



Volume 10, Issue 2 (2022)
Health Educ Health Promot 2022, 10(2): 265-269 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fallahi S, Hesam A, Arabi A, Shojaee A, Zoghi G, Hesam M, et al . The Self-Report Symptoms of COVID-19 in Iranian Population Through a Teleconsultation-Based Service. Health Educ Health Promot 2022; 10 (2) :265-269
URL: http://hehp.modares.ac.ir/article-5-54525-en.html
URL: http://hehp.modares.ac.ir/article-5-54525-en.html
S. Fallahi1  , A.A. Hesam2 , A. Arabi2 , A. Shojaee3 , Gh. Zoghi4 , M.J. Hesam5 , Z. Shahali2 , A. Ayoubian * 2
, A.A. Hesam2 , A. Arabi2 , A. Shojaee3 , Gh. Zoghi4 , M.J. Hesam5 , Z. Shahali2 , A. Ayoubian * 2
, A.A. Hesam2 , A. Arabi2 , A. Shojaee3 , Gh. Zoghi4 , M.J. Hesam5 , Z. Shahali2 , A. Ayoubian * 2
1- Cardiovascular Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran
2- National Center for Health Insurance Research, Tehran, Iran
3- Department of Health Management and Economics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
4- Endocrinology and Metaolism Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran
5- Department of Business Management, Middle East College, Muscat, Oman
2- National Center for Health Insurance Research, Tehran, Iran
3- Department of Health Management and Economics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
4- Endocrinology and Metaolism Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran
5- Department of Business Management, Middle East College, Muscat, Oman
Keywords: COVID-19 [MeSH], Remote Consultation [MeSH], Risk Factors [MeSH], Mass Screening [MeSH], Iran [MeSH]
Full-Text [PDF 797 kb]
(916 Downloads)
| Abstract (HTML) (1172 Views)
Full-Text: (147 Views)
Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first originated in Wuhan, Hubei province, China in December 2019. The rapid spread of the disease all over the world led to its declaration as a global pandemic by the World Health Organization (WHO) on March 11, 2020 [1]. The current COVID-19 pandemic has become a significant burden on the healthcare systems of many countries worldwide including Iran [2].
Transmission to healthcare personnel caring for COVID-19 patients and to people with no direct exposure to the animal market, believed to be the origin of the disease, suggested person-to-person transmission as one of the main modes of transmission, either by direct contact or through droplets produced when coughing or sneezing. Therefore, a very important strategy to prevent the spread of the disease in many countries has been patient isolation [3]. On the other hand, due to the limited resources, it has been crucial to saving the available medical services for those in more critical conditions. In addition, a shortage of medical supplies and hospital beds requires primary screening for COVID-19 to avoid unnecessary hospital admissions [4, 5]. Moreover, although COVID-19 appears to present with various manifestations, some symptoms especially when not accompanied by the most common ones such as fever, cough, and dyspnea, are highly unlikely to arise from SARS-CoV-2 infection; patients with these symptoms can become infected in the process of seeking medical attention in overcrowded hospitals and healthcare centers [6].
Teleconsultation has been used for different diseases amid the COVID-19 crisis including diabetes,7 mental disorders, urological problems, rheumatologic diseases, as well as COVID-19 primary screening and triage to reduce hospital referrals [8-11]. In order to deal with this disease, it is necessary to present its basic symptoms to the community to reduce the spread of this disease by being aware of these symptoms. Therefore this study evaluated the patients’ complaints during the initial period of the COVID-19 pandemic in Iran, recorded from a telephone-based interview with patients calling for a consultation.
Instrument & Methods
In this cross-sectional study, individuals calling for COVID-19 screening and consultation from 2 March 2020 to 19 April 2020 in Iran were included. Inclusion criteria included all individuals who had at least one symptom of COVID-19, and exclusion criteria included incomplete information and questions about prevention and additional information about the disease. Therefore, according to these cases, all 12125 people from the whole country were included in the study with the census method. All contacts were classified into 2 levels in general, 358000 calls were made at the 1st level, from which 53000 were referred to the 2nd level.
A checklist including age, gender, COVID-19-related symptoms, comorbidities, risk factors such as contact with an infected person and history of presence in highly affected areas, and doctors’ recommendations was filled out for each participant.
The current study was approved by the Tehran University of Medical Sciences. In addition, verbal permissions were obtained from callers to obtain the requested information. A telephone number (1666) was assigned by the Iran Health Insurance Organization (IHIO) for consultation with more than 70 nurses responding to first-level questions and more than 30 medical doctors responding to second-level questions. Nurses were trained to refer the necessary calls to the 2nd level. If nurses were unable to answer participants’ questions, they were referred to the 2nd level. The participant who called this number asked questions about themselves or their family and acquaintances about COVID-19 symptoms and they consulted about this disease for the necessary measures for recovery.
Mean, standard deviation, frequency, and percentages were used to describe the results. Chi-squared test was used to compare qualitative variables. Univariate logistic regression analysis was used to determine the relationship between symptoms and risk factors with COVID-19. Statistical Package for the Social Sciences (SPSS) software version 25.0 (Armonk, NY: IBM Corp.) was used for data analysis. P-values ≤0.05 were regarded as statistically significant.
Findings
The mean age of the patients was 37.76±16.61 years. Of the 12125 participants in the current study, 43.5% were male. Table 1 demonstrates the prevalence of symptoms in the participants. Cough was the most common complaint, followed by shortness of breath, and fever. Other common symptoms with more than 20% prevalence included sore throat, body ache/muscle pain, chills (20.9%), and gastrointestinal symptoms, respectively (Table 1).
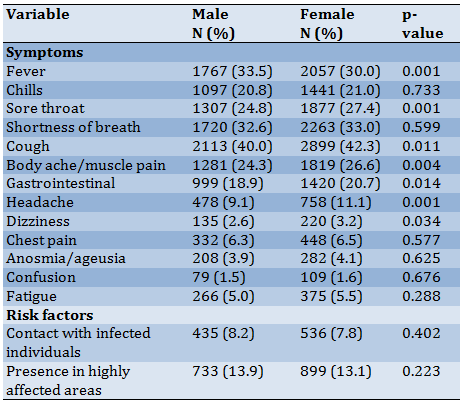
Fever was significantly more prevalent among male patients while sore throat, cough, body ache, gastrointestinal symptoms, headache, and dizziness were significantly more prevalent among female participants. No significant difference was found between males and females regarding risk factors (Table 2).
Table 1) Gender, symptoms, risk factor, and recommendations of the study population
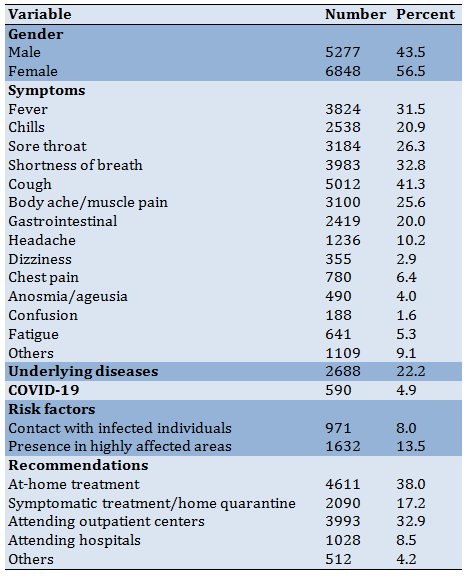
Table 2) Patients’ symptoms and risk factors by gender
Univariate logistic regression revealed that men were at a higher risk of COVID-19 compared to women (OR:1.31, 95% CI 1.10-1.55, p=0.002). In addition, older age was a risk factor for COVID-19 (OR:1.02, 95% CI 1.02-1.03, p<0.001). Also, significant positive relationships were found between fever, chills, sore throat, shortness of breath, cough, body ache, and gastrointestinal symptoms with COVID-19 even after adjustment for gender and age.
Discussion
COVID-19 pandemic was mild during the initial stages and its prolonged incubation period led to a rapid increase in the number of infected cases. Later on, with a high proportion of the infected patients progressing to acute respiratory distress syndrome, the increasing mortality rate, and the person-to-person spread of the disease, governments started to take measures to isolate the afflicted individuals and limit the expansion of COVID-19 [12].
Many studies have reported the common symptoms of COVID-19. At the onset of the disease, the most common symptoms appear to be fever, cough, and fatigue, as well as headache, diarrhea, dyspnea, and hemoptysis mentioned in some studies [13-17]. Similarly, in the current study cough was the most common complaint, followed by shortness of breath/dyspnea, and fever. Other common symptoms with more than 20% prevalence included sore throat, body ache/muscle pain, chills, and gastrointestinal symptoms. Also, Khairat et al. [18] in their study entitle telehealth experience of patients with COVID-19 symptoms stated that the most common diagnoses for patients with COVID-19 symptoms were an upper respiratory infection.
Fever was significantly more prevalent among male patients while sore throat, cough, body ache, gastrointestinal symptoms, headache, and dizziness were significantly more prevalent among female participants. No significant difference was found between males and females regarding risk factors. We found that 22.2% of the participants had an underlying disease or comorbidity. The prevalence of self-reported COVID-19 was 4.9%. Regarding risk factors, 8% of participants had contact with an infected individual and 13.5% had been too highly affected areas.
In the current study, most patients were recommended to stay home and receive at-home treatment (38%), while 32.9% were referred to outpatient centers and only 8.5% to hospitals. Home quarantine was recommended for 17.2% of the participants. Fever was significantly more prevalent among male patients while sore throat, cough, body ache, gastrointestinal symptoms, headache, and dizziness were significantly more prevalent among female participants. No significant difference was found between males and females regarding risk factors.
In our study men were at higher risk of COVID-19 compared to women. The results of several previous studies have been in line with this finding [19-24]. This has been attributed to the higher prevalence of smoking and cardiopulmonary diseases in men increasing their susceptibility to COVID-19. Also, angiotensin-converting enzyme 2 (ACE2) expression as a primary gateway of SARS-CoV-2 introduction into the body seems to be higher in men [25]. In addition, older age was a risk factor for COVID-19. Also, significant positive correlations were found between fever, chills, sore throat, shortness of breath, cough, body ache, and gastrointestinal symptoms with COVID-19 even after adjustment for gender and age.
The strength of this study was that it included a very large number of people which gives an accurate estimation of the general population. There are also some limitations regarding the current study. First, several symptoms such as fever need to be confirmed by physical examination. The patients might feel feverish but their body temperature may not be within the range of the clinical definition of fever. Second, certain diagnoses of COVID-19 can only be made through reverse transcriptase-polymerase chain reaction (RT-PCR) for virus DNA and/or typical computed tomography (CT) findings, both of which were not possible to obtain through teleconsultation.
There are limitations to the present study. First: Several symptoms such as fever should be confirmed by physical examination. The patient may feel feverish but the body temperature is not high enough to determine the clinical definition of fever.
Conclusion
The present study suggests that fever, cough, and shortness of breath are the most common complaints in individuals calling for COVID-19 teleconsultation. The future holds great promise for teleconsultation after the COVID-19 crisis, and thereby, there is a need to optimize telehealth practices to make it a more sustainable, effective, and meaningful health care delivery medium.
Acknowledgments: None declared.
Ethical Permissions: The study was approved by the Tehran University of Medical Sciences with a code of IR.TUMS.MEDICINE.REC.1399.968.
Conflicts of Interests: None declared.
Authors’ Contributions: Fallahi S (First Author), Conception/Design/Main Researcher (20%); Hesam A.A (Second Author), Methodologist/ Assistant Researcher (10%); Arabi A (Third Author), Assistant Researcher/Discussion Writer (10%); Shojaee A (Fourth author), Main Researcher/Design (10%); Zoghi Gh (Fifth author), Introduction Writer/Main Researcher/Statistical Analyst (10%); Hesam M.J (Sixth author), Methodologist /Assistant Researcher (10%); Shahali Z (Seventh author), Introduction Writer/Assistant Researcher (10%); Ayoubain A (Eighth author), Methodologist Main Researcher/Discussion Writer (20%).
Funding/Support: None declared.
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first originated in Wuhan, Hubei province, China in December 2019. The rapid spread of the disease all over the world led to its declaration as a global pandemic by the World Health Organization (WHO) on March 11, 2020 [1]. The current COVID-19 pandemic has become a significant burden on the healthcare systems of many countries worldwide including Iran [2].
Transmission to healthcare personnel caring for COVID-19 patients and to people with no direct exposure to the animal market, believed to be the origin of the disease, suggested person-to-person transmission as one of the main modes of transmission, either by direct contact or through droplets produced when coughing or sneezing. Therefore, a very important strategy to prevent the spread of the disease in many countries has been patient isolation [3]. On the other hand, due to the limited resources, it has been crucial to saving the available medical services for those in more critical conditions. In addition, a shortage of medical supplies and hospital beds requires primary screening for COVID-19 to avoid unnecessary hospital admissions [4, 5]. Moreover, although COVID-19 appears to present with various manifestations, some symptoms especially when not accompanied by the most common ones such as fever, cough, and dyspnea, are highly unlikely to arise from SARS-CoV-2 infection; patients with these symptoms can become infected in the process of seeking medical attention in overcrowded hospitals and healthcare centers [6].
Teleconsultation has been used for different diseases amid the COVID-19 crisis including diabetes,7 mental disorders, urological problems, rheumatologic diseases, as well as COVID-19 primary screening and triage to reduce hospital referrals [8-11]. In order to deal with this disease, it is necessary to present its basic symptoms to the community to reduce the spread of this disease by being aware of these symptoms. Therefore this study evaluated the patients’ complaints during the initial period of the COVID-19 pandemic in Iran, recorded from a telephone-based interview with patients calling for a consultation.
Instrument & Methods
In this cross-sectional study, individuals calling for COVID-19 screening and consultation from 2 March 2020 to 19 April 2020 in Iran were included. Inclusion criteria included all individuals who had at least one symptom of COVID-19, and exclusion criteria included incomplete information and questions about prevention and additional information about the disease. Therefore, according to these cases, all 12125 people from the whole country were included in the study with the census method. All contacts were classified into 2 levels in general, 358000 calls were made at the 1st level, from which 53000 were referred to the 2nd level.
A checklist including age, gender, COVID-19-related symptoms, comorbidities, risk factors such as contact with an infected person and history of presence in highly affected areas, and doctors’ recommendations was filled out for each participant.
The current study was approved by the Tehran University of Medical Sciences. In addition, verbal permissions were obtained from callers to obtain the requested information. A telephone number (1666) was assigned by the Iran Health Insurance Organization (IHIO) for consultation with more than 70 nurses responding to first-level questions and more than 30 medical doctors responding to second-level questions. Nurses were trained to refer the necessary calls to the 2nd level. If nurses were unable to answer participants’ questions, they were referred to the 2nd level. The participant who called this number asked questions about themselves or their family and acquaintances about COVID-19 symptoms and they consulted about this disease for the necessary measures for recovery.
Mean, standard deviation, frequency, and percentages were used to describe the results. Chi-squared test was used to compare qualitative variables. Univariate logistic regression analysis was used to determine the relationship between symptoms and risk factors with COVID-19. Statistical Package for the Social Sciences (SPSS) software version 25.0 (Armonk, NY: IBM Corp.) was used for data analysis. P-values ≤0.05 were regarded as statistically significant.
Findings
The mean age of the patients was 37.76±16.61 years. Of the 12125 participants in the current study, 43.5% were male. Table 1 demonstrates the prevalence of symptoms in the participants. Cough was the most common complaint, followed by shortness of breath, and fever. Other common symptoms with more than 20% prevalence included sore throat, body ache/muscle pain, chills (20.9%), and gastrointestinal symptoms, respectively (Table 1).
Fever was significantly more prevalent among male patients while sore throat, cough, body ache, gastrointestinal symptoms, headache, and dizziness were significantly more prevalent among female participants. No significant difference was found between males and females regarding risk factors (Table 2).
Table 1) Gender, symptoms, risk factor, and recommendations of the study population
Table 2) Patients’ symptoms and risk factors by gender
Univariate logistic regression revealed that men were at a higher risk of COVID-19 compared to women (OR:1.31, 95% CI 1.10-1.55, p=0.002). In addition, older age was a risk factor for COVID-19 (OR:1.02, 95% CI 1.02-1.03, p<0.001). Also, significant positive relationships were found between fever, chills, sore throat, shortness of breath, cough, body ache, and gastrointestinal symptoms with COVID-19 even after adjustment for gender and age.
Discussion
COVID-19 pandemic was mild during the initial stages and its prolonged incubation period led to a rapid increase in the number of infected cases. Later on, with a high proportion of the infected patients progressing to acute respiratory distress syndrome, the increasing mortality rate, and the person-to-person spread of the disease, governments started to take measures to isolate the afflicted individuals and limit the expansion of COVID-19 [12].
Many studies have reported the common symptoms of COVID-19. At the onset of the disease, the most common symptoms appear to be fever, cough, and fatigue, as well as headache, diarrhea, dyspnea, and hemoptysis mentioned in some studies [13-17]. Similarly, in the current study cough was the most common complaint, followed by shortness of breath/dyspnea, and fever. Other common symptoms with more than 20% prevalence included sore throat, body ache/muscle pain, chills, and gastrointestinal symptoms. Also, Khairat et al. [18] in their study entitle telehealth experience of patients with COVID-19 symptoms stated that the most common diagnoses for patients with COVID-19 symptoms were an upper respiratory infection.
Fever was significantly more prevalent among male patients while sore throat, cough, body ache, gastrointestinal symptoms, headache, and dizziness were significantly more prevalent among female participants. No significant difference was found between males and females regarding risk factors. We found that 22.2% of the participants had an underlying disease or comorbidity. The prevalence of self-reported COVID-19 was 4.9%. Regarding risk factors, 8% of participants had contact with an infected individual and 13.5% had been too highly affected areas.
In the current study, most patients were recommended to stay home and receive at-home treatment (38%), while 32.9% were referred to outpatient centers and only 8.5% to hospitals. Home quarantine was recommended for 17.2% of the participants. Fever was significantly more prevalent among male patients while sore throat, cough, body ache, gastrointestinal symptoms, headache, and dizziness were significantly more prevalent among female participants. No significant difference was found between males and females regarding risk factors.
In our study men were at higher risk of COVID-19 compared to women. The results of several previous studies have been in line with this finding [19-24]. This has been attributed to the higher prevalence of smoking and cardiopulmonary diseases in men increasing their susceptibility to COVID-19. Also, angiotensin-converting enzyme 2 (ACE2) expression as a primary gateway of SARS-CoV-2 introduction into the body seems to be higher in men [25]. In addition, older age was a risk factor for COVID-19. Also, significant positive correlations were found between fever, chills, sore throat, shortness of breath, cough, body ache, and gastrointestinal symptoms with COVID-19 even after adjustment for gender and age.
The strength of this study was that it included a very large number of people which gives an accurate estimation of the general population. There are also some limitations regarding the current study. First, several symptoms such as fever need to be confirmed by physical examination. The patients might feel feverish but their body temperature may not be within the range of the clinical definition of fever. Second, certain diagnoses of COVID-19 can only be made through reverse transcriptase-polymerase chain reaction (RT-PCR) for virus DNA and/or typical computed tomography (CT) findings, both of which were not possible to obtain through teleconsultation.
There are limitations to the present study. First: Several symptoms such as fever should be confirmed by physical examination. The patient may feel feverish but the body temperature is not high enough to determine the clinical definition of fever.
Conclusion
The present study suggests that fever, cough, and shortness of breath are the most common complaints in individuals calling for COVID-19 teleconsultation. The future holds great promise for teleconsultation after the COVID-19 crisis, and thereby, there is a need to optimize telehealth practices to make it a more sustainable, effective, and meaningful health care delivery medium.
Acknowledgments: None declared.
Ethical Permissions: The study was approved by the Tehran University of Medical Sciences with a code of IR.TUMS.MEDICINE.REC.1399.968.
Conflicts of Interests: None declared.
Authors’ Contributions: Fallahi S (First Author), Conception/Design/Main Researcher (20%); Hesam A.A (Second Author), Methodologist/ Assistant Researcher (10%); Arabi A (Third Author), Assistant Researcher/Discussion Writer (10%); Shojaee A (Fourth author), Main Researcher/Design (10%); Zoghi Gh (Fifth author), Introduction Writer/Main Researcher/Statistical Analyst (10%); Hesam M.J (Sixth author), Methodologist /Assistant Researcher (10%); Shahali Z (Seventh author), Introduction Writer/Assistant Researcher (10%); Ayoubain A (Eighth author), Methodologist Main Researcher/Discussion Writer (20%).
Funding/Support: None declared.
Article Type: Descriptive & Survey |
Subject:
Health Promotion Setting
Received: 2021/08/2 | Accepted: 2022/01/28 | Published: 2022/06/14
Received: 2021/08/2 | Accepted: 2022/01/28 | Published: 2022/06/14
References
1. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020;91(1):157-60. [Link]
2. Raoofi A, Takian A, Sari AA, Olyaeemanesh A, Haghighi H, Aarabi M. COVID-19 pandemic and comparative health policy learning in Iran. Arch Iran Med. 2020;23(4):220-34. [Link] [DOI:10.34172/aim.2020.02]
3. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433. [Link] [DOI:10.1016/j.jaut.2020.102433]
4. Her M. Repurposing and reshaping of hospitals during the COVID-19 outbreak in South Korea. One Health. 2020;10:100137. [Link] [DOI:10.1016/j.onehlt.2020.100137]
5. Emanuel EJ, Persad G, Upshur R, Thome B, Parker M, Glickman A, et al. Fair allocation of scarce medical resources in the time of Covid-19. N En J Med. 2020;382(21):2049-55. [Link] [DOI:10.1056/NEJMsb2005114]
6. Synowiec A, Szczepański A, Barreto-Duran E, Lie LK, Pyrc K. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): a systemic infection. Clin Microbiol Rev. 2021;34(2):e00133-20. [Link] [DOI:10.1128/CMR.00133-20]
7. Banerjee M, Chakraborty S, Pal R. Teleconsultation and diabetes care amid COVID-19 pandemic in India: scopes and challenges. J Diabetes Sci Technol. 2020;14(4):714-5. [Link] [DOI:10.1177/1932296820929391]
8. Idris H. Utilization of Teleconsultation: Mitigation in Handling Mental Disorders in the COVID-19 Era. Int J Ment Health Addic. 2020;19(6):2320-22. [Link] [DOI:10.1007/s11469-020-00323-y]
9. Pinar U, Anract J, Perrot O, Tabourin T, Chartier-Kastler E, Parra J, et al. Preliminary assessment of patient and physician satisfaction with the use of teleconsultation in urology during the COVID-19 pandemic. World J Urol. 2020;39(6):1991-6. [Link] [DOI:10.1007/s00345-020-03432-4]
10. Shenoy P, Ahmed S, Paul A, Skaria TG, Joby J, Alias B. Switching to teleconsultation for rheumatology in the wake of the COVID-19 pandemic: feasibility and patient response in India. Clin Rheumatol. 2020;39(9):2757-62. [Link] [DOI:10.1007/s10067-020-05200-6]
11. Davarpanah AH, Mahdavi A, Sabri A, Langroudi TF, Kahkouee S, Haseli S, et al. Novel screening and triage strategy in Iran during deadly Coronavirus Disease 2019 (COVID-19) Epidemic: value of Humanitarian Teleconsultation Service. J Am Coll Radiol. 2020;17(6):734-8. [Link] [DOI:10.1016/j.jacr.2020.03.015]
12. Ghebreyesus TA. WHO Director-General's opening remarks at the media briefing on COVID-19-11 March 2020. Geneva: World Health Organization; 2020. [Link]
13. Ren LL, Wang YM, Wu ZQ, Xiang ZC, Guo L, Xu T, et al. Identification of a novel coronavirus causing severe pneumonia in human: a descriptive study. Chin Med J. 2020;133(9):1015-24. [Link] [DOI:10.1097/CM9.0000000000000722]
14. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. lancet. 2020;395(10223):497-506. [Link] [DOI:10.1016/S0140-6736(20)30183-5]
15. Wang W, Tang J, Wei F. Updated understanding of the outbreak of 2019 novel coronavirus (2019‐nCoV) in Wuhan, China. J Medl Virol. 2020;92(4):441-7. [Link] [DOI:10.1002/jmv.25689]
16. Carlos WG, Dela Cruz CS, Cao B, Pasnick S, Jamil S. Novel Wuhan (2019-nCoV) Coronavirus. Am J Respir Crit Care Med. 2020;201(4):P7-8. [Link] [DOI:10.1164/rccm.2014P7]
17. Jin X, Lian JS, Hu JH, Gao J, Zheng L, Zhang YM, et al. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut. 2020;69(6):1002-9. [Link] [DOI:10.1136/gutjnl-2020-320926]
18. Khairat S, Pillai M, Edson B, Gianforcaro R. Evaluating the telehealth experience of patients with COVID-19 symptoms: recommendations on best practices. J Patient Exp. 2020;7(5):665-72. [Link] [DOI:10.1177/2374373520952975]
19. Li LQ, Huang T, Wang Yq, Wang Zp, Liang Y, Huang Tb, et al. COVID‐19 patients' clinical characteristics, discharge rate, and fatality rate of meta‐analysis. J Med Virol. 2020;92(6):577-83. [Link] [DOI:10.1002/jmv.25757]
20. Chen T, Wu D, Chen H, Yan W, Yang D, Chen G, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020;368:m1091. [Link] [DOI:10.1136/bmj.m1091]
21. Mo P, Xing Y, Xiao Y, Deng L, Zhao Q, Wang H, et al. Clinical characteristics of refractory COVID-19 pneumonia in Wuhan, China. Clin Infecti Dis. 2020;73(11):e4208-13. [Link] [DOI:10.1093/cid/ciaa270]
22. Liu R, Han H, Liu F, Lv Z, Wu K, Liu Y, et al. Positive rate of RT-PCR detection of SARS-CoV-2 infection in 4880 cases from one hospital in Wuhan, China, from Jan to Feb 2020. Clini Chim Acta. 2020;505:172-5. [Link] [DOI:10.1016/j.cca.2020.03.009]
23. Leung C. Clinical features of deaths in the novel coronavirus epidemic in China. Rev Med Virol. 2020:e2103. [Link] [DOI:10.1002/rmv.2103]
24. Xu K, Chen Y, Yuan J, Yi P, Ding C, Wu W, et al. Factors associated with prolonged viral RNA shedding in patients with coronavirus disease 2019 (COVID-19). Clin Infect Dis. 2020;71(15):799-806. [Link] [DOI:10.1093/cid/ciaa351]
25. Kopel J, Perisetti A, Roghani A, Aziz M, Gajendran M, Goyal H. Racial and gender-based differences in COVID-19. Front Public Health. 2020;8:418. [Link] [DOI:10.3389/fpubh.2020.00418]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |