



Volume 9, Issue 4 (2021)
Health Educ Health Promot 2021, 9(4): 387-393 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Soleimaninejad A, Asadi Z, Fathi Manesh S, Moqaddas A. Correlation between Electronic Health Literacy and Health Promoting Behaviors in Elderly. Health Educ Health Promot 2021; 9 (4) :387-393
URL: http://hehp.modares.ac.ir/article-5-49623-en.html
URL: http://hehp.modares.ac.ir/article-5-49623-en.html
1- Department of Community Medicine, School of Medicine, Aja University of Medical Sciences, Tehran, Iran
2- Department of Community Medicine, School of Medicine, Aja University of Medical Sciences, Tehran, Iran , zasadi@ajaums.ac.ir
3- Department of Statistics, University of Kurdistan, Sanandaj, Department of Statistics, Faculty of Science, University of Kurdistan, Sanandaj, Iran
4- Department of Health Education and Promotion, School of Public Health, Bushehr University of Medical Sciences, Bushehr, Iran
2- Department of Community Medicine, School of Medicine, Aja University of Medical Sciences, Tehran, Iran , zasadi@ajaums.ac.ir
3- Department of Statistics, University of Kurdistan, Sanandaj, Department of Statistics, Faculty of Science, University of Kurdistan, Sanandaj, Iran
4- Department of Health Education and Promotion, School of Public Health, Bushehr University of Medical Sciences, Bushehr, Iran
Full-Text [PDF 512 kb]
(1077 Downloads)
| Abstract (HTML) (1375 Views)
Table 2) The Mean±SD of the score related to each question in the EHL questionnaire and components of health-promoting lifestyle
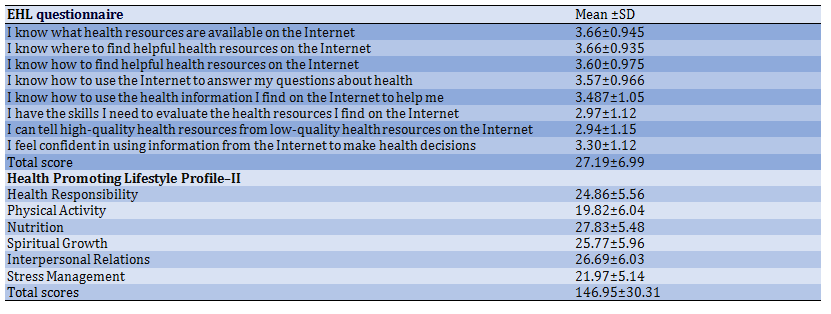
Table 3) The status of underlying variables on the component of the health-promoting lifestyle
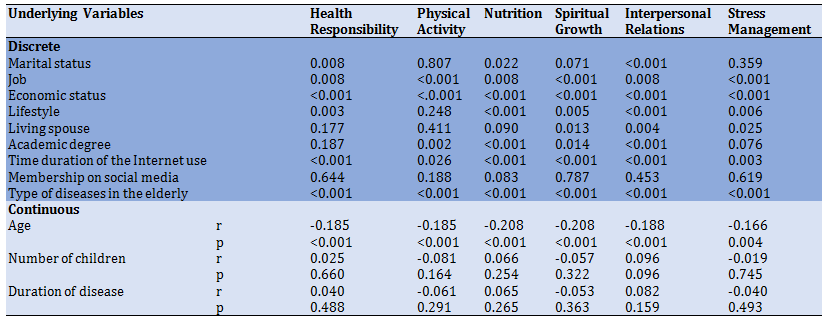
Table 4) Correlation coefficient between the components of HPL and EHL

Discussion
This study investigated the correlation between EHL and HPB among the elderly. Understanding the relationship between HPB and EHL and the related factors and identifying the predicting factors are considered significant issues for the decision-makers of health policy and health care.
The results of this study indicated that the mean score of HPB among the elderly is at a good level. Unlike the findings of Oh et al. [25], another study by Harooni et al. [26] was consistent with the present study. In this study, the elderly had a weak status respectively in physical activity, stress management, health responsibility, spiritual growth, interpersonal relationships, and nutrition, indicating the good behaviors of the elderly. Many studies indicated that the elderly were not appropriate regarding behaviors such as physical activity and having a good diet [27].
Regarding the reason for physical activity as the weakest component of HPB, it can be justified that many barriers affect the physical activity of the elderly. The most important tasks for solving such problems are creating motivation, making the environment appropriate, and presenting a special sports program for the elderly by the experts. It is worth noting that the weak status of spiritual growth among the elderly can create positive and constructive relationships and compatibility with situations [28].
The findings of the previous studies indicated that 76% of the elderly in America use the Internet for gaining health information [29]. Internet use is increasing among the elderly in Europe [30], while most Internet users in Iran are young people [31], not the elderly. On the other hand, the level of EHL among the elderly was low in the present study. Thus, it can be claimed that the lack of trust and ability among the elderly of Iran led to the low score of EHL. In addition, empowering the elderly to change health-related behaviors requires accurate information. Thus, educational interventions for acquiring accurate information from the Internet should be among the occupational priorities of healthcare experts because such measures can improve users’ trust in acquiring e-health information. The findings of this study indicated that the ability to recognize high-quality resources from low-quality ones, the ability to evaluate the resources, and their use for making decisions are among the most effective factors in the reduced privilege of EHL, which are consistent with the results of Park et al. [32]. In this regard, the authorities should increase the awareness of the elderly referred to Tehran retirement center by designing websites, educational programs, and Telegram channels to help them identify reliable sources. In addition, they should explain the information quality evaluation method to the elderly or their families.
However, the most significant findings of this study showed that the EHL level has a significant effect on the health-promoting lifestyle and its components. Since the components of a health-promoting lifestyle also have a high correlation and strongly affect each other, it’s reasonable to conclude that EHL affects some of the components directly and some others indirectly. It is rationales that EHL directly affects health responsibility, nutrition, and interpersonal relationships. In addition, these three variables indirectly affect the other components. Spiritual growth and physical activity can be improved by strengthening health responsibility. However, this study aimed to investigate the relationship between HPB and EHL of the elderly. The finding was consistent with the findings of other studies [13, 33]. Internet is considered the most preferred source of health information for promoting health behaviors. The studies on the relationship between HPB and EHL among the elderly are limited, and extensive should be performed to understand this relationship. The elderly with higher EHL indicated more appropriate health behaviors. The reasons for emphasizing this finding are increasing the use of e-health information by patients before the consultation with the medical tea, preventing the diseases, and regarding the self-care [34]. In addition, those who actively search for health care information often seek to find such information online by visiting websites based on health information [35]. In other words, the findings of this study indicated that higher EHL leads to more responsibility which can lead to more physical activity and improvement in health status. Further, EHL directly affects nutrition and interpersonal relationships, while the improved EHL can promote health responsibility among the elderly. Thus, all these factors promote healthy behaviors that can have a healthy lifestyle for the healthy elderly.
This study indicated that age has a significant relationship but had a weak correlation with health promotion behaviors, which is inconsistent with others' studies' findings [36], maybe because of the studied people in the same age range. In addition, other factors such as chronic diseases, lack of motivation, and illiteracy lead to the negligence of health behaviors. A significant relationship was found between marital status, health responsibility, nutrition, and interpersonal relationships of the studied units, so that married individuals had higher relationships related to the fact that the married elderly maintain a higher level of social relationships. In contrast, the single elderly become more isolated and have fewer daily activities such as health behaviors [37]. This finding was not consistent with the other findings [38]. Individuals with better health behaviors have more ability to have a job. Having a job can be regarded as the cause and effect of gaining health information from the Internet.
The significant relationship between HPB and economic status was another finding of this study, which was inconsistent with the study by Ohm [39] since economic areas can have a positive and negative effect on the status of health behaviors. Based on the other findings, lifestyle had a significant relationship with all other components of health behaviors except physical activity. The results of other studies were inconsistent with the present study [36-39]. The fact that the studied elderly had favorable interpersonal relationships can indicate the effect of loneliness on the motivation of the elderly in health behaviors.
In this study, a significant relationship was found between the studied units' academic level and physical activity [40, 41]. The finding was consistent with other studies because the low academic level is another significant barrier for communication and makes people have less access to health information sources such as the Internet. On the other hand, having high education can increase health and quality of life among the elderly. Despite the precision of the researchers, the high number of questions in the questionnaire, fatigue, and impatience of the elderly may affect their answers.
One of the limitations of this study was the lack of female participants as retirees. Also, the cross-sectional design of the present study was another limitation of this study in which cannot be considered as a gold standard design and the level of bias in cross-sectional studies are more. It is suggested to perform further studies with a larger sample size to be generalized. Identifying and evaluating the EHL of the elderly is the first necessary step in improving health behaviors. Finally, further studies are suggested to perform as cohort design with a large sample size.
Conclusion
There is a correlation between HPB and EHL among the elderly. In addition, EHL affects all the components of HPB positively so that by promoting EHL, all the components will promote. Thus, the improved EHL should be considered a necessary goal for promoting the healthy behaviors of these people because the obtained correlation was significantly positive.
Acknowledgments: The researchers would like to thank all the retirees.
Ethical Permissions: Ethical Permission code of the present study was (IR.AJAUMS.REC.1397.034).
Conflicts of Interests: None of the authors has a conflict of interest to be declared in this study.
Authors’ Contribution: Soleimaninejad A (First Author), Introduction Writer/Original Researcher/Discussion Writer (40%); Asadi ZS (Second Author), Original Researcher/Methodologist (25%); Fathi Manesh S (Third Author), Original Researcher/Statistical Analyst (25%); Moqaddas A (Fourth Author), Original Researcher (10%)
Funding/Support: The current study was supported by the Department of Community Medicine, Aja University of Medical Sciences.
Full-Text: (390 Views)
Introduction
As the body ages, older adults’ health and functioning decline, prone to developing chronic diseases [1]. However, the problem of elderly health promotion and their activation during old age is of special importance. Health-promoting behaviors (HPB) and quality of life in older people are highly significant [2]. In addition, reducing the level of physical activity, suffering from mental, living status, Education level and physical diseases, improper and inadequate care, low income, and other general demographic data probably guide the elderly toward reducing health behaviors [3]. However, it is difficult to design and implement relevant interventions because these socio-demographic characteristics are difficult to change. As a result, people have begun to look for those factors that can be changed, and health literacy has come into focus [4].
Health literacy refers to an individual’s ability to acquire, process, and understand basic health information and services and use them to make appropriate health decisions [5]. A systematic review showed that low health literacy is associated with poor health outcomes [6] and refers to the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to address or solve a health problem [7]. It should be noted the concept of Electronic Health Literacy (EHL) is derived from health literacy, and Previous studies found that the correlation between health literacy and EHL is moderate [8], and EHL is affected by a higher level of health literacy [9]. Therefore, health literacy and EHL need to be distinguished in research. Unlike health literacy, EHL emphasizes obtaining and using relevant health information through electronic media. In other words, individuals with low health literacy can still benefit from their health if they can use electronic media to search for and understand online health information. Given the rapid development of electronic communication technology, improving EHL may help improve the health status of older adults with low health literacy [10].
With the development of Internet information technology, much health information can be transmitted through the Internet. China’s statistical report on Internet development showed that Internet users among Chinese older adults are increasing, with the number of Internet users aged 50 and above rising from 7.3% [11] to 13.6% [12]. On the other hand, the results of other studies considered electronic literacy as one of the most influential factors in HPB [13]. Electronic behaviors such as the Internet lead to positive healthcare behaviors [14]. Further, acquiring e-health information can have the advantages of user empowerment, less anxiety, more sense of security, health management, and conscious health decisions [15]. EHL refers to people's ability to achieve, understand, and evaluate the basic information on web-based sources [16] and has some disadvantages such as complex information search, lack of judgment on the content regarding information accuracy, correctness, and instability [17]. However, there are some concerns about the reliability, accuracy, and quality of health-related information on the Internet [18].
In general, the systematic investigations indicated that using the Internet leads to positive effects on behaviors, including physical activities, smoking, nutrition, etc. [19]. Portnoy et al. showed that computer-delivered interventions improved behavioral health outcomes [19]. Also, in another study, computer-based interventions to increase EHL significantly improved health care outcomes in the participants [20].
Research on EHL and health outcomes is clearly in its early stages [21]. Thus, understanding the EHL of the elderly for health promotion and health behaviors is among the research priorities. The present study aimed to investigate the relationship and correlation between HPB and EHL among the elderly.
Instrument and Methods
This cross-sectional study was carried out on 300 subjects aged 60 years and older referred to Tehran retirement center in 2018. Centers with the more attending retirements were selected in Tehran. Convenient sampling was used for selecting the subjects. Considering 5% alpha and an average estimation error of 0.8 for e-literacy (mean: 27.19) and 3.5 for health promotion behaviors (mean: 146.95), 300 subjects were selected as sample size using the following formula:
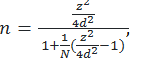 n is sample size, z=1.96, d=.05 is acceptable sample error and N=1400 is the population size. By putting this values in the formula, we can obtain n≃300 which is a conservative sample size for the research. Inclusion criteria were being retired, being familiar with the Internet, and having physical and mental health to answer the questions and the subjects who were not qualified were excluded from the study.
n is sample size, z=1.96, d=.05 is acceptable sample error and N=1400 is the population size. By putting this values in the formula, we can obtain n≃300 which is a conservative sample size for the research. Inclusion criteria were being retired, being familiar with the Internet, and having physical and mental health to answer the questions and the subjects who were not qualified were excluded from the study.
Three questionnaire were used as follow:
The demographic variables were age, marital status, employment status, Living status, lifestyle, spouse’s surviving status, educational level, time duration of using the internet, membership of social media, type of disease in elderly, number of children, and time duration of disease.
Health Promoting Lifestyle Profile-II Questionnaire (HPLP-II): This 52-item questionnaire was designed by Walker et al. for the frequency of health-promoting behaviors in six
dimensions, including health accountability, physical activity, nutrition, spiritual growth, stress management, and interpersonal relationships. The range of the total score for promoting behaviors was 52-208, and its classification was as weak (score: 52-91), moderate (score: 91-130), good (score: 130-169), and perfect (score: 169-208) [22]. Validity and reliability of HPLP-II were conducted by Taheri et al. among the Iranian elderly. Cronbach's alpha of the revised HPLP-II was 0.78, and their subscales were in the range of 0.67–0.84. Intraclass correlation coefficient was 0.79 (95% CI: 0.59–0.86, p<0.001) [23].
EHL Questionnaire: This questionnaire included eight items measuring the skill and self-confidence of subjects who use the Internet to collect data on health. The questions were the 5-point Likert, and their reliability and validity were confirmed by Norman & Skinner [7]. The final score of each answer varied from 8 to 40, and the higher scores indicated the higher EHL. Item analysis was performed on the 8-item scale at baseline, producing a tight-fitting scale with α=0.88. Item-scale correlations ranged from 0.51 to 0.76. Test-retest reliability showed suitable stability over time from baseline to 6-month follow-up (r=0.4 to 0.68) [7]. Also, the validity and reliability of this questionnaire were studied by Bazm et al. in Iran. The internal consistency of the scale was sufficient (α=0.88, p<0.001), and the test-retest coefficients for the items were reliable (r= 0.96, p<0.001) [24].
This study was approved by the AJA University of Medical Sciences. The objectives, details of the study, and confidentiality of results were explained to the elderly, and an informed consent letter was received from each subject. Participation in the study was completely voluntary. The lack of tendency to participate in the study did not deprive them of the routine services from the Tehran retirement center. The face-to-face interview was performed by trained researchers. On average, filling the required questionnaires took 25-35 minutes.
SPSS 19 was used to describe the variables, scores of the health-promoting lifestyle, the EHL, and their components as a mean and standard deviation to analyze the data. Pearson correlation test was used to assess the correlation between the two-questionnaire used. By independent t-test for marital status and living spouse variables and ANOVA methods for the other categorical demographic variables, the difference of demographic variables on the components of a health-promoting lifestyle has been considered.
Findings
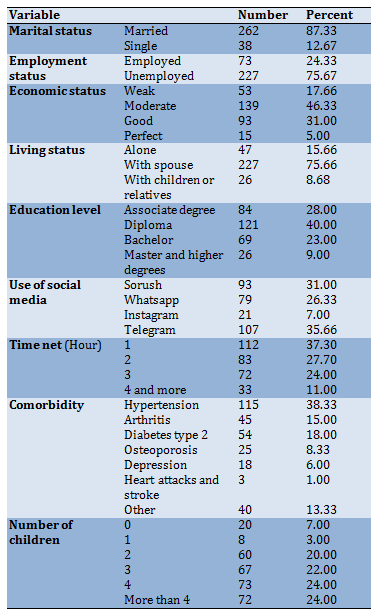
The mean age of the participants was 66.00±5.00 years (60-84 years). The mean time duration for suffering from diseases in individuals was 8.00±3.00 years (Table 1).
Table 1) Results of demographic characteristics of the participants (n=300)
The mean score of HPB and EHL was 146.95±30.31 and 27.19±6.99, respectively. Results of the mean scores showed in Table 2.
According to Table 3, marital status had no difference in physical activity, spiritual growth, and stress management scores. The occupation and economic status of the elderly had a significant difference in respect of all the components. Lifestyle as one of the variables, except physical activity, had a significant difference in respect of other components, which is the best mode of living with a spouse. The spouse’s living had no significant difference regarding HR, PA, and nutrition and had significant differences regarding other items. The academic level of the elderly had a significant difference across all factors except health responsibility and stress management. The duration of the use of the internet per hour a day significantly affected all latent variables. The type of social media was the only variable having no significant difference for any health-promoting lifestyles. Finally, the type of disease had a significant difference for all health-promoting lifestyle components. Depression had the worst possible status among all cases (Table 3). In continuous cases, there were three demographic variables; the number of children, duration of the disease, and age of the elderly. The Pearson correlation coefficients between these variables and all components in health-promoting lifestyle and their values have been computed. The correlation coefficient between the age of the elderly and the components is negative and small, so this variable weakly affected all the components (Table 3).
The Pearson correlation coefficient was used to survey the relationship between health-permeating lifestyle components and electronic health literacy components. According to the results, the correlation coefficients between the components of health-promoting lifestyle were high, which strongly affected each other. By increasing one of them, the others were increased. Most of them were approximately 0.4, which was a moderate positive relationship between electronic health literacy and all the components of the health-promoting lifestyle. This implies that more scores in electronic health literacy lead to more scores in a health-promoting lifestyle (Table 4).
As the body ages, older adults’ health and functioning decline, prone to developing chronic diseases [1]. However, the problem of elderly health promotion and their activation during old age is of special importance. Health-promoting behaviors (HPB) and quality of life in older people are highly significant [2]. In addition, reducing the level of physical activity, suffering from mental, living status, Education level and physical diseases, improper and inadequate care, low income, and other general demographic data probably guide the elderly toward reducing health behaviors [3]. However, it is difficult to design and implement relevant interventions because these socio-demographic characteristics are difficult to change. As a result, people have begun to look for those factors that can be changed, and health literacy has come into focus [4].
Health literacy refers to an individual’s ability to acquire, process, and understand basic health information and services and use them to make appropriate health decisions [5]. A systematic review showed that low health literacy is associated with poor health outcomes [6] and refers to the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to address or solve a health problem [7]. It should be noted the concept of Electronic Health Literacy (EHL) is derived from health literacy, and Previous studies found that the correlation between health literacy and EHL is moderate [8], and EHL is affected by a higher level of health literacy [9]. Therefore, health literacy and EHL need to be distinguished in research. Unlike health literacy, EHL emphasizes obtaining and using relevant health information through electronic media. In other words, individuals with low health literacy can still benefit from their health if they can use electronic media to search for and understand online health information. Given the rapid development of electronic communication technology, improving EHL may help improve the health status of older adults with low health literacy [10].
With the development of Internet information technology, much health information can be transmitted through the Internet. China’s statistical report on Internet development showed that Internet users among Chinese older adults are increasing, with the number of Internet users aged 50 and above rising from 7.3% [11] to 13.6% [12]. On the other hand, the results of other studies considered electronic literacy as one of the most influential factors in HPB [13]. Electronic behaviors such as the Internet lead to positive healthcare behaviors [14]. Further, acquiring e-health information can have the advantages of user empowerment, less anxiety, more sense of security, health management, and conscious health decisions [15]. EHL refers to people's ability to achieve, understand, and evaluate the basic information on web-based sources [16] and has some disadvantages such as complex information search, lack of judgment on the content regarding information accuracy, correctness, and instability [17]. However, there are some concerns about the reliability, accuracy, and quality of health-related information on the Internet [18].
In general, the systematic investigations indicated that using the Internet leads to positive effects on behaviors, including physical activities, smoking, nutrition, etc. [19]. Portnoy et al. showed that computer-delivered interventions improved behavioral health outcomes [19]. Also, in another study, computer-based interventions to increase EHL significantly improved health care outcomes in the participants [20].
Research on EHL and health outcomes is clearly in its early stages [21]. Thus, understanding the EHL of the elderly for health promotion and health behaviors is among the research priorities. The present study aimed to investigate the relationship and correlation between HPB and EHL among the elderly.
Instrument and Methods
This cross-sectional study was carried out on 300 subjects aged 60 years and older referred to Tehran retirement center in 2018. Centers with the more attending retirements were selected in Tehran. Convenient sampling was used for selecting the subjects. Considering 5% alpha and an average estimation error of 0.8 for e-literacy (mean: 27.19) and 3.5 for health promotion behaviors (mean: 146.95), 300 subjects were selected as sample size using the following formula:
n is sample size, z=1.96, d=.05 is acceptable sample error and N=1400 is the population size. By putting this values in the formula, we can obtain n≃300 which is a conservative sample size for the research. Inclusion criteria were being retired, being familiar with the Internet, and having physical and mental health to answer the questions and the subjects who were not qualified were excluded from the study. Three questionnaire were used as follow:
The demographic variables were age, marital status, employment status, Living status, lifestyle, spouse’s surviving status, educational level, time duration of using the internet, membership of social media, type of disease in elderly, number of children, and time duration of disease.
Health Promoting Lifestyle Profile-II Questionnaire (HPLP-II): This 52-item questionnaire was designed by Walker et al. for the frequency of health-promoting behaviors in six
dimensions, including health accountability, physical activity, nutrition, spiritual growth, stress management, and interpersonal relationships. The range of the total score for promoting behaviors was 52-208, and its classification was as weak (score: 52-91), moderate (score: 91-130), good (score: 130-169), and perfect (score: 169-208) [22]. Validity and reliability of HPLP-II were conducted by Taheri et al. among the Iranian elderly. Cronbach's alpha of the revised HPLP-II was 0.78, and their subscales were in the range of 0.67–0.84. Intraclass correlation coefficient was 0.79 (95% CI: 0.59–0.86, p<0.001) [23].
EHL Questionnaire: This questionnaire included eight items measuring the skill and self-confidence of subjects who use the Internet to collect data on health. The questions were the 5-point Likert, and their reliability and validity were confirmed by Norman & Skinner [7]. The final score of each answer varied from 8 to 40, and the higher scores indicated the higher EHL. Item analysis was performed on the 8-item scale at baseline, producing a tight-fitting scale with α=0.88. Item-scale correlations ranged from 0.51 to 0.76. Test-retest reliability showed suitable stability over time from baseline to 6-month follow-up (r=0.4 to 0.68) [7]. Also, the validity and reliability of this questionnaire were studied by Bazm et al. in Iran. The internal consistency of the scale was sufficient (α=0.88, p<0.001), and the test-retest coefficients for the items were reliable (r= 0.96, p<0.001) [24].
This study was approved by the AJA University of Medical Sciences. The objectives, details of the study, and confidentiality of results were explained to the elderly, and an informed consent letter was received from each subject. Participation in the study was completely voluntary. The lack of tendency to participate in the study did not deprive them of the routine services from the Tehran retirement center. The face-to-face interview was performed by trained researchers. On average, filling the required questionnaires took 25-35 minutes.
SPSS 19 was used to describe the variables, scores of the health-promoting lifestyle, the EHL, and their components as a mean and standard deviation to analyze the data. Pearson correlation test was used to assess the correlation between the two-questionnaire used. By independent t-test for marital status and living spouse variables and ANOVA methods for the other categorical demographic variables, the difference of demographic variables on the components of a health-promoting lifestyle has been considered.
Findings
The mean age of the participants was 66.00±5.00 years (60-84 years). The mean time duration for suffering from diseases in individuals was 8.00±3.00 years (Table 1).
Table 1) Results of demographic characteristics of the participants (n=300)
The mean score of HPB and EHL was 146.95±30.31 and 27.19±6.99, respectively. Results of the mean scores showed in Table 2.
According to Table 3, marital status had no difference in physical activity, spiritual growth, and stress management scores. The occupation and economic status of the elderly had a significant difference in respect of all the components. Lifestyle as one of the variables, except physical activity, had a significant difference in respect of other components, which is the best mode of living with a spouse. The spouse’s living had no significant difference regarding HR, PA, and nutrition and had significant differences regarding other items. The academic level of the elderly had a significant difference across all factors except health responsibility and stress management. The duration of the use of the internet per hour a day significantly affected all latent variables. The type of social media was the only variable having no significant difference for any health-promoting lifestyles. Finally, the type of disease had a significant difference for all health-promoting lifestyle components. Depression had the worst possible status among all cases (Table 3). In continuous cases, there were three demographic variables; the number of children, duration of the disease, and age of the elderly. The Pearson correlation coefficients between these variables and all components in health-promoting lifestyle and their values have been computed. The correlation coefficient between the age of the elderly and the components is negative and small, so this variable weakly affected all the components (Table 3).
The Pearson correlation coefficient was used to survey the relationship between health-permeating lifestyle components and electronic health literacy components. According to the results, the correlation coefficients between the components of health-promoting lifestyle were high, which strongly affected each other. By increasing one of them, the others were increased. Most of them were approximately 0.4, which was a moderate positive relationship between electronic health literacy and all the components of the health-promoting lifestyle. This implies that more scores in electronic health literacy lead to more scores in a health-promoting lifestyle (Table 4).
Table 2) The Mean±SD of the score related to each question in the EHL questionnaire and components of health-promoting lifestyle
Table 3) The status of underlying variables on the component of the health-promoting lifestyle
Table 4) Correlation coefficient between the components of HPL and EHL
Discussion
This study investigated the correlation between EHL and HPB among the elderly. Understanding the relationship between HPB and EHL and the related factors and identifying the predicting factors are considered significant issues for the decision-makers of health policy and health care.
The results of this study indicated that the mean score of HPB among the elderly is at a good level. Unlike the findings of Oh et al. [25], another study by Harooni et al. [26] was consistent with the present study. In this study, the elderly had a weak status respectively in physical activity, stress management, health responsibility, spiritual growth, interpersonal relationships, and nutrition, indicating the good behaviors of the elderly. Many studies indicated that the elderly were not appropriate regarding behaviors such as physical activity and having a good diet [27].
Regarding the reason for physical activity as the weakest component of HPB, it can be justified that many barriers affect the physical activity of the elderly. The most important tasks for solving such problems are creating motivation, making the environment appropriate, and presenting a special sports program for the elderly by the experts. It is worth noting that the weak status of spiritual growth among the elderly can create positive and constructive relationships and compatibility with situations [28].
The findings of the previous studies indicated that 76% of the elderly in America use the Internet for gaining health information [29]. Internet use is increasing among the elderly in Europe [30], while most Internet users in Iran are young people [31], not the elderly. On the other hand, the level of EHL among the elderly was low in the present study. Thus, it can be claimed that the lack of trust and ability among the elderly of Iran led to the low score of EHL. In addition, empowering the elderly to change health-related behaviors requires accurate information. Thus, educational interventions for acquiring accurate information from the Internet should be among the occupational priorities of healthcare experts because such measures can improve users’ trust in acquiring e-health information. The findings of this study indicated that the ability to recognize high-quality resources from low-quality ones, the ability to evaluate the resources, and their use for making decisions are among the most effective factors in the reduced privilege of EHL, which are consistent with the results of Park et al. [32]. In this regard, the authorities should increase the awareness of the elderly referred to Tehran retirement center by designing websites, educational programs, and Telegram channels to help them identify reliable sources. In addition, they should explain the information quality evaluation method to the elderly or their families.
However, the most significant findings of this study showed that the EHL level has a significant effect on the health-promoting lifestyle and its components. Since the components of a health-promoting lifestyle also have a high correlation and strongly affect each other, it’s reasonable to conclude that EHL affects some of the components directly and some others indirectly. It is rationales that EHL directly affects health responsibility, nutrition, and interpersonal relationships. In addition, these three variables indirectly affect the other components. Spiritual growth and physical activity can be improved by strengthening health responsibility. However, this study aimed to investigate the relationship between HPB and EHL of the elderly. The finding was consistent with the findings of other studies [13, 33]. Internet is considered the most preferred source of health information for promoting health behaviors. The studies on the relationship between HPB and EHL among the elderly are limited, and extensive should be performed to understand this relationship. The elderly with higher EHL indicated more appropriate health behaviors. The reasons for emphasizing this finding are increasing the use of e-health information by patients before the consultation with the medical tea, preventing the diseases, and regarding the self-care [34]. In addition, those who actively search for health care information often seek to find such information online by visiting websites based on health information [35]. In other words, the findings of this study indicated that higher EHL leads to more responsibility which can lead to more physical activity and improvement in health status. Further, EHL directly affects nutrition and interpersonal relationships, while the improved EHL can promote health responsibility among the elderly. Thus, all these factors promote healthy behaviors that can have a healthy lifestyle for the healthy elderly.
This study indicated that age has a significant relationship but had a weak correlation with health promotion behaviors, which is inconsistent with others' studies' findings [36], maybe because of the studied people in the same age range. In addition, other factors such as chronic diseases, lack of motivation, and illiteracy lead to the negligence of health behaviors. A significant relationship was found between marital status, health responsibility, nutrition, and interpersonal relationships of the studied units, so that married individuals had higher relationships related to the fact that the married elderly maintain a higher level of social relationships. In contrast, the single elderly become more isolated and have fewer daily activities such as health behaviors [37]. This finding was not consistent with the other findings [38]. Individuals with better health behaviors have more ability to have a job. Having a job can be regarded as the cause and effect of gaining health information from the Internet.
The significant relationship between HPB and economic status was another finding of this study, which was inconsistent with the study by Ohm [39] since economic areas can have a positive and negative effect on the status of health behaviors. Based on the other findings, lifestyle had a significant relationship with all other components of health behaviors except physical activity. The results of other studies were inconsistent with the present study [36-39]. The fact that the studied elderly had favorable interpersonal relationships can indicate the effect of loneliness on the motivation of the elderly in health behaviors.
In this study, a significant relationship was found between the studied units' academic level and physical activity [40, 41]. The finding was consistent with other studies because the low academic level is another significant barrier for communication and makes people have less access to health information sources such as the Internet. On the other hand, having high education can increase health and quality of life among the elderly. Despite the precision of the researchers, the high number of questions in the questionnaire, fatigue, and impatience of the elderly may affect their answers.
One of the limitations of this study was the lack of female participants as retirees. Also, the cross-sectional design of the present study was another limitation of this study in which cannot be considered as a gold standard design and the level of bias in cross-sectional studies are more. It is suggested to perform further studies with a larger sample size to be generalized. Identifying and evaluating the EHL of the elderly is the first necessary step in improving health behaviors. Finally, further studies are suggested to perform as cohort design with a large sample size.
Conclusion
There is a correlation between HPB and EHL among the elderly. In addition, EHL affects all the components of HPB positively so that by promoting EHL, all the components will promote. Thus, the improved EHL should be considered a necessary goal for promoting the healthy behaviors of these people because the obtained correlation was significantly positive.
Acknowledgments: The researchers would like to thank all the retirees.
Ethical Permissions: Ethical Permission code of the present study was (IR.AJAUMS.REC.1397.034).
Conflicts of Interests: None of the authors has a conflict of interest to be declared in this study.
Authors’ Contribution: Soleimaninejad A (First Author), Introduction Writer/Original Researcher/Discussion Writer (40%); Asadi ZS (Second Author), Original Researcher/Methodologist (25%); Fathi Manesh S (Third Author), Original Researcher/Statistical Analyst (25%); Moqaddas A (Fourth Author), Original Researcher (10%)
Funding/Support: The current study was supported by the Department of Community Medicine, Aja University of Medical Sciences.
Article Type: Descriptive & Survey |
Subject:
Health Education and Health Behavior
Received: 2021/02/7 | Accepted: 2021/05/24 | Published: 2021/11/12
Received: 2021/02/7 | Accepted: 2021/05/24 | Published: 2021/11/12
References
1. Ferris R, Blaum C, Kiwak E, Austin J, Esterson J, Harkless G, et al. Perspectives of patients, clinicians, and health system leaders on changes needed to improve the health care and outcomes of older adults with multiple chronic conditions. J Aging Health. 2018;30(5):778-99. [Link] [DOI:10.1177/0898264317691166] [PMID]
2. Govindaraju T, Sahle BW, McCaffrey TA, McNeil JJ, Owen AJ. Dietary patterns and quality of life in older adults: A systematic review. Nutrients. 2018;10(8):971. [Link] [DOI:10.3390/nu10080971] [PMID] [PMCID]
3. Buyl R, Beogo I, Fobelets M, Deletroz C, Van Landuyt P, Dequanter S, et al. E-health interventions for healthy aging: A systematic review. Syst Rev. 2020;9(1):128. [Link] [DOI:10.1186/s13643-020-01385-8] [PMID] [PMCID]
4. Nutbeam D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15(3):259-67.
https://doi.org/10.1093/heapro/15.3.183 [Link] [DOI:10.1093/heapro/15.3.259]
5. Berkman ND, Davis TC, McCormack L. Health literacy: What is it. J Health Commun. 2010;15(2):9-19. [Link] [DOI:10.1080/10810730.2010.499985] [PMID]
6. Chesser AK, Keene Woods N, Smothers K, Rogers N. Health literacy and older adults: A systematic review. Gerontol Geriatr Med. 2016;2:2333721416630492. [Link] [DOI:10.1177/2333721416630492] [PMID] [PMCID]
7. Norman CD, Skinner HA. Eheals: The eHealth literacy scale. J Med Internet Res. 2006;8(4):27. [Link] [DOI:10.2196/jmir.8.4.e27] [PMID] [PMCID]
8. Neter E, Brainin E, Baron-Epel O. The dimensionality of health literacy and ehealth literacy. Eur Health Psychol. 2015;17(6):275-80. [Link]
9. Del Giudice P, Bravo G, Poletto M, De Odorico A, Conte A, Brunelli L, et al. Correlation between health literacy and health literacy using the eHealth literacy scale and real-life experiences in the health sector as a proxy measure of functional health literacy: Cross-sectional web-based survey. J Med Internet Res. 2018;20(10):281. [Link] [DOI:10.2196/jmir.9401] [PMID] [PMCID]
10. Li S, Cui G, Yin Y, Wang S, Liu X, Chen L. Health-promoting behaviors mediate the relationship between eHealth literacy and health-related quality of life among Chinese older adults: A cross-sectional study. Qual Life Res. 2021;30(8):2235-43. [Link] [DOI:10.1007/s11136-021-02797-2] [PMID] [PMCID]
11. China Internet Network Information Center. Statistical report on internet development in China (July 2014): the 34th survey report on internet development in China. China Internet Network Information Center; 2014. [Link]
12. China Internet Network Information Center. Statistical report on internet development in China (August 2019): The 44th statistical report on internet development in China . China Internet Network Information Center; 2019. [Link]
13. Kim SH, Son YJ. Relationships between eHealth literacy and health behaviors in Korean adults. CIN Comput Inform Nurs. 2017;35(2):84-90. [Link] [DOI:10.1097/CIN.0000000000000255] [PMID]
14. Hsu W, Chiang C, Yang S. The effect of individual factors on health behaviors among college students: The mediating effects of health literacy. J Med Internet Res. 2014;16(12):287. [Link] [DOI:10.2196/jmir.3542] [PMID] [PMCID]
15. Vahedian-Azimi A, Ebadi A, Saadat S, Ahmadi F. Intelligence care: A nursing care strategy in respiratory intensive care unit. Iran Red Crescent Med J. 2015;17(11):20551. [Persian] [Link] [DOI:10.5812/ircmj.20551]
16. Lee YH, Ji EJ, Yun OJ. Health concern, health information orientation, e-health literacy and health behavior in aged women: Focused on 60-70s. J Converg Inf Technol. 2019;9(4):39-47. [Link]
17. Tan SSL, Goonawardene N. Internet health information seeking and the patient-physician relationship: A systematic review. J Med Internet Res. 2017;19(1):9. [Link] [DOI:10.2196/jmir.5729] [PMID] [PMCID]
18. Nsuangani NM, Perez MA. Accessing web-based health related information by college students. Calif J Health Promot. 2006;4(1):64-74. [Link] [DOI:10.32398/cjhp.v4i1.734]
19. Portnoy DB, Scott-Sheldon LAJ, Johnson BT, Carey MP. Computer-delivered interventions for health promotion and behavioral risk reduction: A meta-analysis of 75 randomized controlled trials, 1988-2007. Prev Med. 2008;47(1):3-16. [Link] [DOI:10.1016/j.ypmed.2008.02.014] [PMID] [PMCID]
20. Xie B. Improving older adults'e-health literacy through computer training using NIH online resources. Libr Inf Sci Res. 2012;34(1):63-71. [Link] [DOI:10.1016/j.lisr.2011.07.006] [PMID] [PMCID]
21. Neter E, Brainin E. Association between health literacy, ehealth literacy, and health outcomes among patients with long-term conditions: A systematic review. Eur Psychol. 2019;24(1):68-81. [Link] [DOI:10.1027/1016-9040/a000350]
22. Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: Development and psychometric characteristics. Nurs Res. 1987;36(2):76-81. [Link] [DOI:10.1097/00006199-198703000-00002]
23. Tanjani PT, Azadbakht M, Garmaroudi G, Sahaf R, Fekrizadeh Z. Validity and reliability of health promoting lifestyle profile II in the Iranian elderly. Int J Prev Med. 2016;7:74. [Link] [DOI:10.4103/2008-7802.182731] [PMID] [PMCID]
24. Bazm S, Mirzaei M, Fallahzadeh H, Bazm R. Validity and reliability of the Iranian version of eHealth literacy scale. J Community Health Res. 2016;5(2):121-30. [Persian]. [Link]
25. Oh JH, Park E. The impact of health literacy on self-care behaviors among hypertensive elderly. Korean J Health Educ Promot. 2017;34(1):35-45. [Link] [DOI:10.14367/kjhep.2017.34.1.35]
26. Harooni J, Hassanzadeh A, Mostafavi F. Influencing factors on health promoting behavior among the elderly living in the community. J Educ Health Promot. 2014;3:40. [Link]
27. Alizadeh L, Salehi L. Older people's perspectives on health, physical activity and nutritional behaviors. Health Promot Perspect. 2015;5(4):288-95. [Persian] [Link] [DOI:10.15171/hpp.2015.034] [PMID] [PMCID]
28. Momeni K, Rafiee Z. Correlation of social support and religious orientation with life satisfaction in the elderly. SALMAND. 2018;13(1):50-61. [Persian] [Link] [DOI:10.21859/sija.13.1.50]
29. Tennant B, Stellefson M, Dodd V, Chaney B, Chaney D, Paige S, et al. Health literacy and web 2.0 health information seeking behaviors among baby boomers and older adults. J Med Internet Res. 2015;17(3):70. [] [DOI:10.2196/jmir.3992] [PMID] [PMCID]
30. Medlock S, Eslami S, Askari M, Arts DL, Sent D, De Rooij SE, et al. Health information-seeking behavior of seniors who use the internet: A survey. J Med Internet Res. 2015;17(1):10. [] [DOI:10.2196/jmir.3749] [PMID] [PMCID]
31. Baji F, Bigdeli Z, Parsa A, Haeusler C. Developing information literacy skills of the 6th grade students using the big 6 model. Malays J Libr Inf Sci. 2018;23(1):1-15. [] [DOI:10.22452/mjlis.vol23no1.1]
32. Park H, Cormier E, Gordon G, Baeg JH. Identifying health consumers' eHealth literacy to decrease disparities in accessing ehealth information. Comput Inform Nurs. 2016;34(2):71-6. [] [DOI:10.1097/CIN.0000000000000205] [PMID]
33. Marrie RA, Salter AR, Tyry T, Fox RJ, Cutter GR. Preferred sources of health information in persons with multiple sclerosis: Degree of trust and information sought. J Med Internet Res. 2013;15(4):67. [] [DOI:10.2196/jmir.2466] [PMID] [PMCID]
34. Chu JT, Wang MP, Shen C, Lam TH, Viswanath K, Chan SSC. How, when and why people seek health information online: Qualitative study in Hong Kong. Interact J Med Res. 2017;6(2):24. [Link] [DOI:10.2196/ijmr.7000] [PMID] [PMCID]
35. Baumeister H, Kraft R, Baumel A, Pryss R, Messner EM. Persuasive e-health design for behavior change. In: Baumeister H, Montag C. Digital phenotyping and mobile sensing. Berlin: Springer Nature Switzerland AG; 2019. [Link] [DOI:10.1007/978-3-030-31620-4_17]
36. Adib-Hajbaghery M, Akbari H. The severity of old age disability and its related factors. FEYZ. 2009;13(3):225-34. [Persian] [Link]
37. Flocke SA, Crabtree BF, Stange KC. Clinician reflections on promotion of healthy behaviors in primary care practice. Health Policy. 2007;84(2-3):277-83. [Link] [DOI:10.1016/j.healthpol.2007.04.003] [PMID] [PMCID]
38. Rashedi S, Bahrami M. Factors related to the health promoting life style among geriatric patients. Nurs. Midwifery J. 2015;13(2):90-8. [Persian] [Link]
39. Ohm R. The African American experience in the Islamic faith. Public Health Nurs. 2003;20(6):478-86. [Link] [DOI:10.1046/j.1525-1446.2003.20608.x] [PMID]
40. Schneider S. Causes of socioeconomic group-related mortality in the federal republic of Germany-tobacco consumption is the predominant risk factor. Int J Public Health. 2007;52(1)39-53. [Link] [DOI:10.1007/s00038-006-5073-y] [PMID]
41. Perna L, Mielck A, Lacruz ME, Emeny RT, Holle R, Breitfelder A, et al. Socioeconomic position, resilience, and health behaviour among elderly people. Int J Public Health. 2012;57(2):341-9. [Link] [DOI:10.1007/s00038-011-0294-0] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |