
Health literacy is a global issue, and according to the World Health Organization (WHO), it plays a key role in determining health equality, both in high and low-income countries [14-16]. Despite the growing importance of health literacy in improving and promoting community health, studies have been conducted limited worldwide, especially self-care in patients with diabetes.
Generally, the results of various studies show the level of health literacy is not desirable in the community worldwide [14, 22, 23].
The review of the present study showed a different relationship between health literacy and self-care in patients with type 2 diabetes so, in some of the studies, there was no significant relationship between health literacy and self-care of patients with type 2 diabetes [13, 14, 24-26].
The reasons for different results in the studies may be due to the following:
Various studies have used different tools to measure health literacy in patients with diabetes. Overall, the design and implementation of health literacy assessment tools are typically limited in time and population. In other words, a significant number of these tools are designed for certain nationalities and languages, including the native versions of TOFHLA and S-TOFHLA [27].
Also, some health literacy assessment tools are designed in a specific language, which is limited due to the specificity of the language spoken in some parts of the world and the limited number of people who speak only this language.
These tools include functional, critical, and communicative health literacy assessment tools, and adult health literacy review tools that are available in a variety of languages [28]. It seems that the lack of a valid international standard tool for measuring the level of health literacy, which can measure people's health literacy in a wide range of scientific disciplines in different countries and a certain class, can be one of the causes of differences in the results of various studies.
Another reason can be attributed to differences in the scope of measurement of different instruments, as several existing instruments only focus on measuring basic skills such as reading and counting, while several other instruments, such as TOFHLA, have a relatively complex structure to answer and to measure functional health literacy or the HLIA tool, which measures five areas of health literacy on a larger scale, including access, reading skills, comprehension, evaluation and decision making, and the use of health information. As a result, due to the different levels of difficulty of different tools, the level of health literacy of communities and, therefore, the relationship between health literacy and self-care can be effective.
Therefore, since the basis for developing health literacy assessment tools is theoretical or practical, defined in scientific documents, it seems that in practice, this index is not measured by a fixed or definite approach or concept. As a result, despite these differences and the incompleteness of definitions, the inevitable result is different and it denies researchers and decision-makers to compare and draw conclusions on a wide range.
Various studies applied different tools to measure health literacy in patients with type 2 diabetes. Overall, it has limited assessment tools for designing and implementing health literacy in terms of time and population. In other words, a significant number of these tools are designed for certain nationalities and languages, including the native versions of TOFHLA and S-TOFHLA [27].
Also, some health literacy assessment tools are designed in a specific language, which is limited due to the specificity of the language spoken in some parts of the world and the limited number of people who speak only this language.
These tools include functional, critical, and communicative health literacy assessment tools, and adult health literacy review tools that are available in a variety of languages [28]. It seems the lack of an internationally valid and standard tool for measuring the level of health literacy-measure people's health literacy in a wide range of scientific disciplines in different countries and a certain class= can be one of the causes of different results in the various studies.
Another reason is different in the scope of measurement in instruments because the number of existing instruments only focus on measuring basic skills such as reading and counting. In contrast, some other instruments such as TOFHLA have a relatively difficult structure to answer the audience and measure functional health literacy or the HLIA scale measures five areas of health literacy on a larger scale, including access, reading skills, comprehension, evaluation and decision making, and the use of health information. Then, because of the different levels of difficulty in health literacy scales of communities, therefore, the relationship between health literacy and self-care can be effective.
Therefore, since in scientific documents, the basis of health literacy scales is theoretical or practical defined, it seems that this concept is not measured by a fixed or definite approach. As a result, despite these differences and the incompleteness of definitions, the inevitable result is different and it denies researchers and decision-makers to compare and draw conclusions on a wide range.
It also appears differences in the self-care status of diabetic patients are a reason for conflicting results. Because factors such as differences in self-care training programs, the level of self-care knowledge and attitudes, as well as differences in how self-care for diabetic patients, can cause self-care behavior was different in various countries and even regions of the country.
It seems different age groups in diabetic patients could be another reason for the discrepancy between the results examined in studies. For example, problems related to vision and other complications that are affecting factors on skills related to functional health literacy are more common in older patients with type 2 diabetes [29-32], They can be a contributing factor to self-care and health literacy. These disorders can also affect the completion of the questionnaire and self-report. It seems previous studies examined only one or two variable concepts of health literacy and self-care behaviors and they had contradictory results.
Conducting studies in different countries with cultural, social, and economic differences education level, place of residence and economic status have been the most important factors that have been studied in different studies on different population groups. In most studies the level of education and economic status have been mentioned as two factors affecting health literacy [33-40].
Studies have also shown that residents of developed areas are more likely to follow health behaviors. Also, social and cultural characteristics have the greatest impact on people's health behaviors. In addition, political and economic characteristics, directly and indirectly, affect health and health behaviors [29, 41-44].
It seems that because studies on health literacy and diabetes self-care have been conducted in different countries with different cultural, social, political, and economic characteristics, these differences can be another reason for the contradictory results of health literacy on self-care diabetic.
It also seems that one of the important and effective factors in contradictory results is the effect of health literacy on self-efficacy as an important mediating factor affecting self-care. Because, skills related to health literacy, including communicative and critical skills, are essential and effective factors in improving self-care behaviors in diabetic patients. Because these skills can increase self-confidence and self-efficacy and help them build effective relationships with health care providers. Such capabilities could eventually allow patients to receive necessary information from various communication channels and evaluate and practice [45-47].
Also, in the study of Reisi et al. [22], self-efficacy was introduced as a strong determinant of diabetes care, so that patients with a high level of self-efficacy had better self-care in diabetes [29].
It seems that the indirect effect of health literacy on the self-care of diabetic patients is achieved through self-efficacy. Also, the study of Panahi et al. [48] showed that health literacy as a facilitating factor directly affects self-efficacy and indirectly influences the adoption of preventive behaviors [48-51]. It can be understood that health literacy is a set of skills, capabilities, and capacities in several dimensions.
The skills and capacities, sometimes in the dimension of obtaining medical information and health, reading them, understanding, processing, and interpretation, and decision-making and implementation of this information emerge and in this way can affect both self-efficacy as an important mediator and self-care.
Conclusion
Health literacy plays an important and key role in promoting self-care behaviors in diabetic patients. It requires paying attention to health literacy and adopting strategies to improve the health literacy of diabetic patients.
Acknowledgments: The authors sincerely appreciate all the researchers whose studies have been used in the present study.
Ethical permissions: This article was reviewe and has no human or animal examples.
Conflicts of Interest: We declare that we have no conflicts of interest.
Authors' contribution: Izadirad H (First Author), Methodologist/Statistical Analyst (30%); Delshad MH (Second Author), Introduction Writer/Discussion Writer (25%); Pourhaji F (Third Author), Introduction Writer (25%); Pourhaji F (Forth Author) Assistant Researcher (20%).
Funding/Support: No funding.
Full-Text: (274 Views)
Introduction
Over the decades, much research has been done to answer how health literacy affects people's health [1-3].
Health literacy is the capacity and ability to obtain, process, and understand health information and services they need for decision-making about their health [4-7]. In these studies, health literacy has been introduced as an influencing factor in the health status, treatment outcome, and physician-patient relationship. The increasing health literacy of diabetic patients makes it easier to understand dietary information, insulin injections, and glucose control. On the other hand, health literacy plays a vital role in accepting their illness.
The results of these studies show that health literacy helps people to be more involved in therapeutic decisions. Also, individuals with higher health literacy pay more attention to their health literacy status [4, 8-12]. Other research examined the relationship between health literacy and patients' self-care behaviors.
These studies have shown that physicians 'attention to patients' health literacy levels, training classes, and various audiovisual media to transfer information about the illness have effectively improved self-care behaviors, self-efficacy, and understanding of the complexity of diabetes [4, 13].
Health literacy is widely regarded as a determinant of health and a priority on the public health policy agenda, and it has the greatest impact on diabetes prevention [14-16].
Low health literacy is more common in the elderly, immigrants, illiterate and low-income people, individuals with low mental health, and patients with chronic diseases such as diabetes type 2 and hypertension. These individuals are considered at-risk groups with adverse effects on low levels of health literacy [17].
Individuals with low health literacy suffer higher medical costs, have poorer health status, and are more likely to be hospitalized and use emergency services. These people have less preventive care. The research suggested that a low level of health literacy is associated with a low level of health, wider inequalities, and higher costs of the health system, addressing the issue of health literacy. It seems essential to use strategies to promote it in society [4].
Diabetes is a metabolic disorder caused by non-secretion or decreasing the hormone insulin [18]. According to World Health Organization (WHO), diabetes is a silent epidemic [13]. This disease is the leading cause of mortality worldwide, so it is estimated that the number of people with diabetes will increase from 171 million in 2000 to more than 366 million in 2030 worldwide [18]. Studies show that patients suffer from side effects of diabetes after 15 years of morbidity (10% with severe visual impairment, 50% with retinopathy, and 75% from heart disease [19, 20]. The American Diabetes Association (ADA) classifies diabetes into four subgroups: type 1 diabetes, type 2 diabetes, gestational diabetes, and other types of diabetes. It depends on obesity, insulin resistance, physical inactivity, genetics, and environmental factors [19, 20].
Self-care improves the quality of life and reduces treatment costs. On the other hand, self-care is influenced by one's beliefs, attitudes, and the values and culture of the society in which one lives. Self-improvement is possible through education. Patient education is an essential component of diabetes control. Many scholars consider the control and treatment of diabetes as the main task of the individual and family and believe patients must accept responsibility to control their disease. One of the important goals in diabetes control is to empower patients to take care of themselves [21].
Self-care in diabetes includes proper and timely insulin injections, diet, regular exercise, detection of high or low blood sugar symptoms, regular use of medications, foot care, and quality of life [13].
Due to the studies performed in a geographical area and limited population about health literacy and self-care of diabetic patients with various tools, methods, procedures, and contexts in the world, It makes necessary to conduct a systematic review and prepare a more accurate report.
The result of this study can be a good basis for the expertise of specialists and the decision of health officials to improve the level of health literacy and consequently improve self-care and improve the quality of life in diabetic patients ultimately. Since the introduction of health literacy, several studies have been conducted on its application. There is little research about self-care in diabetic patients and its effect on health literacy. Then, it seems necessary a review health literacy and self-care in the diabetic patient. Therefore, the present study was conducted to review the relationship between health literacy and self-care of diabetic patients.
Information and Methods
The present study is a systematic review based on the PRISMA statement and was conducted in 2020. An electronic search was implemented for articles in Persian and English in Iran Medex, SID, Magiran databases, Web of Science, PubMed, Scopus, Google Scholar, and Science Direct from January 2011 to April 2020. The terms were used including health literacy, self-care diabetes, health literacy, and diabetes. To maximize the comprehensiveness of the search in Persian references, general and general Persian keywords, including health literacy, self-care, diabetes self-care, health literacy, and self-care, health literacy, and diabetes and their possible combinations in the abstract, title, and keywords were used “AND” and “OR” operators were used for this purpose. For the English equivalent of Latin and MESHE, the words were searched, including “Health literacy”, “diabetes”, “self-care”, “Diabetes self-care”, and a combination of the “AND” and “OR” operators. In the Google Scholar database, the keywords were entered in the title field, and all the articles in the database were reviewed. Inclusion criteria included 1- Quantitative and cross-sectional design in study 2-Both health literacy and self-care in patients with type II diabetes studied, 3- The full text of the article should be available. Short articles and letters to the editor were deleted.
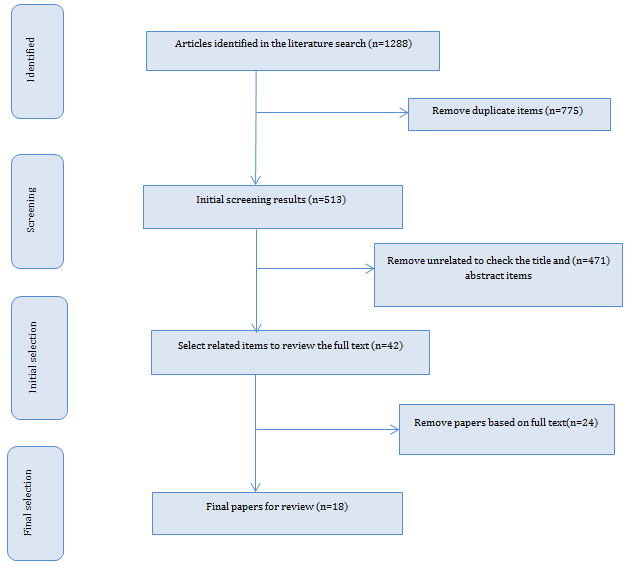
Guidelines developed at the PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses, included a checklist and a flow chart. First, the members of the systematic review team were determined including the supervisor, consultant group, researcher, extractor, data collector, article seeker, and final browser. Firstly, the articles were searched in the title and their abstracts. Then irrelevant and duplicate items were removed. In the next step, the texts of the remaining articles were reviewed, and removed the unrelated items. Finally, 18 selected articles [1, 4, 13, 17, 21, 24-29, 33, 37, 41, 42, 45, 51, 52, ] (Figure 1). To prevent bias in the study, searching, selecting studies, evaluating qualitative, and extracting data were conducted independently by two researchers, and any disagreement between the two researchers was evaluated by a third. Then, All articles that entered the study process were reviewed with a predefined checklist. The checklist included the title, journal name, type of study, target group, volume, sampling method, and results
Over the decades, much research has been done to answer how health literacy affects people's health [1-3].
Health literacy is the capacity and ability to obtain, process, and understand health information and services they need for decision-making about their health [4-7]. In these studies, health literacy has been introduced as an influencing factor in the health status, treatment outcome, and physician-patient relationship. The increasing health literacy of diabetic patients makes it easier to understand dietary information, insulin injections, and glucose control. On the other hand, health literacy plays a vital role in accepting their illness.
The results of these studies show that health literacy helps people to be more involved in therapeutic decisions. Also, individuals with higher health literacy pay more attention to their health literacy status [4, 8-12]. Other research examined the relationship between health literacy and patients' self-care behaviors.
These studies have shown that physicians 'attention to patients' health literacy levels, training classes, and various audiovisual media to transfer information about the illness have effectively improved self-care behaviors, self-efficacy, and understanding of the complexity of diabetes [4, 13].
Health literacy is widely regarded as a determinant of health and a priority on the public health policy agenda, and it has the greatest impact on diabetes prevention [14-16].
Low health literacy is more common in the elderly, immigrants, illiterate and low-income people, individuals with low mental health, and patients with chronic diseases such as diabetes type 2 and hypertension. These individuals are considered at-risk groups with adverse effects on low levels of health literacy [17].
Individuals with low health literacy suffer higher medical costs, have poorer health status, and are more likely to be hospitalized and use emergency services. These people have less preventive care. The research suggested that a low level of health literacy is associated with a low level of health, wider inequalities, and higher costs of the health system, addressing the issue of health literacy. It seems essential to use strategies to promote it in society [4].
Diabetes is a metabolic disorder caused by non-secretion or decreasing the hormone insulin [18]. According to World Health Organization (WHO), diabetes is a silent epidemic [13]. This disease is the leading cause of mortality worldwide, so it is estimated that the number of people with diabetes will increase from 171 million in 2000 to more than 366 million in 2030 worldwide [18]. Studies show that patients suffer from side effects of diabetes after 15 years of morbidity (10% with severe visual impairment, 50% with retinopathy, and 75% from heart disease [19, 20]. The American Diabetes Association (ADA) classifies diabetes into four subgroups: type 1 diabetes, type 2 diabetes, gestational diabetes, and other types of diabetes. It depends on obesity, insulin resistance, physical inactivity, genetics, and environmental factors [19, 20].
Self-care improves the quality of life and reduces treatment costs. On the other hand, self-care is influenced by one's beliefs, attitudes, and the values and culture of the society in which one lives. Self-improvement is possible through education. Patient education is an essential component of diabetes control. Many scholars consider the control and treatment of diabetes as the main task of the individual and family and believe patients must accept responsibility to control their disease. One of the important goals in diabetes control is to empower patients to take care of themselves [21].
Self-care in diabetes includes proper and timely insulin injections, diet, regular exercise, detection of high or low blood sugar symptoms, regular use of medications, foot care, and quality of life [13].
Due to the studies performed in a geographical area and limited population about health literacy and self-care of diabetic patients with various tools, methods, procedures, and contexts in the world, It makes necessary to conduct a systematic review and prepare a more accurate report.
The result of this study can be a good basis for the expertise of specialists and the decision of health officials to improve the level of health literacy and consequently improve self-care and improve the quality of life in diabetic patients ultimately. Since the introduction of health literacy, several studies have been conducted on its application. There is little research about self-care in diabetic patients and its effect on health literacy. Then, it seems necessary a review health literacy and self-care in the diabetic patient. Therefore, the present study was conducted to review the relationship between health literacy and self-care of diabetic patients.
Information and Methods
The present study is a systematic review based on the PRISMA statement and was conducted in 2020. An electronic search was implemented for articles in Persian and English in Iran Medex, SID, Magiran databases, Web of Science, PubMed, Scopus, Google Scholar, and Science Direct from January 2011 to April 2020. The terms were used including health literacy, self-care diabetes, health literacy, and diabetes. To maximize the comprehensiveness of the search in Persian references, general and general Persian keywords, including health literacy, self-care, diabetes self-care, health literacy, and self-care, health literacy, and diabetes and their possible combinations in the abstract, title, and keywords were used “AND” and “OR” operators were used for this purpose. For the English equivalent of Latin and MESHE, the words were searched, including “Health literacy”, “diabetes”, “self-care”, “Diabetes self-care”, and a combination of the “AND” and “OR” operators. In the Google Scholar database, the keywords were entered in the title field, and all the articles in the database were reviewed. Inclusion criteria included 1- Quantitative and cross-sectional design in study 2-Both health literacy and self-care in patients with type II diabetes studied, 3- The full text of the article should be available. Short articles and letters to the editor were deleted.
Guidelines developed at the PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses, included a checklist and a flow chart. First, the members of the systematic review team were determined including the supervisor, consultant group, researcher, extractor, data collector, article seeker, and final browser. Firstly, the articles were searched in the title and their abstracts. Then irrelevant and duplicate items were removed. In the next step, the texts of the remaining articles were reviewed, and removed the unrelated items. Finally, 18 selected articles [1, 4, 13, 17, 21, 24-29, 33, 37, 41, 42, 45, 51, 52, ] (Figure 1). To prevent bias in the study, searching, selecting studies, evaluating qualitative, and extracting data were conducted independently by two researchers, and any disagreement between the two researchers was evaluated by a third. Then, All articles that entered the study process were reviewed with a predefined checklist. The checklist included the title, journal name, type of study, target group, volume, sampling method, and results
Figure 1) Flow Chart of study entry to a systematic review
Findings
The results showed different sampling methods so that 14 studies (77.77%) used simple random sampling, 1 study (5.55%) census, 2 The study (11.11%) was performed using the multistage sampling, and one study (5.55%) was performed by the cluster sampling. In these studies, patients with type 2 diabetes were studied from different age groups so that the minimum age of the patients was 28 years and the maximum age was 87 years.
To assess health literacy, various assessment tools such as a short survey of adult functional health literacy (STOFHLA) in 4 studies (22.22%), a communication and Persian critical versionin1 study (5.55%), and European health literacy were used. Questionnaire (47 cases) in a study (5.55%), version of the Japanese Functional, Communication and Critical Health Literacy Questionnaire (Ishikawa), in five studies (27.77%), in one study (5.55%) of the Adult Functional Literacy Test, Questionnaire Chewing health literacy screening in two studies (11.11%), in two studies (11.11%) the Adult Functional Health Literacy Questionnaire (TOFHLA), in two studies (11.11%) the Iranian Adult Health Literacy Questionnaire (HELIA) was used. In 27.77% of the studies, there was no statistically significant relationship between health literacy and self-care of type2 diabetic patients. The findings of the selected studies are reported in Table 1.
The results showed different sampling methods so that 14 studies (77.77%) used simple random sampling, 1 study (5.55%) census, 2 The study (11.11%) was performed using the multistage sampling, and one study (5.55%) was performed by the cluster sampling. In these studies, patients with type 2 diabetes were studied from different age groups so that the minimum age of the patients was 28 years and the maximum age was 87 years.
To assess health literacy, various assessment tools such as a short survey of adult functional health literacy (STOFHLA) in 4 studies (22.22%), a communication and Persian critical versionin1 study (5.55%), and European health literacy were used. Questionnaire (47 cases) in a study (5.55%), version of the Japanese Functional, Communication and Critical Health Literacy Questionnaire (Ishikawa), in five studies (27.77%), in one study (5.55%) of the Adult Functional Literacy Test, Questionnaire Chewing health literacy screening in two studies (11.11%), in two studies (11.11%) the Adult Functional Health Literacy Questionnaire (TOFHLA), in two studies (11.11%) the Iranian Adult Health Literacy Questionnaire (HELIA) was used. In 27.77% of the studies, there was no statistically significant relationship between health literacy and self-care of type2 diabetic patients. The findings of the selected studies are reported in Table 1.
Table 1) Characteristics and information related to studies based on health literacy and self-care of diabetic patients
Continue of Table 1) Characteristics and information related to studies based on health literacy and self-care of diabetic patients
Discussion
the present study was conducted to review the relationship between health literacy and self-care of diabetic patients. One of the largest challenges is the increasing burden of chronic diseases such as diabetes in today's world.
Health literacy is a global issue, and according to the World Health Organization (WHO), it plays a key role in determining health equality, both in high and low-income countries [14-16]. Despite the growing importance of health literacy in improving and promoting community health, studies have been conducted limited worldwide, especially self-care in patients with diabetes.
Generally, the results of various studies show the level of health literacy is not desirable in the community worldwide [14, 22, 23].
The review of the present study showed a different relationship between health literacy and self-care in patients with type 2 diabetes so, in some of the studies, there was no significant relationship between health literacy and self-care of patients with type 2 diabetes [13, 14, 24-26].
The reasons for different results in the studies may be due to the following:
Various studies have used different tools to measure health literacy in patients with diabetes. Overall, the design and implementation of health literacy assessment tools are typically limited in time and population. In other words, a significant number of these tools are designed for certain nationalities and languages, including the native versions of TOFHLA and S-TOFHLA [27].
Also, some health literacy assessment tools are designed in a specific language, which is limited due to the specificity of the language spoken in some parts of the world and the limited number of people who speak only this language.
These tools include functional, critical, and communicative health literacy assessment tools, and adult health literacy review tools that are available in a variety of languages [28]. It seems that the lack of a valid international standard tool for measuring the level of health literacy, which can measure people's health literacy in a wide range of scientific disciplines in different countries and a certain class, can be one of the causes of differences in the results of various studies.
Another reason can be attributed to differences in the scope of measurement of different instruments, as several existing instruments only focus on measuring basic skills such as reading and counting, while several other instruments, such as TOFHLA, have a relatively complex structure to answer and to measure functional health literacy or the HLIA tool, which measures five areas of health literacy on a larger scale, including access, reading skills, comprehension, evaluation and decision making, and the use of health information. As a result, due to the different levels of difficulty of different tools, the level of health literacy of communities and, therefore, the relationship between health literacy and self-care can be effective.
Therefore, since the basis for developing health literacy assessment tools is theoretical or practical, defined in scientific documents, it seems that in practice, this index is not measured by a fixed or definite approach or concept. As a result, despite these differences and the incompleteness of definitions, the inevitable result is different and it denies researchers and decision-makers to compare and draw conclusions on a wide range.
Various studies applied different tools to measure health literacy in patients with type 2 diabetes. Overall, it has limited assessment tools for designing and implementing health literacy in terms of time and population. In other words, a significant number of these tools are designed for certain nationalities and languages, including the native versions of TOFHLA and S-TOFHLA [27].
Also, some health literacy assessment tools are designed in a specific language, which is limited due to the specificity of the language spoken in some parts of the world and the limited number of people who speak only this language.
These tools include functional, critical, and communicative health literacy assessment tools, and adult health literacy review tools that are available in a variety of languages [28]. It seems the lack of an internationally valid and standard tool for measuring the level of health literacy-measure people's health literacy in a wide range of scientific disciplines in different countries and a certain class= can be one of the causes of different results in the various studies.
Another reason is different in the scope of measurement in instruments because the number of existing instruments only focus on measuring basic skills such as reading and counting. In contrast, some other instruments such as TOFHLA have a relatively difficult structure to answer the audience and measure functional health literacy or the HLIA scale measures five areas of health literacy on a larger scale, including access, reading skills, comprehension, evaluation and decision making, and the use of health information. Then, because of the different levels of difficulty in health literacy scales of communities, therefore, the relationship between health literacy and self-care can be effective.
Therefore, since in scientific documents, the basis of health literacy scales is theoretical or practical defined, it seems that this concept is not measured by a fixed or definite approach. As a result, despite these differences and the incompleteness of definitions, the inevitable result is different and it denies researchers and decision-makers to compare and draw conclusions on a wide range.
It also appears differences in the self-care status of diabetic patients are a reason for conflicting results. Because factors such as differences in self-care training programs, the level of self-care knowledge and attitudes, as well as differences in how self-care for diabetic patients, can cause self-care behavior was different in various countries and even regions of the country.
It seems different age groups in diabetic patients could be another reason for the discrepancy between the results examined in studies. For example, problems related to vision and other complications that are affecting factors on skills related to functional health literacy are more common in older patients with type 2 diabetes [29-32], They can be a contributing factor to self-care and health literacy. These disorders can also affect the completion of the questionnaire and self-report. It seems previous studies examined only one or two variable concepts of health literacy and self-care behaviors and they had contradictory results.
Conducting studies in different countries with cultural, social, and economic differences education level, place of residence and economic status have been the most important factors that have been studied in different studies on different population groups. In most studies the level of education and economic status have been mentioned as two factors affecting health literacy [33-40].
Studies have also shown that residents of developed areas are more likely to follow health behaviors. Also, social and cultural characteristics have the greatest impact on people's health behaviors. In addition, political and economic characteristics, directly and indirectly, affect health and health behaviors [29, 41-44].
It seems that because studies on health literacy and diabetes self-care have been conducted in different countries with different cultural, social, political, and economic characteristics, these differences can be another reason for the contradictory results of health literacy on self-care diabetic.
It also seems that one of the important and effective factors in contradictory results is the effect of health literacy on self-efficacy as an important mediating factor affecting self-care. Because, skills related to health literacy, including communicative and critical skills, are essential and effective factors in improving self-care behaviors in diabetic patients. Because these skills can increase self-confidence and self-efficacy and help them build effective relationships with health care providers. Such capabilities could eventually allow patients to receive necessary information from various communication channels and evaluate and practice [45-47].
Also, in the study of Reisi et al. [22], self-efficacy was introduced as a strong determinant of diabetes care, so that patients with a high level of self-efficacy had better self-care in diabetes [29].
It seems that the indirect effect of health literacy on the self-care of diabetic patients is achieved through self-efficacy. Also, the study of Panahi et al. [48] showed that health literacy as a facilitating factor directly affects self-efficacy and indirectly influences the adoption of preventive behaviors [48-51]. It can be understood that health literacy is a set of skills, capabilities, and capacities in several dimensions.
The skills and capacities, sometimes in the dimension of obtaining medical information and health, reading them, understanding, processing, and interpretation, and decision-making and implementation of this information emerge and in this way can affect both self-efficacy as an important mediator and self-care.
Conclusion
Health literacy plays an important and key role in promoting self-care behaviors in diabetic patients. It requires paying attention to health literacy and adopting strategies to improve the health literacy of diabetic patients.
Acknowledgments: The authors sincerely appreciate all the researchers whose studies have been used in the present study.
Ethical permissions: This article was reviewe and has no human or animal examples.
Conflicts of Interest: We declare that we have no conflicts of interest.
Authors' contribution: Izadirad H (First Author), Methodologist/Statistical Analyst (30%); Delshad MH (Second Author), Introduction Writer/Discussion Writer (25%); Pourhaji F (Third Author), Introduction Writer (25%); Pourhaji F (Forth Author) Assistant Researcher (20%).
Funding/Support: No funding.
Article Type: Systematic Review |
Subject:
Health Literacy
Received: 2021/08/24 | Accepted: 2021/09/30 | Published: 2022/04/11
Received: 2021/08/24 | Accepted: 2021/09/30 | Published: 2022/04/11
References
1. Reisi M, Mostafavi F, Javadzade H, Mahaki B, Tavassoli E, Sharifirad G. Communicative and critical health literacy and self-care behaviors in patients with type 2 diabetes. Iran J Diabetes Metab. 2015;14(3):199-208. [Persian] [Link]
2. Bailey SC, Brega AG, Crutchfield TM, Elasy T, Herr H, Kaphingst K, et al. Update on health literacy and diabetes. Diabetes Educ. 2014;40(5):581-604. [Link] [DOI:10.1177/0145721714540220]
3. Berkman ND, Davis TC, McCormack L. Health literacy: What is it?. J Health Commun. 2010;15 Suppl 2:9-19. [Link] [DOI:10.1080/10810730.2010.499985]
4. Vasli P, Eshghbaz F. Survey condition regarding self- caring of children suffering from diabetes type 1 and It's relation with family reaction. J Mazandaran Univ Med Sci. 2009;19(69):38-44. [Persian] [Link]
5. Shahbazi H, Ghofranipour F, Amiri P, Rajab A . Factors affecting self-care performance in adolescents with type I diabetes according to the PEN-3 cultural model. Int J Endocrinol Metab. 2018;16(4):e62582. [Link] [DOI:10.5812/ijem.62582]
6. Tavousi M, Ebadi M, Azin SA, Shakerinejad Gh, Hashemi A, Fattahi E, et al. Definitions of health literacy: A review of the literature. PAYESH. 2014;13(1):119-24. [Persian] [Link]
7. Esteghamati A, Etemad K, Koohpayehzadeh J, Abbasi M, Meysamie A, Noshad S, et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005-2011. Diabetes Res Clin Pract. 2014;103(2):319-27. [Link] [DOI:10.1016/j.diabres.2013.12.034]
8. Kooshyar H, Shoorvazi M, Dalir Z, Hosseini M. Health literacy and its relationship with medical adherence and health-related quality of life in diabetic community-residing elderly. J Mazandaran Univ Med Sci. 2014;23(1):134-43. [Persian] [Link]
9. Mehrtak M, Hemmati A, Bakhshzadeh A. Health literacy and its relationship with the medical, dietary adherence and exercise in patients with type II Diabetes mellitus. J Health Literacy. 2018;3(2):137-44. [Link]
10. Goli Roshan A, Hosseinkhani S N, Norouzadeh R. The relationship between health literacy of elderly diabetics and adherence to treatment, Babol, Iran, 2021. Qom Univ Med Sci J. 2021;14(12):70-80. [Persian] [Link] [DOI:10.52547/qums.14.12.70]
11. Hussain N, Said AS, Khan ZJIqoche. Influence of health literacy on medication adherence among elderly females with type 2 diabetes in Pakistan. Int Q Community Health Educ. 2020;41(1):35-44. [Link] [DOI:10.1177/0272684X19896724]
12. Jeong J, Park N, Shin SYJJoKAoCHN. The influence of health literacy and diabetes knowledge on diabetes self-care activities in Korean low-income elders with diabetes. J Korean Acad Community Health Nurs. 2014;25(3):217-24. [Link] [DOI:10.12799/jkachn.2014.25.3.217]
13. AbbasZadeh Bazzi M, Karimiaval M. Relationship between health literacy and self-care behaviors in diabetic patients type II referred to the center of diabetes control and prevention in Zabol. J Health Literacy. 2018;3(1):10-9. [Link]
14. Seyedoshohadaee M, Barasteh S, Jalalinia F, Eghbali M, Nezami M. The relationship between health literacy and self-care behaviors in patients with type 2 diabetes. Iran J Nurs Res. 2016;10(4):43-51. [Link]
15. Borhaninejad V, Iranpour A, Shati M, Naghibzadeh Tahami A, Yousefzadeh G, Fadayevatan R. Predictors of self-care among the elderly with diabetes type 2: using social cognitive theory. Diabetes Metab Syndr. 2017;11(3):163-6. [Link] [DOI:10.1016/j.dsx.2016.08.017]
16. Nigatu T. Epidemiology, complications and management of diabetes in Ethiopia: a systematic review. J Diabetes. 2012;4(2):174-80. [Link] [DOI:10.1111/j.1753-0407.2011.00181.x]
17. Peyman N, Samiee-Roudi K. Investigating the status of health literacy among health providers of rural area. J Health Literacy. 2016;1(1):46-52. [Link]
18. Telo GH, Cureau FV, de Souza MS, Andrade TS, Copês F, Schaan BD. Prevalence of diabetes in Brazil over time: a systematic review with meta-analysis. Diabetol Metab Syndr. 2016;8:65. [Link] [DOI:10.1186/s13098-016-0181-1]
19. Bianco A, Pomara F, Thomas E, Paoli A, Battaglia G, Petrucci M, et al. Type 2 diabetes family histories, body composition and fasting glucose levels: a cross-section analysis in healthy sedentary male and female. Iran J Public Health. 2013;42(7):681-90. [Link]
20. Goran MI, Coronges K, Bergman RN, Cruz ML, Gower BA. Influence of family history of type 2 diabetes on insulin sensitivity in prepubertal children. J Clin Endocrinol Metab. 2003;88(1):192-5. [Link] [DOI:10.1210/jc.2002-020917]
21. Lael-Monfared E, Tehrani H, Moghaddam ZE, Ferns GA, Tatari M, Jafari A. Health literacy, knowledge and self-care behaviors to take care of diabetic foot in low-income individuals: Application of extended parallel process model. Diabetes Metab Syndr. 2019;13(2):1535-41. [Link] [DOI:10.1016/j.dsx.2019.03.008]
22. Reisi M, Mostafavi F, Javadzade H, Mahaki B, Tavassoli E, Sharifirad G. Impact of health literacy, self-efficacy, and outcome expectations on adherence to self-care behaviors in iranians with type 2 diabetes. Oman Med J. 2016;31(1):52-9. [Link] [DOI:10.5001/omj.2016.10]
23. de Oliveira Santos MIP, Portella MR. Conditions of functional health literacy of an elderly diabetics group. Revista Brasileira de Enfermagem. 2016;69(1):144-52. [Link]
24. Almigbal TH, Almutairi KM, Vinluan JM, Batais MA, Alodhayani A, Alonazi WB, et al. Association of health literacy and self-management practices and psychological factor among patients with type 2 diabetes mellitus in Saudi Arabia. Saudi Med J. 2019;40(11):1158-66. [Link] [DOI:10.15537/smj.2019.11.24585]
25. Banihashemi T SA, Amirkhani MA. Health literacy and the influencing factors: a study in five provinces of Iran. Strides Dev Med Educ J. 2007;4(1):1-9. [Link]
26. Maneze D, Everett B, Astorga C, Yogendran D, Salamonson Y. The influence of health literacy and depression on diabetes self-management: a cross-sectional study. J Diabetes Res. 2016;2016:3458969. [Link] [DOI:10.1155/2016/3458969]
27. Chang LC, Hsieh PL, Liu CH. Psychometric evaluation of the Chinese version of short‐form test of functional health literacy in adolescents. J Clin Nurs. 2012;21(17‐18):2429-37. [Link] [DOI:10.1111/j.1365-2702.2012.04147.x]
28. Tavousi M, Ebadi M, Fattahi E, Jahangiry L, Hashemi A, Hashemiparast M, et al. Health literacy measures: A systematic review of the literature. PAYESH. 2015;14(4):485-96. [Persian] [Link]
29. Abbaszadeh M, Alizadeh E, Badri GR, Vedadhir A. Investigation of social and cultural factors affecting self-care lifestyle of citizens. J Stud Soc Cult Dev. 2012;1:119-41. [Persian] [Link]
30. Osokpo O, Riegel B. Cultural factors influencing self-care by persons with cardiovascular disease: An integrative review. Int J Nurs Stud. 2021;116:103383. [Link] [DOI:10.1016/j.ijnurstu.2019.06.014]
31. Gurmu Y, Gela D, Aga F. Factors associated with self-care practice among adult diabetes patients in West Shoa Zone, Oromia Regional State, Ethiopia. BMC Health Serv Res.2018;18:732. [Link] [DOI:10.1186/s12913-018-3448-4]
32. Bohanny W, Vivienne Wu SF, Liu CY, Yeh SH, Tsay SL, Wang TJ. Health literacy, self-efficacy, and self-care behaviors in patients with type 2 diabetes mellitus. J Am Assoc Nurs Pract. 2013;25(9):495-502. [Link] [DOI:10.1111/1745-7599.12017]
33. Saatchi M, Panahi M, Ashraf Mozafari A, Sahebkar M, Azarpakan A, Baigi V, et al. Health literacy and its associated factors: A population-based study, Hormuz Island. Iran J Epidemiol. 2017;13(2):136-44. [Persian] [Link]
34. Mohammed BAS, Fujii Y, Kiriya J, Fujiya R, Giacaman R, Kitamura A, et al. Exploring health literacy and its associated factors among Palestinian university students: a cross-sectional study. Health Promot Int. 2021;36(3):854-65. [Link] [DOI:10.1093/heapro/daaa089]
35. Moeini B, Rostami-Moez M, Besharati F, Faradmal J, Bashirian S. Adult functional health literacy and its related factors: a cross-sectional study. Int J Epidemiol Res. 2019;6(1):24-9. [Link] [DOI:10.15171/ijer.2019.05]
36. Ansari H, Almasi Z, Ansari-Moghaddam A, Mohammadi M, Peyvand M, et al. Health literacy in older adults and its related factors: a cross-sectional study in southeast Iran. Health Scope. 2016;5(4):e37453. [Persian] [Link] [DOI:10.17795/jhealthscope-37453]
37. Mohammadi Farah S, Saati Asr MH, Kavivani Manesh A, Barati M, Afshari M, Mohammadi Y. Health literacy level and its related factors among college students of Hamadan University of Medical Sciences, Hamadan, Iran. J Educ Community Health. 2017;4(2):11-7. [Link] [DOI:10.21859/jech.4.2.11]
38. Baji Z, Tehrani M, Shakerinejad G, Jarvandi F, Hajinajaf S. Health literacy level and its related demographic factors among employees of iranian academic center for education, culture & research (ACECR)-Khuzestan Branch. J Health Literacy. 2019;3(4):46-54. [Link]
39. Dehghankar L, Panahi R, Kekefallah L, Hosseini N, Hasannia E. The study of health literacy and its related factors among female students at high schools in Qazvin. J Health Literacy. 2019;4(2):18-26. [Link]
40. Taheri S, Tavousi M , Momenimovahed Z , Direkvand-Moghadam A , Rezaei N, et al. Determining health literacy level and its related factors among pregnant women referred to medical and health centers of Tehran in 2019: a cross-sectional study. Shiraz E Med J. 2021;22(10);e109592 [Link] [DOI:10.5812/semj.109592]
41. Tol A, Mohebbi B, Yekaninejad M, Sabouri M. Influential factors on health promoting behaviors and happiness among women. Razi J Med Sci. 2018;25(169):11-22. [Persian] [Link]
42. Fathnezhad-Kazemi A, Hajian S. Factors influencing the adoption of health promoting behaviors in overweight pregnant women: a qualitative study. BMC Pregnancy Childbirth. 2019;19:43. [Link] [DOI:10.1186/s12884-019-2199-5]
43. Harooni J, Hassanzadeh A, Mostafavi F. Influencing factors on health promoting behavior among the elderly living in the community. J Educ Health Promot. 2014;3:40. [Link]
44. Pishkar Mofrad Z, Jahantigh M, Arbabisarjou A. Health promotion behaviors and chronic diseases of aging in the elderly people of Iranshahr*- IR Iran. Glob J Health Sci. 2015;8(3):139-45. [Link] [DOI:10.5539/gjhs.v8n3p139]
45. Lai AY, Ishikawa H, Kiuchi T, Mooppil N, Griva K. Communicative and critical health literacy, and self-management behaviors in end-stage renal disease patients with diabetes on hemodialysis. Patient Educ Couns. 2013;91(2):221-7. [Link] [DOI:10.1016/j.pec.2012.12.018]
46. Heijmans M, Waverijn G, Rademakers J, van der Vaart R, Rijken M. Functional, communicative and critical health literacy of chronic disease patients and their importance for self-management. Patient Educ Couns. 2015;98(1):41-8. [Link] [DOI:10.1016/j.pec.2014.10.006]
47. Rafiezadeh Gs, Tabarsy B, Hassanjani S, Razavi M, Amjady M, Hojjati H. Relationship between the Health Literacy with selfefficacy of the diabetic patient's type 2 referred to Gorgan city clinic in 2014. J Diabetes Nurs. 2015;3(2):30-42. [Persian] [Link]
48. Panahi R, Ramezankhani A, Tavousi M, Haeri Mehrizi A, Rezaei M, Niknami S. Investigating the health literacy influencing ways on the adoption of smoking preventive behaviors in health belief model developed by health literacy. J Health Field. 2018;6(2):232-43. [Persian] [Link]
49. Panahi R, Ramezankhani A, Tavousi M, Osmani F, Karami A, Niknami S. Effect of educational intervention on health literacy and adoption of smoking preventive behaviors among university students. J Educ Community Health. 2018;5(2):26-35. [Link] [DOI:10.21859/jech.5.2.26]
50. Khaleghi M. Evaluating the effect of educational intervention on health literacy through social networks to promote quality of life for students [Dissertation]. Tehran: Tarbiat Modares University; 2017. [Persian] [Link]
51. van der Heide I, Uiters E, Rademakers J, Struijs JN, Schuit AJ, Baan CA. Associations among health literacy, diabetes knowledge, and self-management behavior in adults with diabetes: results of a dutch cross-sectional study. J Health Commun. 2014;19 Suppl 2:115-31. [Link] [DOI:10.1080/10810730.2014.936989]
52. Ghaedi M, Banihashemi F, Latifi M, Soleymaninejad M. The relationship between health literacy and self-care among patients with type 2 diabetes residing in the city of Bastak. Iran J Endocrinol Metab. 2016;18(2):90-6. [Persian] [Link]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |