



Volume 9, Issue 3 (2021)
Health Educ Health Promot 2021, 9(3): 243-249 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Roozbahani S, Alamolhoda S, Rezaee Moradali M, Yahyavi Koochaksaraei F, Zareipour M, Tasouji Azari M. Determinants of Dairy Use Status and Effective Factors on Consumption Behaviors based on Health Belief Model. Health Educ Health Promot 2021; 9 (3) :243-249
URL: http://hehp.modares.ac.ir/article-5-50612-en.html
URL: http://hehp.modares.ac.ir/article-5-50612-en.html
S. Roozbahani1, S.H. Alamolhoda *2, M. Rezaee Moradali1, F. Yahyavi Koochaksaraei1, M.A. Zareipour3, M. Tasouji Azari4
1- "Student Research Committee" and "Department of Midwifery and Reproductive Health, School of Nursing and Midwifery", Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- "Midwifery and Reproductive Health Research Center" and "Department of Midwifery and Reproductive Health, School of Nursing and Midwifery", Shahid Beheshti University of Medical Sciences, Tehran, Iran , alamolhoda.h@gmail.com
3- Health System Research Unit, Health Center of Urmia, Urmia University of Medical Sciences, Urmia, Iran
4- Department of English Language, Tabriz Branch, Islamic Azad University, Tabriz, Iran
2- "Midwifery and Reproductive Health Research Center" and "Department of Midwifery and Reproductive Health, School of Nursing and Midwifery", Shahid Beheshti University of Medical Sciences, Tehran, Iran , alamolhoda.h@gmail.com
3- Health System Research Unit, Health Center of Urmia, Urmia University of Medical Sciences, Urmia, Iran
4- Department of English Language, Tabriz Branch, Islamic Azad University, Tabriz, Iran
Keywords: Health Belief Model [MeSH], Dairy Products [MeSH], Health Behavior [MeSH], Health Personnel [MeSH]
Full-Text [PDF 438 kb]
(951 Downloads)
| Abstract (HTML) (1485 Views)
Full-Text: (368 Views)
Introduction
Because of having biological compositions, dairy products are considered one of the most important components of human diet for all age groups and the foundation of maintenance and preservation of the health of the nutrition [1]. Milk and its products contain a great amount of calcium, phosphorus, and milk proteins such as Casein, Curd, and Bioactive Peptides [2]. In addition to their constitution composition, these productions contain water and fat-soluble vitamins, adequate amounts of Vitamins B1, B2, B6, B12, Biotin, and a small amount of Vitamin C [2]. According to different studies, health specialists introduce milk and its products as an exceptional food in providing necessary and vital elements of the body and nutritional needs of which the body is unable to produce alone [3]. Milk and dairy productions are helpful in prevention and reduction of the risk of cardiovascular diseases, weight-losing and consequently keeping the weight, type 2 diabetes, beneficial effects on mineral density in the bones, and some types of cancers (colon, bladder, breast, and gastric) [4].
Despite the very advantages of milk and dairy products, raw milk (its unpasteurized type), containing severe, dangerous microorganisms, is regarded as a great threat to human health [5]. Unpasteurized milk and dairy products are of main reasons for joint diseases of humans and animals like brucellosis [6]; according to the report of Centers for Disease Control and Prevention (CDC), there was a remarkable increase in the number of cases of illness and death relevant to unpasteurized milk and its products in 2007-2012 [7]. Providing proper and accurate nutrition is taken as the basic element of health [8]. According to the Health Ministry report, investigating the consumption status of milk and dairy products revealed that per capita consumption of milk in Iran was 35 liters every year, while it was 350 liters worldwide in 2020 [9]. The consumption and intake amount of dairy products are very low in Iran, as the rate of consumption is estimated to be only 10% for each Iranian family, which means 38 grams of a dairy product are used by each person daily [10]. There are many reasons proposed as the existing barriers in the promotion of healthy diet as well as milk and dairy products consumption, including availability and cultural acceptance of healthy food, disfavoring the flavor of milk and its products, intolerance of the lactose in milk, the high price of milk, being afraid of obesity and cardiovascular diseases because of the existing fat in dairy products [11]. The low amount of consumed milk and dairy products in Iran can result from socioeconomic status, cultural, social, geographic factors, personal characteristics, a small portion of subsidized milk, and the most important factor [12]. Therefore, it is necessary to consider the perceived barriers of healthy nutritional behaviors as a major step in effective food intervention to promote health [13]. Planned education, especially based on existing educational models, is one of the most basic prevention methods, treatment, and control of diseases [14]. Experts believe that the efficiency of behavior change programs and health education depends greatly on implementing health education theories and models. Therefore, selecting the appropriate health education model would be the first step of each health education program [15]. Health Belief Model (HBM) is one of the most useful frameworks for the perception of health behavior [16], which is based on the assumption that the health-related behavior depends on the combination of some factors, including the susceptibility to disease (perceived sensitivity), perceived severity, perceived advantages and barriers, cues to action, and self-efficiency [17]. This model has triggered successful results in different studies on the ground of changing nutritional behaviors, alike with health behaviors on large populations [18, 19]. Using the HBM on the behavior change of different classes of society in terms of milk and dairy consumption has been studied [20]. There have been a few studies regarding the behavior change in different scopes of health on the health care providers based on HBM, of which the majority had been conducted on the nurses to promote preventive behaviors from nosocomial infections [21], or on health liaisons in terms of investigating the effect of teaching health in different scopes [22] through using the HBM.
Since there has been no study done in the scope of dairy product behavior on health care providers according to the HBM, and since WHO has introduced health care providers as the most valuable human resources [23], paying attention to their health seems necessary to promote and preserve the health of the society. In this regard, the present study was done to investigate the determinants of the dairy consumption status and the factors influencing the consumption behaviors based on HBM among health care providers.
Instrument and Methods
The present cross-sectional descriptive-analytical study was conducted on all health care providers of health centers of Urmia, Iran, for two months (May 31-August 1) in 2020. By the census method, the required sample size was estimated to be 303 individuals. Inclusion criteria were included living in Urmia and using at least one dairy product. The exclusion criterion was withdrawal from participating in the research study.
The three-section researcher-made questionnaire (personal profile, the status of consumption of different types of dairy, and HBM [16]) was used to collect data through interviews. The questionnaire of investigation the dairy products consumption status contains three sections, each had six questions with answers including "always" using pasteurized and sterilized dairy all the time; "sometimes" using both types pasteurized/sterilized and local dairy; and "never" not using pasteurized and sterilized dairy at all. Furthermore, HBM includes six structures of perceived sensitivity, perceived severity, perceived benefits and barriers, cues to action, and self-efficiency, designed according to the 5-Likert scale, namely "completely agree" (5scores), "agree" (4 scores), "neither agree" "nor disagree" (3 scores), "disagree" (2 scores) and "completely disagree" (1 score), including each of the structures of "perceived sensitivity" (5 questions) with the score range of 5-25, "perceived severity" (5 questions) with the score range of 5-25, "perceived benefits" (6 questions) with the score range of 5-30, "cues to action" (5 questions) with the score range of 5-25, "perceived barriers" (5 questions) with the score range of 5-25. To meet the reliability of the questionnaires, formal and content methods were applied qualitatively and quantitatively. Thus, in the formal qualitative reliability, the questionnaires were available for at least ten health care providers to examine the proportionality of and relationship between the structures, any ambiguity, improper concept, and complexity of understanding, so any needed modifications were applied in the questionnaires as well. To investigate the formal reliability quantitatively, the impact score criterion was used, then by taking the score above 1.5, all constituting questions of the structures were accepted. The content reliability in a qualitative way was done using the expert panel opinion. In this way, the questionnaires were given to at least ten experts in the scope of health (nutrition and reproductive health) to evaluate the content and proportionality of the covering of the questions. Therein, the content reliability in a qualitative way was assessed through two criteria of content validity ratio (CVR) as 0.78 and content validity index (CVI) as 0.90. Moreover, the validity of all questions related to the structures of the model through Test-retest, using Cronbach's alpha coefficient, was assessed to be over 0.07.
Typical ethical considerations, including asking for permission from authorities of health centers of Urmia, explaining the objectives of the research to the participants of the study, obtaining informed written consent, and assuring the confidentiality of the data, were taken into account. The researcher referred to health centers and delivered questionnaires to health care providers to complete and collect them within two months.
The collected data through descriptive statistics (frequency index, percentage, mean, and standard deviation) and also inferential statistics (ANOVA test and Linear Regression) were analyzed by SPSS 24 at a significance level of p<0.05. The ANOVA Test-answers whether there was a meaningful, significant difference between different independent groups (health care providers with various demographic features like education, ethnicity, etc.) and multi-mode qualitative variables in dairy consumption behavior. Hence, a one-way analysis of variance was utilized in the present study. Linear regression is used to predict the value of a continuous variable (dairy consumption behavior) based on one or more input predictor variables (Health Belief Model Structures).
Findings
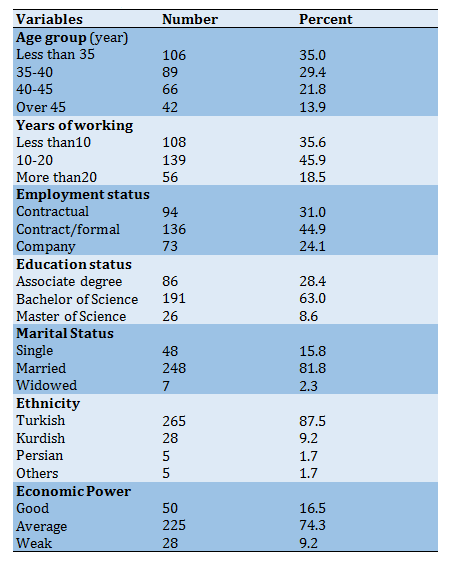
The mean±SD age was 38.57±6.36, while the smallest age group of the participants was more than 45 years old (13.9%). One hundred thirty-six participants (44.9%) had contract/formal employment status with an average working experience of 13.54 years. The majority of the participants (191 persons: 63%) were married, having a bachelor's degree (81.8%), and had Turkish ethnicity (87.5%). Regarding economic status, 225 persons (74.3%) were average (Table 1).
Table 1) Demographic characteristics (n=303)
The majority of the participants used both types of dairies, namely sterilized/pasteurized and local ones (Table 2).
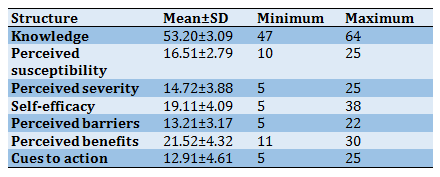
Mean±SD score of awareness of the dairy consumption behavior, as well as each s structure of (HBM), were computed and indicated that the highest and lowest scores were for the structures of perceived benefits (21.52±4.32) and cues to action (12.91±4.61) respectively (Table 3).
Table 2) Distribution of absolute and relative frequency of consumption status of each type of dairy products in terms of pasteurized/sterilized and local (traditional) in health care providers
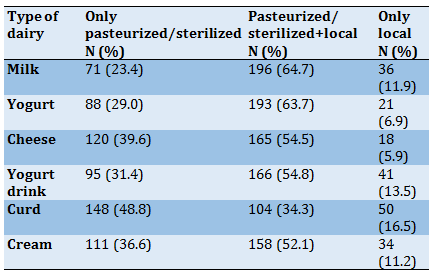
Table 3) Mean±SD of the acquired scores based on structures of (HBM) and awareness of the dairy consumption behavior (n=303)
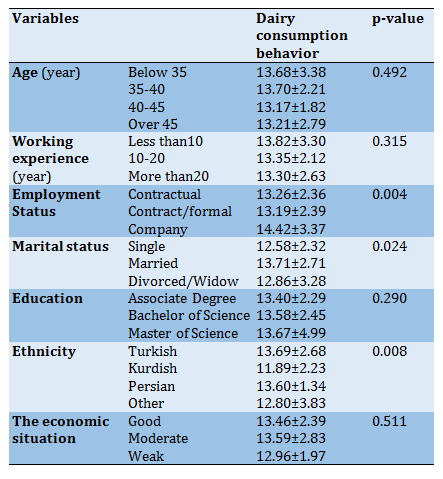
The results of the ANOVA test showed that the highest mean score of dairy production behavior allocated for the age group of 35-40 years old with the working experience of fewer than ten years, of which statistically, there was no significant difference among two variables being investigated (p=0.492, and p=0.315 respectively). Additionally, there was a statistically significant relationship between the mean score of the dairy consumption with the employment and marital status among health care providers (p=0.004, and p=0.024 respectively), of which the highest mean score of the dairy consumption behavior was for married company-employed staff working in health centers in Urmia. The findings revealed that health care providers with the Master's degree had the highest mean score of dairy consumption behavior compared with other ranks of education, although there was no significant statistical difference (p=0.290). Moreover, regarding ethnicity, there was a statistically significant relationship with the average mean score of dairy consumption behavior (p=0.008) which is the highest mean score of the dairy consumption behavior in health care providers with the ethnicity of Turkish. Additionally, the highest mean score of the dairy consumption behavior was ascribed for the health care providers with the average economic power, while there was no significant difference with other economic status groups (p=0.511; Table 4).
Table 4) Investigating the relationship between demographic data and the types of dairy consumption behavior of health care providers (Mean±SD)
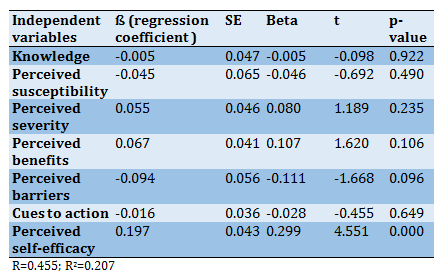
According to the HBM model, self-efficiency was recognized as the strongest significant structure (B=0.299, p=0.000) predicting the dairy consumption behavior among health care providers. The two structures of the perceived benefits (B=0.107) and perceived severity (B=0.080) had indicated a positive relationship in predicting the dairy consumption pattern despite not having any meaningful statistical relationship. However, the structures of perceived sensitivity (B=-0.046), perceived barriers (B=-0.111), and cues for action (B=-0.028) were not considered as predictive factors in the dairy consumption behavior of the population being studied. In general, the linear regression model results showed that the health belief model had 20% of the ability to predict dairy consumption behavior among health care providers. (Table 5).
Table 5) Results of the linear regression model in predicting dairy consumption behaviors based on (HBM) structures in health care providers
Discussion
In this study, the structures of the HBM as the influencing factors on choosing the type of dairy were identified. In this vein, the structure of self-efficiency showed a significant relationship with dairy consumption behavior in health care providers. The highest amount of dairy consumption related to milk is 64.7% in health care providers. This amount was 41% in the study done by Hosseini et al., [20] and 64% in Baghianimoghadam et al., among College Students [24]. Different factors influence the rate of dairy consumption, especially milk, including differences in education, income, cultural attitudes, consumption motivation, the cost of diaries, and their availability [25].
In this study, most health care providers consumed pasteurized/sterilized and local dairies like milk, yogurt, yogurt drink, cheese, and cream, while they always used pasteurized/sterilized curd. This can be ascribed to their perception of the advantages of pasteurized/sterilized curd compared to its local type due to its low risk of getting moldy, standardized quality monitoring, and control system. However, during a study in the chromatography method, the amount of fungal contamination of the examined types of curd in terms of aflatoxin (the toxic produced by the mold available in dairies) was revealed to be more in pasteurized/ industrial curd than its local type [26]. In the present study, there has been a significant statistical relationship between ethnicity and marital status with dairy consumption behavior, as the highest mean score of dairy consumption behavior was for married Turk health care providers. The majority of these people consumed all types of dairy, except curd, in either pasteurized/sterilized types, while they mostly used curd in its pasteurized/sterilized form. The study conducted by Esfarjani et al. stated that the most consumed type of milk among families in West Azerbaijan, Iran, has been in bulk (62.5%). This study was in line with the present study indicating a significant relationship in ethnicity and dairy consumption behavior (milk) regarding its pasteurized/sterilized and local type [27].
The study conducted by Buzby et al. proposed that the probability of unpasteurized milk consumption was high among men and women of Spanish descent having lower income and education [28]. The existence of various ethnicities, the local culture, and different perspectives would be effective in choosing the type of diaries consumed. In the present study, most married people consumed both types of pasteurized/sterilized and local milk. Accordingly, the study done by Fu et al. showed a significant relationship between the marital status and the consumption of both types of milk by married households. Throughout the study, married people spent more money buying both low-fat and whole milk [29]. It can be justified by referring to the more number of people and the variety in tastes of family members, the attitude and concern level of people, especially women, about the diet's health.
In the present study, there was a meaningful relationship between job situations and the behavior of dairy consumption, of which the highest mean score of dairy consumption was for the health care providers working as a company-employed staff. The majority of these people consumed all types of dairy products except curd and cheese in both pasteurized/sterilized and local types, while their using of cheese and curd had been mainly in their sterilized/pasteurized type. Being in line with the present study, a study in Turkey revealed a statistically significant relationship between the types of milk consumed with the employment status of the households. In this study, employed families had more tendency to consume qualified, packed dairy, especially milk, while unemployed families used milk in bulk [30]. It seems that the employment status of the families would be effective on the amount of family income, and consequently, on the type of dairy being used. In the present study, the highest mean score was for the structure of awareness (53.20±3.09), and then perceived benefits (21.52±4.32), and self-efficiency (19.11±4.09), also the lowest was for the cues to action (12.92±4.61) respectively. It can be claimed that the primary awareness of the health care providers of the differences between pasteurized/sterilized and local dairy products, their perception of the benefits of using pasteurized/sterilized dairy products compared to local ones, and assurance of the ability to change dairy consumption to the pasteurized/sterilized types are regarded as the influential variables on the causes of dairy use by health care providers.
Although the awareness on the behavior changing is necessary, it is not the only good factor. The study of Burr et al. stated that despite providing necessary information for pregnant women, there had not seen any significant improvement, especially on their nutritional behaviors [31]. However, some studies are in line with the present study results, indicating the growing increase of people's awareness of improving dairy consumption behaviors [32]. The study done by Ramzani et al. showed a significant increase in the mean score of the awareness following the educational intervention related to health lesions [33]. The current study was descriptive research, and people obtained the highest score in awareness despite not receiving any educational intervention. The difference in the findings may be best explained by the type of the studies (interventional vs. descriptive), the educational target age and gender group, and the difference in the education received. Furthermore, the participation of health care providers in health education courses held in health centers administered by the authorities can be another reason for their higher education and knowledge on the proposed issue.
The second structure effects on the consumption behavior of the participants of the current study were the perceived benefits together with six common items, ordered as the most important to the least, including prevention from the transmitted diseases by using pasteurized/sterilized dairy products, saving time, preserve and promote personal health, easier availability, reduction of treatment expenses, and pleasant taste. In the study conducted by Kholdi et al., the most important perceived benefit of dairy consumption for women was its physical benefits (healthy bones and teeth) and preserving their health in the future [34].
In the present study, the mean score of self-efficiency was at the average level (19.11±4.09), indicating a significant relationship with health care providers' dairy consumption behavior. In line with the present study, the significant relationship between self-efficiency and the score of dairy consumption behavior was highlighted in several studies. In the study of Ziaee et al., a significant relationship was noticed between self-efficiency structures and pregnant women's nutritional behavior [35]. The study of Morrovati et al. was between the scores of self-efficiency and nutritional behaviors of the elderly [36], as well as between the scores of self-efficiency and dairy consumption among students [20]. In the present study, the structure of self-efficiency was the strongest predictor of the pasteurized/sterilized dairy products consumption behavior among other structures of the HBM. In the same vein, in the study done by Karimi et al., self-efficiency, along with the perceived barriers and benefits, were identified as the most important predictors of the healthy behavior of pregnant women [37].
Ultimately, the structures of HBM have predicted 20.7% of the variance of the behaviors of dairy consumption among health care providers. The findings of the study done by Morvvati et al. could be able to predict the variance of the nutritional behaviors of the elderly in the similar amount of 20.2% [36], while in the study of Ayatollahi et al., it was determined as 62% based on the structures of the HBM [38].
Among the limitations of this study, it can be indicated to issues like employing researcher-made questionnaire to collect data, the cross-sectional nature of the study (the effect of the season on the dairy consumption behavior), and investigating the mere personal related factors (awareness, attitude, etc.) in adopting consumption behavior in HBM. Furthermore, the existence of cultural and financial differences and ethnic variation prevent overgeneralizing the findings of the present study to the entire population of the health care providers of the country.
The present study's findings indicated the growing need and efficiency of applying the HBM in adopting the consumption behaviors of health care providers. Thus, it is suggested that other educational health models of health promotion of the health staff consider inter-personal and social factors, in addition to personal factors, to improve the dairy consumption behavior of the health care providers.
Conclusion
Self-efficacy has the most predictive power of dairy consumption behavior in health care providers; Also, awareness was recognized as one of the influential variables on dairy consumption behavior in health care providers.
Acknowledgments: We would like to thank all the participants who helped us with this project.
Ethical Permissions: Ethical code of the present study was issued by the Ethics Committee in the research department of Urmia Azad University to the code of IR.IAU.URMIA.REC.1398.034.
Conflicts of Interests: The authors declare no conflict of interest.
Authors' Contribution: Roozbahani S. (First Author), Methodologist/Original Researcher/ Discussion Writer (45%); Alamolhoda S.H. (Second Author), Discussion Writer (15%); Rezaee Moradali M. (Third Author), Statistical Analyst/Discussion Writer (10%); Yahyavi Koochaksaraei F. (Forth Author), Introduction Writer (10%); Zareipour M.A. (Fifth Author), Statistical Analyst (10%); Tasouji Azari M. (Sixth Author), Introduction Writer (10%)
Funding/Support: This study has not received any financial support.
Because of having biological compositions, dairy products are considered one of the most important components of human diet for all age groups and the foundation of maintenance and preservation of the health of the nutrition [1]. Milk and its products contain a great amount of calcium, phosphorus, and milk proteins such as Casein, Curd, and Bioactive Peptides [2]. In addition to their constitution composition, these productions contain water and fat-soluble vitamins, adequate amounts of Vitamins B1, B2, B6, B12, Biotin, and a small amount of Vitamin C [2]. According to different studies, health specialists introduce milk and its products as an exceptional food in providing necessary and vital elements of the body and nutritional needs of which the body is unable to produce alone [3]. Milk and dairy productions are helpful in prevention and reduction of the risk of cardiovascular diseases, weight-losing and consequently keeping the weight, type 2 diabetes, beneficial effects on mineral density in the bones, and some types of cancers (colon, bladder, breast, and gastric) [4].
Despite the very advantages of milk and dairy products, raw milk (its unpasteurized type), containing severe, dangerous microorganisms, is regarded as a great threat to human health [5]. Unpasteurized milk and dairy products are of main reasons for joint diseases of humans and animals like brucellosis [6]; according to the report of Centers for Disease Control and Prevention (CDC), there was a remarkable increase in the number of cases of illness and death relevant to unpasteurized milk and its products in 2007-2012 [7]. Providing proper and accurate nutrition is taken as the basic element of health [8]. According to the Health Ministry report, investigating the consumption status of milk and dairy products revealed that per capita consumption of milk in Iran was 35 liters every year, while it was 350 liters worldwide in 2020 [9]. The consumption and intake amount of dairy products are very low in Iran, as the rate of consumption is estimated to be only 10% for each Iranian family, which means 38 grams of a dairy product are used by each person daily [10]. There are many reasons proposed as the existing barriers in the promotion of healthy diet as well as milk and dairy products consumption, including availability and cultural acceptance of healthy food, disfavoring the flavor of milk and its products, intolerance of the lactose in milk, the high price of milk, being afraid of obesity and cardiovascular diseases because of the existing fat in dairy products [11]. The low amount of consumed milk and dairy products in Iran can result from socioeconomic status, cultural, social, geographic factors, personal characteristics, a small portion of subsidized milk, and the most important factor [12]. Therefore, it is necessary to consider the perceived barriers of healthy nutritional behaviors as a major step in effective food intervention to promote health [13]. Planned education, especially based on existing educational models, is one of the most basic prevention methods, treatment, and control of diseases [14]. Experts believe that the efficiency of behavior change programs and health education depends greatly on implementing health education theories and models. Therefore, selecting the appropriate health education model would be the first step of each health education program [15]. Health Belief Model (HBM) is one of the most useful frameworks for the perception of health behavior [16], which is based on the assumption that the health-related behavior depends on the combination of some factors, including the susceptibility to disease (perceived sensitivity), perceived severity, perceived advantages and barriers, cues to action, and self-efficiency [17]. This model has triggered successful results in different studies on the ground of changing nutritional behaviors, alike with health behaviors on large populations [18, 19]. Using the HBM on the behavior change of different classes of society in terms of milk and dairy consumption has been studied [20]. There have been a few studies regarding the behavior change in different scopes of health on the health care providers based on HBM, of which the majority had been conducted on the nurses to promote preventive behaviors from nosocomial infections [21], or on health liaisons in terms of investigating the effect of teaching health in different scopes [22] through using the HBM.
Since there has been no study done in the scope of dairy product behavior on health care providers according to the HBM, and since WHO has introduced health care providers as the most valuable human resources [23], paying attention to their health seems necessary to promote and preserve the health of the society. In this regard, the present study was done to investigate the determinants of the dairy consumption status and the factors influencing the consumption behaviors based on HBM among health care providers.
Instrument and Methods
The present cross-sectional descriptive-analytical study was conducted on all health care providers of health centers of Urmia, Iran, for two months (May 31-August 1) in 2020. By the census method, the required sample size was estimated to be 303 individuals. Inclusion criteria were included living in Urmia and using at least one dairy product. The exclusion criterion was withdrawal from participating in the research study.
The three-section researcher-made questionnaire (personal profile, the status of consumption of different types of dairy, and HBM [16]) was used to collect data through interviews. The questionnaire of investigation the dairy products consumption status contains three sections, each had six questions with answers including "always" using pasteurized and sterilized dairy all the time; "sometimes" using both types pasteurized/sterilized and local dairy; and "never" not using pasteurized and sterilized dairy at all. Furthermore, HBM includes six structures of perceived sensitivity, perceived severity, perceived benefits and barriers, cues to action, and self-efficiency, designed according to the 5-Likert scale, namely "completely agree" (5scores), "agree" (4 scores), "neither agree" "nor disagree" (3 scores), "disagree" (2 scores) and "completely disagree" (1 score), including each of the structures of "perceived sensitivity" (5 questions) with the score range of 5-25, "perceived severity" (5 questions) with the score range of 5-25, "perceived benefits" (6 questions) with the score range of 5-30, "cues to action" (5 questions) with the score range of 5-25, "perceived barriers" (5 questions) with the score range of 5-25. To meet the reliability of the questionnaires, formal and content methods were applied qualitatively and quantitatively. Thus, in the formal qualitative reliability, the questionnaires were available for at least ten health care providers to examine the proportionality of and relationship between the structures, any ambiguity, improper concept, and complexity of understanding, so any needed modifications were applied in the questionnaires as well. To investigate the formal reliability quantitatively, the impact score criterion was used, then by taking the score above 1.5, all constituting questions of the structures were accepted. The content reliability in a qualitative way was done using the expert panel opinion. In this way, the questionnaires were given to at least ten experts in the scope of health (nutrition and reproductive health) to evaluate the content and proportionality of the covering of the questions. Therein, the content reliability in a qualitative way was assessed through two criteria of content validity ratio (CVR) as 0.78 and content validity index (CVI) as 0.90. Moreover, the validity of all questions related to the structures of the model through Test-retest, using Cronbach's alpha coefficient, was assessed to be over 0.07.
Typical ethical considerations, including asking for permission from authorities of health centers of Urmia, explaining the objectives of the research to the participants of the study, obtaining informed written consent, and assuring the confidentiality of the data, were taken into account. The researcher referred to health centers and delivered questionnaires to health care providers to complete and collect them within two months.
The collected data through descriptive statistics (frequency index, percentage, mean, and standard deviation) and also inferential statistics (ANOVA test and Linear Regression) were analyzed by SPSS 24 at a significance level of p<0.05. The ANOVA Test-answers whether there was a meaningful, significant difference between different independent groups (health care providers with various demographic features like education, ethnicity, etc.) and multi-mode qualitative variables in dairy consumption behavior. Hence, a one-way analysis of variance was utilized in the present study. Linear regression is used to predict the value of a continuous variable (dairy consumption behavior) based on one or more input predictor variables (Health Belief Model Structures).
Findings
The mean±SD age was 38.57±6.36, while the smallest age group of the participants was more than 45 years old (13.9%). One hundred thirty-six participants (44.9%) had contract/formal employment status with an average working experience of 13.54 years. The majority of the participants (191 persons: 63%) were married, having a bachelor's degree (81.8%), and had Turkish ethnicity (87.5%). Regarding economic status, 225 persons (74.3%) were average (Table 1).
Table 1) Demographic characteristics (n=303)
The majority of the participants used both types of dairies, namely sterilized/pasteurized and local ones (Table 2).
Mean±SD score of awareness of the dairy consumption behavior, as well as each s structure of (HBM), were computed and indicated that the highest and lowest scores were for the structures of perceived benefits (21.52±4.32) and cues to action (12.91±4.61) respectively (Table 3).
Table 2) Distribution of absolute and relative frequency of consumption status of each type of dairy products in terms of pasteurized/sterilized and local (traditional) in health care providers
Table 3) Mean±SD of the acquired scores based on structures of (HBM) and awareness of the dairy consumption behavior (n=303)
The results of the ANOVA test showed that the highest mean score of dairy production behavior allocated for the age group of 35-40 years old with the working experience of fewer than ten years, of which statistically, there was no significant difference among two variables being investigated (p=0.492, and p=0.315 respectively). Additionally, there was a statistically significant relationship between the mean score of the dairy consumption with the employment and marital status among health care providers (p=0.004, and p=0.024 respectively), of which the highest mean score of the dairy consumption behavior was for married company-employed staff working in health centers in Urmia. The findings revealed that health care providers with the Master's degree had the highest mean score of dairy consumption behavior compared with other ranks of education, although there was no significant statistical difference (p=0.290). Moreover, regarding ethnicity, there was a statistically significant relationship with the average mean score of dairy consumption behavior (p=0.008) which is the highest mean score of the dairy consumption behavior in health care providers with the ethnicity of Turkish. Additionally, the highest mean score of the dairy consumption behavior was ascribed for the health care providers with the average economic power, while there was no significant difference with other economic status groups (p=0.511; Table 4).
Table 4) Investigating the relationship between demographic data and the types of dairy consumption behavior of health care providers (Mean±SD)
According to the HBM model, self-efficiency was recognized as the strongest significant structure (B=0.299, p=0.000) predicting the dairy consumption behavior among health care providers. The two structures of the perceived benefits (B=0.107) and perceived severity (B=0.080) had indicated a positive relationship in predicting the dairy consumption pattern despite not having any meaningful statistical relationship. However, the structures of perceived sensitivity (B=-0.046), perceived barriers (B=-0.111), and cues for action (B=-0.028) were not considered as predictive factors in the dairy consumption behavior of the population being studied. In general, the linear regression model results showed that the health belief model had 20% of the ability to predict dairy consumption behavior among health care providers. (Table 5).
Table 5) Results of the linear regression model in predicting dairy consumption behaviors based on (HBM) structures in health care providers
Discussion
In this study, the structures of the HBM as the influencing factors on choosing the type of dairy were identified. In this vein, the structure of self-efficiency showed a significant relationship with dairy consumption behavior in health care providers. The highest amount of dairy consumption related to milk is 64.7% in health care providers. This amount was 41% in the study done by Hosseini et al., [20] and 64% in Baghianimoghadam et al., among College Students [24]. Different factors influence the rate of dairy consumption, especially milk, including differences in education, income, cultural attitudes, consumption motivation, the cost of diaries, and their availability [25].
In this study, most health care providers consumed pasteurized/sterilized and local dairies like milk, yogurt, yogurt drink, cheese, and cream, while they always used pasteurized/sterilized curd. This can be ascribed to their perception of the advantages of pasteurized/sterilized curd compared to its local type due to its low risk of getting moldy, standardized quality monitoring, and control system. However, during a study in the chromatography method, the amount of fungal contamination of the examined types of curd in terms of aflatoxin (the toxic produced by the mold available in dairies) was revealed to be more in pasteurized/ industrial curd than its local type [26]. In the present study, there has been a significant statistical relationship between ethnicity and marital status with dairy consumption behavior, as the highest mean score of dairy consumption behavior was for married Turk health care providers. The majority of these people consumed all types of dairy, except curd, in either pasteurized/sterilized types, while they mostly used curd in its pasteurized/sterilized form. The study conducted by Esfarjani et al. stated that the most consumed type of milk among families in West Azerbaijan, Iran, has been in bulk (62.5%). This study was in line with the present study indicating a significant relationship in ethnicity and dairy consumption behavior (milk) regarding its pasteurized/sterilized and local type [27].
The study conducted by Buzby et al. proposed that the probability of unpasteurized milk consumption was high among men and women of Spanish descent having lower income and education [28]. The existence of various ethnicities, the local culture, and different perspectives would be effective in choosing the type of diaries consumed. In the present study, most married people consumed both types of pasteurized/sterilized and local milk. Accordingly, the study done by Fu et al. showed a significant relationship between the marital status and the consumption of both types of milk by married households. Throughout the study, married people spent more money buying both low-fat and whole milk [29]. It can be justified by referring to the more number of people and the variety in tastes of family members, the attitude and concern level of people, especially women, about the diet's health.
In the present study, there was a meaningful relationship between job situations and the behavior of dairy consumption, of which the highest mean score of dairy consumption was for the health care providers working as a company-employed staff. The majority of these people consumed all types of dairy products except curd and cheese in both pasteurized/sterilized and local types, while their using of cheese and curd had been mainly in their sterilized/pasteurized type. Being in line with the present study, a study in Turkey revealed a statistically significant relationship between the types of milk consumed with the employment status of the households. In this study, employed families had more tendency to consume qualified, packed dairy, especially milk, while unemployed families used milk in bulk [30]. It seems that the employment status of the families would be effective on the amount of family income, and consequently, on the type of dairy being used. In the present study, the highest mean score was for the structure of awareness (53.20±3.09), and then perceived benefits (21.52±4.32), and self-efficiency (19.11±4.09), also the lowest was for the cues to action (12.92±4.61) respectively. It can be claimed that the primary awareness of the health care providers of the differences between pasteurized/sterilized and local dairy products, their perception of the benefits of using pasteurized/sterilized dairy products compared to local ones, and assurance of the ability to change dairy consumption to the pasteurized/sterilized types are regarded as the influential variables on the causes of dairy use by health care providers.
Although the awareness on the behavior changing is necessary, it is not the only good factor. The study of Burr et al. stated that despite providing necessary information for pregnant women, there had not seen any significant improvement, especially on their nutritional behaviors [31]. However, some studies are in line with the present study results, indicating the growing increase of people's awareness of improving dairy consumption behaviors [32]. The study done by Ramzani et al. showed a significant increase in the mean score of the awareness following the educational intervention related to health lesions [33]. The current study was descriptive research, and people obtained the highest score in awareness despite not receiving any educational intervention. The difference in the findings may be best explained by the type of the studies (interventional vs. descriptive), the educational target age and gender group, and the difference in the education received. Furthermore, the participation of health care providers in health education courses held in health centers administered by the authorities can be another reason for their higher education and knowledge on the proposed issue.
The second structure effects on the consumption behavior of the participants of the current study were the perceived benefits together with six common items, ordered as the most important to the least, including prevention from the transmitted diseases by using pasteurized/sterilized dairy products, saving time, preserve and promote personal health, easier availability, reduction of treatment expenses, and pleasant taste. In the study conducted by Kholdi et al., the most important perceived benefit of dairy consumption for women was its physical benefits (healthy bones and teeth) and preserving their health in the future [34].
In the present study, the mean score of self-efficiency was at the average level (19.11±4.09), indicating a significant relationship with health care providers' dairy consumption behavior. In line with the present study, the significant relationship between self-efficiency and the score of dairy consumption behavior was highlighted in several studies. In the study of Ziaee et al., a significant relationship was noticed between self-efficiency structures and pregnant women's nutritional behavior [35]. The study of Morrovati et al. was between the scores of self-efficiency and nutritional behaviors of the elderly [36], as well as between the scores of self-efficiency and dairy consumption among students [20]. In the present study, the structure of self-efficiency was the strongest predictor of the pasteurized/sterilized dairy products consumption behavior among other structures of the HBM. In the same vein, in the study done by Karimi et al., self-efficiency, along with the perceived barriers and benefits, were identified as the most important predictors of the healthy behavior of pregnant women [37].
Ultimately, the structures of HBM have predicted 20.7% of the variance of the behaviors of dairy consumption among health care providers. The findings of the study done by Morvvati et al. could be able to predict the variance of the nutritional behaviors of the elderly in the similar amount of 20.2% [36], while in the study of Ayatollahi et al., it was determined as 62% based on the structures of the HBM [38].
Among the limitations of this study, it can be indicated to issues like employing researcher-made questionnaire to collect data, the cross-sectional nature of the study (the effect of the season on the dairy consumption behavior), and investigating the mere personal related factors (awareness, attitude, etc.) in adopting consumption behavior in HBM. Furthermore, the existence of cultural and financial differences and ethnic variation prevent overgeneralizing the findings of the present study to the entire population of the health care providers of the country.
The present study's findings indicated the growing need and efficiency of applying the HBM in adopting the consumption behaviors of health care providers. Thus, it is suggested that other educational health models of health promotion of the health staff consider inter-personal and social factors, in addition to personal factors, to improve the dairy consumption behavior of the health care providers.
Conclusion
Self-efficacy has the most predictive power of dairy consumption behavior in health care providers; Also, awareness was recognized as one of the influential variables on dairy consumption behavior in health care providers.
Acknowledgments: We would like to thank all the participants who helped us with this project.
Ethical Permissions: Ethical code of the present study was issued by the Ethics Committee in the research department of Urmia Azad University to the code of IR.IAU.URMIA.REC.1398.034.
Conflicts of Interests: The authors declare no conflict of interest.
Authors' Contribution: Roozbahani S. (First Author), Methodologist/Original Researcher/ Discussion Writer (45%); Alamolhoda S.H. (Second Author), Discussion Writer (15%); Rezaee Moradali M. (Third Author), Statistical Analyst/Discussion Writer (10%); Yahyavi Koochaksaraei F. (Forth Author), Introduction Writer (10%); Zareipour M.A. (Fifth Author), Statistical Analyst (10%); Tasouji Azari M. (Sixth Author), Introduction Writer (10%)
Funding/Support: This study has not received any financial support.
Article Type: Descriptive & Survey |
Subject:
Health Education and Health Behavior
Received: 2021/05/2 | Accepted: 2021/06/26 | Published: 2021/09/12
Received: 2021/05/2 | Accepted: 2021/06/26 | Published: 2021/09/12
References
1. Pereira PC. Milk nutritional composition and its role in human health. Nutrition. 2014;30(6):619-27. [Link] [DOI:10.1016/j.nut.2013.10.011] [PMID]
2. Beck KL, Coad J. Dairy product (calcium) consumption and iron nutrition. Nutr Dairy Their Implic Health Dis. 2017 December:149-60. [Link] [DOI:10.1016/B978-0-12-809762-5.00012-7]
3. Koca T, Akcam M, Serdaroglu F, Dereci S. Breakfast habits, dairy product consumption, physical activity, and their associations with body mass index in children aged 6-18. Eur J Pediatr. 2017;176(9):1251-7. [Link] [DOI:10.1007/s00431-017-2976-y] [PMID]
4. Thorning TK, Raben A, Tholstrup T, Soedamah-Muthu SS, Givens I, Astrup A. Milk and dairy products: Good or bad for human health? an assessment of the totality of scientific evidence. Food Nutr Res. 2016;60:32527. [Link] [DOI:10.3402/fnr.v60.32527] [PMID] [PMCID]
5. Food and drug administration. The dangers of raw milk: Unpasteurized milk can pose a serious health risk [Internet]. Silver Spring: Food and Drug Administration; 2011 [cited 2021 Jul 9]. Available from: https://b2n.ir/z50653. [Link]
6. Karimyan K, Khezeli M, Latifi A. Effect of student's empowerment program on brucellosis prevention: An application of extended health belief model. J Prev Med Hyg. 2020;61(1):25-30. [Link]
7. Food safety. Outbreak studies [Internet]. Atlanta: Center for Disease Control and Preventation; 2020 [cited 2020 Oct 31]. Available from: https://www.cdc.gov/foodsafety/rawmilk/rawmilk-outbreaks.html. [Link]
8. Mahan LK, Raymond JL, Escott-Stump S. Krause's food and the nutrition care process-e-book. Amsterdam: Elsevier Health Sciences; 2013. [Link]
9. Gholami S, Rezaei Aliabadi H, Hashemi SY, Gholinia B, Shojapour A, Attarmadraki F, et al. The families' attitude and awareness toward consumption of milk and dairy products in Ardabil, Iran. Int J Nutr Sci. 2020;5(1):24-32. [Persian] [Link]
10. Pour-Abdolahi P, Hakeshzadeh F. Consumption frequency of milk and its products among female students of Tabriz university of medical sciences. J Res Health Sci. 2002;2(1):23-7. [Persian] [Link]
11. Mobley AR, Jensen JD, Maulding MK. Attitudes, beliefs, and barriers related to milk consumption in older, low-income women. J Nutr Educ Behav. 2014;46(6):554-9. [Link] [DOI:10.1016/j.jneb.2013.11.018] [PMID]
12. Rabieia S, Zahedia M, Abtahiab M, Doustmohammadiand A, Dadkhaha M, Zoghi T. Consumption of milk and dairy products in Iranian population; barriers and facilitators. Clin Nutr Open Sci. 2021;38:1-23. [Link] [DOI:10.1016/j.nutos.2021.05.002]
13. Lara J, Yong V, Mathers JC. Perceived barriers to healthy eating: A systematic review. Proc Nutr Soc.2016;75(3):152. [Link] [DOI:10.1017/S0029665116001671]
14. Jorvand R, Tavousi M, Ghofranipour F. Determinants of the regular physical activity among employees of healthcare network: Application of health belief model. J Educ Community Health. 2018;5(3):4-12. [Persian] [Link] [DOI:10.21859/jech.5.3.4]
15. Navabi SM, Khorsandi M, Roozbahani N, Ranjbaran M. Investigating the relationship between health belief model structures with the mothers' performance in preventing growth retardation in children aged 1-5 years in Shazand city, 2014. Arak Med Univ J. 2016;18(10):87-95. [Persian] [Link]
16. Naghashpour M, Shakerinejad G, Lourizadeh MR, Hajinajaf S, Jarvandi F. Nutrition education based on health belief model improves dietary calcium intake among female students of junior high schools. J Health Popul Nutr. 2014;32(3):420-9. [Link]
17. Lordo RF. The importance of interdisciplinarity: Redefining the health belief model [dissertation]. Columbia: University of South Carolina; 2018. [Link]
18. Diddana TZ, Kelkay GN, Dola AN, Sadore AA. Effect of nutrition education based on health belief model on nutritional knowledge and dietary practice of pregnant women in Dessie Town, northeast Ethiopia: A cluster randomized control trial. J Nutr Metab. 2018;2018:6731815. [Link] [DOI:10.1155/2018/6731815] [PMID] [PMCID]
19. Vahedian Shahroodi M, Tehrani H, Esmaily H, Olyani S. Effect of education intervention on nutrition behaviors of high school female students along with promoting health literacy. Health Educ Health Promot. 2019;7(4):169-76. [Persian] [Link]
20. Hosseini Z, Gharlipour Z, Mohebi S, Sharifirad G, Mohammadbeigi A, Kazazloo Z. Associated factors of milk consumption among students: using health belief model (HBM). Int J Pediatr. 2017;5(2):4439-48. [Persian] [Link]
21. Jeihooni AK, Kashfi SH, Bahmandost M, Afzali Harsini P. Promoting preventive behaviors of nosocomial infections in nurses: The effect of an educational program based on health belief model. Invest Educ Enferm. 2018;36(1):9. [Link] [DOI:10.17533/udea.iee.v36n1e09] [PMID]
22. Barzgar Mahmoodi T, Khorsandi M, Shamsi M, Ranjbaran M. Knowledge, beliefs and practice of health liaisons in Malayer regarding hepatitis B: Application of health belief model. Pajouhan Sci J. 2015;14(2):24-33. [Persian] [Link]
23. Joseph B, Joseph M. The health of the healthcare workers. Indian J Occup Environ Med. 2016;20(2):71-2. [Link] [DOI:10.4103/0019-5278.197518] [PMID] [PMCID]
24. Baghianimoghadam MH, Rahimi T, Khajedehi Z, Jowzi F, Daryafti H, Akbari Z, et al. Factors associated with milk consumption among college students of Yazd university of medical sciences based on theory of planned behavior. J Community Health Res. 2016;5(1):1-10. [Persian] [Link]
25. Kurajdova K, Taborecka-Petrovicova J, Kascakova A. Factors influencing milk consumption and purchase behavior-evidence from Slovakia. Proc Econ Finance. 2015;34:573-80. [Link] [DOI:10.1016/S2212-5671(15)01670-6]
26. Amirpour M, Amini M, Khademi Shurmasti D. Determination of aflatoxin M1 in pasteurized Kashk distributed in Tehran metropolitan. Iran J Health Environ. 2015;8(1):109-16. [Persian] [Link]
27. Esfarjani F, Mohammadi Nasr Abadi F, Khalafi M, Nouri-Saeidlou S, Rashidi A. Assessment of milk consumption and some of its related factors in households of western Azarbayjan province in 2012-13. Stud Med Sci. 2014;25(2):139-49. [Persian] [Link]
28. Buzby JC, Hannah Gould L, Kendall ME, Jones TF, Robinson T, Blayney DP. Characteristics of consumers of unpasteurized milk in the United States. J Consum Aff. 2013;47(1):153-66. [Link] [DOI:10.1111/joca.12001]
29. Fu S, Klepacka AM, Florkowski WJ. Household whole and low fat milk consumption in Poland: A bivariate two-part model. 2014 Annual Meeting, 1-4 February 2014, Dallas, United States. Kuala Lampur: IDEAS; 2014. [Link]
30. Yayar R, Economics A. Consumer characteristics influencing milk consumption preference: The Turkey case. Theor Appl Econ. 2012;7(572):25-52. [Link]
31. Burr ML, Trembeth J, Jones KB, Geen J, Lynch LA, Roberts ZES. The effects of dietary advice and vouchers on the intake of fruit and fruit juice by pregnant women in a deprived area: A controlled trial. Public Health Nutr. 2007;10(6):559-65. [Link] [DOI:10.1017/S1368980007249730] [PMID]
32. Maryam F, Chughtai A, Iqbal S, Tahir SK. Impact of nutrition education interventions on milk consumption among students (20-22 years). Life Sci J Pak. 2019;1(1):33-9. [Link]
33. Ramazani AA, Miri MR, Shayegan F. Effect of health education on health coordinating volunteers of Birjand health center to promote the community healthy life styles. J Birjand Univ Med Sci. 2007;14(4):27-33. [Persian] [Link]
34. Kholdi N, Piraste A, Khajavi Shojaie K, Shetkhani A, Zayeri F, Meskin A. Assessing the perceived barriers and benefits for milk products consumption in women living in Tehran. Iran J Health Educ Health Promot. 2018;6(1):29-38. [Persian] [Link] [DOI:10.30699/acadpub.ijhehp.6.1.29]
35. Ziaee R, Jalili Z, Tavakoli Ghouchani H. The effect of education based on Health Belief Model (HBM) in improving nutritional behaviors of pregnant women. J North Khorasan Univ Med Sci. 2016;8(3):427-37. [Persian] [Link] [DOI:10.18869/acadpub.jnkums.8.3.427]
36. Morowatisharifabad MA, Amani F, Kaseb F, Namayandeh SM. Predictors of healthy nutrition behaviors among elderlies of kalat county based on health belief model. Elder Health J. 2018;4(1):11-7. [Persian] [Link]
37. Karimy M, Taher M, Azarpira H. Measurement of health belief model construct in relation with nutritional practices of pregnant women in Saveh university of medical sciences. Avicenna J Nurs Midwifery. 2016;24(3):167-73. [Persian] [Link] [DOI:10.21859/nmj-24034]
38. Bayrami R, Didarlou A, Khalkhali H, Ayatollahi H, Ghorbani B. Relationship between health belief model and human papillomavirus vaccine intent among female students of Urmia university of medical sciences. Nurs Midwifery J. 2020;17(11):897-906. [Persian] [Link] [DOI:10.2174/1573404817999201228105419]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |