



Volume 9, Issue 3 (2021)
Health Educ Health Promot 2021, 9(3): 251-256 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rahimi F, Lamyian M, Maasoumi R. Female Orgasm Scale: Translation and Psychometric Assessment of an Iranian Version. Health Educ Health Promot 2021; 9 (3) :251-256
URL: http://hehp.modares.ac.ir/article-5-50858-en.html
URL: http://hehp.modares.ac.ir/article-5-50858-en.html
1- Department of Reproductive Health and Midwifery, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
2- School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran ,r_masoumi@sina.tums.ac.ir
2- School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran ,
Full-Text [PDF 521 kb]
(4272 Downloads)
| Abstract (HTML) (2851 Views)
Full-Text: (3490 Views)
Introduction
According to Masters and Johnson's model, the sexual response cycle consists of four stages, excitement, plateau, orgasm, and resolution [1]. The female orgasm is influenced by several factors and plays a crucial role in sexual compatibility and marital satisfaction [2]. In women, orgasm involves the myotonic response of the smooth and striated muscles, along with a sense of sexual stress relief emanating from the stimulation period. Orgasm is described as the most pleasurable sexual sensation [3]. During orgasm, 3 to 5 regular contractions occur in the vagina, perineum, and anal muscles, each of which lasts 0.8 seconds and reaches the uterus [4]. Clitoral tissue is the most sensitive part of anatomical sex for most women that stimulates the most powerful sexual feelings and orgasms [3]. Physiological and mental changes during orgasm are variable and differ among women proportionate to their conditions [5].
Persistent or recurrent delay in or absence of orgasm following a normal excitement phase is defined as Female orgasmic disorder (FOD) by the Diagnostic and Statistical Manual of Mental Disorders 4th Ed. (DSM-IV) [6]. Reduced intensity, delay, infrequency, or absence of orgasm for at least six months, which is not related to other physical, mental, or relational problems, is added by the DSM-V for more explanations of FOD [6].
Results of several studies suggest that the prevalence of orgasmic disorders among women is 18-61% in the general population [7]. Wolpe et al. reported that the prevalence of female sexual dysfunctions in Brazil was between 13.33 and 73.3%, and the orgasmic performance was 18.0-55.4% [8]. According to Zhang et al., the prevalence of sexual dysfunctions in women aged 20-70 in China was 29.7%, and orgasm was 27.9% [9]. According to a survey conducted by Ramezani et al., the prevalence of orgasmic disorders among women in the general population of Iran was 35.3% [10].
FOD is a multidimensional problem influenced by personal, relational, psychological, sociocultural, and religious context factors [11, 12]. Accurate FOD assessment requires applying a gender-based, culturally competent, valid, and reliable instrument [13]. The Female Orgasm Scale (FOS) is a gender-based, short, self-administered tool designed to assess female orgasm. The validity of the FOS questionnaire was assessed by Fisher et al. [14] in Canada for the first time. The study was conducted on three groups of women (n=651) aged 17–49 years. The main feature of the FOS is its assessment of orgasm during sex, including vaginal intercourse and clitoral stimulation. So, it seems that FOS is a culturally safe instrument for assessing orgasm among Iranian women.
Nevertheless, the cross-cultural adaptation of FOS in the Iranian population is necessary. Cross-cultural adaptation is defined as a process that includes language and cultural adaptation of a questionnaire for use in another setting and community [14]. The cultural adaptation process consists of three steps: translation, cross-cultural adaptation, and verification of the instrument's psychometric properties in the target population (i.e., standardization) [15].
There is no valid and reliable Persian version of FOS. Thus, this study aimed to translate and test the psychometric properties of the Iranian version of FOS –namely its cross-cultural adaptation- from English to Persian.
Instrument and Methods
This was a cross-sectional study carried out in Tehran, Iran, during September-December 2018. Two hundred thirty-five women attending three maternal health and family planning centers affiliated with Tehran and Beheshti Universities of Medical Sciences for routine care (excluding pregnancy) were chosen through convenience sampling. The inclusion criteria were aged 15 to 49 (reproductive age), married and sexually active, not pregnant, and willing to participate in the study. Thirty-five women did not agree to fill the IV-FOS; So, 200 women completed the questionnaire for construct validity assessment.
The FOS is a short, self-administered questionnaire developed by McIntyre-Smith & Fisher [14]. It assesses the consistency of female orgasm during partnered sexual activities (e.g., intercourse, oral stimulation, self-stimulation in the partner's presence) and overall satisfaction with orgasm frequency and quality. The scale is comprised of seven items. Five items inquire about the frequency of orgasm during different sexual activities: (a) intercourse, (b) intercourse with additional direct clitoral stimulation, (c) manual stimulation of the clitoris and/or genitals by a partner, (d) self-stimulation of the clitoris and/or genitals in the presence of a partner, and (e) oral stimulation. Two other items assess perceived satisfaction with the number and quality of orgasms experienced during sexual activity with a partner. This scale has two subscales: orgasm from clitoral stimulation and orgasmic satisfaction. In this scale, items 1-5 are scored as 0%=0, 10%=1, 20%=2 … 100%=10. Items 6-7 are scored as "Very Unsatisfied" = 1 to "Very Satisfied" = 7. Because items 1-5 are essentially coded on a 10-point scale, and the rest are coded on a 7-point scale, items should be weighted in the following manner: a) multiply items 1-5 by 7; b) Multiply items 6-7 by 10. Scoring the responses marked "Does not apply to me" can be coded as 0, depending on the researcher's rationale and use of the scale [15].
After obtaining a translation permit from the main author, the tool was translated into Persian. The concepts in the translated version were matched with the ones in the original version in the five following steps:
Step 1-Forward translation: The questionnaire was translated separately by two English translators who were native Persian speakers.
Step 2-Expert panel: At this stage, the integration of the two translated versions was done by the panel of experts. The two translators took part in a meeting, reviewed the translations, and reached a consensus after exchanging views, leading to an identical final version. At this stage, the goal was to check the terminology and rectify the deficiencies.
Step 3-Backward translation: The two translators (whose mother tongue was English) and had sufficient fluency in Persian, and had not yet received the English version of the questionnaire, were asked to translate the translated Persian version of the questionnaire into English.
Step 4-Pre-testing and cognitive interviewing: By performing a pre-test, the clarity and transparency of the translated version were measured, and the incomprehensible phrases were identified and reviewed. The translated version of the scale became available to 10 people for inclusion in the study. These people were preferably those who were not in the main study. Then, respondents were asked about the items they had not understood and the ones they found unacceptable or offensive. This information was obtained through detailed personal interviews.
Step 5-Final version: The original versions of the Iranian and translated English versions were compared. The necessary changes were made to the Iranian version of the female orgasm scale (IV-FOS) wording, and it was finalized [16].
After explaining the study's objective, women who agreed to take part in the study filled in the FOS questionnaire.
Psychometric properties of the IV-FOS were assessed through reliability and validity tests. Further details are given below.
- Reliability: The stability or repeatability was examined by the test-retest method. Twenty eligible women completed the questionnaire twice at a two-week interval. The correlation between the scores obtained from the two surveys was determined by the intraclass correlation (ICC) index. ICC is the most acceptable index for testing stability. If this index is between 70- 80%, the stability level is desirable. For internal consistency, an appropriate time tool is suitable for reliability, with a Cronbach's alpha coefficient equal or greater than 0.7. Measurement error (Standard Error of Measurement) calculates the standard deviation of a patient's scores at different test times, which is obtained using the formula [17, 18].
[17, 18].
- Validity: content assessed face and construct validities of the IV-FOS questionnaire as follows:
1-Face validity: To determine the qualitative face validity, appropriate wording and writing style was used for the questionnaire. To this end, after performing the translation process, the questionnaire was presented to 15 eligible women, and a face-to-face interview was conducted to examine the questionnaire and announce the level of difficulty, the degree of irrelevancy, and ambiguity of the items [19].
2-Content validity: Two qualitative and quantitative methods were applied to assess content validity. In the qualitative phase, an expert panel consisting of 10 specialists, two sexologists, five reproductive health experts, two midwives, and one social medicine specialist assessed the content validity. All the experts were familiar with the principles of psychometric properties assessment. They assessed the grammar, wording, item allocation, and scaling of the questionnaire [20].
The content validity index (CVI) and the content validity ratio (CVR) were used to evaluate quantitative content validity. To determine the CVR, experts were asked to examine each item based on a 3-point Likert scale (i.e., "necessary", "useful but not necessary" and "not necessary"). Then the responses were calculated according to the CVI formula. If the calculated value was larger than the values in the Lawshe table, the content validity of that item was accepted [20-22]. To determine CVI, experts rated each questionnaire item in terms of relevancy, clarity, and simplicity. This was done in the form of a 4-point Likert scale below:
According to Masters and Johnson's model, the sexual response cycle consists of four stages, excitement, plateau, orgasm, and resolution [1]. The female orgasm is influenced by several factors and plays a crucial role in sexual compatibility and marital satisfaction [2]. In women, orgasm involves the myotonic response of the smooth and striated muscles, along with a sense of sexual stress relief emanating from the stimulation period. Orgasm is described as the most pleasurable sexual sensation [3]. During orgasm, 3 to 5 regular contractions occur in the vagina, perineum, and anal muscles, each of which lasts 0.8 seconds and reaches the uterus [4]. Clitoral tissue is the most sensitive part of anatomical sex for most women that stimulates the most powerful sexual feelings and orgasms [3]. Physiological and mental changes during orgasm are variable and differ among women proportionate to their conditions [5].
Persistent or recurrent delay in or absence of orgasm following a normal excitement phase is defined as Female orgasmic disorder (FOD) by the Diagnostic and Statistical Manual of Mental Disorders 4th Ed. (DSM-IV) [6]. Reduced intensity, delay, infrequency, or absence of orgasm for at least six months, which is not related to other physical, mental, or relational problems, is added by the DSM-V for more explanations of FOD [6].
Results of several studies suggest that the prevalence of orgasmic disorders among women is 18-61% in the general population [7]. Wolpe et al. reported that the prevalence of female sexual dysfunctions in Brazil was between 13.33 and 73.3%, and the orgasmic performance was 18.0-55.4% [8]. According to Zhang et al., the prevalence of sexual dysfunctions in women aged 20-70 in China was 29.7%, and orgasm was 27.9% [9]. According to a survey conducted by Ramezani et al., the prevalence of orgasmic disorders among women in the general population of Iran was 35.3% [10].
FOD is a multidimensional problem influenced by personal, relational, psychological, sociocultural, and religious context factors [11, 12]. Accurate FOD assessment requires applying a gender-based, culturally competent, valid, and reliable instrument [13]. The Female Orgasm Scale (FOS) is a gender-based, short, self-administered tool designed to assess female orgasm. The validity of the FOS questionnaire was assessed by Fisher et al. [14] in Canada for the first time. The study was conducted on three groups of women (n=651) aged 17–49 years. The main feature of the FOS is its assessment of orgasm during sex, including vaginal intercourse and clitoral stimulation. So, it seems that FOS is a culturally safe instrument for assessing orgasm among Iranian women.
Nevertheless, the cross-cultural adaptation of FOS in the Iranian population is necessary. Cross-cultural adaptation is defined as a process that includes language and cultural adaptation of a questionnaire for use in another setting and community [14]. The cultural adaptation process consists of three steps: translation, cross-cultural adaptation, and verification of the instrument's psychometric properties in the target population (i.e., standardization) [15].
There is no valid and reliable Persian version of FOS. Thus, this study aimed to translate and test the psychometric properties of the Iranian version of FOS –namely its cross-cultural adaptation- from English to Persian.
Instrument and Methods
This was a cross-sectional study carried out in Tehran, Iran, during September-December 2018. Two hundred thirty-five women attending three maternal health and family planning centers affiliated with Tehran and Beheshti Universities of Medical Sciences for routine care (excluding pregnancy) were chosen through convenience sampling. The inclusion criteria were aged 15 to 49 (reproductive age), married and sexually active, not pregnant, and willing to participate in the study. Thirty-five women did not agree to fill the IV-FOS; So, 200 women completed the questionnaire for construct validity assessment.
The FOS is a short, self-administered questionnaire developed by McIntyre-Smith & Fisher [14]. It assesses the consistency of female orgasm during partnered sexual activities (e.g., intercourse, oral stimulation, self-stimulation in the partner's presence) and overall satisfaction with orgasm frequency and quality. The scale is comprised of seven items. Five items inquire about the frequency of orgasm during different sexual activities: (a) intercourse, (b) intercourse with additional direct clitoral stimulation, (c) manual stimulation of the clitoris and/or genitals by a partner, (d) self-stimulation of the clitoris and/or genitals in the presence of a partner, and (e) oral stimulation. Two other items assess perceived satisfaction with the number and quality of orgasms experienced during sexual activity with a partner. This scale has two subscales: orgasm from clitoral stimulation and orgasmic satisfaction. In this scale, items 1-5 are scored as 0%=0, 10%=1, 20%=2 … 100%=10. Items 6-7 are scored as "Very Unsatisfied" = 1 to "Very Satisfied" = 7. Because items 1-5 are essentially coded on a 10-point scale, and the rest are coded on a 7-point scale, items should be weighted in the following manner: a) multiply items 1-5 by 7; b) Multiply items 6-7 by 10. Scoring the responses marked "Does not apply to me" can be coded as 0, depending on the researcher's rationale and use of the scale [15].
After obtaining a translation permit from the main author, the tool was translated into Persian. The concepts in the translated version were matched with the ones in the original version in the five following steps:
Step 1-Forward translation: The questionnaire was translated separately by two English translators who were native Persian speakers.
Step 2-Expert panel: At this stage, the integration of the two translated versions was done by the panel of experts. The two translators took part in a meeting, reviewed the translations, and reached a consensus after exchanging views, leading to an identical final version. At this stage, the goal was to check the terminology and rectify the deficiencies.
Step 3-Backward translation: The two translators (whose mother tongue was English) and had sufficient fluency in Persian, and had not yet received the English version of the questionnaire, were asked to translate the translated Persian version of the questionnaire into English.
Step 4-Pre-testing and cognitive interviewing: By performing a pre-test, the clarity and transparency of the translated version were measured, and the incomprehensible phrases were identified and reviewed. The translated version of the scale became available to 10 people for inclusion in the study. These people were preferably those who were not in the main study. Then, respondents were asked about the items they had not understood and the ones they found unacceptable or offensive. This information was obtained through detailed personal interviews.
Step 5-Final version: The original versions of the Iranian and translated English versions were compared. The necessary changes were made to the Iranian version of the female orgasm scale (IV-FOS) wording, and it was finalized [16].
After explaining the study's objective, women who agreed to take part in the study filled in the FOS questionnaire.
Psychometric properties of the IV-FOS were assessed through reliability and validity tests. Further details are given below.
- Reliability: The stability or repeatability was examined by the test-retest method. Twenty eligible women completed the questionnaire twice at a two-week interval. The correlation between the scores obtained from the two surveys was determined by the intraclass correlation (ICC) index. ICC is the most acceptable index for testing stability. If this index is between 70- 80%, the stability level is desirable. For internal consistency, an appropriate time tool is suitable for reliability, with a Cronbach's alpha coefficient equal or greater than 0.7. Measurement error (Standard Error of Measurement) calculates the standard deviation of a patient's scores at different test times, which is obtained using the formula
[17, 18].- Validity: content assessed face and construct validities of the IV-FOS questionnaire as follows:
1-Face validity: To determine the qualitative face validity, appropriate wording and writing style was used for the questionnaire. To this end, after performing the translation process, the questionnaire was presented to 15 eligible women, and a face-to-face interview was conducted to examine the questionnaire and announce the level of difficulty, the degree of irrelevancy, and ambiguity of the items [19].
2-Content validity: Two qualitative and quantitative methods were applied to assess content validity. In the qualitative phase, an expert panel consisting of 10 specialists, two sexologists, five reproductive health experts, two midwives, and one social medicine specialist assessed the content validity. All the experts were familiar with the principles of psychometric properties assessment. They assessed the grammar, wording, item allocation, and scaling of the questionnaire [20].
The content validity index (CVI) and the content validity ratio (CVR) were used to evaluate quantitative content validity. To determine the CVR, experts were asked to examine each item based on a 3-point Likert scale (i.e., "necessary", "useful but not necessary" and "not necessary"). Then the responses were calculated according to the CVI formula. If the calculated value was larger than the values in the Lawshe table, the content validity of that item was accepted [20-22]. To determine CVI, experts rated each questionnaire item in terms of relevancy, clarity, and simplicity. This was done in the form of a 4-point Likert scale below:
- Relevancy: 1=completely relevant, 2=relevant, 3=somewhat relevant, 4=not relevant;
- Clarity: 1=completely clear, 2=clear, 3=somewhat clear, 4=not clear; and
- Simplicity: 1=completely simple, 2=simple, 3=somewhat simple, 4=not simple.
3-Construct validity: Exploratory factor analysis (EFA) was performed to determine the underlying constructs of the questionnaire. Principal component analysis (PCA) with varimax rotation was applied. Before performing EFA, the suitability of the obtained data was investigated by Bartlett and Kaiser-Meyer-Olkin (KMO) tests. [23-26]. SPSS 22 was used.
Findings
The mean age of the participants was 31.35±7.13 years, with a range of 15-49 years. Most of the participants were housewives, and the majority were high school graduates (Table 1).
The mean score for female orgasm was 262.20, and the median score was 274. Reliability was evaluated using internal consistency. The Cronbach's alpha coefficient for the questionnaire was 0.7 for the whole scale, well above acceptable thresholds. The ICC was calculated and found to be 0.99. The mean, standard error was calculated at 0.7.
Following qualitative face and content validity, three items were corrected in the questionnaire. The result of quantitative content validity was a CVI of 0.84 and a CVR of 0.97 (Table 2).
Construct validity was evaluated by exploratory factor analysis (EFA). The Kaiser-Meyer-Olkin (KMO) and Bartlett's test indicated that the data were appropriate for factor analysis (KMO index=0.70, χ2=602.191, p=0.001). Principal component analysis with varimax rotation identified three factors with eigenvalues greater than one and factor loading equal to or greater than 0.4, accounting for 74.44% of the variance observed. The results obtained from EFA of the Iranian version of FOS showed in Table 3. The factors were loaded as follows:
I. Factor 1 (Vaginal and oral orgasm) including three
items: (items 1, 2, 5)
II. Factor 2 (Orgasmic satisfaction) including two items (items 6 & 7)
III. Factor 3 (Manual orgasm) including two items: (items 3 & 4)
Table 1) Demographic characteristics of the participants (n=200)
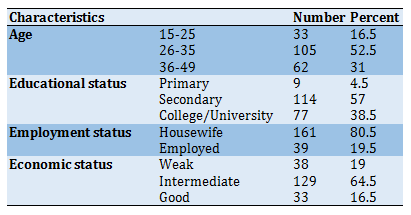
Table 2) CVI and CVR of the Iranian Version of Female Orgasm Scale (IV-FOS)

Table 3) The exploratory factor analysis (EFA) of the Iranian version of FOS (Rotated Component Matrix)

Findings
The mean age of the participants was 31.35±7.13 years, with a range of 15-49 years. Most of the participants were housewives, and the majority were high school graduates (Table 1).
The mean score for female orgasm was 262.20, and the median score was 274. Reliability was evaluated using internal consistency. The Cronbach's alpha coefficient for the questionnaire was 0.7 for the whole scale, well above acceptable thresholds. The ICC was calculated and found to be 0.99. The mean, standard error was calculated at 0.7.
Following qualitative face and content validity, three items were corrected in the questionnaire. The result of quantitative content validity was a CVI of 0.84 and a CVR of 0.97 (Table 2).
Construct validity was evaluated by exploratory factor analysis (EFA). The Kaiser-Meyer-Olkin (KMO) and Bartlett's test indicated that the data were appropriate for factor analysis (KMO index=0.70, χ2=602.191, p=0.001). Principal component analysis with varimax rotation identified three factors with eigenvalues greater than one and factor loading equal to or greater than 0.4, accounting for 74.44% of the variance observed. The results obtained from EFA of the Iranian version of FOS showed in Table 3. The factors were loaded as follows:
I. Factor 1 (Vaginal and oral orgasm) including three
items: (items 1, 2, 5)
II. Factor 2 (Orgasmic satisfaction) including two items (items 6 & 7)
III. Factor 3 (Manual orgasm) including two items: (items 3 & 4)
Table 1) Demographic characteristics of the participants (n=200)
Table 2) CVI and CVR of the Iranian Version of Female Orgasm Scale (IV-FOS)
Table 3) The exploratory factor analysis (EFA) of the Iranian version of FOS (Rotated Component Matrix)
Discussion
The present study reported the psychometric properties of the IV-FOS among a sample of Iranian women. Overall, the results indicated that the scale is a valid and reliable instrument for evaluating female orgasm. The Cronbach's alpha coefficient and intraclass correlation coefficient were acceptable and indicated good reliability and stability of the questionnaire. The CVI and CVR indicated reasonable content validity.
Although the original version of the FOS is unidimensional, the present study explored three dimensions of 'vaginal and oral orgasm', 'orgasmic satisfaction', and 'manual orgasm'. The following explanations may be presented to justify these findings. For instance, different sociocultural contexts may lead women to respond differently to orgasm questions. In fact, –like other sexuality issues- orgasm is affected by social, cultural, and religious variables and physical and psychological factors. The explored dimensions of the Persian version of the FOS showed that Iranian women perceived orgasm from two perspectives; the methods of orgasm achievement and orgasmic satisfaction.
The variance of the first dimension (vaginal and oral orgasm) was 44.94% of the total variance observed. In Iran, sex is generally accepted through marriage, which is highly influenced by religion and culture [27, 28]. Vaginal intercourse is the most acceptable form of sex for Iranian couples [29]. So, it was predictable that the most significant dimension of the IV-FOS would be related to vaginal orgasm. Additionally, the simultaneity of vaginal orgasm with oral orgasm in the first dimension can be justified by saying that the cunnilingus –defined as the spectrum of oral female genital stimulation by the partner- can play an important role in achieving female orgasm vaginally, orally, or from both routes. In other words, cunnilingus can be applied by the partner during foreplay to prepare a woman for vaginal intercourse by helping the woman achieve greater arousal and excitement. Under such circumstances, the probability of vaginal orgasm may increase. Cunnilingus can also be applied without vaginal intercourse, and orgasm can be experienced by the woman through high-quality oral stimulation of the genitals by the partner, especially the clitoris. We labeled this condition "oral orgasm" as part of the first dimension of the IV-FOS. Although there is no clear viewpoint in Islam confirming or rejecting oral sex [30], it can be a part of a sexual relationship experienced by some Iranian couples.
Orgasmic satisfaction is the second dimension of the Iranian version of FOS explored with EFA, with 15.98% observed variance. This dimension can be justified by Basson's model of female sexual response as recent evidence on women's sexology [30]. Based on her models, the focus on the frequency of female orgasm is far less than before, and physical, emotional, sexual, and relational satisfaction in a sexual relationship is emphasized [31]. Furthermore, orgasmic satisfaction is more important than the frequency of its achievement. In addition, the results of a study conducted to explore the variables affecting Iranian women's quality of sexual life indicate that orgasmic satisfaction is an important component when describing their sexual experiences [32].
Manual orgasm is the last dimension of the IV-FOS explored with EFA, with an observed variance of 13.51%. This dimension can assess clitoral orgasm, but based on the methods of genital stimulation which were described in the items of this dimension, we labeled it as 'manual orgasm'. Women can achieve orgasm through the clitoris and vagina. Clitoral orgasm is more common than vaginal orgasm [33]. So, it seems that a valid and reliable tool for the better study of female orgasm should contain a dimension for assessing clitoral/manual orgasm.
The validity of the FOS questionnaire was assessed by Fisher et al. [14] in Canada for the first time. The study was conducted on three groups of women (n=651) aged 17–49 years. The internal consistency of the FOS was good in all three studies (α=0.836-0.855). The corrected item-total correlation ranged from r=0.414-0.773. In addition, inter-item correlations ranged from r=0.187-0.606. Test-retest reliability was also excellent for the scale [14].
The results of the current study and Fisher et al.'s study [14] show that FOS is a questionnaire with appropriate cross-cultural adaptation properties. A comprehensible translation was achieved for use among Iranian women during this process, and satisfactory psychometric properties were found during the methodological process.
Although the present study sample included women of reproductive age, we suggest that similar research be conducted to increase the generalizability of the results. In addition, we recommend other psychometric properties such as convergent validity tests in future studies.
Conclusion
The present study's findings indicate that the Iranian version of FOS, which we labeled as the IV-FOS questionnaire, is a reliable and valid instrument. In other words, IV-FOS is a good questionnaire with a high degree of appropriateness toward Iranian sociocultural norms. Therefore, it can be applied to assess female orgasm in Iran's setting.
Acknowledgments: We would like to thank our colleagues in this institution sincerely. We are grateful to Alexandra McIntyre-Smith and William A. Fisher for giving their permission to translate and validate the Iranian version of the FOS questionnaire and Ali Akbar Rasekhi for assisting us in the statistical analysis.
Ethical Permissions: The ethical code was IR.MODARES.REC.1397.168.
Conflicts of Interests: The present study was part of a thesis for M.Sc. in Midwifery supported by the Faculty of Medical Sciences, Tarbiat Modares University, Iran. The authors declare no conflict of interest.
Authors' Contribution: Rahimi F. (First Author) Introduction author (35%); Lamyian M. (Second Author) Methodologist (30%); Masoumi R. (Third Author) Introduction author/Discussion author (35%).
Funding/Support: The financial support of this study has been provided by Tarbiat Modares University.
The present study reported the psychometric properties of the IV-FOS among a sample of Iranian women. Overall, the results indicated that the scale is a valid and reliable instrument for evaluating female orgasm. The Cronbach's alpha coefficient and intraclass correlation coefficient were acceptable and indicated good reliability and stability of the questionnaire. The CVI and CVR indicated reasonable content validity.
Although the original version of the FOS is unidimensional, the present study explored three dimensions of 'vaginal and oral orgasm', 'orgasmic satisfaction', and 'manual orgasm'. The following explanations may be presented to justify these findings. For instance, different sociocultural contexts may lead women to respond differently to orgasm questions. In fact, –like other sexuality issues- orgasm is affected by social, cultural, and religious variables and physical and psychological factors. The explored dimensions of the Persian version of the FOS showed that Iranian women perceived orgasm from two perspectives; the methods of orgasm achievement and orgasmic satisfaction.
The variance of the first dimension (vaginal and oral orgasm) was 44.94% of the total variance observed. In Iran, sex is generally accepted through marriage, which is highly influenced by religion and culture [27, 28]. Vaginal intercourse is the most acceptable form of sex for Iranian couples [29]. So, it was predictable that the most significant dimension of the IV-FOS would be related to vaginal orgasm. Additionally, the simultaneity of vaginal orgasm with oral orgasm in the first dimension can be justified by saying that the cunnilingus –defined as the spectrum of oral female genital stimulation by the partner- can play an important role in achieving female orgasm vaginally, orally, or from both routes. In other words, cunnilingus can be applied by the partner during foreplay to prepare a woman for vaginal intercourse by helping the woman achieve greater arousal and excitement. Under such circumstances, the probability of vaginal orgasm may increase. Cunnilingus can also be applied without vaginal intercourse, and orgasm can be experienced by the woman through high-quality oral stimulation of the genitals by the partner, especially the clitoris. We labeled this condition "oral orgasm" as part of the first dimension of the IV-FOS. Although there is no clear viewpoint in Islam confirming or rejecting oral sex [30], it can be a part of a sexual relationship experienced by some Iranian couples.
Orgasmic satisfaction is the second dimension of the Iranian version of FOS explored with EFA, with 15.98% observed variance. This dimension can be justified by Basson's model of female sexual response as recent evidence on women's sexology [30]. Based on her models, the focus on the frequency of female orgasm is far less than before, and physical, emotional, sexual, and relational satisfaction in a sexual relationship is emphasized [31]. Furthermore, orgasmic satisfaction is more important than the frequency of its achievement. In addition, the results of a study conducted to explore the variables affecting Iranian women's quality of sexual life indicate that orgasmic satisfaction is an important component when describing their sexual experiences [32].
Manual orgasm is the last dimension of the IV-FOS explored with EFA, with an observed variance of 13.51%. This dimension can assess clitoral orgasm, but based on the methods of genital stimulation which were described in the items of this dimension, we labeled it as 'manual orgasm'. Women can achieve orgasm through the clitoris and vagina. Clitoral orgasm is more common than vaginal orgasm [33]. So, it seems that a valid and reliable tool for the better study of female orgasm should contain a dimension for assessing clitoral/manual orgasm.
The validity of the FOS questionnaire was assessed by Fisher et al. [14] in Canada for the first time. The study was conducted on three groups of women (n=651) aged 17–49 years. The internal consistency of the FOS was good in all three studies (α=0.836-0.855). The corrected item-total correlation ranged from r=0.414-0.773. In addition, inter-item correlations ranged from r=0.187-0.606. Test-retest reliability was also excellent for the scale [14].
The results of the current study and Fisher et al.'s study [14] show that FOS is a questionnaire with appropriate cross-cultural adaptation properties. A comprehensible translation was achieved for use among Iranian women during this process, and satisfactory psychometric properties were found during the methodological process.
Although the present study sample included women of reproductive age, we suggest that similar research be conducted to increase the generalizability of the results. In addition, we recommend other psychometric properties such as convergent validity tests in future studies.
Conclusion
The present study's findings indicate that the Iranian version of FOS, which we labeled as the IV-FOS questionnaire, is a reliable and valid instrument. In other words, IV-FOS is a good questionnaire with a high degree of appropriateness toward Iranian sociocultural norms. Therefore, it can be applied to assess female orgasm in Iran's setting.
Acknowledgments: We would like to thank our colleagues in this institution sincerely. We are grateful to Alexandra McIntyre-Smith and William A. Fisher for giving their permission to translate and validate the Iranian version of the FOS questionnaire and Ali Akbar Rasekhi for assisting us in the statistical analysis.
Ethical Permissions: The ethical code was IR.MODARES.REC.1397.168.
Conflicts of Interests: The present study was part of a thesis for M.Sc. in Midwifery supported by the Faculty of Medical Sciences, Tarbiat Modares University, Iran. The authors declare no conflict of interest.
Authors' Contribution: Rahimi F. (First Author) Introduction author (35%); Lamyian M. (Second Author) Methodologist (30%); Masoumi R. (Third Author) Introduction author/Discussion author (35%).
Funding/Support: The financial support of this study has been provided by Tarbiat Modares University.
Article Type: Descriptive & Survey |
Subject:
Sexual Health Education/Promotion
Received: 2021/05/11 | Accepted: 2021/06/26 | Published: 2021/09/12
Received: 2021/05/11 | Accepted: 2021/06/26 | Published: 2021/09/12
References
1. Jabs F, Brotto LA. Identifying the disruptions in the sexual response cycles of women with Sexual Interest/Arousal Disorder. Can J Human Sex. 2018;27(2):123-32. [Link] [DOI:10.3138/cjhs.2018-0011]
2. Nekoolaltak M, Keshavarz Z, Simbar M, Nazari AM, Baghestani AR. Women's orgasm obstacles: A qualitative study. Int J Reprod Biomed. 2017;15(8):479-90. [Link] [DOI:10.29252/ijrm.15.8.479]
3. De Lucena B, Abdo C. Personal factors that contribute to or impair women's ability to achieve orgasm. Int J Impotence Res. 2014;26(5):177-81. [Link] [DOI:10.1038/ijir.2014.8] [PMID]
4. Nemati P, Nazariy AM. Orgasmic disorders subset of sexual dysfunction in women and improve it. J Saf Promot Inj Prev. 2014;1(4):228-35. [Persian] [Link]
5. Faubion SS, Rullo JE. Sexual dysfunction in women: A practical approach. Am Fam Physician. 2015;92(4):281-8. [Link]
6. Graham CA. The DSM diagnostic criteria for female orgasmic disorder. Arch Sex Behav. 2010;39(2):256-70.
https://doi.org/10.1007/s10508-009-9542-2 [Link] [DOI:10.1007/s10508-009-9535-1] [PMID]
7. Tavares IM, Laan ETM, Nobre PJ. Sexual inhibition is a vulnerability factor for orgasm problems in women. J Sex Med. 2018;15(3):361-72. [Link] [DOI:10.1016/j.jsxm.2017.12.015] [PMID]
8. Wolpe RE, Zomkowski K, Silva FP, Queiroz APA, Sperandio FF. Prevalence of female sexual dysfunction in Brazil: A systematic review. Eur J Obstet Gynecol Reprod Biol. 2017;211:26-32. [Link] [DOI:10.1016/j.ejogrb.2017.01.018] [PMID]
9. Zhang C, Tong J, Zhu L, Zhang L, Xu T, Lang J, et al. A population-based epidemiologic study of female sexual dysfunction risk in mainland China: Prevalence and predictors. J Sex Med. 2017;14(11):1348-56. [Link] [DOI:10.1016/j.jsxm.2017.08.012] [PMID]
10. Ramezani MA, Ahmadi K, Ghaemmaghami A, Marzabadi EA, Pardakhti F. Epidemiology of sexual dysfunction in Iran: A systematic review and meta-analysis. Int J Prev Med. 2015;6:43. [Link] [DOI:10.4103/2008-7802.157472] [PMID] [PMCID]
11. Maloney KM, Krakower DS, Ziobro D, Rosenberger JG, Novak D, Mayer KH. Culturally competent sexual healthcare as a prerequisite for obtaining preexposure prophylaxis: Findings from a qualitative study. LGBT Health. 2017;4(4):310-4. [Link] [DOI:10.1089/lgbt.2016.0068] [PMID] [PMCID]
12. Maasoumi R, Zarei F, Emami Razavi SH, Merghati Khoei E. How Iranian women with spinal cord injury understand sexuality. Trauma Mon. 2017;22(3):1-5. [Persian] [Link] [DOI:10.5812/traumamon.33116]
13. Arafat SY, Chowdhury HR, Qusar M, Hafez MA. Cross cultural adaption & psychometric validation of research instruments: A methodological review. J Behav Health. 2016;5(3):129-36. [Link] [DOI:10.5455/jbh.20160615121755]
14. Fisher TD, Davis CM, Yarber WL, Davis SL. Handbook of sexuality-related measures. Abingdon: Routledge; 2011. [Link]
15. Borsa JC, Damasio B, Bandeira DR. Cross-cultural adaptation and validation of psychological instruments: Some considerations. Paideia. 2012;22(53):423-32. [Link] [DOI:10.1590/S0103-863X2012000300014]
16. World Health Organization. Process of translation and adaptation of instruments [Internet]. Geneva: World Health Organization; 2019 [cited: unknown]. Available from: Not Found. [Link]
17. Mokhlesi S, Kariman N, Ebadi A, Khoshnejad F, Dabiri F. psychometric properties of the questionnaire for urinary incontinence diagnosis of married women of Qom city in 2015. J Rafsanjan Univ Med Sci. 2017;15(10):955-66. [Persian] [Link]
18. Zamani F, Talepasand S, Taghinezhad A. Psychometric properties of the phubbing scale among Iranian students. Health Educ Health Promot. 2020;8(1):25-30. [Persian] [Link]
19. Maasoumi R, Lamyian M, Montazeri A, Azin SA, Aguilar-Vafaie ME, Hajizadeh E. The sexual quality of life-female (SQOL-F) questionnaire: Translation and psychometric properties of the Iranian version. Reprod Health. 2013;10:25. [Link] [DOI:10.1186/1742-4755-10-25] [PMID] [PMCID]
20. Lawshe CH. A quantitative approach to content validity. Pers Psychol. 1975;28(4):563-70. [Link] [DOI:10.1111/j.1744-6570.1975.tb01393.x]
21. Maasoumi R, Mokarami H, Nazifi M, Stallones L, Taban A, Yazdani Aval M, et al. Psychometric properties of the persian translation of the sexual quality of life-male questionnaire. Am J Mens Health. 2017;11(3):564-72. [Link] [DOI:10.1177/1557988316629641] [PMID] [PMCID]
22. Solimani Zadeh L, Shokravi FA, Tavafian SS, Gholami Fesharaki M. Translation and psychometric evaluation of short-form decisional balance scale for smoking cessation among Iranian workers. Health Educ Health Promot. 2015;3(3):65-74. [Persian] [Link]
23. Ferguson E, Cox T. Exploratory factor analysis: A users' guide. International journal of selection and assessment. Int J Sel Assess. 1993;1(2):84-94. [Link] [DOI:10.1111/j.1468-2389.1993.tb00092.x]
24. Gholamnia Shirvani Z, Ghofranipour F, Gharakhanlou R, Kazemnejad A. Psychometric properties of the developed theory of planned behavior questionnaire about physical activity of military personnel's wives in Tehran. Health Educ Health Promot. 2014;2(3):31-43. [Persian] [Link]
25. Farahani AS, Rassouli M, Yaghmaie F, Majd HA, Sajjadi M. Psychometric Properties of the Persian Version of Self-Transcendence Scale: Adolescent Version. Int J Commun Nurs Midwifery. 2016;4(2):157-67. [Link]
26. Ghasemi E, Janani L, Dehghan Nayeri N, Negarandeh R. Psychometric Properties of Persian version of the competency inventory for registered nurse (CIRN). Iran J Nurs. 2014;27(87):1-13. [Persian] [Link] [DOI:10.29252/ijn.27.87.1]
27. Maasoumi R, Taket A, Zarei F. How Iranian women conceptualize the role of cultural norms in their sexual lives. Sex Cult. 2018;22(4):1376-90. [Link] [DOI:10.1007/s12119-018-9531-5]
28. Maasoumi R, Shivarani M, Lamb R, Zarei F. Exploring the role of religious teachings in Iranian women's sexual life scenarios. Sex Cult. 2020;24:197-208. [Link] [DOI:10.1007/s12119-019-09634-2]
29. Merghati ST, Samani RO. Islamic ideas about sexual relations. Reprod Biomed Online. 2008;17 Suppl 1:54. [Link] [DOI:10.1016/S1472-6483(10)60190-3]
30. Maasoumi R. Exploring the concept of female quality of sexual life, factors and dimensions: Development and psychometric properties of a cultural-based instrument [dissertation]. Tehran: Tarbiat Modares University; 2014. [Persian] [Link]
31. Ferenidou F, Kirana PS, Fokas K, Hatzichristou D, Athanasiadis L. Sexual Response Models: Toward a more flexible pattern of women's sexuality. J Sex Med. 2016;13(9):1369-76. [Link] [DOI:10.1016/j.jsxm.2016.07.008] [PMID]
32. Lamyian M, Zarei F, MontazeriA, Hajizadeh E, Maasoumi R. Exploring the factors affecting Iranian women's quality of sexual life. HAYAT. 2016;22(2):185-200. [Persian] [Link]
33. Rahimi F. Psychometric assessment of female orgasm scale and investigation of related factors [dissertation]. Tehran: Tarbiat Modares University; 2019. [Persian] [Link]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |