



Volume 9, Issue 2 (2021)
Health Educ Health Promot 2021, 9(2): 165-170 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Motlagh Z, Mombani A, Rakhshani T, Bizhani B, Tavakoli Ghouchani H. Effect of Education in Choosing the Type of Delivery in Primiparous Pregnant Women. Health Educ Health Promot 2021; 9 (2) :165-170
URL: http://hehp.modares.ac.ir/article-5-46775-en.html
URL: http://hehp.modares.ac.ir/article-5-46775-en.html
1- Department of Public Health, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran
2- Jondi Shapoor University of Medical Science, Ahvaz, Iran
3- Research Center for Health Sciences, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran , virtualhealth20@gmail.com
4- Department of Health Education and Promotion, School of Public Health, North Khorasan University of Medical Sciences, Bojnord, Iran
2- Jondi Shapoor University of Medical Science, Ahvaz, Iran
3- Research Center for Health Sciences, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran , virtualhealth20@gmail.com
4- Department of Health Education and Promotion, School of Public Health, North Khorasan University of Medical Sciences, Bojnord, Iran
Full-Text [PDF 488 kb]
(960 Downloads)
| Abstract (HTML) (1053 Views)
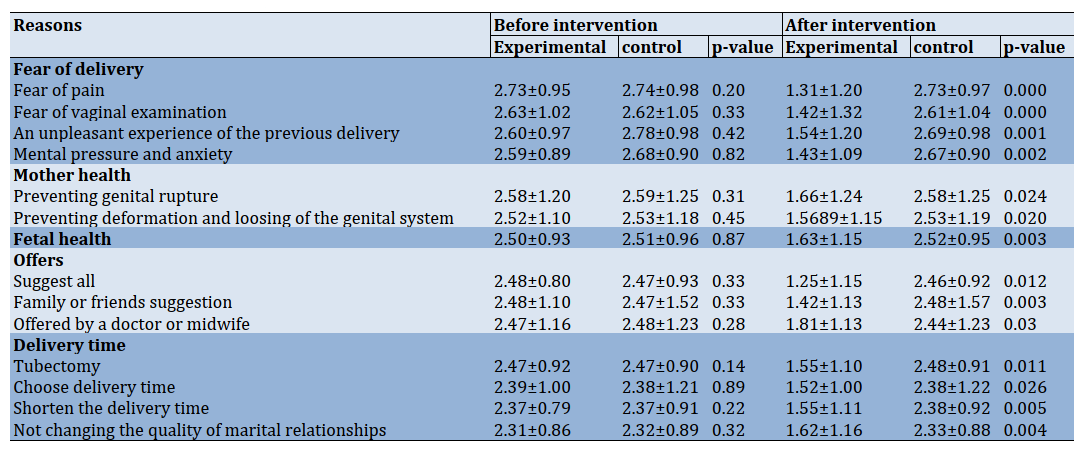
Table 3) Comparing the mean±SD of reasons for choosing cesarean section and their dimensions before and after intervention in experimental and control groups
Full-Text: (344 Views)
Introduction
Cesarean refers to removing a fetus from the cutting place of the abdominal cavity and the womb. When natural vaginal is prohibited, a cesarean is done to ensure the health of the mother and the baby [1]; fetal distress, high maternal age at delivery, delivery arrest, fetal distress, and abnormal fetal positions are common reasons for C-section [2] All of these causes are 10 percent of giving birth, and about 90 percent of the childbirth can be taken as natural without therapeutic intervention. Despite the recommendations by WHO that no region in the world is justified to have a cesarean section rate greater than 10-15%, it is the most common obstetrical operation worldwide [3]. The rate of C-section has been increased globally such that in Canada, England it is 20, 25 respectively [4, 5]. In recent years, the rate of C-sections in Iran has been raised in both private and public centers so that the country has been among the first four countries with high C-sections rates in the world. Here, in Iran,47% of deliveries are terminated by C-section [3].
Like other surgical operations, CS carries the risk of infection, including local wounds, pelvic, respiratory tract, urinary tract infections, lung emboli, venous thrombosis, and complications of anesthesia. Thus morbidity and mortality rates are higher in CS than normal vaginal delivery (NVD) in both mother and child [6].
Nowadays, it tried to reduce the cesarean rate by applying new maternal and child health policies and many interventions in most developed countries. For example, they could significantly decrease the cesarean rate by using a successful strategy by penetrating doctors and changing their motivation for cesarean [7]. In a US study, the incidence of cesarean section decreased from 13.5% to 6.5%, the first cesarean section decreased from 9.5% to 4%, repeat cesarean decreased from 4% to 2.5%, and cesarean section caused by fetal distress decreased from 2.7% to 0.63% [8].
Iran also managed to reduce the rate of cesarean section by 15% based on the study of Tavassoli by teaching mothers and creating mental and psychological readiness in mothers for natural childbirth [9]. The high rate of cesarean in Iran, distance from WHO slogan (Cesarean delivery by 15% by 2010), and interventions on decreasing cesarean section show the need for more serious interventions in these subjects [10]. One of the plans to reduce unnecessary cesarean section is focusing on educational efforts during pregnancy. One service predicted during prenatal care is teaching pregnant women to raise knowledge about childbirth to maintain and improve their health and the fetus [11]. Teaching pregnant women about giving birth and its process can lead to their mental and psychological readiness to deal with labor pain [12]. We can increase the knowledge of pregnant women about delivery methods to select a suitable method by the doctor advised not to select a cesarean section without clinical causes [13].
The studies have shown that teaching mothers has affected their knowledge and increased the natural childbirth rate [12, 13]. Lashgari et al. used video, speech, and brochure in the intervention group and compared cesarean rate to testimonial who received only normal perinatal care. They conclude that teaching mothers lead to a decrease cesarean rate by mother's wish. Therefore, they advise teaching mothers during pregnancy [14]. Other studies also show that teaching mothers are very effective in increasing knowledge and selecting childbirth. In a raiding study, the women were trained for natural childbirth had fewer fears of childbirth than the control group [15].
Increasing the level of knowledge and understanding of pregnant mothers about the problems and complications related to cesarean section and correcting some misconceptions about natural childbirth reduces the fear of facing the unknown. Due to the importance of providing, maintaining and health of mothers and infants as two vulnerable groups in society and promoting natural childbirth as a basic policy in the health system, the present study was conducted with the aim determining of the effect of education in choosing the type of delivery in primiparous pregnant women. In the present study, the training was based on reducing barriers to vaginal delivery.
Materials and Methods
This randomized controlled trial was conducted in 2018 on 190 pregnant women referring to health centers in Ramhormoz, Iran. Samples were randomly assigned to groups by using a random number table. Randomization was concealed in sequentially numbered, opaque, sealed, and stapled envelopes. The sample size for the present study was determined according to a similar study [12], by taking α=0.01 and β=0.05, 80 subjects for each group using the Pocake formula [16]. The potential loss to follow-up was anticipated to be 30% per group, so 95 subjects were planned to be randomized to each group. The criteria for entering the study included: 1. Pregnant women who were primiparous 2. Pregnant women who were in the third trimester of pregnancy (26-40 weeks of pregnancy). 3. Pregnant women who have chosen cesarean delivery to give birth to their baby. 4. Participate in this study must be acquiescent. The criteria to exit of study include preterm childbirth, multiple pregnancy diagnosis, small pelvic glands, diabetes, and history of high blood pressure.
The questionnaire written by Seyedeh Nouri & Jamshidi [17] was used, which contained 65 questions and consisted of 4 parts: the first part consists of 14 questions related to demographic characteristics and midwifery records, the second part consists of 22 questions related to the level of knowledge and Their sources of information about the benefits and disadvantages of cesarean section, the third part consists of 14 questions related to the attitudes of research units on cesarean section, and the fourth part contains 14 questions related to some reasons for choosing cesarean section by research units. The criteria for measuring knowledge were the number of correct answers. Each correct answer has 2 points, and the "false" and "I do not know" have zero points. Thus, the knowledge rating is from 0 to 44, which means that higher scores mean more knowledge. Measurement of attitude level was also scored based on a Likert scale of 5 parts of 0 (totally disagree) to 4 (totally agree). Thus, the points of view have a range of 0-56, so that the increase in the score points to an increased inclination to perform a cesarean section. The reasons for choosing a cesarean section were scored based on the number of items and the 4-part Likert scale. The validity and reliability of the questionnaire have been confirmed by Seyedeh Nouri & Jamshidi to determine reliability was used from test-retest (r=0.89) [17]. Also, the reliability of this questionnaire has been confirmed by Fathian et al., based on Cronbach's alpha test (Cronbach's alpha=0.96) [16].
This study was approved by the Ethics Committee of Shiraz University of Medical Sciences. The objectives were explained to each participant, and the informed consent form was completed by them. The questionnaire was completed before and after the last training session for both experimental and control groups. The education program for the experimental group consisted of 4 sessions of a 90-minute group training session within a month; additionally, an educational session for pregnant women's husbands and one meeting for a person having an impact on the pregnant woman. The content of the lecture classes included providing the necessary training mothers a variety of vaginal delivery methods, and cesarean section, the benefits and complications of each, appropriate nutrition, tensile and adequate ventilation techniques, and the book of pregnancy training and Preparedness for childbirth was introduced by the Ministry of Health [18]; presentation of educational materials was via PowerPoint, as well as educational pamphlets were provided to pregnant women; At the end of each educational class, opportunities for expressing the opinions and questions and ambiguities of women participated in class. Mothers completed post-test questionnaires in the last session of the training class. The control group received common prenatal care.
Kolmogorov-Smirnov statistical test was used to assess the normal distribution of data. The independent t-test was used to compare intergroup differences; paired t-test was deployed to compare intra-group differences. The Chi-square test was used to compare categorical variables. Results were considered significant at p<0.05. The data were analyzed by SPSS 19.0.
Findings
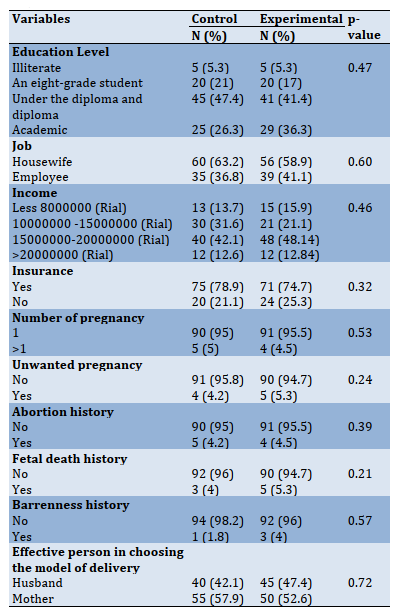
The mean age of the experimental group was 27.37±0.00, and the control group was 27.91±0.00. There was no significant difference between the experimental group and control group in age (p>0.05) and other variables (Table 1).
Table 1) Demographic characteristics of the women in the study
The independent t-test showed that before training, the mean of knowledge was not significantly different between the experimental and control groups, but it was significantly different (Table 2).
Table 2) Comparison of the mean of knowledge and attitude before and after the intervention in the experimental and control group

The mean scores of dimensions of the reasons for choosing cesarean section before training were not significantly different between the experimental group and control group (p>0.05), but after training, there were significant differences between the two groups (p<0.05).
Cesarean refers to removing a fetus from the cutting place of the abdominal cavity and the womb. When natural vaginal is prohibited, a cesarean is done to ensure the health of the mother and the baby [1]; fetal distress, high maternal age at delivery, delivery arrest, fetal distress, and abnormal fetal positions are common reasons for C-section [2] All of these causes are 10 percent of giving birth, and about 90 percent of the childbirth can be taken as natural without therapeutic intervention. Despite the recommendations by WHO that no region in the world is justified to have a cesarean section rate greater than 10-15%, it is the most common obstetrical operation worldwide [3]. The rate of C-section has been increased globally such that in Canada, England it is 20, 25 respectively [4, 5]. In recent years, the rate of C-sections in Iran has been raised in both private and public centers so that the country has been among the first four countries with high C-sections rates in the world. Here, in Iran,47% of deliveries are terminated by C-section [3].
Like other surgical operations, CS carries the risk of infection, including local wounds, pelvic, respiratory tract, urinary tract infections, lung emboli, venous thrombosis, and complications of anesthesia. Thus morbidity and mortality rates are higher in CS than normal vaginal delivery (NVD) in both mother and child [6].
Nowadays, it tried to reduce the cesarean rate by applying new maternal and child health policies and many interventions in most developed countries. For example, they could significantly decrease the cesarean rate by using a successful strategy by penetrating doctors and changing their motivation for cesarean [7]. In a US study, the incidence of cesarean section decreased from 13.5% to 6.5%, the first cesarean section decreased from 9.5% to 4%, repeat cesarean decreased from 4% to 2.5%, and cesarean section caused by fetal distress decreased from 2.7% to 0.63% [8].
Iran also managed to reduce the rate of cesarean section by 15% based on the study of Tavassoli by teaching mothers and creating mental and psychological readiness in mothers for natural childbirth [9]. The high rate of cesarean in Iran, distance from WHO slogan (Cesarean delivery by 15% by 2010), and interventions on decreasing cesarean section show the need for more serious interventions in these subjects [10]. One of the plans to reduce unnecessary cesarean section is focusing on educational efforts during pregnancy. One service predicted during prenatal care is teaching pregnant women to raise knowledge about childbirth to maintain and improve their health and the fetus [11]. Teaching pregnant women about giving birth and its process can lead to their mental and psychological readiness to deal with labor pain [12]. We can increase the knowledge of pregnant women about delivery methods to select a suitable method by the doctor advised not to select a cesarean section without clinical causes [13].
The studies have shown that teaching mothers has affected their knowledge and increased the natural childbirth rate [12, 13]. Lashgari et al. used video, speech, and brochure in the intervention group and compared cesarean rate to testimonial who received only normal perinatal care. They conclude that teaching mothers lead to a decrease cesarean rate by mother's wish. Therefore, they advise teaching mothers during pregnancy [14]. Other studies also show that teaching mothers are very effective in increasing knowledge and selecting childbirth. In a raiding study, the women were trained for natural childbirth had fewer fears of childbirth than the control group [15].
Increasing the level of knowledge and understanding of pregnant mothers about the problems and complications related to cesarean section and correcting some misconceptions about natural childbirth reduces the fear of facing the unknown. Due to the importance of providing, maintaining and health of mothers and infants as two vulnerable groups in society and promoting natural childbirth as a basic policy in the health system, the present study was conducted with the aim determining of the effect of education in choosing the type of delivery in primiparous pregnant women. In the present study, the training was based on reducing barriers to vaginal delivery.
Materials and Methods
This randomized controlled trial was conducted in 2018 on 190 pregnant women referring to health centers in Ramhormoz, Iran. Samples were randomly assigned to groups by using a random number table. Randomization was concealed in sequentially numbered, opaque, sealed, and stapled envelopes. The sample size for the present study was determined according to a similar study [12], by taking α=0.01 and β=0.05, 80 subjects for each group using the Pocake formula [16]. The potential loss to follow-up was anticipated to be 30% per group, so 95 subjects were planned to be randomized to each group. The criteria for entering the study included: 1. Pregnant women who were primiparous 2. Pregnant women who were in the third trimester of pregnancy (26-40 weeks of pregnancy). 3. Pregnant women who have chosen cesarean delivery to give birth to their baby. 4. Participate in this study must be acquiescent. The criteria to exit of study include preterm childbirth, multiple pregnancy diagnosis, small pelvic glands, diabetes, and history of high blood pressure.
The questionnaire written by Seyedeh Nouri & Jamshidi [17] was used, which contained 65 questions and consisted of 4 parts: the first part consists of 14 questions related to demographic characteristics and midwifery records, the second part consists of 22 questions related to the level of knowledge and Their sources of information about the benefits and disadvantages of cesarean section, the third part consists of 14 questions related to the attitudes of research units on cesarean section, and the fourth part contains 14 questions related to some reasons for choosing cesarean section by research units. The criteria for measuring knowledge were the number of correct answers. Each correct answer has 2 points, and the "false" and "I do not know" have zero points. Thus, the knowledge rating is from 0 to 44, which means that higher scores mean more knowledge. Measurement of attitude level was also scored based on a Likert scale of 5 parts of 0 (totally disagree) to 4 (totally agree). Thus, the points of view have a range of 0-56, so that the increase in the score points to an increased inclination to perform a cesarean section. The reasons for choosing a cesarean section were scored based on the number of items and the 4-part Likert scale. The validity and reliability of the questionnaire have been confirmed by Seyedeh Nouri & Jamshidi to determine reliability was used from test-retest (r=0.89) [17]. Also, the reliability of this questionnaire has been confirmed by Fathian et al., based on Cronbach's alpha test (Cronbach's alpha=0.96) [16].
This study was approved by the Ethics Committee of Shiraz University of Medical Sciences. The objectives were explained to each participant, and the informed consent form was completed by them. The questionnaire was completed before and after the last training session for both experimental and control groups. The education program for the experimental group consisted of 4 sessions of a 90-minute group training session within a month; additionally, an educational session for pregnant women's husbands and one meeting for a person having an impact on the pregnant woman. The content of the lecture classes included providing the necessary training mothers a variety of vaginal delivery methods, and cesarean section, the benefits and complications of each, appropriate nutrition, tensile and adequate ventilation techniques, and the book of pregnancy training and Preparedness for childbirth was introduced by the Ministry of Health [18]; presentation of educational materials was via PowerPoint, as well as educational pamphlets were provided to pregnant women; At the end of each educational class, opportunities for expressing the opinions and questions and ambiguities of women participated in class. Mothers completed post-test questionnaires in the last session of the training class. The control group received common prenatal care.
Kolmogorov-Smirnov statistical test was used to assess the normal distribution of data. The independent t-test was used to compare intergroup differences; paired t-test was deployed to compare intra-group differences. The Chi-square test was used to compare categorical variables. Results were considered significant at p<0.05. The data were analyzed by SPSS 19.0.
Findings
The mean age of the experimental group was 27.37±0.00, and the control group was 27.91±0.00. There was no significant difference between the experimental group and control group in age (p>0.05) and other variables (Table 1).
Table 1) Demographic characteristics of the women in the study
The independent t-test showed that before training, the mean of knowledge was not significantly different between the experimental and control groups, but it was significantly different (Table 2).
Table 2) Comparison of the mean of knowledge and attitude before and after the intervention in the experimental and control group
The mean scores of dimensions of the reasons for choosing cesarean section before training were not significantly different between the experimental group and control group (p>0.05), but after training, there were significant differences between the two groups (p<0.05).
Table 3) Comparing the mean±SD of reasons for choosing cesarean section and their dimensions before and after intervention in experimental and control groups
Discussion
In the present study, after the intervention, the mean score of knowledge about cesarean in the experimental group was more than the control group. Lashgari et al., who considered the effect of training on selecting the kind of childbirth, the knowledge of the mothers of the trained group about normal delivery and cesarean section was significantly increased [14]. The findings of Basharati et al. Study, based on the theory of planned behavior on pregnant women, showed that after the intervention, there was a significant difference in the mean score of knowledge, evaluation of the results, attitude, and practice between the intervention and control groups [19]. In the study of Isfaya et al. On pregnant women referring to Tehran health centers, after the intervention, the mean score of knowledge about cesarean section was significantly higher than before the study [20]. A study conducted in England on female interference in deciding for cesarean section showed that most women were satisfied by the information given them during the cesarean section about their pregnancy, and they were pleased to be involved in their decision to perform a cesarean section. However, half of the women were not convinced of the reasons for the cesarean section before discharge from the department. The study concludes that pregnant women are not the same in need of information and decision making for a delivery method, and therefore health workers should respond to different information needs of women at different levels [21].
In the present study, the mean score of attitude toward a cesarean section in the experimental group was less than in the intervention group. In Besharati et al.'s study [19] and Rezakhani et al.'s study [13], the intervention means a score of attitude in the experimental group was significantly different from the CG. In the study of Kananikandeh [22] on pregnant women in Parsabad after the intervention, the mean score of attitude toward natural childbirth was significantly higher than the control group. In the study of Khani-Jeihooni et al. [23] On pregnant women covered by health centers in Fasa city, the mean attitude score was significantly different between the experimental and control groups after the intervention. Nevertheless, in Toghayani et al., although the subjects' training, knowledge, and practice significantly increased, the attitude has not been affected [24], which can be due to differences in educational contents. The educational contents of Toghayani et al. included education topics in the first trimester (genital anatomy, diagnosis of pregnancy, natural variations, and risk symptoms), second trimester (normal changes and risk symptoms), and third trimester of pregnancy (normal changes, common complaints, Sign of the risk of delivery methods, the benefits of natural vaginal delivery, contraceptive methods and exclusive breastfeeding), but in the present study, more specialized training on the types of delivery (natural and cesarean), the benefits and complications of each one, proper nutrition, tensile and suitable ventilators of breathing.
In the present study, after the intervention, the criteria for selecting the cesarean section were significantly lower in the experimental group than in the control group. For example, the fear of pain in the experimental group was significantly lower than the control group, which indicates the effect of training on the change in mothers' intention towards the cesarean section. In Amidimazaheri et al.'s study on 130 pregnant women referred to Shahrekord health centers, after the intervention, the fear of childbirth in the intervention group was significantly lower than the control group that Consistent with the present study [25].
Miri [26] showed that the first reason for selecting cesarean section in research departments by the highest average is the fear of pain and following the health of the fetus and the fear of reproductive system rupture by mothers. In the Hopkins-based multicenter study in Brazil, many women were scared of childbirth, and some of them were scared of vaginal consequences for the child. The researcher says this method of birth by surgery is a common practice to be more immune to it and consider it a safe or safer way of vaginal delivery [27]. In a study by Lee et al. in Hong Kong, more than 70% of participants in this study believed that there was no abnormal case in their pregnancy, but because it was possible to choose a cesarean section, it is necessary to tolerate pregnancy pain or to accept a possible risk to the fetus during natural vaginal delivery they did not see [28]. In order to reduce the fear of pain in pregnant women, psychotherapy, teaching different methods of relaxation during classes about delivery readiness and planning about pain relief in stages before delivery and natural vaginal.
One of the limitations of the present study was not measuring performance, which is suggested to be measured in future studies. Other limitations of the present study include the impossibility of holding more meetings for the wives of pregnant women, which is suggested in future studies to hold more meetings for the wives of pregnant women. Another limitation of this study is the low presence of pregnant women with a very good economic situation in this research because of referring these women to private centers of provincial capital for prenatal care. It is suggested that these types of studies should continue for a longer period until the delivery date to determine the impact of training in practice, and we can teach more effectively by the findings of this study. Also, due to the effectiveness of education and routine nursing care in health centers, preparation classes for delivery are done. On the other hand, due to the discomfort of some pregnant women to receive training, it is suggested that research on the effectiveness of online education methods of pregnant mothers about choosing the type of delivery and side effects of Caesarean section.
Conclusion
The effect of education on increasing pregnant mothers' knowledge and attitude can become effective in choosing the kind of delivery method and reducing cesarean rates.
Acknowledgments: We would like to thank Shiraz and Ahvaz University of Medical Sciences, Ramhormoz health centers, and participants in this study.
Ethical Permissions: The Ethics Committee Board of Shiraz University of Medical Sciences has approved this study (the ethics code: IR.SUMS.REC.1396.42).
Conflicts of Interests: This article is taken from Azita Mombani dissertation, and there was no conflict of interest.
Authors' Contribution: Motlagh Z. (First author), Methodologist/Original researcher (20%); Mombani A. (Second author), Introduction author/Assistant researcher/Discussion author (20%); Rakhshani T. (Third author), Methodologist/Original researcher (20%); Bizhani B. (Forth author), Statistical analyst (20%); Tavakoli Ghouchani H. (Fifth author), Discussion author (20%).
Funding/Sources: This study was not supported financially.
In the present study, after the intervention, the mean score of knowledge about cesarean in the experimental group was more than the control group. Lashgari et al., who considered the effect of training on selecting the kind of childbirth, the knowledge of the mothers of the trained group about normal delivery and cesarean section was significantly increased [14]. The findings of Basharati et al. Study, based on the theory of planned behavior on pregnant women, showed that after the intervention, there was a significant difference in the mean score of knowledge, evaluation of the results, attitude, and practice between the intervention and control groups [19]. In the study of Isfaya et al. On pregnant women referring to Tehran health centers, after the intervention, the mean score of knowledge about cesarean section was significantly higher than before the study [20]. A study conducted in England on female interference in deciding for cesarean section showed that most women were satisfied by the information given them during the cesarean section about their pregnancy, and they were pleased to be involved in their decision to perform a cesarean section. However, half of the women were not convinced of the reasons for the cesarean section before discharge from the department. The study concludes that pregnant women are not the same in need of information and decision making for a delivery method, and therefore health workers should respond to different information needs of women at different levels [21].
In the present study, the mean score of attitude toward a cesarean section in the experimental group was less than in the intervention group. In Besharati et al.'s study [19] and Rezakhani et al.'s study [13], the intervention means a score of attitude in the experimental group was significantly different from the CG. In the study of Kananikandeh [22] on pregnant women in Parsabad after the intervention, the mean score of attitude toward natural childbirth was significantly higher than the control group. In the study of Khani-Jeihooni et al. [23] On pregnant women covered by health centers in Fasa city, the mean attitude score was significantly different between the experimental and control groups after the intervention. Nevertheless, in Toghayani et al., although the subjects' training, knowledge, and practice significantly increased, the attitude has not been affected [24], which can be due to differences in educational contents. The educational contents of Toghayani et al. included education topics in the first trimester (genital anatomy, diagnosis of pregnancy, natural variations, and risk symptoms), second trimester (normal changes and risk symptoms), and third trimester of pregnancy (normal changes, common complaints, Sign of the risk of delivery methods, the benefits of natural vaginal delivery, contraceptive methods and exclusive breastfeeding), but in the present study, more specialized training on the types of delivery (natural and cesarean), the benefits and complications of each one, proper nutrition, tensile and suitable ventilators of breathing.
In the present study, after the intervention, the criteria for selecting the cesarean section were significantly lower in the experimental group than in the control group. For example, the fear of pain in the experimental group was significantly lower than the control group, which indicates the effect of training on the change in mothers' intention towards the cesarean section. In Amidimazaheri et al.'s study on 130 pregnant women referred to Shahrekord health centers, after the intervention, the fear of childbirth in the intervention group was significantly lower than the control group that Consistent with the present study [25].
Miri [26] showed that the first reason for selecting cesarean section in research departments by the highest average is the fear of pain and following the health of the fetus and the fear of reproductive system rupture by mothers. In the Hopkins-based multicenter study in Brazil, many women were scared of childbirth, and some of them were scared of vaginal consequences for the child. The researcher says this method of birth by surgery is a common practice to be more immune to it and consider it a safe or safer way of vaginal delivery [27]. In a study by Lee et al. in Hong Kong, more than 70% of participants in this study believed that there was no abnormal case in their pregnancy, but because it was possible to choose a cesarean section, it is necessary to tolerate pregnancy pain or to accept a possible risk to the fetus during natural vaginal delivery they did not see [28]. In order to reduce the fear of pain in pregnant women, psychotherapy, teaching different methods of relaxation during classes about delivery readiness and planning about pain relief in stages before delivery and natural vaginal.
One of the limitations of the present study was not measuring performance, which is suggested to be measured in future studies. Other limitations of the present study include the impossibility of holding more meetings for the wives of pregnant women, which is suggested in future studies to hold more meetings for the wives of pregnant women. Another limitation of this study is the low presence of pregnant women with a very good economic situation in this research because of referring these women to private centers of provincial capital for prenatal care. It is suggested that these types of studies should continue for a longer period until the delivery date to determine the impact of training in practice, and we can teach more effectively by the findings of this study. Also, due to the effectiveness of education and routine nursing care in health centers, preparation classes for delivery are done. On the other hand, due to the discomfort of some pregnant women to receive training, it is suggested that research on the effectiveness of online education methods of pregnant mothers about choosing the type of delivery and side effects of Caesarean section.
Conclusion
The effect of education on increasing pregnant mothers' knowledge and attitude can become effective in choosing the kind of delivery method and reducing cesarean rates.
Acknowledgments: We would like to thank Shiraz and Ahvaz University of Medical Sciences, Ramhormoz health centers, and participants in this study.
Ethical Permissions: The Ethics Committee Board of Shiraz University of Medical Sciences has approved this study (the ethics code: IR.SUMS.REC.1396.42).
Conflicts of Interests: This article is taken from Azita Mombani dissertation, and there was no conflict of interest.
Authors' Contribution: Motlagh Z. (First author), Methodologist/Original researcher (20%); Mombani A. (Second author), Introduction author/Assistant researcher/Discussion author (20%); Rakhshani T. (Third author), Methodologist/Original researcher (20%); Bizhani B. (Forth author), Statistical analyst (20%); Tavakoli Ghouchani H. (Fifth author), Discussion author (20%).
Funding/Sources: This study was not supported financially.
Article Type: Original Research |
Subject:
Family Health Education/Promotion
Received: 2020/10/13 | Accepted: 2021/03/12 | Published: 2021/07/13
Received: 2020/10/13 | Accepted: 2021/03/12 | Published: 2021/07/13
References
1. Cunningham FG, Leveno K, Bloom S, Spong C, Dashe J, Hoffman B, et al. Williams Obstetrics. New York: McGraw-Hill Education; 2018. [Link]
2. Bagheri A, Masoodi-Alavi N, Abbaszade F. Effective factors for choosing the delivery method among the pregnant women in Kashan. FEYZ. 2012;16(2):146-53. [Persian] [Link]
3. Zamani-Alavijeh F, Araban M, Hassanzadeh A, Makhouli K. Contributing factors of pregnant women's beliefs towards mode of delivery: A cross-sectional study from Iran. Matern Health Neonatol Perinatol. 2018;4:9. [Link] [DOI:10.1186/s40748-018-0077-1] [PMID] [PMCID]
4. Rafati F, Rafati SH, Madani A, Mashayekhi F, Pilevarzadeh M. Related factors to choose cesarean section among Jiroft pregnant women. J Prev Med. 2014;1(1):23-30. [Persian] [Link]
5. Li WY, Liabsuetrakul T, Stray-Pedersen B. Effect of mode of delivery on perceived risks of maternal health outcomes among expectant parents: A cohort study in Beijing, China. BMC Pregnancy Childbirth. 2014;14:12. [Link] [DOI:10.1186/1471-2393-14-12] [PMID] [PMCID]
6. Ghotbi F, Akbari Sene A, Azargashb E, Shiva F, Mohtadi M, Zadehmodares S, et al. Women's knowledge and attitude towards mode of delivery and frequency of cesarean section on mother's request in six public and private hospitals in Tehran, Iran, 2012. J Obstet Gynaecol Res. 2014;40(5):1257-66. [Link] [DOI:10.1111/jog.12335] [PMID]
7. Naghibi KH, Allameh K and Montazeri K. Which one is better? painless delivery or cesarean section. Isfahan Univ Med Sci. 2001;1(1):38-40. [Persian] [Link]
8. Iran data portal. Ministry of health and medical education [Internet] Tehran: Iran Data Portal; 2015 [Unknown Cited]. Available from: https://irandataportal.syr.edu/ministry-of-health-and-medical-education. [Link]
9. Signorelli C, Cattaruzza MS, Osborn JF. Risk factors for cesarean section in Italy: Resulted of multicenter study. Public Health. 1995;109(3):191-9. [Link] [DOI:10.1016/S0033-3506(05)80052-6]
10. Porreco RP. Meeting the challenge of the rising cesarean birth rate. Obstet Gynecol. 1990;75(1):133-6. [Link] [DOI:10.1016/0020-7292(90)90662-5]
11. Tully KP, Ball HL. Misrecognition of need: Women's experiences of and explanations for undergoing cesarean delivery. Soc Sci Med. 2013;85:103-11. [Link] [DOI:10.1016/j.socscimed.2013.02.039] [PMID] [PMCID]
12. Shahraki Sanavi F, Ansari-Moghaddam A, Rakhshan F, Navabi Rigi S. Two teaching methods to encourage pregnant women for performing normal vaginal delivery. Iran J Med Educ. 2012;12(3):184-92. [Persian] [Link]
13. Rezakhani Moghaddam H, Shojaeizadeh D, Taghdisi MH, Hamidzadeh Arbabi Y, Savadpour MT. The effect of education by community health volunteers on choice of delivery kind in pregnant women based on the Behavioral Intention Model (BIM). J Sch Public Health Inst Public Health Res. 2013;10(3):27-40. [Persian] [Link]
14. Lashgari MH, Delavari S, Markazi Moghadam N, Gorouhi F. Effects of training programs of pregnant women on their delivery type selection: A single blind, randomized control trial. Ann Mil Health Sci Res. 2005;3(4):679-84. [Persian] [Link]
15. Ryding EL, Persson A, Onell C, Kvist L. An evaluation of midwives' counseling of pregnant women in fear of childbirth. Acta Obstet Gynecol Scand. 2003;82(1):10-7. [Link] [DOI:10.1034/j.1600-0412.2003.820102.x] [PMID]
16. Fathian Z, Sharifi G, Hasanzadeh A, Fathian Z. The effect of education on knowledge, attitude and operation of pregnant women than vaginal delivery based on behavioral intention model in Khomein city, 2006. Zahedan J Res Med Sci. 2007;9(2):123-31. [Persian] [Link]
17. Seyedeh Nouri T, Jamshidi Yvanaki F. Evaluation of relationship between knowledge and attitude of pregnant women applicant for cesarean section with the reasons for choosing cesarean section by them referring to health center in Rasht. Guilan Univ Med Sci. 2006;15(59):75-84. [Persian] [Link]
18. Imami Afshar N, Torkzahrani S, Jalilvand P, Changizi N, Hejazi S, Khodakarami N, et al. Pregnancy training and preparation for delivery. Tehran: PAJHWAK ARMAN; 2009. [Persian] [Link]
19. Besharati F, Hazavehei SMM, Moeini B, Moghimbeigi A. Effect of educational interventions based on theory of planned behavior (TPB) in selecting delivery mode among pregnant women referred to Rasht health centers. J Adv Med Biomed Res. 2011;19(77):94-106. [Persian] [Link]
20. Asfia A, Azam K, Babaei Heydarabadi A, Gilasi HR, Ghanei Z, Dariyani A, et al. The effect of health education on knowledge and attitudes about cesarean in Tehrani women. Adv Nurs Midwifery. 2013;22(79). [Persian] [Link]
21. Litch CR, Walker JJ. The rise in cesarean section rate: The same indication but a lower threshold. Br J Obstet Gynaecol. 1998;105(6):621-6. [Link] [DOI:10.1111/j.1471-0528.1998.tb10176.x] [PMID]
22. Kananikandeh S. Persuading Iranian women toward normal vaginal delivery: Using pictorial perception of the labour process. Open Access Maced J Med Sci. 2018;6(6):1145-52. [Link] [DOI:10.3889/oamjms.2018.211] [PMID] [PMCID]
23. Khan-Jeihooni A, Shahidi F, Kashfi SM. Effectiveness of educational program based on the theory of reasoned action to decrease the rate of cesarean delivery among pregnant women in Fasa, southern Iran. J Educ Community Health. 2014;1(1):62-71. [Persian] [Link] [DOI:10.20286/jech-010162]
24. Toughyani R, Ramezani MA, Izadi M, shahidi S, Aghdak P, Motie Z, et al. The effect of prenatal care group education on pregnant mothers' knowledge, attitude and practice. Iran J Med Educ. 2008;7(2):317-24. [Persian] [Link]
25. Amidimazaheri M, Amiri M, Khorsandi M, Hasanzadeh A, Taheri Z. Does maternal education can reduce the cesarean section. PAYESH. 2015;14(5):577-86. [Persian] [Link]
26. Miri MR, Shafiee F, Haydaniya AR, Kazemnejad A. Study on behavioral intention model (BIM) to the attitude of tribermen towards family planning. J Mazandaran Univ Med Sci. 2002;12(37):67-75. [Persian] [Link]
27. Hopkins K. Are Brazilian women really choosing to deliver by cesarean. Soc Sci Med. 2000;51(5):725-40. [Link] [DOI:10.1016/S0277-9536(99)00480-3]
28. Lee LY, Holroyd E, Ng CY. Exploring factors influencing Chinese women's decision to have elective cesarean surgery. Midwifery. 2001;17(4):314-22. [Link] [DOI:10.1054/midw.2001.0274] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |